
Abstract
Aim
The “Five moments of hand hygiene” (World Health Organization 2009) can be classified into moments of hand hygiene before and after patient care. Based on research indicating that hand hygiene compliance differs with regard to moments before and after patient care, this research evaluates the effectiveness of an empathy-based intervention in motivating hand hygiene compliance with regard to moments before patient care which protect vulnerable individuals from contamination and infection.
Subjects and method
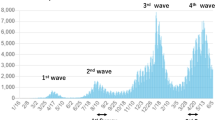
An online experiment involving 68 healthcare professionals working at a German hospital during the first wave of the COVID-19 pandemic investigates whether instructing healthcare professionals to consider consequences for others (vs for themselves) if they contracted SARS-CoV-2 promotes hand hygiene compliance referring to moments before (vs after) patient care.
Results
In the condition in which healthcare professionals considered consequences for others if they contracted SARS-CoV-2 (other-focus condition), ratings of importance increased (M = 3.49, SD = 1.30) compared to the condition in which healthcare professionals considered consequences for themselves (M = 2.68, SD = 1.24), F(1,66) = 6.87, p = .011, partη2 = .09. Participants in the other-focus condition reported more intentions to comply with “before moments” in the future (M = 3.34, SD = 1.14) compared to participants in the self-focus condition (M = 2.77, SD = 0.80), F(1,66) = 6.15, p = .016, partη2 = .09.
Conclusion
Results indicate that activating an empathic focus in the context of the current pandemic promotes perceived importance and motivation of healthcare professionals to comply with moments aiming at protecting vulnerable others.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hand hygiene compliance by healthcare workers is vital for preventing healthcare-associated infections (HAIs) and also plays a significant role in preventing pathogen transmission such as COVID19 in hospitals (Gundersborg Sandbøl et al. 2022; World Health Organization (WHO) 2020). Nevertheless, compliance with hand hygiene guidelines is still alarmingly low in many healthcare institutions (Clancy et al. 2021). Therefore, the present study examined whether activating an empathic focus within this pandemic — by activating thoughts about the implications for others (vs for themselves) if participants contracted SARS-CoV-2 — fosters healthcare professionals’ hand hygiene compliance (HHC), particularly in contexts in which vulnerable others are protected by correctly performed hand hygiene behavior. This notion is based on the argument that empathy as an interpersonal orientation involves both an affective connection as well as adopting the perspective of other individuals (Batson 2009). This in turn leads to increased valuing of other individuals’ welfare and finally results in providing help and assistance (Batson 2009). Activating an empathic focus should therefore ultimately promote behavior that supports other individuals’ well-being. Hand hygiene behavior is a likely candidate in this context, because it represents a behavior clearly affecting others’ well-being, namely their state of health, to a considerable extent (Allegranzi and Pittet 2009). A recent meta-analysis indicates, for instance, that a single hand hygiene action is associated with a decrease in the daily likelihood of an acute respiratory infection (Mo et al. 2022).
Appropriate hand hygiene behavior in healthcare is exactly defined by evidence-based guidelines, precisely by the WHO (2009), which include the “Five moments of hand hygiene”. These guidelines describe in which types of situations and by what means hand hygiene behavior should be performed to interrupt pathogen transmission. The WHO’s five moments (WHO 2009) comprise “before patient contact” (Moment 1), “before aseptic procedure” (Moment 2), “after body fluid exposure risk” (Moment 3), “after patient contact” (Moment 4), and “after contact with patient surroundings” (Moment 5). Moments 1 and 2 represent the two “before moments”, which mainly serve the goal to prevent patients from colonization and infection. Moments 3, 4, and 5 represent the three “after moments” and are mainly concerned with preventing healthcare workers’ colonization and contamination (cf. Kingston et al. 2016). Consequently, hand hygiene behavior can be motivated by both the goal of protecting oneself and the goal of protecting others. Furthermore, recent research indicates that HHC differs with regard to the two types of moments, with lower compliance before patient contact than after. Specifically, Wetzker et al. (2016) provided data from German hospitals indicating that HHC before patient contact is lower (70%) compared to HHC after patient contact (82,5%). These findings are mirrored in a systemic review of published studies by Kingston et al. (2016), which also indicates that HHC is lower before patient contact (21%) compared to HHC after patient contact (47%). These findings are noteworthy given that patients are more vulnerable with regard to infections, as they can be weakened by their medical condition (immune status, wounds) and/or the treatment they receive. Moreover, it has been shown that invasive procedures (e.g., catheterization) are associated with an increased risk of HAIs (Schreiber et al. 2018). Consequently, patients probably benefit more (in absolute terms) from correctly performed disinfection measures than healthcare professionals, especially with regard to the “before moments”.
The development and testing of interventions aimed at increasing HHC involving “before moments” is, therefore, urgently needed. A promising approach in this context is the activation of an empathic focus in healthcare professionals. This assumption can be further substantiated when conceptualizing empathy as a basic moral emotional process fostering morality-motivated actions (Tangney et al. 2007). In the context of healthcare, morally appropriate actions mean that patients are saved from (further) suffering (e.g., by transmission of pathogens). Accordingly, one means of realizing this morally motivated inclination is the diligent observance of hand hygiene standards, especially with regard to the "before moments", which specifically serve to protect patients from the transmission of pathogens (Sax et al. 2007). Notably, previous research already demonstrated the positive impact of an empathy induction on healthcare workers’ frequency of hand hygiene behavior (Sassenrath et al. 2016). However, given that an increase in mere frequency might also include unnecessary hand disinfections, which may be detrimental because they unnecessarily consume valuable time (see Stahmeyer et al. 2017), the present study goes one step beyond. Here, we test the impact of activating an empathic focus within the present pandemic on healthcare workers hand hygiene compliance; that is, whether they are willing to more diligently adhere to guidelines defining when to perform a hand hygiene activity — particularly those guidelines aiming at protecting of vulnerable others.
Therefore, this study investigated whether instructing healthcare professionals to consider the consequences for others (compared to the consequences for themselves) if they became infected with SARS-CoV-2 leads to higher ratings of the importance of HHC in relation to 'before moments'. It was also tested whether this manipulation leads to increased self-reported behavioral intentions to perform appropriate hand hygiene in situations involving “before moments”.
We conducted an online rather than an on-site study, because the nationwide lockdown impeded entering hospitals or healthcare facilities during the study period (June–July 2020).
Method
Participants and design
Sixty-eight individuals who worked at a German municipal hospital of basic and regular care with more than 250 beds of nine medical, surgical, and interdisciplinary specialties, treating about 12.000 inpatients and 20.000 outpatients per year, participated in the study. Nurses were 78% of participants, 22% were physicians; 72 % of them had worked in their profession for 10 years or more; 19% took care of COVID-19 patients during the study period. All participants gave their consent to participate in a 10-minute online experiment with two experimental conditions. As compensation they received a voucher for 7.50 €, which could be redeemed in local stores and businesses. The study was approved by hospital management and employee representation. Participants were recruited by email via the hospital staff mailing list.
Materials and procedure
Participants were recruited for a study addressing potential barriers to hand hygiene compliance in patient care during the COVID-19 pandemic. All instructions, tasks, and measures were presented using the software Unipark (https://www.unipark.com). By implementing a trigger, the experimental software ensured that all participants were randomly assigned to one of the two experimental conditions. Notably, a true randomization as implemented by the experimental software implies some variation and, thus, is associated with a not perfectly equal distribution of participants to the conditions (self-focus condition: n = 31; other-focus condition: n = 37). Table 1 depicts the distribution of participants’ profession (nurse, physician, or other), participants’ gender, and whether they had taken care of CVOID19 patients during the study period to the two conditions.
Hence, in the self-focus condition, the study started with asking participants to think about the consequences of contracting SARS-CoV-2 for themselves, both in terms of their personal health and their social and professional situation. In the other-focus condition, participants were asked to think about the consequences of contracting SARS-CoV-2 for other individuals with whom they were in contact. Participants should consider consequences for these individuals’ social and professional situation. In both conditions, participants were instructed to take notes.
Afterwards, participants in both experimental conditions indicated for each of the “Five moments of hand hygiene” (WHO 2009) how important they evaluate compliance with each moment, applying a Likert scale ranging from “1 = not at all important” to “7 = very important”. Subsequently, they indicated how difficult they viewed compliance with each of the five moments under current pandemic working conditions (Likert scale: “1 = not at all difficult” to “7 = very difficult”). Then, participants in both conditions made comparative judgments by indicating for which of the five moments they viewed compliance as most important. Next, participants answered the following item assessing behavioral intention in a comparative manner: “When thinking about the consequences of a SARS-CoV-2-infection for others (vs for yourself), which of the Five moments of hand hygiene do you intend to comply with most diligently during your work in the future?” by clicking on one of all five moments which were presented simultaneously at the screen.
Finally, as control variables, we assessed participants' perceived comprehensibility of the five moments (using a Likert scale from "1 = not at all comprehensible" to "7 = completely comprehensible"), and whether reducing the recommended exposure time from 30 to 15 seconds when using alcohol-based hand rubs would facilitate compliance with the five moments (using a Likert scale from "1 = would not facilitate at all" to "7 = would facilitate significantly"). Participants also rated their current working conditions according to how pleasant, harmonious, uncomplicated, inspiring, and challenging they perceived it. Additionally, participants answered the Empathic Concern subscale of the Interpersonal Reactivity Index (IRI, Davis 1983) and completed the Perceived Stress Scale (Cohen et al. 1983).
Results
This study tested whether instructing healthcare professionals to consider the consequences for others (other-focus condition) if they contracted SARS-CoV-2 leads them to assign a higher importance to HHC indications involving “before moments” compared to participants imagining consequences for themselves (self-focus condition). Similarly, it was examined whether self-reported behavioral intention to perform appropriate hand hygiene in situations involving “before moments” is higher in the other-focus compared to the self-focus condition. Therefore, a multivariate ANOVA with the between-subjects factor (focus: self vs other) as independent variable and the reported absolute importance regarding each of the five moments as multivariate dependent variable revealed a significant main effect for the experimental factor, F(5,62) = 2.47, p = .042, partη2 = .17 (see Table 2). Likewise, when analyzing comparative judgments in which participants compared the importance of compliance between the five moments, participants indicated higher importance of compliance with “before moments” in the other-focus condition (M = 3.49, SD = 1.30) compared to the self-focus condition (M = 2.68, SD = 1.24), F(1,66) = 6.87, p = .011, partη2 = .09. Even more importantly, participants in the other-focus condition reported more intentions to comply with “before moments” in the future (M = 3.34, SD = 1.14) compared to participants in the self-focus condition (M = 2.77, SD = 0.80), F(1,66) = 6.15, p = .016, partη2 = .09 (see Table 2 for mean absolute importance ratings as well as for comparative importance and behavioral intention ratings).
The experimentally induced focus (self vs other) did not affect any of the control variables (all F-values < 1). Also, including mean empathic concern and mean perceived stress as covariate into the analyses does not change results regarding comparative importance ratings as well as self-reported intentions regarding the “Five moments of hand hygiene”. However, it does slightly change the main effect of condition on absolute importance rating of each of the five moments from F(5,62) = 2.47, p = .042, partη2 = .17 to F(5,60) = 2.33, p = .053, partη2 = .16.
Likewise, including participants’ profession (nurse, physician, or other), participants’ gender and whether they had taken care of CVOID19 patients during the study period as control variable into analyses does not change results regarding comparative importance ratings as well as self-reported intentions regarding the “Five moments of hand hygiene”. However, it does slightly change the main effect of condition on absolute importance rating of each of the five moments from F(5,62) = 2.47, p = .042, partη2 = .17 to F(5,59) = 2.04, p = .086, partη2 = .15.
Discussion
In summary, these findings indicate that empathy can be employed to foster the motivation in healthcare professionals to comply with hand hygiene guidelines, especially those aimed at protecting patients (i.e., Moment 1 ‘before patient contact’ and Moment 2 ‘before aseptic task’). Thereby, these findings bear relevant policy implications, as they suggest that it is not enough to simply activate thoughts about infectious diseases (such as COVID-19), for instance, by providing comprehensive information or by instructing healthcare professionals adequately. Instead, the focus on others is needed to increase compliance with evidence-based guidelines for appropriate hand hygiene that are particularly aiming at shielding patients from potentially lethal infections. This is noteworthy, given that numerous intervention programs have been developed to improve HHC without differentiating between “before moments“ and “after moments” (e.g., Ellingson et al. 2014), although compliance differs between these types (Kingston et al. 2016, Wetzker et al. 2016).
Notably, the present findings result from an online experiment using self-reports. Moreover, the experimental intervention (inducing an empathic focus in the context of the present pandemic) was realized only for a short time. Accordingly, it is helpful to replicate these findings using different empathy-inductions and also involving healthcare professionals from various healthcare institutions to test generalizability. As an additional limitation of this study, it should be noted that there was no condition including a “no-focus instruction”, which would have represented a baseline condition for the present outcomes. Also, we only assessed psychological determinants of compliant behavior and not compliant behavior itself, which certainly represents a limitation given well-known gaps between knowledge, behavioral intentions, and actual behavior (Sheeran and Webb 2016). Put differently, measuring potential long-term consequences of (repeated) empathy inductions and assessing their effect on actual HHC calls for on-site intervention studies in the future. Nevertheless, it should also be acknowledged that during nationwide lockdowns, assessing healthcare workers’ thoughts and self-reported motivations and intentions online by self-report is as close as a researcher can get when aiming at investigating this specific and highly relevant population during a global pandemic.
Taken together, the current findings highlight the usefulness of empathy in developing tailored interventions, pointing a fruitful path for future tools to be implemented in healthcare settings to enhance patient safety in public healthcare.
Data availability
Data will be submitted as supplemental material.
Code availability
Not applicable.
References
Allegranzi B, Pittet D (2009) Role of hand hygiene in healthcare-associated infection prevention. J Hosp Infect 73:305–315. https://doi.org/10.1016/j.jhin.2009.04.019
Batson CD (2009) These things called empathy. In: Decety J, Ickes W (eds) The social neuroscience of empathy. MIT Press, Cambridge
Clancy C, Delungahawatta T, Dunne CP (2021) Hand hygiene-related clinical trials reported between 2014 and 2020: a comprehensive systematic review. J Hosp Infect 111:6–26. https://doi.org/10.1016/j.jhin.2021.03.007
Cohen S, Kamarck T, Mermelstein R (1983) Perceived stress scale (PSS). J Health Soc Behav 24:285–296. https://doi.org/10.2307/2136404
Davis MH (1983) Measuring individual differences in empathy: Evidence for a multidimensional approach. J Pers Soc Psych 44:113–126. https://doi.org/10.1037/0022-3514.44.1.113
Ellingson K, Haas JP, Aiello AE et al (2014) Strategies to prevent healthcare-associated infections through hand hygiene. Infect Control Hosp Epidemiol 35:937–960. https://doi.org/10.1086/677145
Gundersborg Sandbøl S, Glassou EN, Ellermann-Eriksen S, Haagerup A (2022) Hand hygiene compliance among healthcare workers before and during the COVID-19 pandemic. Am J Infect Control Mar 30 [Online ahead of print]. https://doi.org/10.1016/j.ajic.2022.03.014
Kingston L, O’Connell NH, Dunne CP (2016) Hand hygiene-related clinical trials reported since 2010: A systematic review. J Hosp Infect 92:309–320. https://doi.org/10.1016/j.jhin.2015.11.012
Mo Y, Pham TM, Lim C, Horby P et al (2022) The effect of hand hygiene frequency on reducing acute respiratory infections in the community: a meta-analysis. Epidemiol Infect 150(e79):1–8. https://doi.org/10.1017/S0950268822000516
Sassenrath C, Diefenbacher S, Siegel A, Keller J (2016) A person-oriented approach to hand hygiene behaviour: Emotional empathy fosters hand hygiene practice. Psych Health 31:205–227. https://doi.org/10.1080/08870446.2015.1088945
Sax H, Allegranzi B, Uckay I, Larson E, Boyce J, Pittet D (2007) ‘My five moments for hand hygiene’: a user-centred design approach to understand, train, monitor and report hand hygiene. J Hosp Infect 67:9–21. https://doi.org/10.1016/j.jhin.2007.06.004
Schreiber PW, Sax H, Wolfensberger A, Clack L, Kuster SP (2018) The preventable proportion of healthcare-associated infections 2005–2016: systematic review and meta-analysis. Infect Control Hosp Epidemiol 39:1277–1295. https://doi.org/10.1017/ice.2018.183
Sheeran P, Webb TL (2016) The intention–behavior gap. Soc Pers Psych Comp 10:503–518. https://doi.org/10.1111/spc3.12265
Stahmeyer JT, Lutze B, Von Lengerke T, Chaberny IF, Krauth C (2017) Hand hygiene in intensive care units: a matter of time? J Hosp Infect 95:338–343. https://doi.org/10.1016/j.jhin.2017.01.011
Tangney JP, Stuewig J, Mashek DJ (2007) Moral emotions and moral behavior. Annu Rev Psych 58:345–372. https://doi.org/10.1146/annurev.psych.56.091103.070145
Wetzker W, Bunte-Schonberger K, Walter J, Pilarski G, Gastmeier P, Reichard C (2016) Compliance with hand hygiene: reference data from the national hand hygiene campaign in Germany. J Hosp Infect 92:328–331. https://doi.org/10.1016/j.jhin.2016.01.022
World Health Organization (2009) WHO guidelines on hand hygiene in health care: First global patient safety challenge. Clean care is safer care. WHO, Geneva. http://whqlibdoc.who.int/publications/2009/9789241597906_eng.pdf. Accessed 6 May 2022
World Health Organization (2020) Infection prevention and control during health care when novel coronavirus (nCoV) infection is suspected. Interim Guidance 2020. WHO, Geneva. https://www.who.int/publications/i/item/10665-33149. Accessed 6 May 2022
Funding
Open Access funding enabled and organized by Projekt DEAL. The study was investigator initiated. The study was partially funded by BODE Chemie GmbH, a company of the HARTMANN group. Viktoria Kolbe and Heide Niesalla are employees of BODE Chemie GmbH.
Author information
Authors and Affiliations
Contributions
All authors substantially contributed to this manuscript. Claudia Sassenrath generated the research question, conceptualized and designed the study, analyzed and interpreted the data, and drafted the article. Svenne Diefenbacher contributed to design of the study, data acquisition as well as data interpretation, and to reviewing and editing of the manuscript draft. Viktoria Kolbe, Heide Niesalla, and Johannes Keller contributed to study design as well as to critically reviewing and editing of the manuscript with regard to important intellectual content. All authors approved of this final version of the manuscript to be submitted.
Corresponding author
Ethics declarations
Ethics approval
The survey did not need approval from an ethics committee because it did not meet the criteria for requiring an ethical statement (risk for the respondents, lack of information about the aims of the study, examination of patients). This rationale is supported by the German Research Foundation-guidelines available at https://www.dfg.de/en/research_funding/faq/faq_humanities_ social_ science/ index. html. The survey meets the ethical standards delineated in the 1964 Declaration of Helsinki and its amendments. The study was approved by hospital management and employee representation prior to implementation of the study.
Consent to participate
Participation in the study was contingent upon providing informed consent. Only participants who had read the study information and had given informed consent electronically were able to participate in the study.
Consent for publication
Not applicable.
Conflicts of interest/competing interests
Vikroria Kolbe and Heide Niesalla are employees of BODE Chemie GmbH.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sassenrath, C., Diefenbacher, S., Kolbe, V. et al. The impact of activating an empathic focus during COVID19 on healthcare workers motivation for hand hygiene compliance in moments serving the protection of others: a randomized controlled trial study. J Public Health (Berl.) 31, 1381–1385 (2023). https://doi.org/10.1007/s10389-022-01725-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-022-01725-z