
Abstract
Aim
A shortage in primary care physicians has been a well-known challenge in many Western countries for several years. In addition, we currently see a trend in primary care, where an increasing number of physicians work as employees instead of being self-employed, even among general practitioners. To address this shortage, knowledge of the future specialists’ attitudes toward working self-employed is needed. This qualitative systematic review aims to explore the attitudes of future specialists towards self-employment in private practice, and what factors influence these attitudes.
Subject and methods
We conducted a systematic search using PubMed, Embase, and Web of Science. We developed a search strategy that collected terms for future specialists, career choices, and self-employment and linked these with the Boolean operator “AND”. We analysed the results using a qualitative content analysis, as both qualitative and quantitative studies were included in the research.
Results
Self-employment is less attractive to future specialists. In particular, women prefer to be employed and receive a fixed salary. The main factors that influence the decision as to whether to become self-employed or not are financial conditions, bureaucracy and non-medical tasks, organisation, job satisfaction during residency, personal responsibility, career opportunities, specialty-dependent factors, personal environment, and education.
Conclusion
Among future specialists, being self-employed is less attractive than being an employee. Students should be better informed about future career opportunities to make an informed decision. However, it should be examined whether other forms of organisation are more in line with the wishes of future specialists.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Health systems in Europe are facing the problem of physician shortage (Berthier 2018; Mohammadiaghdam et al. 2020). Indeed it is controversial whether there is a real shortage of physicians or an allocation problem, as the number of doctors per capita has increased in most European countries over the last few years (OECD 2022a). It is a matter of fact that demographic aging and medical progress are increasing the demand for health care services, and many doctors will retire shortly (eurostat 2020). If this demand is not met through recruitment, it may lead to a real shortage of doctors in the near future (Pedersen et al. 2012). However, it could be possible that the problem does not lie in the total amount of doctors but in their distribution. Some geographical areas are experiencing an oversupply of physicians in certain specialisms, while others have a shortage. General medicine and rural areas are most affected by shortages (Behmane et al. 2019; Chevreul et al. 2015; Bachner et al. 2018; Gerkens and Merkur 2020; Habicht et al. 2018; Kroneman et al. 2016; Olejaz et al. 2012; DePietro et al. 2015; Saunes et al. 2020). Due to the ageing population, the demand for health services is increasing (Gerlach et al. 2018). Thus, by acting as a gatekeeper in many countries, general practitioners (GP) in particular will see an increasing demand in the future (Siewert et al. 2013).
In many countries in Northern and Western Europe, both GPs and other specialists have the opportunity to work self-employed. Self-employment is for example a general career option in the following countries: Austria, Belgium, Denmark, France, Germany, Ireland, Netherland, Norway, Switzerland, and the United Kingdom (Bachner et al. 2018; Gerkens and Merkur 2020; Kringos et al. 2015; Tikkanen et al. 2020). The remuneration of self-employed physicians differs. In Germany and Switzerland, for example, physicians are mainly remunerated via fee-for-service. Norway and Denmark use a mixture of capitation and fee-for-service, with a user-charge being added in Norway (Tikkanen et al. 2020). An overview on the structure of the different health care systems can be found in International Profiles of Health Care Systems from the Commonwealth Fund (Tikkanen et al. 2020).
A self-employed physician in private practice is a physician who runs their own practice, either alone or in a partnership, and is, thus, responsible for its long-term success. The physician also bears the full economic risk of their practice. A self-employed physician in private practice could be remunerated through the statutory health insurance or the national health system. They are not directly bound by instructions and are free to choose the time and place of their work, within the limits of the law (Becher 2022). In some European countries, however, restrictions exist on the choice of practice location (Nüsken and Busse 2011). These restrictions are based on demand planning, which is carried out for example in Germany by the Federal Association of Statutory Health Insurance Physicians (Kassenärztliche Bundesvereinigung (KBV) 2022a).
The proportion of self-employed physicians within the total number of physicians in Germany decreased from 37% in 2010 to 28% in 2020 (Bundesärztekammer 2011, 2021). GPs, who are mainly affected by the shortage of doctors, can work as employees or as self-employed in their own practices. Most GPs in Northern and Western Europe are self-employed in single-handed or group practices, and the proportion of group practices vs single-handed practices has increased in recent years in many countries (Gerkens and Merkur 2020; Olejaz et al. 2012; DePietro et al. 2015; Kroneman et al. 2016; Kassenärztliche Bundesvereinigung (KBV) 2022b). In France and Germany, approximately 67% of GPs were self-employed in 2020 (Tikkanen et al. 2020; Bundesärztekammer 2021). However, the proportion of GPs within the total number of physicians has decreased significantly in most countries in Northern and Western Europe (eurostat 2020). Rural areas are also severely affected by the shortage of doctors. These regions are sparsely populated and fewer patients are available in the catchment area, leading to more self-employed physicians in single-handed practices (Pedersen et al. 2012). Hence, the specialties and regions most affected by the shortage of doctors are thus those in which physicians work mainly self-employed.
The question then arises as to whether self-employment discourages future specialists. This qualitative systematic review will examine how medical students and junior physicians who have not obtained specialist registration imagine their future working conditions. Including attitudes towards self-employment in rural areas due to the physicians’ shortage. The aim of the study is to describe the attitudes of future specialists toward self-employment in Northern and Western Europe. The results can be used to form recommendations to ensure demand-oriented care.
Methods
The study was conducted as a qualitative systematic review, where the PICo framework was used to frame the literature searches. The population (P) was defined as medical students and junior doctors not yet holding specialist registration, for example resident. The interest (I) was the attitude towards self-employment including attitudes towards self-employment in rural areas. The context (Co) was Northern and Western Europe. With these aspects in mind, we developed the following research question: What attitudes do future specialists in northern and western Europe have towards self-employment and what factors influence these attitudes?
Search strategy
The search strategy consisted of three keyword blocks linked to each other with the Boolean operator “AND”. The first section dealt with the population and collected various terms for medical students and junior doctors and linked them with “OR”. We collected different terms for future specialists by checking the literature. Preliminary we used the study by Wijnen-Meijer et al. (2013) to find relevant search terms, since it describes the different processes of medical education in different countries and also presents an overview of the terminologies. The second considered keywords related to career choice. The last considered self-employment in private practice. We also collected these keywords by checking the literature. The search strategy can be found in the supplementary information.
Identification and screening of studies
We performed a systematic literature search in the PubMed, Embase, and Web of Science. Two reviewers (JM and SG) performed title/abstract screenings and full-text screenings independently. Only JM understood the German studies. In order to make a reasoned decision about these studies, the abstract had to be in English. Additionally, JM presented the contents of the German-language articles to SG. We conducted an unsystematic search alongside the systematic literature search. The reviewers checked the references of studies dealing with self-employment in private practice and searched in Google Scholar using the same keyword as in the systematic search.
Inclusion and exclusion criteria
The inclusion and exclusion criteria were determined according to PICo before screening the texts. The search only considered studies from 2011 to 2021 that were available in German, Danish, Swedish, Norwegian, or English and that had an English abstract available. Since the mind-sets of the generations change (Parment 2013) and the components of health care systems are constantly being modified, a longer period of time did not seem reasonable. Studies that did not unambiguously deal with self-employment in private practice were excluded. This led to the exclusion of descriptive studies that examined the choice of specialisation, without looking at self-employment. Both qualitative and quantitative studies on the topic of self-employment were included. The included studies had to examine the population of future specialists in countries in Northern and Western Europe. However, studies in countries where self-employment in private practice is not a general career option were excluded. This led to a possible inclusion of studies from Austria, Belgium, Denmark, France, Germany, Ireland, Netherland, Norway, Switzerland, and the United Kingdom. Systematic reviews were not included, as results should only be considered from the primary source. In addition, no quality assessment tools were used to select the studies.
Evaluation
We did a qualitative content analysis in which we compared both qualitative studies and quantitative studies. Qualitative as well as quantitative results were assigned to the categories. In conducting this qualitative content analysis, we followed recommendations of Kuckartz (2018). JM inductively formed categories while reading the studies. After reading half of the studies, JM and SG made the first summary of the categories. During further reading, the text passages and results were then assigned to these categories. If necessary, we created a new category. JM and SG further summarised the categories and generalised them as far as possible. Differences in the category summary were discussed and debated together. The category system (shown in Table 1) consists of various subcategories that have been arranged hierarchically, and represents all factors mentioned in the included studies.
Results
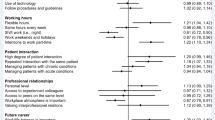
The PRISMA diagram in Fig. 1 presents the study selection process. We analysed a total of 19 full texts, 13 of which come from Germany and four others from German-speaking Switzerland. The remaining two studies are from Denmark and Norway. Eleven of the 19 studies examined the field of general medicine, while six publications conducted a survey independent from the field. These were mostly concerning medical students who had not yet chosen a specialisation. One study was from the field of rheumatology and one was related to the field of primary care. The surveys were mostly conducted via a questionnaire that used open questions. Approximately equal numbers of studies looking at medical students and residents were included. The included studies are listed in Table 2, and the results of the qualitative content analysis are presented below. An overview of all factors discussed in the following results can be found in Fig. 2.

PRISMA diagram

Influencing factors from the qualitative content analysis
Intention to work as self-employed in private practice
The intention to work as self-employed is considered in 14 of the included studies (Barth et al. 2017; Cerutti et al. 2015; Deutsch et al. 2013; Gedrose et al. 2012; Gibis et al. 2012; Gisler et al. 2017; Heinz and Jacob 2012; Pfeil et al. 2020; Roick et al. 2012; Schneider et al. 2013; Steinhäuser et al. 2013; Streit 2011; Ziegler et al. 2017; Zupanic et al. 2011). The proportion of future specialists who want to work as an employee was found to be higher than the proportion of those who want to pursue a career as a self-employed physician. A large proportion of the students surveyed stated that they found employment in a hospital very attractive. With regard to this, the results of Gibis et al. (2012) (78.1%) and Heinz and Jacob (2012) (77.3%) were similar. Surveyed students rated self-employment as a medical specialist other than GP (non-GP specialist) as almost as attractive as being employed at a hospital. Both career paths were described to be more attractive than working as a self-employed GP (Gibis et al. 2012; Heinz and Jacob 2012). According to Roick et al. (2012), the proportion of residents in general medicine who want to work self-employed (87.1%) is higher than that of non-GP residents (46.6%). However, Streit (2011) found that only 59% of the surveyed residents in general medicine wanted to work self-employed. This result is supported by Barth et al. (2017).
Ten of the included studies examined gender differences in attitudes towards self-employment (Barth et al. 2017; Cerutti et al. 2015; Gedrose et al. 2012; Gibis et al. 2012; Gisler et al. 2017; Heinz and Jacob 2012; Pfeil et al. 2020; Schneider et al. 2013; Steinhäuser et al. 2013; Ziegler et al. 2017). Half of the studies concluded that the desire to work in an employment setting was greater among women and to work self-employed was greater among men (Barth et al. 2017; Gibis et al. 2012; Gisler et al. 2017; Schneider et al. 2013; Ziegler et al. 2017). Two studies found no significant difference between the genders (Heinz and Jacob 2012; Steinhäuser et al. 2013). Another two studies specifically focused on being self-employed as a non-GP specialist (Gedrose et al. 2012; Pfeil et al. 2020). Here, more women than men could imagine themselves working as a non-GP specialist in private practice. Gedrose et al. (2012) found that the proportion of female students considering self-employment as a non-GP specialist was 1.3 times higher than their male counterparts. However, there was no significant difference between the genders in the study from Gedrose et al. (2012) when it came to the general willingness to work as self-employed. Only one study indicated that more female students want to work self-employed in primary care (Cerutti et al. 2015).
Gisler et al. (2017) examined the question of when medical students and residents decide to become self-employed. Ninety-three percent of the female participants stated that they wanted to work as salaried employees in their first job, in comparison to 80% of their male counterparts. Sixty-four percent of the men wanted to work as an employee for less than 2 years before setting up a practice, while 64% of women wanted to be employed for 2 to 5 years first (Gisler et al. 2017). One study takes this aspect into account; Zupanic et al. asked students about their long-term expectations. In this survey, only 4% stated that they could not imagine working as self-employed in private practice in the long term (Zupanic et al. 2011).
Financial conditions
The financial conditions were considered in eight of the included studies (Abelsen and Olsen 2012; Barth et al. 2017; Buddeberg-Fischer et al. 2011; Deutsch et al. 2020; Gibis et al. 2012; Heinz and Jacob 2012; Pfeil et al. 2020; Roick et al. 2012). Both students and residents rated the financial conditions of self-employed physicians as poor (Barth et al. 2017; Heinz and Jacob 2012; Gibis et al. 2012). Financial conditions should be considered carefully, given the results of Roick et al. (2012) which concluded that financial conditions are of high importance for future physicians. Students in Germany estimated the median monthly income of a GP to be €4500 (Deutsch et al. 2020). According to Deutsch et al. (2020) this was around €2000 less than the actual income at that time. The income level considered adequate by female students surveyed was €1000 lower than that of male students (Heinz and Jacob 2012). They also preferred receiving a fixed salary, while their male counterparts were more satisfied with activity-based remuneration (Abelsen and Olsen 2012). Almost half of the students in the study carried out by Abelsen and Olsen (2012) preferred a mixed remuneration system consisting of a fixed salary and activity-based remuneration. Only 20% preferred a pure activity-based remuneration or pure fixed salary (Abelsen and Olsen 2012). Financial risk was frequently named as a disadvantage of self-employment by both students and residents (Barth et al. 2017; Heinz and Jacob 2012; Gibis et al. 2012). High investment costs involved in setting up and taking over a practice were mentioned, among other things (Gibis et al. 2012; Buddeberg-Fischer et al. 2011). In German studies, the fear of recourse claims by health insurance was also mentioned (Barth et al. 2017; Heinz and Jacob 2012; Pfeil et al. 2020; Gibis et al. 2012).
Bureaucracy and non-medical tasks
Four studies addressed bureaucracy, which was named as a negative factor of self-employment by both students and residents (Barth et al. 2017; Gibis et al. 2012; Heinz and Jacob 2012; Pfeil et al. 2020). Students noted the lack of experience with bureaucracy as discouraging when setting up a practice (Gibis et al. 2012; Heinz and Jacob 2012). Germany’s accounting system was also highlighted by the surveyed students and residents as being a negative factor (Heinz and Jacob 2012; Pfeil et al. 2020). Interviewed students wanted targeted support and advice about administrative and legal issues (Gibis et al. 2012).
Organisation
Five of the studies deal with different aspects of the organisation (Barth et al. 2017; Buddeberg-Fischer et al. 2011; Gibis et al. 2012; Lillevang et al. 2019; Roick et al. 2012). In a German study, residents in general medicine stated that there are no externally-created circumstances within the scope of being a GP that are attractive (Barth et al. 2017). They also mentioned uncertainties with regard to planning at all levels and being torn between different claims and views. Thus, the surveyed residents wanted transparent professional framework conditions provided by politicians (Barth et al. 2017). Among the residents in general medicine surveyed by Buddeberg-Fischer et al. (2011), 51.2% stated that the restrictions on acquiring a practice license negatively influence opening their own practice.
Professional collaboration opportunities were important to respondents in the included studies. For example, residents in general medicine in the study by Lillevang et al. (2019) valued the close relationship with their colleagues in small group practices. Cooperation opportunities seemed to be more important to female residents, and they seemed to be more relevant for physicians who want to work as an employee (Roick et al. 2012).
Job satisfaction during residency
Job satisfaction during residency was primarily examined in two studies, one from Germany and one from Denmark both looking on residents in general medicine (Barth et al. 2017; Lillevang et al. 2019). Here the experiences were very contradictory. Danish respondents spoke of a high level of satisfaction in their jobs and a good sense of well-being (Lillevang et al. 2019), while German respondents were very dissatisfied. In an interview, one GP resident stated that they felt like being “trampled underfoot”. However, changing from working in a hospital to private practice encourages residents to work in private practice (Barth et al. 2017). For example, Buddeberg-Fischer et al. (2011) also indicated that 48.2% of surveyed residents viewed being a deputy GP in family practice as a positive influence on opening their own practice.
Personal responsibility
Personal responsibility were considered in four studies all looking at residents and was seen as an advantage of self-employment (Barth et al. 2017; Buddeberg-Fischer et al. 2011; Lillevang et al. 2019; Pfeil et al. 2020). Self-determined work and the more flexible working hours associated with it were seen as clear advantages (Barth et al. 2017; Buddeberg-Fischer et al. 2011; Lillevang et al. 2019; Pfeil et al. 2020). Respondents to Lillevang et al. (2019) also appreciated the responsibility they took over for the staff.
Career opportunities
Two studies addressed career opportunities by looking at GPs and primary care physicians (Barth et al. 2017; Cerutti et al. 2015). The unanimous opinion of the students and residents was that GPs and primary care physicians have good career opportunities with many job openings (Cerutti et al. 2015; Barth et al. 2017). Primary care physicians’ career paths appeared to be diverse for the surveyed students (Cerutti et al. 2015).
Specialty-dependent factors
Four studies look at factors that deal with the medical work of a self-employed physician (Cerutti et al. 2015; Heinz and Jacob 2012; Lillevang et al. 2019; Pfeil et al. 2020). The influencing factors differ depending on the specialty considered. In regard to the specialty of general medicine, a broad and diverse patient spectrum was mentioned. This was linked to a unique long-term doctor–patient relationship (Cerutti et al. 2015; Lillevang et al. 2019). The specialty-dependent factors in general medicine were rated positively. In contrast, surveyed rheumatologists in residency rated the outpatient spectrum of rheumatologic diseases as a negative point for self-employment (Pfeil et al. 2020).
Personal environment
Five of the included studies considered the personal environment (Barth et al. 2017; Buddeberg-Fischer et al. 2011; Heinz and Jacob 2012; Lillevang et al. 2019; Roick et al. 2012). Compatibility with the family and work–life balance were important for all specialists (Barth et al. 2017; Heinz and Jacob 2012; Lillevang et al. 2019; Roick et al. 2012), but were stronger deciding factors for women than men (Barth et al. 2017; Roick et al. 2012). Moreover, these conditions were especially important for younger physicians. Quality of life within the environment was more important for men than women, as well as for physicians who grew up in the city rather than in a rural region (Roick et al. 2012).
The positive influence of personal role models who are self-employed in private practice was also mentioned by residents in general medicine. Thus, personal role models could motivate others to establish their own practice (Barth et al. 2017; Buddeberg-Fischer et al. 2011).
Education
Education was considered in six of the included studies (Abelsen and Olsen 2012; Buddeberg-Fischer et al. 2011; Deutsch et al. 2013; Heinz and Jacob 2012; Lillevang et al. 2019; Ziegler et al. 2017). Students described practical experience and teaching content during training as influencing career choice (Abelsen and Olsen 2012; Heinz and Jacob 2012). The lack of information about taking over a practice was one of the six most frequently chosen reasons against setting up a practice in the survey from Buddeberg-Fischer et al. (2011). Heinz and Jacob (2012) reported a positive influence of practical experience during their studies. In the Danish study, residency in general medicine is described as very attractive and seems to help residents prepare well for later career opportunities (Lillevang et al. 2019). Ziegler et al. (2017) noted a contrary trend among students undertaking their residency in outpatient care. Here, attitudes towards self-employment changed during the residency, moving away from self-employment toward being employed. Deutsch et al. (2013) investigated the influence of an early community-based family practice elective with one-to-one mentoring on the students’ attitudes towards general practice. The proportion of those who favoured general medicine as a specialisation increased from 26% to 32.7%. Willingness to work as self-employed was neither positively nor negatively influenced by the course.
Rural area
Rural areas were considered in three of the included studies (Heinz and Jacob 2012; Steinhäuser et al. 2013; Wilhelmi et al. 2018). The most frequently described aspect of setting up a practice in rural areas is the personal context. Steinhäuser et al. (2013) found a positive significant correlation between the idea of being self-employed in a rural area and a family-friendly environment. Another aspect was the physician’s personal connection to the region. Coming from a rural area increased the probability that a resident will work as self-employed in a rural area more than twofold (Steinhäuser et al. 2013). According to Heinz and Jacob (2012), 76.2% of medical students who came from a village with less than 5000 inhabitants would also settle in a similar-sized village. However, a personal connection to the region does not only have to be linked to where the physician comes from. Friends, hobbies, vacations, or other stays in rural regions can also create such a relationship (Wilhelmi et al. 2018).
Another important factor was the collegial environment. The respondents of Wilhelmi et al. (2018) and Heinz and Jacob (2012) stated that they would feel more alone in rural areas. Lack of professional exchange with colleagues would deter them from settling in rural areas. Long distances to the nearest hospital and colleagues was also mentioned. Future specialists would have to become more confident and self-assured to dare to take this step. The lack of further training in rural areas was also criticised. However, the perceived lack of support from colleagues contrasts with the significantly higher perceived support from the communities (Wilhelmi et al. 2018).
The financial situation of rural physicians in private practice is assessed differently. Wilhelmi et al. (2018) describe the financial situation as positive, while medical students who responded to Heinz and Jacob (2012) state that it is poor.
Rural areas were described as boring working environments where there is a danger of routinisation of work that may arise due to a narrow patient spectrum. It was mentioned that the patient spectrum includes many old patients and that there is little freedom of therapy (Heinz and Jacob 2012; Wilhelmi et al. 2018).
Discussion
This is the first systematic review of the attitudes of future specialists towards self-employment in private practice, to the best of our knowledge. One of the most frequently mentioned factors was work–life balance and the associated compatibility with family. This also coincides with the results of studies on generational research. Ernst and Young (2013) found that family and friends are of the greatest value to the younger generation. In addition to this, work–life balance and compatibility with the family is more important for women than men (Diderichsen et al. 2013). Due to the increasing proportion of female physicians, the work–life balance might also be considered to be more important.
It can also be seen in entrepreneurship research that more men than women start their own businesses. The proportion of self-employed women is lower than that of men in all OECD countries (OECD 2022b). In the included studies, we noticed a security aspect, which was particularly important for women. Women are more likely to be employed and prefer a fixed salary. Employment promises a high degree of security due to fixed salaries and good cooperation opportunities. It should also be taken into account that in families, even today, it is often the women who tend to stay at home when a child falls ill (Hobler et al. 2017). Employees receive their income even in the event of illness. Thus, employment is increasingly attractive, especially for young women with children. Gisler et al. (2017) came to the same conclusion, as future female specialists want to work longer in employment than men.
Flexibility is often rated as a positive aspect of being self-employed in private practice. This refers to the flexibility of the work itself. Flexibility with regard to a quick change of job is not guaranteed when self-employed. However, this type of flexibility is important to Generation Y. They have grown up with a multitude of choices and want to keep them open (Parment 2013). This could also explain Zupanic et al.’s results (2011), according to which only 4% of students would not want to be self-employed for their entire career. Young doctors want to keep their choices open. Moreover, Generation Y changes its attitudes and views more quickly (Parment 2013). These aspects contradict the idea of opening a practice and spending one’s whole professional life in the same place.
As previously mentioned, future specialists seem to prefer more cooperation opportunities. This was also seen in studies on Generation Y (Parment 2013; Brinkmann 2020). These cooperation possibilities promise support in the event of unclear questions. Young physicians often leave their residencies with low levels of self-confidence. Cooperation opportunities provide more security in many respects. Physicians can discuss medical issues and exchange experience in practice management. In the case of a group practice, patient care can be organised easier in the event of physician illness. Responsibility for staff and the financial and economic risks can also be shared. A trend towards group practices can be seen in many countries (Gerkens and Merkur 2020; Olejaz et al. 2012; DePietro et al. 2015; Kroneman et al. 2016; Kassenärztliche Bundesvereinigung (KBV) 2022b). This trend is likely to continue due to the increasing attractiveness of collaborative opportunities, especially among women. Group practices also have economic advantages. For example, health care efficiency could be improved and resources are saved by sharing equipment. In rural areas, establishing a group practice is likely to be more difficult due to the sparse population (Pedersen et al. 2012). In these cases, a mentor could support the young physicians. The mentor can help build a communication infrastructure with colleagues and answer important questions (Wilhelmi et al. 2018). Generation Y also wish to received direct feedback on their work (Evans et al. 2016; Brinkmann 2020).
Early information to future specialists about the working conditions of a physician in private practice seems to be very important. Future specialists have no real idea about the financial situation of self-employed physicians. On the one hand, income is greatly underestimated, and on the other hand, financial risk is often a topic of discussion (Deutsch et al. 2020). Targeted information is crucial here. Future specialists’ concerns about financial risks could be reduced. Informing future specialists about average income may also increase the attractiveness of setting up a practice. Furthermore, the lack of administrative knowledge was named as an obstacle to setting up a practice (Heinz and Jacob 2012). Medical students are still too far away from opening their own practice. Thus, this knowledge is not yet considered important in their studies. This leads to them mostly having little information about practice management. Many studies have shown that a primary care curriculum positively influences participants’ attitudes towards a career in this field. Informing students at an early stage seems to have an impact on their attitudes (Chung et al. 2016; Ford et al. 2018; Hawthorne and Dinh 2017; Phillips and Keys 2018). This indicates that curricula could be developed that also address self-employment in private practice.
Practical experience has been shown to have a positive influence on self-employment in private practice. This could be due to role models, as well as to a better assessment of working conditions. The study by Deutsch et al. (2013) found that an early community-based family practice elective did not affect the idea of setting up a practice. However, this may also be due to the content selected to be part of the curriculum. Further research is needed to find out what information should be displayed and how. Evans et al. (2016) found that moving from pure lecture-based courses to those that incorporate hands-on activities increased the interest and information retention of Generation Y medical students.
Limitations
The strengths and weaknesses of this work lie in the strengths and weaknesses of the included studies. In this regard, the most frequently addressed issue is the study population. Thus, future specialists, who are already interested in self-employment, may have been more likely to participate in these surveys. As a consequence, there might be an overrepresentation of the willingness to work as self-employed in private practice.
Another limitation is the high proportion of studies found via the unsystematic search, as there is a risk that relevant studies were not identified by the search strategy used. A large proportion of the included studies comes from Germany. This could result in a potential bias, as the main author is from Germany. However, the Danish author also conducted the unsystematic search and found studies that were mainly published in Germany. This could be due to the fact that German has a specific term for a self-employed physician in private practice. This may give the topic more attention and make searches more precise. In English, there is only a description of the job profile. For this reason, the commonly used terms for self-employment in private practice were collected in the search strategy. However, it is possible that some countries use terminology that we have not identified, which may have resulted in the loss of studies. In addition, there are different terms for future specialists in different countries, which also may have resulted in the loss of studies.
Creating the search strategy was the biggest challenge in this review due to the incongruence in terminology. We have tried to meet the challenge by carefully working out the keywords. Extensive non-systematic research was carried out to include as many relevant studies as possible. If relevant studies were not found, this may be due to the linguistic diversity of the topic rather than the diligence of the author.
Different definitions of terms also posed a challenge in the evaluation of the studies. For example, the term primary care is used differently in several countries. Cerutti et al. (2015) look at primary care physicians without defining this term. Readers are left to make their own assumptions. Since this is a Swiss study, it is likely that general practitioners, paediatricians, internal medicine doctors, and gynaecologists are considered here (Kringos et al. 2015).
Another limitation is that no quality assessment tools have been used in this qualitative systematic review. We piloted quality assessment, but did not follow through out of concern that only few studies would remain. Given that similar patterns could be observed across the included studies it is likely that our results are reliable. We further believe it is important to provide an overview of all relevant studies conducted on this topic. It is clear that although research has been done in this field, further research with strong methodology is needed. This circumstance could also explain the higher proportion of search results from the PubMed database, which provides larger access to the grey literature.
The health care systems and training of future specialists differ in the countries considered. One difference, for example, lies in the remuneration of self-employed physicians. Also the role of the GPs varies; in some countries, they function as gatekeepers to more specialised treatment. Structural differences in medical training mean that residency is perceived very differently in Germany and Denmark, as suggested by our results. We did, however, exclude studies from contexts where self-employment is not a general career option (e.g., in Sweden), to diminish the potential effect of structural differences between health care systems.
Conclusion
This work shows a wide range of factors that influence future specialists in terms of self-employment. It can be seen that opportunities for cooperation, compatibility with family, and a need for security are deciding factors for many future specialists. The attractiveness of self-employment could be increased by intervening in education. Universities should be aware of informing medical students about possible career paths to provide an informed decision-making process. Contact with colleagues is also a crucial factor. In rural areas, a mentor could be organised to assist young doctors with any questions they may have. This mentor should be available for all questions (medical and administrative). This would perhaps also reduce the uncertainty of future specialists.
However, Generation Y seem less interested in long-term work commitments. This indicates that it might be time to consider whether self-employment in private practice is outdated and new forms of organisation should be brought into focus in the long term. The focus could be on group practices or medical centres. In sparsely populated regions, several doctors could share practice rooms. Here, different specialists could work on different days to save acquisition costs and have contact with colleagues. New forms of working in outpatient care should be developed, or medical education structured in a way that makes working self-employed in private practice attractive to young physicians, as this will help ensure demand-oriented care.
Data availability
Not applicable.
Code availability
Not applicable.
References
Abelsen B, Olsen JA (2012) Does an activity based remuneration system attract young doctors to general practice? BMC Health Serv Res 12:1–8. https://doi.org/10.1186/1472-6963-12-68
Bachner F, Bobek J, Habimana K, Ladurner J, Lepuschütz L, Ostermann H, Rainer L, Schmidt AE, Zuba M, Quentin W, Winkelmann J (2018) Austria: health system review. Health Syst Transit 20(3):1–256
Barth N, Linde K, Schneider A (2017) Niederlassungsmotive — Die Bereitschaft zur Niederlassung in eigener Praxis von Ärztinnen und Ärzten in Weiterbildung zum Facharzt für Allgemeinmedizin. Gesundheitswesen 79(8–09):638–644. https://doi.org/10.1055/s-0035-1547299
Becher L (2022) Selbständigkeit. Bundeszentrale für politische Bildung, Bonn. https://www.bpb.de/themen/arbeit/arbeitsmarktpolitik/328982/selbstaendigkeit/. Accessed 07 Apr 2022
Behmane D, Dudele A, Villerusa A, Misins J, Kļaviņa K, Mozgis D, Scarpetti G (2019) Latvia: health system review. Health Syst Transit 21(4):1–165
Berthier D (2018) Europe has a shortage of doctors. https://www.europeandatajournalism.eu/News/Data-news/Europe-has-a-shortage-of-doctors. Accessed 20 May 2022
Brinkmann S (2020) Arbeitswerte der Generation Y im internationalen Vergleich: Analyse der Heterogenität arbeitsbezogener Werte nach den GLOBE-Kulturclustern. BestMasters. Springer, Wiesbaden
Buddeberg-Fischer B, Klaghofer R, Stamm M (2011) Family physicians in Switzerland: transition from residency to family practice // family physicians in Switzerland: transition from residency to family practice. Fam Med 43(1):29–36. https://doi.org/10.5167/UZH-50247
Bundesärztekammer (2011) Ärztestatistik zum 31.12.2010: Alle Abbildungen und Tabellen. Bundesärztekammer, Bonn. https://www.bundesaerztekammer.de/ueber-uns/aerztestatistik/aerztestatistik-der-vorjahre/aerztestatistik-2010/. Accessed 04 May 2022
Bundesärztekammer (2021) Ärztestatistik zum 31. Dezember 2020: Alle Diagramme und Tabellen. Bundesärztekammer, Bonn. https://www.bundesaerztekammer.de/ueber-uns/aerztestatistik/aerztestatistik-2020/. Accessed 07 Apr 2022
Cerutti B, Junod Perron N, van Gessel E, Haensgen K-D, Sommer J (2015) Changes in the perception of primary care practice during the medical curriculum in Geneva, Switzerland. Swiss Med Wkly 145:w14124. https://doi.org/10.4414/smw.2015.14124
Chevreul K, Berg Brigham K, Durand-Zaleski I, Hernández-Quevedo C (2015) France: health system review. Health Syst Transit 17(3):1–218
Chung C, Maisonneuve H, Pfarrwaller E, Audétat M-C, Birchmeier A, Herzig L, Bischoff T, Sommer J, Haller DM (2016) Impact of the primary care curriculum and its teaching formats on medical students' perception of primary care: a cross-sectional study. BMC Fam Pract 17(1):135. https://doi.org/10.1186/s12875-016-0532-x
DePietro C, Camenzind P, Sturny I, Crivelli L, Edwards-Garavoglia S, Spranger A, Wittenbecher F, Quentin W (2015) Switzerland: health system review. Health Syst Transit 17(4):1–288
Deutsch T, Hönigschmid P, Frese T, Sandholzer H (2013) Early community-based family practice elective positively influences medical students' career considerations—a pre-post-comparison. BMC Fam Pract 14:1–6. https://doi.org/10.1186/1471-2296-14-24
Deutsch T, Heine A, Lippmann S, Geier A-K, Bauer A, Frese T (2020) Medical students' perspectives on earning opportunities of self-employed physicians - realistic and relevant for the process of career choice? BMC Med Educ 20(1):42. https://doi.org/10.1186/s12909-020-1950-y
Diderichsen S, Johansson EE, Verdonk P, Lagro-Janssen T, Hamberg K, Diderichsen S, Johansson EE, Verdonk P, Lagro-Janssen T, Hamberg K (2013) Few gender differences in specialty preferences and motivational factor: a cross-sectional Swedish study on last-year medical students // few gender differences in specialty preferences and motivational factors: a cross-sectional Swedish study on last-year medical students. BMC Med Educ 13(39):1–8. https://doi.org/10.1186/1472-6920-13-39
Ernst & Young (2013) Absolventenstudie 2012–2013. Ernst & Young, Hamburg. https://www.reif.org/wp-content/uploads/2013/08/EY-Absolventenbefragung-2013-Studie.pdf. Accessed 28 Apr 2021
Eurostat (2020) Healthcare personnel statistics — physicians. Eurostat, Luxembourg. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Healthcare_personnel_statistics_-_physicians&oldid=561101#Healthcare_personnel. Accessed 02 May 2022
Evans KH, Ozdalga E, Ahuja N (2016) The medical education of generation Y. Academic Psychiatry 40(2):382–385. https://doi.org/10.1007/s40596-015-0399-5
Ford CD, Patel PG, Sierpina VS, Wolffarth MW, Rowen JL (2018) Longitudinal continuity learning experiences and primary care career interest: outcomes from an innovative medical school curriculum. J Gen Intern Med 33(10):1817–1821. https://doi.org/10.1007/s11606-018-4600-x
Gerkens S, Merkur S (2020) Belgium: health system review. Health Syst Transit 22(5):1–237
Gerlach F, Greiner W, Haubitz M, Meyer G, Schreyögg J, Thürmann P, Wille E (2018) Bedarfsgerechte Steuerung der Gesundheitsversorgung. Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen, Bonn/Berlin
Gibis B, Heinz A, Jacob R, Müller C-H (2012) The career expectations of medical students: findings of a nationwide survey in Germany. Dtsch Arztebl Int 109(18):327–332. https://doi.org/10.3238/arztebl.2012.0327
Gisler LB, Bachofner M, Moser-Bucher CN, Scherz N, Streit S (2017) From practice employee to (co-)owner: young GPs predict their future careers: a cross-sectional survey. BMC Fam Pract 18(1):1–9. https://doi.org/10.1186/s12875-017-0591-7
Habicht T, Reinap M, Kasekamp K, Sikkut R, Aaben L, van Ginneken E (2018) Estonia: health system review. Health Syst Transit 20(1):1–193
Hawthorne MR, Dinh A (2017) Meeting the demand of the future: a curriculum to stimulate interest in careers in primary care internal medicine. Med Educ Online 22(1):1340780. https://doi.org/10.1080/10872981.2017.1340780
Heinz A, Jacob R (2012) Medizinstudenten und ihre Berufsperspektiven. In welcher Facharztrichtung, wo und wie wollen sie arbeiten? Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 55(2):245–253. https://doi.org/10.1007/s00103-011-1413-z
Hobler D, Klenner C, Pfahl S, Sopp P, Wagner A (2017) Wer leistet unbezahlte Arbeit? Hausarbeit, Kindererziehung und Pflege im Geschlechtervergleich. Aktuelle Auswertungen aus dem WSI GenderDatenPortal. Hans-Böckler-Stiftung, Wirtschafts- und Sozialwissenschaftliches Institut (WSI), Düsseldorf
Kassenärztliche Bundesvereinigung (KBV) (2022a) Bedarfsplanung. Kassenärztliche Bundesvereinigung (KBV), Berlin. https://www.kbv.de/html/bedarfsplanung.php. Accessed 10 Aug 2022
Kassenärztliche Bundesvereinigung (KBV) (2022b) Ärzte in Praxen. Kassenärztliche Bundesvereinigung (KBV), Berlin https://gesundheitsdaten.kbv.de/cms/html/17019.php. Accessed 07 Apr 2022
Kringos DS, Boerma WGW, Hutchinson A, Saltman RB (eds) (2015) Building primary care in a changing Europe: case studies. Observatory studies series 40. European Observatory on Health Systems and Policies, Copenhagen
Kroneman M, Boerma W, van den Berg M, Groenewegen P, de Jong J, van Ginneken E (2016) Netherlands: health system review. Health Syst Transit 18(2):1–239
Kuckartz U (2018) Qualitative Inhaltsanalyse: Methoden, Praxis, Computerunterstützung, 4th edn. Grundlagentexte Methoden. Beltz Juventa, Weinheim, Basel
Lillevang G, Henriksen M, Brodersen J, Lewandowska K, Kjær NK (2019) Why do Danish junior doctors choose general practice as their future specialty? Results of a mixed-methods survey. Eur J Gen Pract 25(3):149–156. https://doi.org/10.1080/13814788.2019.1639668
Mohammadiaghdam N, Doshmangir L, Babaie J, Khabiri R, Ponnet K (2020) Determining factors in the retention of physicians in rural and underdeveloped areas: a systematic review. BMC Fam Pract 21(1):216. https://doi.org/10.1186/s12875-020-01279-7
Nüsken J, Busse R (2011) Ansatzpunkte und Kriterien der Bedarfsplanung in anderen Gesundheitssystemen. Im Auftrag der Bundesärztekammer. https://www.bundesaerztekammer.de/fileadmin/user_upload/_old-files/downloads/Internationale-Bedarfsplanung.pdf. Accessed 10 Aug 2022
OECD (2022a) Availability of doctors | Health at a Glance: Europe 2020 State of Health in the EU Cycle | OECD iLibrary. OECD, Paris. https://www.oecd-ilibrary.org/sites/1d767767-en/index.html?itemId=/content/component/1d767767-en. Accessed 03 May 2022
OECD (2022b) Employment - Self-employment rate - OECD Data. OECD, Paris. https://data.oecd.org/emp/self-employment-rate.htm. Accessed 20 May 2022
Olejaz M, Juul Nielsen A, Rudkjøbing A, Okkels Birk H, Krasnik A, Hernández-Quevedo C (2012) Denmark: health system review. Health Syst Transit 14(2):1–192
Parment A (2013) Die Generation Y. Gabler, Wiesbaden
Pedersen KM, Andersen JS, Søndergaard J (2012) General practice and primary health Care in Denmark. J Am Board Fam Med 25(Suppl 1):S34–S38. https://doi.org/10.3122/jabfm.2012.02.110216
Pfeil A, Baerwald C, Sieburg M, Boche K, Kupka TA, Linde T, Heldmann F, Unger L, Oelzner P, Aringer M, Keyßer G (2020) Future of rheumatologists: what are the perspectives?: survey of resident physicians in rheumatology in middle Germany. Z Rheumatol 79(2):168–174. https://doi.org/10.1007/s00393-019-00713-1
Phillips WR, Keys T (2018) Interprofessional primary care course curriculum and evaluation. Fam Med 50(3):217–222. https://doi.org/10.22454/FamMed.2018.998057
Roick C, Heider D, Günther OH, Kürstein B, Riedel-Heller SG, König HH (2012) Was ist künftigen Hausärzten bei der Niederlassungsentscheidung wichtig? Ergebnisse einer postalischen Befragung junger Ärzte in Deutschland. Gesundheitswesen 74(1):12–20. https://doi.org/10.1055/s-0030-1268448
Saunes IS, Karanikolos M, Sagan A (2020) Norway: health system review. Health Syst Transit 22(1):1–163
Schneider A, Karsch-Völk M, Rupp A, Fischer MR, Drexler H, Schelling J, Berberat P (2013) Predictors of a positive attitude of medical students towards general practice - a survey of three Bavarian medical faculties // Determinanten für eine hausärztliche Berufswahl unter Studierenden der Medizin: Eine Umfrage an drei bayerischen Medizinischen Fakultäten. GMS Z Med Ausbild 30(4):Doc45. https://doi.org/10.3205/zma000888
Siewert U, Fendrich K, Markus MRP, Baumeister SE, Doblhammer-Reiter G, Scholz RD, Hoffmann W (2013) Future outpatient health-care utilisation in an ageing population: projections up to the year 2020 based on the study of health in Pomerania (SHIP). J Public Health 21:289–296. https://doi.org/10.1007/s10389-012-0550-7
Steinhäuser J, Joos S, Szecsenyi J, Götz K (2013) Welche Faktoren fördern die Vorstellung sich im ländlichen Raum niederzulassen? Zeitschrift für Allgemeinmedizin 89(1):10–15. https://doi.org/10.3238/zfa.2013.0010-0015
Streit S (2011) Moderne Praxisformen: Resultate einer schweizweiten Umfrage unter zukünftigen Hausärztinnen und Hausärzten. PrimaryCare (de) 11(19):342–343. https://doi.org/10.4414/pc-d.2011.08998
Tikkanen R, Osborn R, Mossialos E, Djordjevic A, Wharton GA (2020) International profiles of health care systems. Commonwealth Fund, New York. https://www.commonwealthfund.org/sites/default/files/2020-12/International_Profiles_of_Health_Care_Systems_Dec2020.pdf. Accessed 07 Apr 2022
Wijnen-Meijer M, Burdick W, Alofs L, Burgers C, Ten CO (2013) Stages and transitions in medical education around the world: clarifying structures and terminology. Med Teach 35(4):301–307. https://doi.org/10.3109/0142159X.2012.746449
Wilhelmi L, Ingendae F, Steinhaeuser J (2018) What leads to the subjective perception of a 'rural area'? A qualitative study with undergraduate students and postgraduate trainees in Germany to tailor strategies against physician's shortage. Rural Remote Health 18(4):4694. https://doi.org/10.22605/RRH4694
Ziegler S, Zimmermann T, Krause-Solberg L, Scherer M, van den Bussche H, Ziegler S, Zimmermann T, Krause-Solberg L, Scherer M, van den Bussche H (2017) Male and female residents in postgraduate medical education — a gender-comparative analysis of differences in career perspectives and their conditions in Germany. GMS Zeitschrift fur medizinische Ausbildung 34(5):1–17. https://doi.org/10.3205/zma001130
Zupanic M, Hofmann M, Osenberg D, Gardeik K, Jansen P, Fischer MR, Zupanic M, Hofmann M, Osenberg D, Gardeik K, Jansen P, Fischer MR (2011) Die angestrebte oder befürchtete berufliche Zukunft von Wittener Medizinstudierenden // the aimed or feared professional future of medical students at the Univesity of Witten/Herdecke. GMS Z Med Ausbild. 28(2):1–12. https://doi.org/10.3205/zma000737
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
The idea for the systematic review came from Juliana Meyer and Steffen Flessa. The protocol for the systematic review was agreed with all authors. The systematic research was conducted by Sofie Gjessing and Juliana Meyer. The data analysis was performed by Juliana Meyer. The first draft of the manuscript was written by Juliana Meyer, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflicts of interest/competing interests
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOC 27 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Meyer, J., Gjessing, S., Kristensen, J.K. et al. Attitudes of medical students and junior physicians towards working self-employed in private practice in Northern and Western Europe: a systematic review. J Public Health (Berl.) 31, 1759–1772 (2023). https://doi.org/10.1007/s10389-022-01760-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-022-01760-w