
Abstract
Aim
Alcohol-related illnesses represent a major burden and challenge to families and pose health risks for all involved. Therefore, health promotion attempts need to focus on these vulnerable families and identify effective interventions. A systematic review was conducted of approaches to health promotion and prevention and their effectiveness for families with addiction concerns. The review focused on parental alcohol dependency.
Subject and methods
A systematic search of relevant databases was conducted, followed by a multistep screening process and a narrative synthesis of results.
Results
A total of 20 studies were included that evaluated 14 intervention programmes. The main target group was children with any form of fetal alcohol spectrum disorders and their caregivers. The study sample was dominated by behavioural approaches. The evidence base was heterogeneous. There was limited evidence of the effectiveness of combined counselling and coaching interventions that aimed to strengthen psychosocial resources.
Conclusion
The robustness of the results is limited by the moderate methodological quality of the studies. Because of the search strategy, which focused on studies with outcomes for parents with alcohol dependence, and the systematic review methodology, almost all studies reviewed featured behavioural prevention interventions. Very few studies provided specific information on the effectiveness of interventions for alcohol-dependent parents with a focus on environmental changes. The selected approach provided a limited mapping of the field of interest. However, these review findings provide the foundation for an evidence-based approach to health promotion for families with parental alcohol dependence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Alcohol consumption is a very important global issue. The transitions from rather low alcohol consumption, which has few health implications, to manifest alcohol dependence are difficult to define. This is reflected in the use of numerous terms to describe alcohol dependence, which include alcohol use disorders, alcohol abuse/dependence/addiction, and the generic term alcoholism (NIAAA 2020).
Global alcohol consumption has increased by 70% since 1990 (WHO 2021). The global average in 2019 was 5.8 litres of pure alcohol per capita (WHO 2021). Alcohol consumption reduces life expectancy, increases the risk of accidents, and increases the propensity to violence (WHO 2018). Approximately 3 million people worldwide die each year because of alcohol consumption, and nearly 1 in 20 deaths can be attributed to alcohol (WHO 2021). Serious long-term health consequences of alcohol consumption include mental illness (depression, anxiety); damage to the liver, heart, and pancreas; and an increased risk of various types of cancer (WHO 2018). The social and economic damage caused by alcohol consumption are no less serious (John et al. 2020). Short-term alcohol-related problems include mistakes at work; long-term consequences include social decline, job loss, and family breakup (John et al. 2020).
Alcohol consumption in pregnant women can have serious health consequences for the unborn child (Dejong et al. 2019; NIAAA 2017). The terminology of alcohol-related health impairments sometimes overlaps, for example, fetal alcohol syndrome (FAS), partial FAS, fetal alcohol effects, alcohol-related birth defects, and fetal alcohol spectrum disorders (FASD) (Dejong et al. 2019; NIAAA 2017; Warren et al. 2011). Studies have identified consistently high alcohol use in some pregnant women and women of childbearing age, underscoring the need for effective prevention strategies and interventions (Warren et al. 2011).
Preventing addiction is a priority in strategies to prevent excessive alcohol consumption; interventions to reduce risky alcohol consumption and to protect the health of uninvolved third parties are particularly important (WHO 2018). There is a need for health promotion/prevention strategies for alcohol-dependent people to address the effects of addiction on families. Parental alcohol addiction affects not only family life and parental health, but also the health of children and partners (Family First Intervention 2016). Therefore, close relatives of addicted individuals have a substantial need for support because they live in a stressful environment. An important general goal is cooperation between the various actors in health promotion and prevention, with a focus on strengthening the entire family (Laging 2018). One important approach is the so-called think-family interventions, also known as ‘family paediatrics’, ‘whole-family’, or ‘family-centred’ approaches or ‘child-centred’ approaches within adult services (Woodman et al. 2020). They address parental mental health, substance and alcohol misuse, and/or domestic violence (Woodman et al. 2020). Behavioural prevention alone has limited effectiveness; a combination of behavioural and environmental prevention is more effective (John et al. 2020). That is why ‘think-family’ interventions combine screening, health promotion, and developing relationships (Woodman et al. 2020). Another systematic review by Bischof et al. (2019) concluded that the effectiveness of family-based support in the field of addiction has been well documented. At the same time, there is a need to evaluate the effectiveness and efficacy of the extensive prevention and intervention services for alcohol abusers (NIAAA 2017). Existing reviews often focused on several alcohol prevention programmes for children and/or adolescents (e.g., Cho and Cho 2021), on parent-related interventions and programmes on reducing/preventing adolescent substance use (tobacco, alcohol, drugs) (e.g., Allen et al. 2016; Hurley et al. 2019), or on any kind of family-based prevention programmes for preventing alcohol use in young people up to 18 years of age (e.g., Gilligan et al. 2019). Even more reviews have a wider range, and address multiple risk factors among children (e.g., MacArthur et al. 2018). The results of these studies show no clear benefits of the programmes. The realist review from Usher et al. (2015) highlighted supportive peer relationships, knowledge, and encouragement of positive parent–child interactions as effective factors of family-based interventions for children of substance-abusing parents (alcohol or drugs). At the same time, the authors noted ‘significant gaps in the level of evaluation’.
The present review aimed to address a gap in the literature. It provides the systematic findings that so far have been missing regarding the effectiveness of health promotion or health-related prevention measures and interventions for families with alcohol addiction problems of parents. The following research questions were addressed:
What national and international studies have been conducted on health promotion and prevention approaches in families with parental problems with alcohol addiction?
What is the evidence regarding the effectiveness of the interventions?
Methods
To answer the research questions, a systematic review was conducted as part of the research project 01EL2021 funded by the German Federal Ministry of Education and Research. More information for the whole study can be found in the study protocol (Geene et al. 2021).
A systematic search was carried out of the following databases in July 2020: Cochrane Database, LIVIVO (including BASE, TIB, Publishing Data, and SOMED), PubMed, Scopus, EBSCOhost (including APA PsycInfo, Psychology and Behavioural Science Collection, SocINDEX, ERIC, and PSYNDEX), and PubPsych (including Pascal and Narcis). In addition, the reference lists of the included studies were searched for additional relevant publications (‘citation tracking’). The search strategy contained combinations of keywords describing the intervention and target groups. See the given example from Cochrane (Table 1).
The study selection process was carried out using defined inclusion and exclusion criteria (Table 2) using the software program Covidence [Covidence systematic review software (online) n.d.], which supports the conducting of systematic reviews. Screening, data extraction, and quality assessment were performed by two reviewers in parallel and independently. The review software detected clear duplicates during file import. The reviewers identified further duplicates in the screening process.
The methodological quality of the quantitative studies was assessed using the Effective Public Healthcare Panacea Project (EPHPP) assessment tool (2020). Data extraction was performed using a deductively formulated and inductively refined data collection form. To systematize the evidence on effectiveness and to analyse this evidence, eight outcome categories were defined and the outcomes from the included studies were thematically assigned to these categories (Table 3).
Results
General findings
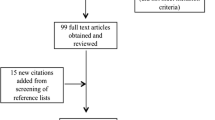
The review identified 499 publications (Fig. 1). At the end of the multistep screening process, 20 publications remained that examined 14 different interventions. Randomized controlled trials were the main design, followed by three before-and-after studies and three non-randomized controlled trials (Table 3). These and further details of the quantitative studies (n = 14) can be found in Table 3, which summarizes the findings. Three systematic reviews (Krahn et al. 2018; Reid et al. 2015; Templeton et al. 2010) and two qualitative studies were also included to complete the body of research (Gibbs 2019; Nordenfors and Höjer 2017). Most of the studies were carried out in the USA (n = 8).

Flowchart for study selection based on the PRISMA flow diagram (Moher et al. 2009)
In the methodological evaluation using the EPHPP (2020), three of the 14 quantitative studies achieved an overall rating of moderate, indicating a medium risk of bias (Table 3). The remaining studies showed a high risk of bias (Table 3). The qualitative studies (Gibbs 2019; Nordenfors and Höjer 2017) had shortcomings in the discussion of methods, disclosure of limitations, and ethical and privacy considerations. The following results section focuses on the quantitative studies identified by the review.
Characteristics of included interventions
The primary study target groups were children with any form of FASD or prenatal alcohol disposition, their custodians, and persons close to those addicted to alcohol (these individuals were referred to in the studies as ‘concerned significant others’ or CSOs). CSOs included children, domestic partners, other close relatives (e.g., grandparents), and friends. Parents and/or pregnant women with alcohol problems were the focus of three studies (Nordenfors and Höjer 2017; Schaeffer et al. 2013; Slesnick and Erdem 2012). The survey by Chersich et al. (2012) is noteworthy because the prevention campaign addressed mothers with newborns (with and without substance dependence), women of childbearing age, and the general population.
The interventions examined in the included studies were conducted over an average period of 5 weeks to 6 months. Exceptions were the prevention campaign in the Chersich et al. study (2012), which lasted over a year, and an intervention from Sweden that included support from pregnancy to up to 6 months after birth (Nordenfors and Höjer 2017).
Individual counselling services, mostly as a subcomponent of programmes (Bischof et al. 2016; Chersich et al. 2012; Eék et al. 2020; Gustafson et al. 2012; Leenaars et al. 2012; Nordenfors and Höjer 2017; Petrenko et al. 2019; Petrenko et al. 2017; Schaeffer et al. 2013; Slesnick and Erdem 2012), and (individual) coaching or therapeutic approaches (Chersich et al. 2012; Coles et al. 2015; Gustafson et al. 2012; Kable et al. 2016; Leenaars et al. 2012; Nash et al. 2015; Schaeffer et al. 2013; Slesnick and Erdem 2012) were represented the most. Both group (Gibbs 2019; Kable et al. 2016; Keil et al. 2010; Petrenko et al. 2019; Petrenko et al. 2017; Schaeffer et al. 2013; Son and Choi 2010) and online interventions (Eék et al. 2020; Gustafson et al. 2012; Kable et al. 2012) were examined. In terms of content, the focus was often on dealing with the consequences and effects of FASD. This was accompanied by approaches to resource strengthening and skills development in the form of behavioural and communication training, stress and emergency management, and social skills training. Environmental prevention approaches featured as subcomponents in interventions that used an advocacy approach (Gibbs 2019; Leenaars et al. 2012; Nordenfors and Höjer 2017; Slesnick and Erdem 2012). Six interventions were mainly aimed at expanding the social network of the target group and improving the networking of existing services (Gustafson et al. 2012; Kable et al. 2012; Leenaars et al. 2012; Nordenfors and Höjer 2017; Petrenko et al. 2019; Petrenko et al. 2017; Slesnick and Erdem 2012). The Housing First model additionally focused on the temporary provision of housing and employment assistance (Slesnick and Erdem 2012).
Evaluation of outcome categories
Grouping the outcomes from the included studies resulted in a thematic systematization consisting of eight categories. The study outcomes were assigned to these categories during the evaluation process (Table 3). The results for the effectiveness of the included interventions are grouped thematically according to category.
-
1.
Mental health and well-being
In this outcome category, CSOs tended to show improvements in depressive symptoms and stress, and reductions in distress and feelings of anger, loneliness, and anxiety (Bischof et al. 2016; Eék et al. 2020; Gustafson et al. 2012; Leenaars et al. 2012; Schaeffer et al. 2013; Son and Choi 2010). A family training and coaching programme (Leenaars et al. 2012) and an anger management programme (Son and Choi 2010) generated positive significant results. Alcohol abusers experienced short-term reductions in depressive symptoms (Schaeffer et al. 2013; Slesnick and Erdem 2012). The multicomponent Families on Track intervention generated improvements in self-care and self-efficacy among caregivers of children with FASD (Petrenko et al. 2019; Petrenko et al. 2017).
-
2.
Promotion of health and health behaviours in children with FASD
Studies in the second outcome category demonstrated positive effects on behaviour, reductions in behavioural problems, and improved emotional control in children with FASD (Coles et al. 2015; Kable et al. 2012, 2016; Keil et al. 2010; Petrenko et al. 2019; Petrenko et al. 2017; Slesnick and Erdem 2012). In particular, the frequency of anger episodes and frustration levels were significantly reduced by the GoFar®, a combined intervention comprising parent training, behavioural therapy, and a computer game for children (Kable et al. 2016).
-
3.
Compliance of addicted persons
In this category, a combination of three therapeutic approaches (Multisystemic Therapy–Building Stronger Families, MST-BSF) achieved a significant reduction in relapse rate and frequency of child abuse under the influence of alcohol (Schaeffer et al. 2013). Furthermore, the CRAFT (Community Reinforcement and Family Training) programme, which comprised coaching sessions and behavioural therapy for family members, positively affected treatment adherence among addicted individuals (Bischof et al. 2016). In contrast, the Internet-based iCRAFT had no significant effect on alcohol treatment initiation (Eék et al. 2020). Alcohol consumption was significantly (Schaeffer et al. 2013; Slesnick and Erdem 2012) to slightly reduced in some studies (Bischof et al. 2016; Chersich et al. 2012; Eék et al. 2020).
-
4.
Social relationships
Outcomes in this domain were heterogeneous. Studies described significant to non-significant improvements in family cohesion (Leenaars et al. 2012), partnerships (Bischof et al. 2016; Eék et al. 2020; Gustafson et al. 2012; Leenaars et al. 2012; Slesnick and Erdem 2012), social support (Leenaars et al. 2012), and various family needs (Petrenko et al. 2019, 2017).
-
5.
Other
Four categories are summarized here owing to their low frequency. In the social living situation category, three interventions achieved significant improvements in housing (Leenaars et al. 2012; Schaeffer et al. 2013; Slesnick and Erdem 2012). The Housing First model did not contribute to long-term stabilization of employment (Slesnick and Erdem 2012). Other studies provided evidence of programme effectiveness in the areas of knowledge levels (Chersich et al. 2012; Kable et al. 2012; Petrenko et al. 2019, 2017) and parenting skills (Leenaars et al. 2012; Petrenko et al. 2019, 2017; Schaeffer et al. 2013). A FASD information campaign achieved a significant reduction in FASD prevalence (Chersich et al. 2012).
Discussion
This systematic review included 20 studies that examined 14 intervention programmes. The results presented here are focused on the quantitative studies (Table 3). Individual counselling and coaching services combined with behavioural therapy approaches appear promising, although the robustness of the results is compromised by methodological weaknesses and a predominantly behavioural preventive orientation.
A family training and coaching programme (Leenaars et al. 2012) and a combined approach using various therapies (Schaeffer et al. 2013) demonstrated significant improvements in all assessed outcomes (Table 3). Usher et al. (2015) also concluded the parent–child interaction, knowledge, and support from peers are key factors for the effectiveness of family-based intervention programmes (Usher et al. 2015). It should be noted that all the interventions considered here tended to positively, albeit not always significantly, improve individual outcomes (Table 3). This is consistent with the conclusion from a review by Templeton et al. (2010) that there is no ‘best’ intervention for family members living with alcohol abuse. But other reviews also concluded that the engagement of parents and the community is necessary (Cho and Cho 2021). Moreover, the GoFAR® was the only reviewed intervention that provided joint exercises and sessions for addicted individuals and family members (Coles et al. 2015; Kable et al. 2016). Although there is a substantial call for holistic and multilevel approaches for affected families (Cho and Cho 2021), this is not reflected much in the health promotion programmes included here. This review confirmed the inadequacy of target group-specific prevention programmes for the whole family.
The present data were dominated by FAS/FASD, a serious consequence of maternal alcohol consumption during pregnancy, even though this was not directly addressed by the search strategy. Interventions targeting this problem were deliberately included in this review to reflect the range of interventions for this vulnerable group in the context of family health promotion. However, this vulnerable group was not explicitly considered in the search strategy. This should be seen as a limitation regarding the completeness of the evidence base and should be addressed in further reviews. Alcohol-related harm to the child cannot be cured but it can be mitigated through targeted support. Behavioural preventive approaches may reduce deficits in the target group and thus enable them to experience better (participation) opportunities in everyday life, at school, or at work. Reid et al. (2015) report that there is increasing evidence for the effectiveness of interventions that improve outcomes in children with FASD in early to middle childhood. However, they point out the lack of interventions for adolescents and young adults. The present findings provide no evidence regarding this point, as the review targeted interventions with a specific family focus and excluded programmes that focused only on children or adolescents.
To improve the living conditions of families with addiction problems while simultaneously ensuring the use of health-promoting services and reducing barriers, low-threshold support services for daily coping, such as driving services or the provision of childcare, are needed (Warren et al. 2011). However, the available data are dominated by interventions for individual competence development, resource strengthening, and counselling. Support to improve the living circumstances of families, the provision of housing and support for employment, childcare (Slesnick and Erdem 2012), referral to other assistance services (Gustafson et al. 2012; Kable et al. 2012; Leenaars et al. 2012; Petrenko et al. 2019, 2017; Reid et al. 2015; Slesnick and Erdem 2012), and advocacy (Gibbs 2019; Leenaars et al. 2012; Nordenfors and Höjer 2017; Slesnick and Erdem 2012) was provided, but mainly only as part of the programmes. More action should be undertaken in realizing ‘family-centred’ approaches (‘Think-Family’), as Woodman et al. (2020) mentioned. The review by Krahn et al. (2018) concluded that case management combined with housing placement was most effective for homeless pregnant women and young mothers with alcohol dependence. Only the study by Chersich et al. (2012) featured an information campaign that included public information strategies (discussion rounds, advertising, information booths) for the general population and for women in particular.
Overall, the evidence base provided here is ambiguous. These findings are hard to compare with other reviews, though no existing review addresses the same research question in this way. The above-mentioned reviews either focus on various addiction problems or address only children or parents. Nevertheless, they show some ambiguous evidence while at the same time pointing out the need for further research with high quality (Allen et al. 2016; Gilligan et al. 2019; Hurley et al. 2019; MacArthur et al. 2018). The methodological weaknesses were already highlighted as study limitations in other reviews and resulted in asking for improvement of study quality in further research (Allen et al. 2016; Hurley et al. 2019; MacArthur et al. 2018). This review underlines these findings and the requirements.
A limitation of the present study is the small study sample that reflected the stringent inclusion and exclusion criteria. Additionally, the systematic research methodology was insufficient to represent the complex field of health promotion and prevention for this vulnerable group of families coping with alcohol addiction. Many existing programmes address not only the problem of alcohol dependence, but also tobacco addiction, other substance use disorders (e.g., illegal drugs), or so-called multiple-risk behaviours, which often occur in combination. Additionally, these programmes often focus on a predefined group or setting, such as young people or universal school-based interventions (Cho and Cho 2021; MacArthur et al. 2018). Such programmes were not considered in this review. The focus on alcohol addiction in the family setting, especially among parents, led to selection bias. In addition, it was difficult to identify evaluated health-promoting programmes that addressed the whole family and were not medical interventions in a clinical setting (e.g., rehabilitation clinics). A relatively broad definition of ‘family’ was used to include interventions involving partnerships (with and without children) in the review.
The strengths of the review are its timeliness, the identification of inconsistent findings, the transparent and rule-based process, and the reproducibility of the search strategy and screening process. The specific and comprehensive inclusion and exclusion criteria enabled the generation of a database in a clearly defined field of family health promotion with reference to a highly vulnerable target group.
Conclusion
The systematic analysis and evaluation of the diverse programmes and interventions identified is an important first step in determining the effectiveness of targeted prevention measures for families with parental alcohol problems. The data presented could provide a foundation for evidence-based health promotion and prevention for families with alcohol problems. These findings identify interventions that are effective for the target group in some reported outcomes. The findings demonstrate the need for further evaluations of existing interventions in this area and for high-quality studies. Finally, it underlines the need for holistic ‘think-family’ approaches, especially for the families with alcohol problems that are the primary focus of this study.
Data availability
The data used and/or analysed during the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable
Abbreviations
- CSO:
-
Concerned significant other
- EPHPP:
-
Effective Public Healthcare Panacea Project
- FAS:
-
Fetal alcohol syndrome
- FASD:
-
Fetal alcohol spectrum disorders
- NIAAA:
-
National Institute on Alcohol Abuse and Alcoholism
- WHO:
-
World Health Organization
References
Allen ML, Garcia-Huidobro D, Porta C, Curran D, Patel R, Miller J, Borowsky I (2016) Effective Parenting Interventions to Reduce Youth Substance Use: A Systematic Review. Pediatrics 138. https://doi.org/10.1542/peds.2015-4425
Bischof G, Iwen J, Freyer-Adam J, Rumpf H-J (2016) Efficacy of the community reinforcement and family training for concerned significant others of treatment-refusing individuals with alcohol dependence: A randomized controlled trial. Drug Alcohol Depend 163:179–185. https://doi.org/10.1016/j.drugalcdep.2016.04.015
Bischof G, Trachte A, Krüger JH, Brandt D, Bischof A, Rumpf HJ (2019) Wirksamkeit angehörigenbasierter Interventionen im Suchtbereich: Ergebnisse eines systematischen Reviews. Suchttherapie 20:S14–S04. https://doi.org/10.1055/s-0039-1696136
Chersich MF, Urban M, Olivier L, Davies L-A, Chetty C, Viljoen DJA (2012) Universal prevention is associated with lower prevalence of fetal alcohol spectrum disorders in Northern Cape, South Africa: a multicentre before–after study. Alcohol Alcohol 47:67–74. https://doi.org/10.1093/alcalc/agr145
Cho MK, Cho YH (2021) Do Alcohol Prevention Programs Influence Adolescents' Drinking Behaviors? A Systematic Review and Meta-Analysis. Int J Environ Res Public Health 18. https://doi.org/10.3390/ijerph18168524
Coles CD, Kable JA, Taddeo E, Strickland DC (2015) A metacognitive strategy for reducing disruptive behavior in children with fetal alcohol spectrum disorders: goFAR pilot. Alcohol Clin Exp Res 39:2224–2233. https://doi.org/10.1111/acer.12885
Covidence systematic review software (online) (n.d.) Melbourne, Australia: Veritas Health Innovation. Available: www.covidence.org [Accessed 22.05.2022]
Dejong K, Olyaei A, Lo JO (2019) Alcohol Use in Pregnancy. Clin Obstet Gynecol 62:142–155. https://doi.org/10.1097/GRF.0000000000000414
Eék N, Romberg K, Siljeholm O, Johansson M, Andreasson S, Lundgren T, Fahlke C, Ingesson S, Bäckman L, Hammarberg A (2020) Efficacy of an Internet-Based Community Reinforcement and Family Training Program to Increase Treatment Engagement for AUD and to Improve Psychiatric Health for CSOs: A Randomized Controlled Trial. Alcohol Alcoholism (Oxford, Oxfordshire) 55:187–195. https://doi.org/10.1093/alcalc/agz095
EPHPP - Effective public healthcare panacea project (2020) Effective Public Healthcare Panacea Project: Independent source of information about health care in Canada. Quality Assessment Tool for Quantitative Studies. [Online]. online. Available: https://www.ephpp.ca/quality-assessment-tool-for-quantitative-studies/ [Accessed 20.11.2020]
Family First Intervention (2016) Understanding alcoholism within families [Online]. Available: https://family-intervention.com/blog/understanding-alcoholism-within-families/ [Accessed 08.03.2022]
Geene R, Kuschick D, Kuck J, Rattay P, Pachanov A (2021) Studienprotokoll zum Projekt: “Literaturrecherche und Evidenzauswertung von Ansätzen zur Gesundheitsförderung bei sozial belasteten Familien (LEFaG)”. https://nbn-resolving.org/urn:nbn:de:kobv:b1533-opus-3732
Gibbs A (2019) An evidence-based training and support course for caregivers of children with foetal alcohol spectrum disorder (FASD) in New Zealand. Adv Dual Diagn 12:73–84. https://doi.org/10.1108/ADD-10-2018-0013
Gilligan C, Wolfenden L, Foxcroft DR, Williams AJ, Kingsland M, Hodder RK, Stockings E, Mcfadyen TR, Tindall J, Sherker S, Rae J, Wiggers J (2019) Family-based prevention programmes for alcohol use in young people. Cochrane Database System Rev 3:Cd012287. https://doi.org/10.1002/14651858.CD012287.pub2
Gustafson DH, Mctavish FM, Schubert CJ, Johnson RA (2012) The effect of a computer-based intervention on adult children of alcoholics. J Addict Med 6:24–28. https://doi.org/10.1097/ADM.0b013e31822b80ca
Hurley E, Dietrich T, Rundle-Thiele S (2019) A systematic review of parent based programs to prevent or reduce alcohol consumption in adolescents. BMC Public Health 19:1451. https://doi.org/10.1186/s12889-019-7733-x
John U, Meyer C, Baumann S, Rumpf H-J, Freyer-Adam J (2020) Alkoholkonsum – Bedeutung für Prävention und Gesundheitsförderung. In: Tiemann M, Mohokum M (eds) Prävention und Gesundheitsförderung. Springer Berlin Heidelberg, Berlin
Kable JA, Coles CD, Strickland D, Taddeo E (2012) Comparing the Effectiveness of On-Line versus In-Person Caregiver Education and Training for Behavioral Regulation in Families of Children with FASD. Int J Ment Heal Addict 10:791–803. https://doi.org/10.1007/s11469-012-9376-3
Kable JA, Taddeo E, Strickland D, Coles CD (2016) Improving FASD Children's Self-Regulation: Piloting Phase 1 of the GoFAR Intervention. Child Fam Behav Ther 38:124–141. https://doi.org/10.1080/07317107.2016.1172880
Keil V, Paley B, Frankel F, O´Connor MJ (2010) Impact of a Social Skills Intervention on the Hostile Attributions of Children With Prenatal Alcohol Exposure. Alcohol Clin Exp Res 34(2):231-241.
Krahn J, Caine V, Chaw-Kant J, Singh AE (2018) Housing interventions for homeless, pregnant/parenting women with addictions: a systematic review. J Soc Distress Homeless 27:75–88. https://doi.org/10.1080/10530789.2018.1442186
Laging M (2018) Soziale Arbeit in der Suchthilfe, 70565 Stuttgart. W. Kohlhammer Verlag
Leenaars LS, Denys K, Henneveld D, Rasmussen C (2012) The impact of fetal alcohol spectrum disorders on families: Evaluation of a family intervention program. Community Ment Health J 48:431–435. https://doi.org/10.1007/s10597-011-9425-6
Macarthur G, Caldwell DM, Redmore J, Watkins SH, Kipping R, White J, Chittleborough C, Langford R, Er V, Lingam R, Pasch K, Gunnell D, Hickman M, Campbell R (2018) Individual-, family-, and school-level interventions targeting multiple risk behaviours in young people. Cochrane Database System Rev 10:Cd009927. https://doi.org/10.1002/14651858.CD009927.pub2
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Nash K, Stevens S, Greenbaum R, Weiner J, Koren G, Rovet J (2015) Improving executive functioning in children with fetal alcohol spectrum disorders. Child Neuropsychol 21(2):191–209. https://doi.org/10.1080/09297049.2014.889110
NIAAA (2017) Strategic plan 2017-2021 [Online]. National Institute on Alcohol Abuse and Alcoholism Available: https://www.niaaa.nih.gov/sites/default/files/StrategicPlan_NIAAA_optimized_2017-2020.pdf [Accessed 11.10.2021]
NIAAA (2020) Understanding alcohol use disorder [Online]. National Institute on Alcohol Abuse and Alcoholism. Available: https://www.niaaa.nih.gov/sites/default/files/publications/Alcohol_Use_Disorder_0.pdf [Accessed 22.09.2021]
Nordenfors M, Höjer I (2017) Mothers with substance and alcohol abuse—support through pregnancy and early infancy. Soc Work Health Care 56:381–399. https://doi.org/10.1080/00981389.2017.1299072
Petrenko CLM, Pandolfino ME, Robinson LK (2017) Findings from the Families on Track Intervention Pilot Trial for Children with Fetal Alcohol Spectrum Disorders and Their Families. Alcohol Clin Exp Res 41:1340–1351. https://doi.org/10.1111/acer.13408
Petrenko CLM, Demeusy EM, Alto ME (2019) Six-Month Follow-up of the Families on Track Intervention Pilot Trial for Children With Fetal Alcohol Spectrum Disorders and Their Families. Alcohol Clin Exp Res 43:2242–2254. https://doi.org/10.1111/acer.14180
Reid N, Dawe S, Shelton D, Harnett P, Warner J, Armstrong E, Legros K & O'callaghan F (2015) Systematic Review of Fetal Alcohol Spectrum Disorder Interventions Across the Life Span. 39:2283-2295. https://doi.org/10.1111/acer.12903
Schaeffer CM, Swenson CC, Tuerk EH, Henggeler SW (2013) Comprehensive treatment for co-occurring child maltreatment and parental substance abuse: outcomes from a 24-month pilot study of the MST-Building Stronger Families program. Child Abuse Negl 37:596-607. https://doi.org/10.1016/j.chiabu.2013.04.004.
Slesnick N, Erdem G (2012) Intervention for homeless, substance abusing mothers: findings from a non-randomized pilot. Behavioral Med (Washington, DC) 38:36–48. https://doi.org/10.1080/08964289.2012.657724
Son JY, Choi YJ (2010) The Effect of an Anger Management Program for Family Members of Patients With Alcohol Use Disorders. Arch Psychiatr Nurs 24:38–45. https://doi.org/10.1016/j.apnu.2009.04.002
Templeton L, Velleman R, Russell C (2010) Psychological interventions with families of alcohol misusers: A systematic review. Addict Res Theory 18:616–648. https://doi.org/10.3109/16066350903499839
Usher AM, Mcshane KE, Dwyer C (2015) A realist review of family-based interventions for children of substance abusing parents. Syst Rev 4:177. https://doi.org/10.1186/s13643-015-0158-4
Warren KR, Hewitt BG, Thomas JD (2011) Fetal alcohol spectrum disorders: research challenges and opportunities. Alcohol Res Health 34:4–14. https://pubmed.ncbi.nlm.nih.gov/23580035https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3756137/
WHO (2018) Global status report on alcohol and health 2018. Journal. https://www.who.int/publications/I/item/9789241565639 [Àccessed 08.03.2022]
WHO (2021) Länder mit dem höchsten Pro-Kopf-Alkoholkonsum unter Erwachsenen im Jahr 2019 (in Liter puren Alkohols) [Countries with the highest per capita alcohol consumption among adults in 2019 (in liters of pure alcohol)] [Online]. World Health Organization, Statista Available: https://de.statista.com/statistik/daten/studie/232485/umfrage/laender-mit-dem-hoechsten-alkoholkonsum-unter-erwachsenen/ [Accessed 11.10.2021]
Woodman J, Simon A, Hauari H, Gilbert R (2020) A scoping review of 'think-family' approaches in healthcare settings. J Public Health (Oxford, England) 42:21–37. https://doi.org/10.1093/pubmed/fdy210
Acknowledgements
We thank Diane Williams, PhD, from Edanz (https://www.edanz.com/ac) for editing a draft of this manuscript.
Funding
Open Access funding enabled and organized by Projekt DEAL. German Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung) (01EL2021)
Author information
Authors and Affiliations
Contributions
All authors were involved in the screening and selection process. All authors discussed the analysis and results. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics declaration
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kuschick, D., Kuck, J., Pachanov, A. et al. Health promotion for families with parental alcohol addiction: a systematic review. J Public Health (Berl.) 32, 1057–1067 (2024). https://doi.org/10.1007/s10389-023-01845-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-023-01845-0