
Abstract
Aim
The 2019 novel coronavirus epidemic (COVID-19) is a highly contagious viral disease with a high rate of morbidity and mortality. Food insecurity has frequently been linked to the emergence of infectious diseases. The present study was conducted to determine the association of food insecurity and socioeconomic status with COVID-19 in the Iranian population.
Subject and methods
The study was a case–control study including 248 participants (124 COVID-19-infected people with a positive PCR test and a history of clinical symptoms of COVID-19 and 124 non-infected people with a negative PCR test and no history of clinical symptoms of COVID-19 infection) aged 20 to 60 years. The participants in the two groups were matched based on age, sex, and BMI. Anthropometric and socioeconomic data were collected. Individuals’ food insecurity status during the previous 12 months (before the disease for the case group) was assessed using a validated 18-item USDA questionnaire.
Results
About 44% of the controls and 76% of the case group were food-insecure (P < 0.001). After controlling for any possible confounders, only food insecurity and poor economic level increased the risk of COVID-19, by about three times (OR = 3.10; 95% CI = 1.44–6.68; P = 0.004) and 9.5 times (OR = 9.53; 95% CI = 3.73–24.30; P < 0.001), respectively.
Conclusion
Food insecurity and poor economic status are linked to an increased risk of COVID-19. Future prospective studies are needed to confirm these outcomes and identify the underlying mechanisms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In late 2019 in Wuhan, China, a novel coronavirus infection epidemic began. Coronavirus disease 2019 (COVID-19), which is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is an extremely contagious and potentially fatal viral infection. The direct cause of death in this emerging disease is unusually severe pneumonia. However, there are other unusual features that lead to death (Chen et al. 2020; Huang et al. 2020; Wang et al. 2020; Zhu et al. 2020). The pathogen, the host, and the environment all play a role in determining risk factors for the severity of infectious diseases (Mouliou et al. 2021). COVID-19 encompasses a range of disease symptoms, from asymptomatic infection to severe pneumonia. Risk factors related to disease severity include aging, diabetes, immunosuppression, and organ failure (Li et al. 2021). The death rate is estimated at between 1 and 5%, but it varies according to the age and health conditions of infected individuals (Verity et al. 2020).
Food is one of the fundamental needs of human society and an integral part of people's lives, and the provision of adequate food is described by the term “food security” (Shaw 2007). The concept of food security at the household level has been taken into consideration by the efforts of international institutions, including the Food and Agriculture Organization (FAO) in the 1980s (FAO 2001). Today, the issue of food security has taken on new dimensions and has become one of the most important discussions in all countries of the world. According to the definition of the World Health Organization (WHO), “food security is the physical and economic access to healthy and nutritious food sufficient to meet the needs and food preferences for an active and healthy life,” which includes the availability of healthy and nutritionally sufficient food and the ability and confidence in obtaining acceptable foods through socially acceptable means (Bickel et al. 2006). According to the presented definition, the nutritional status of a household is determined by four factors: (1) availability of food, (2) access to food, (3) stability in supply and accessibility, and (4) safe and nutritious degree of food (Peng and Berry 2019). Lack of food security, or in other words “food insecurity,” can cause many socioeconomic issues or have negative effects on people's health, such as weakening the functioning of the immune system (Dorosty 2016; Weigel et al. 2007; Kelly et al. 2018).
In Iran, the overall prevalence of food insecurity in families is estimated between 20 and 60% in different provinces (Alimoradi et al. 2015). Recent studies show the widespread prevalence of food insecurity in Iran, with average prevalence reported to be about 49% (Daneshi-Maskooni et al. 2017).
Only a few studies have assessed the relationship between food insecurity and COVID-19 infection (Escobar et al. 2021; Kimani et al. 2021). In light of the scarcity of data on the subject among Iranians, the objective of this study was to assess and compare the status of food insecurity and socioeconomic status among COVID-19-infected and non-infected people.
Methods
Study design and population
In this case–control study, we examined 248 participants (124 COVID-19-infected patients and 124 non-infected), aged 20–60 years, from North Khorasan province, Iran. The case group subjects were considered infected with the coronavirus if they had a positive polymerase chain reaction (PCR) test together with a history of clinical symptoms of disease. The case group was included in the study if a maximum of 3 months had passed since the onset of the disease. The control group subjects were considered non-infected with the coronavirus if they had a negative PCR test and no history of clinical symptoms of disease. No participant in either group had mental or physical disabilities. The study sample was selected from office workers, factories, administrative departments of universities and hospitals, and those who were referred to public and private laboratories from March to August 2021.
The exclusion criteria included presenting symptoms or history of COVID-19 infection during the completion of the questionnaires (for the control group) and incomplete answers to questionnaires.
The case and control groups were matched according to their age (divided into four groups of 10 years each: 20–29, 30–39, 40–49, 50–59 years), gender, and body mass index (BMI, based on the WHO definition: underweight, ≤18.5; normal weight, 18.5–24.9; overweight, 25–29.9; obesity class I, 30–34.9; obesity class II, 35–39.9).
For sample size determination, a pilot study was performed on cases (n = 13) and controls (n = 13). According to the results, food insecurity was experienced by 46% of healthy people and 69% of infected patients. A sample size of 118 was calculated. However, the sample size was increased to 124 in order to ensure reliability and to account for the probability of sample loss.
Data collection
Data on general characteristics (anthropometric and socioeconomic factors) and food insecurity status were collected from all participants using validated and reliable questionnaires through face-to-face interviews after a full explanation of the study’s goals and methodology and after receiving written consent.
General characteristics
A generic questionnaire that asked about education, marital status, employment status, number of children, health insurance coverage, whether participants were receiving benefits from public and private organizations, and medical history was used to examine socioeconomic and anthropometric data. Family economic status was assessed using a nine-item questionnaire. A family’s economic level was classified as follows: ≤ 3 items as poor, 4–6 items as moderate, and ≥ 7 items as wealthy. A seca scale with accuracy of 0.1 kg was used to weigh the participants when they were wearing light clothing. Height was also measured by a measuring tape with accuracy of 0.5 cm. Then, for each participant, BMI was calculated by dividing the weight by the square of height (kg/m2). In addition, the waist circumference was measured between the chest and the hips with participants wearing light clothing, with accuracy of 0.1 cm (Taylor et al. 2000).
18-Item food security questionnaire
To assess the status of household food insecurity over the previous 12 months, the 18-item United States Department of Agriculture (USDA) food security questionnaire, which has already been validated in Iran (Ramesh et al. 2010), was used. The case group was specifically asked about food insecurity before the definitive diagnosis of COVID-19. The participants were stratified into two groups based on their scores from positive answers (score 1) or negative answers (score 0). Answers of “often,” “sometimes,” “almost every month,” “some months,” and “yes” were considered positive, and answers of “not correct,” “refused” or “did not know,” “only once or twice a month,” and no” were considered negative.” For better comparison, participants were divided into four groups based on the number of positive answers obtained from the questionnaire: score of 0–2, food-secure; 3–7, food-insecure without hunger; , 8–12, food-insecure with moderate hunger; and 13–18, food-insecure with extreme hunger (Table 1).
Statistical analysis
Quantitative and qualitative variables were presented as mean (standard deviation) and frequency (percentage), respectively. In addition, the t-test and chi-square or Fisher’s exact test were used for quantitative and qualitative data analysis, respectively. All significant variables in the primary analysis models were entered into the final analysis (multiple logistic regression) to identify independent risk factors for COVID-19. Statistical analyses were performed using IBM SPSS software (version 24). Values were considered significant for P < 0.05.
Results
A total of 248 participants who met the study inclusion criteria, including 124 infected patients with COVID-19 as the case group and 124 non-infected participants as the control group, were included in the study (Fig. 1).

Study flowchart
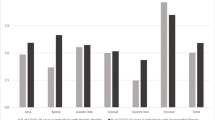
According to the data in Table 2 on the food security, anthropometric, and socioeconomic status of both groups, the prevalence of food insecurity was significantly higher in the case group than the control group (P < 0.001). Seventy-six percent of infected patients (n = 94) had food insecurity, and approximately 39% of them (n = 48) experienced food insecurity with hunger. In contrast, only 44% of the control group (n = 55) had food insecurity, and the majority (n = 42) had no hunger (Fig. 1).
Table 2 shows that the case group had a significantly poorer economic level and lower education level and house ownership than the control group (P < 0.05). There were no significant differences in waist circumference, ethnicity, employment status, insurance support, receiving benefits from public and private organizations, marriage, children and family numbers, or disease history between infected patients and healthy people (P > 0.05).
The final analysis model for the association between significant independent risk factors for COVID-19 is presented in Table 3. The odds ratios (OR) and confidence intervals (CI) indicated a significant positive association between the risk of COVID-19 and food insecurity (OR = 3.10, 95% CI = 1.44–6.68; P = 0.004) and poor economic level (OR = 9.53, 95% CI = 3.73–24.30; P < 0.001) after controlling for the potential confounders.
Discussion
In the present study, the results showed that food insecurity was significantly higher among COVID-19-infected patients than healthy individuals. Moreover, the COVID-19 risk was positively associated with food insecurity and poor economic level even after controlling for any potential confounders (Table 3). We demonstrated that participants with food insecurity and poor economic level had about 3 and 9.5 greater odds of being infected with COVID-19. To the best of our knowledge, this is the first such case–control study in Iran.
We assessed the impact of food insecurity in the previous year on the probability of COVID-19 infection. Based on the results of our study, 76% of COVID-19-infected patients and 44% of non-infected people were food-insecure. In agreement with the results of the present study, an online cross-sectional study showed that Household Food Insecurity Access Scale (HFIAS) scores were significantly higher among a COVID-19-infected group than those who were not infected (OR = 1.03, 95% CI = 1.00–1.05; P < 0.05) (Kalantari et al. 2021). Escobar et al. in a study on Californians showed that food insecurity score trended towards association with house-hold COVID-19 infection (OR = 1.25, 95% CI = 0.97–1.61) (Escobar et al. 2021). In another cross-sectional study, Kimani et al. reported that the rate of COVID-19 infection in counties of the United States with large black, American Indian, or Alaska Native populations increased as the level of food insecurity increased (Kimani et al. 2021). Also, an Iranian cross-sectional study showed that the probability of being hospitalized for COVID-19 was about four times greater (OR = 3.93, 95% CI = 1.30–11.90; P < 0.05) in patients with food insecurity than in food-secure people (Ariya et al. 2021).
Household stress, inflammatory cytokines, and behavioral pathways are three mechanisms by which food insecurity is considered a risk factor for short- and long-term health consequences (Leddy et al. 2020). People with food insecurity, especially women and families with children under 5 years old, are more afraid of contracting COVID-19 than others (Ezzeddin et al. 2022). In addition, lack of access to sufficient food and the expectation of food insecurity are especially toxic stressors. It is possible that the stress and changes in dietary patterns associated with food insecurity cause an inflammatory state and alter immune function in food-insecure individuals that not only increases the risk of chronic diseases, but also increases the risk of facing complications related to infections and greater susceptibility to infections themselves (Suardi et al. 2021). In addition, as shown in a review study, the effectiveness of antiviral drugs in food-insecure patients with HIV is lower than that in food-secure patients (Aibibula et al. 2017).
On the other hand, it has been shown that food-insecure and low-income people are less inclined to stay at home during a pandemic because they are the provider of food and basic family needs (Wolfson and Leung 2020). People who live in households with more severe food insecurity may eat less food or skip meals entirely, thus reducing the essential nutrients available for the proper functioning of the body's immune system, which can weaken the host's defense mechanisms and help reduce immunity and subsequently increase susceptibility to infectious and viral diseases (Weigel et al. 2007; Seligman and Berkowitz 2019).
Considering the results of the present study, about 57% of the case group and 19% of the control group were living at a poor economic level. Contrary to the results of the present study, a study in France reported that participants infected with COVID-19 had higher income than non-infected participants (Deschasaux-Tanguy et al. 2021). Also, two other studies did not observe a significant difference in income between COVID-19-infected and non-infected subjects (Mohseni et al. 2021; Kalantari et al. 2021). In the present study, participants were not asked to provide their income level, as people generally do not report their true income. Usually, people who live in poor economic conditions also have low levels in various other aspects such as nutritional status, food security, health status, and other factors, all of which can lead to nutritional deficiencies and subsequently increase the likelihood of infectious and viral disease, including COVID-19 (Ecob and Smith 1999; Bhattacharya et al. 2004).
Several studies have shown that poor economic level is associated with increased food insecurity (Asadi-Lari et al. 2019; Dastgiri et al. 2006). Food insecurity by itself can disrupt the immune system function and increase susceptibility to infection (Seligman and Berkowitz 2019; Weiser et al. 2011).
There are several major strengths in the present study. First, this case–control study examined the relationship between food insecurity and COVID-19 for the first time in Iran. Second, compared with cross-sectional studies, this study makes it possible to compare COVID-19-infected and uninfected individuals in a case–control design. Third, this study provided a fairly comprehensive review of participants' socioeconomic information and allowed them to be compared. However, our study had some limitations, including a relatively small sample and the risk of dishonesty in completing the questionnaires.
Conclusion
In general, this case–control study has shown that the risk of COVID-19 was positively associated with food insecurity and poor economic level, even after controlling for potential confounders. Further prospective studies with larger sample sizes are needed to confirm our findings and increase our understanding of the association of food security and socioeconomic status with COVID-19.
Data availability
The datasets that were used and/or analyzed during the current study are available from the corresponding author on a reasonable request.
References
Aibibula W, Cox J, Hamelin A-M, McLinden T, Klein MB, Brassard P (2017) Association between food insecurity and HIV viral suppression: a systematic review and meta-analysis. AIDS Behav 21(3):754–765. https://doi.org/10.1007/s10461-016-1605-5
Alimoradi Z, Kazemi F, Estaki T, Mirmiran P (2015) Household food security in Iran: a systematic review of Iranian articles. Adv Nurs Midwifery-SBMU J 24(87):63–76 Available from: https://journals.sbmu.ac.ir/en-jnm/article/view/9103
Ariya M, Karimi J, Abolghasemi S, Hematdar Z, Naghizadeh MM, Moradi M et al (2021) Food insecurity arises the likelihood of hospitalization in patients with COVID-19. Sci Rep 11(1):1–9. https://doi.org/10.1038/s41598-021-99610-4
Asadi-Lari M et al (2019) Socio-economic risk factors of household food insecurity and their population attributable risk: A population-based study. Med J Islam Repub Iran 33:119. https://doi.org/10.34171/mjiri.33.119
Bhattacharya J, Currie J, Haider S (2004) Poverty, food insecurity, and nutritional outcomes in children and adults. Health Econ J 23(4):839–862. https://doi.org/10.1016/j.jhealeco.2003.12.008
Bickel G, Nord M, Price C, Hamilton W, Cook J (2006) Guide to measuring household food security. Dep Agric Food Nutrition Service 6(3):52–72
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y et al (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223):507–513. https://doi.org/10.1016/S0140-6736(20)30211-7
Daneshi-Maskooni M, Sakineh S-B, Badri-Fariman M, Erfan A, Mohammadi Y, Jafarnejad S, Djafarian K (2017) Questionnaire-based prevalence of food insecurity in Iran: a review article. Iran J Public Health 46(11):1454
Dastgiri S, Mahboob S, Tutunchi H, Ostadrahimi A (2006) Determinants of food insecurity: a cross–sectional study in Tabriz. J Ardabil Univ Med Sci 6(3):233–239
Deschasaux-Tanguy M et al (2021) Nutritional risk factors for SARS-CoV-2 infection: a prospective study within the NutriNet-Santé cohort. BMC 19(1):1–18. https://doi.org/10.1186/s12916-021-02168-1
Dorosty AR (2016) Food insecurity and chronic diseases: the editorial. Nutrition Food Sci Res 3(3):1–2
Ecob R, Smith GD (1999) Income and health: what is the nature of the relationship? Social Sci Med J 48(5):693–705. https://doi.org/10.1016/S0277-9536(98)00385-2
Escobar M, Mendez AD, Encinas MR, Villagomez S, Wojcicki JM (2021) High food insecurity in Latinx families and associated COVID-19 infection in the Greater Bay Area, California. BMC Nutrition 7(1):1–9. https://doi.org/10.1186/s40795-021-00419-1
Ezzeddin N, Eini-Zinab H, Kalantari N, Ahmadi M, Beheshti Z (2022) Fear of COVID-19 Higher among Food-Insecure Households: a Model-Based Study, Mediated by Perceived Stress among Iranian Populations. Iran J Psychiatry 17(4):401–410
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223):497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
Kalantari N, Ezzeddin N, Eini-Zinab H (2021) Household Food Insecurity Scores are higher among adults infected with COVID-19: a cross-sectional online study among an Iranian population. J Environ Health Sustain 6(4):1449–1458. https://doi.org/10.18502/jehsd.v6i4.8151
Kelly JD et al (2018) Food insecurity as a risk factor for outcomes related to ebola virus disease in Kono District, Sierra Leone: a cross-sectional study. Am J Trop Med Hyg 98(5):1484. https://doi.org/10.4269/ajtmh.17-0820
Kimani ME, Sarr M, Cuffee Y, Liu C, Webster NS (2021) Associations of race/ethnicity and food insecurity with COVID-19 infection rates across US counties. JAMA Netw Open 4(6):e2112852. https://doi.org/10.1001/jamanetworkopen.2021.12852
Leddy AM, Weiser SD, Palar K, Seligman H (2020) A conceptual model for understanding the rapid COVID-19 related increase in food insecurity and its impact on health and healthcare. Am J Clin Nutr 112(5):1162–1169. https://doi.org/10.1093/ajcn/nqaa226
Li J, Huang DQ, Zou B, Yang H, Hui WZ, Rui F, Yee NT, Liu C, Nerurkar SN, Kai JC, Teng ML (2021) Epidemiology of COVID-19: a systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J Med Virol 93(3):1449–1458. https://doi.org/10.1002/jmv.26424
Mohseni H, Amini S, Abiri B, Kalantar M, Kaydani M, Barati B, Pirabbasi E, Bahrami F (2021) Are history of dietary intake and food habits of patients with clinical symptoms of COVID 19 different from healthy controls? a case–control study. Clin Nutr ESPEN 42:280–285. https://doi.org/10.1016/j.clnesp.2021.01.021
Mouliou DS, Kotsiou OS, Gourgoulianis KI (2021) Estimates of COVID-19 risk factors among social strata and predictors for a vulnerability to the infection. Int J Environ Res Public Health 18(16):8701. https://doi.org/10.3390/ijerph18168701
Organization A (2001) Handbook for Defining and Setting Up a Food Security Information and Early Warning System (FSIEWS): Food & Agriculture Org
Peng W, Berry EM (2019) The concept of food security. Encyclopedia Food Secur Sustainabil 2(1):1–7
Ramesh T, Dorosty Motlagh A, Abdollahi M (2010) Prevalence of household food insecurity in the City of Shiraz and its association with socio-economic and demographic factors, 2008. Iranian J Nutrition Sci Food Technol 4(4):53–64
Seligman HK, Berkowitz SA (2019) Aligning programs and policies to support food security and public health goals in the United States. Annu Rev Public Health 40:319. https://doi.org/10.1146/annurev-publhealth-040218-044132
Shaw DJ (2007) World food security: a history since 1945. Palgrave Macmilla J
Suardi C, Cazzaniga E, Graci S, Dongo D, Palestini P (2021) Link between viral infections, immune system, inflammation and diet. Int J Environ Res Public Health 18(5):2455. https://doi.org/10.3390/ijerph18052455
Taylor RW, Jones IE, Williams SM, Goulding A (2000) Evaluation of waist circumference, waist-to-hip ratio, and the conicity index as screening tools for high trunk fat mass, as measured by dual-energy X-ray absorptiometry, in children aged 3–19 y. Am J Clin Nutr 72(2):490–495. https://doi.org/10.1093/ajcn/72.2.490
Verity R et al (2020) Estimates of the severity of coronavirus disease 2019: a model-based analysis. Lancet Infect Dis 20(6):669–677. https://doi.org/10.1016/S1473-3099(20)30243-7
Wang D et al (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. J Am Med Assoc 323(11):1061–1069. https://doi.org/10.1001/jama.2020.1585
Weigel MM, Armijos RX, Hall YP, Ramirez Y, Orozco R (2007) The household food insecurity and health outcomes of US–Mexico border migrant and seasonal farmworkers. J Immigr Minor Health 9(3):157–169. https://doi.org/10.1007/s10903-006-9026-6
Weiser SD, Young SL, Cohen CR, Kushel MB, Tsai AC, Tien PC et al (2011) Conceptual framework for understanding the bidirectional links between food insecurity and HIV/AIDS. Am J Clin Nutr 94(6):1729S–1739S. https://doi.org/10.3945/ajcn.111.012070
Wolfson JA, Leung CW (2020) Food insecurity during COVID-19: an acute crisis with long-term health implications. Am Public Health Assoc. p. 1763-5. https://doi.org/10.2105/AJPH.2020.305953
Zhu N, Zhang D, Wang W, Li X, Yang B, Song J et al (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 382(8):727–733. https://doi.org/10.1056/NEJMoa2001017
Acknowledgements
The authors are grateful for the support of Tabriz University of Medical Sciences and all subjects who participated in the study.
Funding
The present study was based on an MSc thesis in Nutrition Sciences by S. Badri-Fariman and supported by a grant from the Vice-Chancellor for Research of Tabriz University of Medical Sciences (grant number [Pazhoohan Code]: 66519).
Author information
Authors and Affiliations
Contributions
SBF, MDM, and BPG designed and developed the study, verified the analytical methods, and contributed to statistical interpretations. SBF and MBF contributed to data collection and measurements. All authors discussed the results, contributed to the manuscript, and reviewed, revised, read, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical consideration and approval
The protocol of the study was approved by the Medical Ethics Committee at the Tabriz University of Medical Sciences (Registration No.: IR.TBZMED-REC.1399.1053). All stages of this research were performed according to the tenets of the Helsinki Declaration.
Ethical statement
The authors declare that this manuscript has been submitted to the Journal of Public Health only and that they accept all ethical statements of the journal.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Badri-Fariman, S., Daneshi-Maskooni, M., Badri-Fariman, M. et al. The association between food insecurity status and COVID-19 in an Iranian population: a case–control study. J Public Health (Berl.) 32, 865–871 (2024). https://doi.org/10.1007/s10389-023-01867-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-023-01867-8