
Abstract
Aim
In 1993, a study of 1000 automotive workers in Sweden and France looked into national differences of cardiovascular disease. Here, we evaluate the proportion of the Swedish cohort that suffered a stroke or died over a 25-year period and associated risk factors.
Subject and methods
Data from 1993 included a life-style questionnaire, a health examination and laboratory data. Figures on stroke and survival status up until the end of 2018 were collected from national registers. Survival analysis was used for both univariable and multivariable analyses to study associations between potential risk factors and stroke and death, respectively.
Results
By the end of 2018, 65 individuals had suffered a stroke and 160 had died. In the univariable analysis, we found age, systolic blood pressure, Framingham risk index and diabetes at baseline to be significantly associated with stroke during follow-up.
For death, most of the traditional risk factors were significantly associated with the outcome, as was blue-collar work and living alone. In the multivariable analysis, age and diabetes at baseline remained significantly associated with stroke, whereas eight factors (age, blue-collar work, living alone, systolic blood pressure, waist–hip ratio, smoking habits, diabetes and hypertension at baseline) were significantly associated with death during follow-up.
Conclusion
Few of the traditional risk factors were significantly associated with stroke possibly explained by low power and/or different pathogenetic mechanism than for myocardial infarction.
Partly because death occurred more often, we did find a number of potential risk factors to be significantly associated with this outcome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Stroke burden
Stroke is one of the leading causes of death worldwide (Donkor 2018). In 2017, the mean age for stroke among Swedish men was 74 years, unlike for women where it was 78, though every fifth stroke patient was under the age of 65 (Wester 2017). Stroke-incidence in 2017 included 251 women and 270 men per 100,000 inhabitants in Sweden (The Public Health Agency of Sweden 2017). In comparison, the corresponding figures for myocardial infarction were 192 women and 335 men per 100,000 inhabitants in Sweden (The Public Health Agency of Sweden 2020). However, over the past eight years, there has been a 17% decrease in both first-time stroke and recurrent stroke in Sweden, likely due to better control of risk factors (Riksstroke 2018).
Classification and pathophysiology
Stroke is defined by the World Health Organization (WHO) as ‘rapidly developed clinical signs of focal or global disturbance of cerebral function, lasting more than 24 hours or until death, with no apparent non-vascular cause’ (Aho et al. 1980). It is divided into subgroups: ischemic stroke (IS), accounting for approximately 85% of cases, and haemorrhagic stroke (HS), with the latter being further subdivided into intracerebral haemorrhage (ICH), approximately 10% of cases and subarachnoid bleeding (SAH) making up the remaining 5% (Wester 2017). Their origin slightly differs, which is why it could be important to differentiate between the subtypes for optimal prevention of risk factors.
Ischemic stroke can be caused by large-artery atherosclerosis, small-vessel disease or cardio embolism (Grau et al. 2001), wherein the latter case, atrial fibrillation is the most common source (Babkair 2017). In the study by Babkair (2017), atrial fibrillation exists in approximately 24% of stroke patients at the age of 80 (Babkair 2017). A less common method of stroke is by a deep venous thrombosis (DVT) travelling from a vein in the leg to the heart and through a patent foramen ovale (present in approximately 25% of the healthy population), entering the arterial circulation to end up in the cerebral vessels, obstructing the blood supply in that area (Sun Homma 2016).
The process of atherosclerosis may lead to a thicker intima wall, with a decrease in blood flow as a result. If the plaque is unstable, it can lead to a rupture with subsequent thrombosis, causing a block of the blood supply in that vessel, which occasionally can disseminate an embolus. If this process occurs in the carotid artery, the embolus would typically migrate to the middle cerebral artery leading to an IS in that area (Fig. 1). Small-vessel disease or so-called lacunar infarct is also caused by atherosclerosis but affects small vessels in the brain that lack collaterals (Wester 2017). Build-up of plaques is a reaction to high blood pressure, hypercholesterolemia or smoking, resulting in weakening of the vessel wall (Agewall et al. 2017). Individuals getting HS, or ICH in particular, usually have developed the atherosclerotic plaques as well, but usually also have additional risk factors increasing the risk for ICH, such as poorly regulated blood pressure, smoking, bleeding disturbances or anticoagulants, where high blood pressure is the single most important risk factor. SAH, on the other hand is often triggered by a ruptured aneurysm (Wester 2017).

With permission from the Mayo foundation. Illustration of the mechanism of an embolus dislodging from the carotid artery causing a stroke
Initial care and treatment
Of course, other potential differential diagnoses that can mimic stroke need to be considered and include epilepsy, hypoglycaemia, migraine, and more. Within 4-6 h from symptoms, patients with IS can be treated by thrombolysis or thrombectomy (Lambrinos et al. 2016; Wester 2017). In a systematic review of published trials by the Stroke Unit Trialists Collaboration (1997), patients treated in a specialised stroke unit showed better outcome compared to a general ward with fewer individuals dying from complications, fewer persons in need for institutional care thanks to improved functioning, and improved long-term survival (Collaboration 1997; Indredavik et al. 1997).
Post-stroke rehabilitation and costs
Stroke survivors often experience impact on cognitive ability, activities of daily living (ADL) function and on their capability of returning to work. According to a 2007 study by Hofgren et al., which included 58 patients younger than 65 years of age, only 20% of the post-stroke survivors had returned to profitable employment after three years (Hofgren et al. 2007). In 2004, Ghatnekar et al. showed that an average stroke patient in Sweden annually incurs direct and indirect costs of SEK 513,800 (59,473 USD) plus SEK 125,110 (14,482 USD), respectively, with social services accounting for the major portion of the direct cost. Additional aspects included the cost of rehabilitation, drugs, in-patient care and loss of production cost because of early death or retirement (Ghatnekar et al. 2004). Considering our growing proportion of elderly, it is of great importance to emphasise the denotation of preventive factors (Hallstrom et al. 2008).
Risk factors and prevention
Common, well-known modifiable risk factors for stroke are hypertension, smoking, diabetes mellitus, atrial fibrillation, physical inactivity, high blood lipids and high alcohol intake (Yew Cheng 2015). In 2016, the INTERSTROKE case-control study performed in 32 countries, analysed these risk factors together with some additional variables, including waist-to-hip ratio, diet risk score, psychosocial stress and depression, and found ten potentially modifiable risk factors accounting for 90% of the population-attributable risk for all stroke (O'Donnell et al. 2016). Over the past two decades, a decline in stroke mortality has been observed in the United States of America. This is associated with better control of risk factors, especially cigarette smoking, blood pressure, blood lipids and diabetes. This trend was already visible in the 1970s when the anti-hypertensive drug treatment revolutionised the market (Lackland et al. 2014).
Background to this project
In 1993, a study of 1000 automotive workers in Sweden (Volvo) and France (Renault) looked into national differences of cardiovascular disease (Simon et al. 1997). In 2015, we reached out to the Volvo cohort with a health survey and collected Swedish register data on myocardial infarction (MI) and mortality over 22 years (Hashem 2017). That study examined the incidence of MI and mortality, and their association with certain risk factors. The result implied that MI and mortality were strongly, positively associated with Framingham risk index (FRI) at baseline. Pulse rate, blood pressure, BMI smoking and diabetes also showed significant associations with both MI and death. The study indicated an increased risk of death for manual workers, while education, being married or cohabiting, number of children and having a partner working outside the home, were independently associated with a lower risk of death (Dimberg et al. 2019).
Occupational health departments have a unique position to develop methods to identify and advise on risk factor prevention. The present study will examine the Swedish cohort of automotive workers, to find the 25-year incidence of stroke and death and some associated risk factors.
Objectives
The aim of this study is to explore certain modifiable risk factors associated with stroke and death in order to target them for prevention.
Methods
Participants
The present study commenced in 1993 as a prospective longitudinal French–Swedish cohort study and builds on the Swedish cohort which includes a random selection of 1000 45–50-year-old men working in the automotive industry. Simon et al. (1997) describe the original project and the data collection and rigorous methods in a previous paper (Simon et al. 1997).
We now present on a 25-year follow-up to evaluate the cumulative incidence of first stroke or death and some associated risk factors through 2018.
1993, health examinations and questionnaire
The recruited men were invited to a nurse-led health examination, including certain blood tests, blood pressure, anthropometrics and ECG. Furthermore, they completed a self-administered questionnaire containing questions on cardiovascular risk factors, lifestyle, working conditions, demographics, social and psychological factors. The examinations occurred at the occupational health department at their workplace during working hours.
Variables
The questions answered at baseline that were included in this survey are: age; blue-collar worker (manual work) or white-collar worker (clerical work); education: elementary school, high school, university; marital status: married or cohabitant/divorced/single; number of children; family history of diabetes or stroke; hypertension at baseline defined as a blood pressure > 140/90 mmHg; alcohol intake in g/week calculated and adjusted by the size of the glass as follows: 1 glass of beer = 6 g, 1 glass of wine = 12 g, 1 glass of distilled spirit = 13 g; smoking (yes/no) with the question defined as ‘do you smoke at least one cigarette per day for the last three months?’; noisy work environment defined as ‘Is it too noisy to be able to talk to fellow workers at your work-site?’. The measurements and blood samples taken into account were systolic and diastolic blood pressure in mmHg, pulse rate in beats/min, total serum cholesterol and serum high-density lipoprotein cholesterol (HDL-C) in mmol/l, TGs in mmol/l, fasting blood glucose in mmol/l, height in cm, weight in kg, waist-to-hip ratio and sagittal abdominal diameter in cm. All of these measurements are described in detail elsewhere (Simon et al. 1997). Body mass index (BMI) in kg/m2 was calculated, and the FRI, which was based on the subsequent variables, left ventricular hypertrophy, diabetes, smoking, age, systolic blood pressure and total/HDL cholesterol ratio, according to Anderson (Anderson et al. 1991).
The clinical end-point data of stroke were acquired from the national quality register of stroke care, Riksstroke, which started in 1994. Diagnoses of atrial fibrillation were also obtained from the stroke register. Death as end-point data was collected from the Swedish mortality register. In addition, data on first myocardial infarction (MI) was obtained from the National Swedish Register of coronary care, Swedeheart (Dimberg et al., 2019). Codes for stroke according to the International Statistical Classification of diseases-10th edition, (ICD-10) include I60-66.
Statistical analyses
Exact (Clopper–Pearson) confidence limits were caluclated for selected proportions in Table 1. Cumulative rates of any stroke and of death were estimated with the Kaplan–Meier method, where for stroke patients who died without having suffered a stroke (earlier or as the cause of death) were censored at the time of death. Hazard ratios (HR) with corresponding confidence intervals were calculated using Cox proportional hazards regression model. The Kent and O’Quigley measure of dependence (R-squared measure) was used to estimate explained variation.
The variable glycaemia did not fulfil the linearity assumption for the Cox regression; therefore, natural logarithm transformed values were used in the analysis. Collinearity was present between systolic and diastolic blood pressure and the latter therefore was excluded from the multivariable analysis. All other variables with a univariable p < 0.20 for association were included in the multivariable analysis of identifying independent predictors of stroke and death, respectively, using Cox proportional hazards model in a stepwise backward selection mode with p < 0.05 for staying in the model.
All tests were two-sided and p values below 0.05 were considered statistically significant. Analysis was performed using SAS for Windows version 9.4.
Variable definitions
Outcomes, endpoints (dependent variable):
Deaths reported, 160 persons
First stroke reported, 65 persons.
Explanatory (independent) variables, components of Framingham risk index:
Systolic blood pressure (mmHg)
Smoking (Yes/No)
HDL cholesterol/ Tot cholesterol
Left ventricular hypertrophy (examined by ECG)
Age
Diabetes (Yes/No).
Additional explanatory variables
Diastolic blood pressure (mmHg)
Heart rate (beats/min)
Triglycerides (mmol/l)
Glycaemia (mmol/l)
Body mass index, BMI(kg/m2)
Waist/hip ratio
Sagittal abdominal diameter (cm)
Total alcohol consumption (g/week)
Blue-Collar Workers (Yes/No)
Married or cohabiting (Yes/No)
University education (Yes/No)
Noisy work environment (Yes/No)
Hypertension (Yes/No)
Family diabetes (Yes/No)
Family stroke (Yes/No).
Results
In total, 999 men out of the 1000 enrolled, were included and analysed in this study. No data exists for 1 person. Out of the participants (Table 1), a larger proportion (61%) performed clerical work at Volvo and were married/living together (76%). Almost one third were smokers at baseline (28%). The average Framingham risk-index score was 0.09 compared to 0.10 in the group that suffered a stroke, 10% had hypertension, and 1 % had diabetes.
Over the 25 years, according to the national stroke registry 65 persons suffered at least one stroke and the national death registry showed 160 men had died. As evident in Table 1, the mean systolic and diastolic blood pressure at baseline were significantly higher in the stroke group than in the participants free of stroke, but still within normal ranges. The mean value for the systolic blood pressure was 120 compared to 117 in the group free of stroke and the diastolic blood pressure was 77 compared to 75, respectively. One could also observe a significantly higher proportion of diabetes (4.9%) in the stroke group (p value 0.041 with Fisher’s exact test) compared to the group not suffering a stroke (1%) and a higher proportion in the stroke group having blue-collar work (46 versus 39%) and being married/cohabitant (82 to 76%). Anthropometric variables and the following laboratory data: total cholesterol, HDL-cholesterol, triglycerides and glycaemia were similar between those who had suffered a stroke and those who remained free of stroke during the 25-year observation period. Please note that the number of end-points and number of variables differ slightly in the Tables owing to missing information for some of the variables.
Table 2 presents the distribution of stroke types, with brain infarction occurring most frequently (87%). Out of the 57 people suffering a cerebral infarction, 18 people (33%) had atrial fibrillation at the time of the event.
The mean age of men with a first stroke was 67 years, which is significantly higher than that of a first MI, 63 years Table 3.
Hazard ratio for stroke was significantly elevated with age, systolic blood pressure, Framingham’s risk index and diabetes at baseline as shown in Table 4. Most traditional cardiovascular risk variables, however, displayed significantly elevated HRs for death. In the multivariable analyses (Table 5), only age and diabetes at baseline remained significantly associated with stroke. As for death, the strongest positive associations were seen with diabetes (HR = 4.1) and being a smoker (HR = 2.2). Negative associations were seen for being married/cohabitant (HR = 0.5).
Table 6 presents the continuous variables with stroke as end-point where the FRI displays a tendency of a J-shaped curve over the quintiles and so does the pulse rate. No anthropometric variables reached statistical significance.
Table 7 has the same arrangement as Table 6 but with death as end-point.
Statistically significant HRs are seen for the FRI, systolic and diastolic blood pressure, pulse rate, sagittal abdominal diameter/height and waist/hip ratio. A negative association was seen between alcohol and death.
The dichotomous variables and their relation to incidence of stroke or death are shown in Table 8. As for stroke, only diabetes was shown as a significant factor, with a family history of stroke only reaching borderline significance. Contrary to stroke, death as clinical end-point had many significant variables with the strongest being diabetes (OR = 9), smoking (OR = 2.5) and manual work (OR = 2.0). Among the smokers, 6.6% had a stroke and 25% died, compared to the whole population where 6.4% had a stroke and 16% died. Interestingly several variables were negatively associated (possibly protective) with death, but not with stroke: high school (OR = 0.5) and university education (OR = 0.6), being married (OR = 0.5) and having a wife that works outside of home (OR = 0.6).
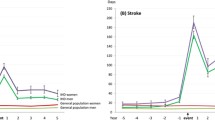
Figure 2 illustrates the cumulative incidence over time, indicating an increase of stroke starting after 10 years (ages 55–60) compared to deaths occurring over a wider time period.

Cumulative incidence of first stroke (n=65) and death (n=160) in the cohort of middle-aged men (n=999) over 25 years
Discussion
Main findings
It should be emphasised that 30% (19/65) of the stroke patients suffered from atrial fibrillation (Table 2). This is a well-known cause of ischemic stroke. Unfortunately, we have no knowledge of the cumulative incidence of this condition in the entire cohort. A recent Swedish study of a similar age group of men suggests an accumulated incidence of 4% (Lindberg et al. 2019). This figure applied to our population would thus give an OR of atrial fibrillation in stroke of 10.5 (95% CI 5.59–19.7), p < 0.0001. Atrial fibrillation is one of ten potentially modifiable risk factors presented in the INTERSTROKE study by O’Donnell and colleagues (O'Donnell et al. 2016).
One of the findings in this study was the significant difference in mean systolic and diastolic blood pressure between the group who had a stroke and those who did not (Table 1). Interestingly, both of these groups were within normal blood pressure ranges; however, this finding lost significance after multivariable analyses (Table 5). An article published in 2017 by Li et al. looked at different blood pressure ranges and the risk for developing a stroke. In this study with nearly 80,000 participants, they observed much higher incidence of strokes in participants with prehypertension (120–140 mmHg) compared to normotensive persons (100–120 mmHg) (Li et al. 2017). This may suggest that the normotensive limit is perhaps set too high.
An important finding in this study was the weak association of traditional risk factors with stroke. When comparing the fifth and first quintile, significant findings were seen for systolic and diastolic blood pressure, but not for the FRI or any other studied risk factor. Only diabetes and age stood out as statistically significant after multivariable analysis. This may of course be due to the limited number of end-points (n = 65). However, our previous study of this cohort on myocardial infarction (n = 89) showed a strong prediction of many traditional cardiovascular risk factors (Dimberg et al. 2019).
An alternate explanation could be that the predictive power of traditional risk factors is weaker for stroke than for myocardial infarction. This theory is supported by a recent study by Giang and colleagues who have followed middle-aged Swedish men for 35 years and concluded that traditional risk factors can effectively be used to predict coronary heart disease but not stroke to the same extent (Giang et al. 2013).
In the physician’s health study (PHS), Glynn and Rosner (2005), compared the risk factor profile for coronary heart disease, stroke and venous thromboembolism in 18,662 male US physicians followed for 20 years. They found the risk factors for stroke and CHD relatively similar, though hypertension and diabetes mellitus had a slightly bigger impact on stroke, whereas cholesterol had a greater influence on CHD (Glynn and Rosner 2005).
They also observed the increase in these outcomes with age with different curves. The incidence of stroke was higher in the age range of 70–79, whereas CHD was more common in the age range of 60–69. The oldest men in our cohort were 75 years at follow-up, and according to the PHS, the age range where most strokes take place is between 70 and 79.
There was a significant positive association with diabetes and stroke. This was rather expected because diabetes and stroke have been well researched (Kannel McGee 1979). Having diabetes is also linked to worse clinical outcomes following a stroke (Chen et al. 2016; Hill 2014). Taking into consideration the growing population of seniors and the fact that a higher proportion are becoming obese, the incidence of diabetes is likely to increase. The American Heart Association forecast a 69% increase in diabetes in developed countries by 2030 (Heidenreich et al. 2011). Consequently, despite the decrease in stroke rates the past decade, an increase is imminent unless prevention of risk factors is intensified.
In our study, most traditional cardiovascular risk variables displayed significantly elevated HRs for death. One variable that did not reach significance was BMI. Interestingly, the third quintile has the lowest odds for both stroke and death. The persons included in the third quintile are those with a BMI of 25–26, where 24.9 is the upper normal limit. It is controversial whether overweight (defined as a BMI of 25–29.9) is related to an increase or decrease in all-cause mortality. An article by Lin et al. showed that the risk of death was lowest for those with a BMI of 24.0–25.9, similar to our findings, often called the obesity paradox (Lin et al. 2011). Still, another study comparing overweight and obesity to normal weight revealed an increase in total mortality (Batty et al. 2006).
Potentially protective factors with death in this study was high school and university education, being married and alcohol intake (Table 8). In a study conducted in 2008 by Kohler et al., educational level and marital status and their association with death were studied by observing death records and census records in the three countries Bulgaria, Finland and the United States. Kohler et al. concluded that a high level of education and being married are both correlated with decreased mortality (Kohler et al. 2008). For decades, the link between a lower level of education and mortality has been discussed (Kohler et al. 2008; Pappas et al. 1993).
Another exciting connection is the negative correlation between alcohol (g/week) and mortality, which reached statistical significance. Looking at Table 6, the odds for mortality decreases for almost every quintile, indicating that the greater amount of alcohol, the lower is the odds for death. Whether alcohol has a positive or negative liaison with death and if the amount of alcohol matters has been discussed back and forth in many studies (Breslow Graubard 2008; Dawson 2000; Mukamal et al. 2010; Xi et al. 2017). However, most studies agree upon the harmful effects of heavy drinking or binge drinking (Mukamal et al. 2010; Xi et al. 2017).
Strength and weaknesses
The original cohort was randomly selected from a well-defined population of male workers followed over a very long time (25 years). Very few rejected to participate. The nurses and health professionals were specially trained and well-defined methods were used. The procedures for baseline information acquisition were carefully developed based on current standards (Simon et al. 1997). Accurate information about the end-points was available through national registers with quality control to contain valid data. The internal validity of the study and its results havebeen carefully secured throughout.
Thorough statistical analyses using multivariable techniques and adjustments is another strength.
An additional value was the great enthusiasm from the participants to be a part of this study, which resulted in good compliance. The fact that the interview and examination took place at the occupational clinic at the workplace during working hours was also helpful. Nevertheless, there is some limitation to the stroke register (Riksstroke), which started in 1994, but did not include all the hospitals in Sweden until 1998, which means that there is a possibility that some strokes that happened early on in the study are not registered. The external validity, i.e. validity for other populations with other contextual structures is clearly limited because the study is confined to men in a certain age range in a particular industry and a certain country.
Confounding factors and biases
Confounding factors that limit this study include not taking into account the possibility of the participants’ behaviour to change over time. Perhaps some of the men quit smoking or started to smoke, had changes in blood pressure over time, started with medication for hypertension or high cholesterol, altered their alcohol habits, or gained or lost weight. In any of these cases, the baseline data would not be reliable to analyse. Although we do not have secular, longitudinal data of the 25-year period, the findings presented in another longitudinal Swedish study of 50-year old men followed for 50 years shows secular changes (smoking less, lower cholesterol but higher BMI and a more sedentary lifestyle) in cardiovascular risk factors over time that are likely to apply to our cohort (Zhong et al. 2017). Furthermore, addition of medication during this period may have changed the prognosis of some endpoints.
There are also always risks for biases, particularly when some questions are self-reported. For example, people tend to underestimate their drinking habits. There is also a possibility that laboratory results are not accurate due to incorrect calibrations, although every reasonable attempt to standardise the equipment and to use hospital laboratories with certified quality control was made. In addition, there may be typing errors upon entering the data despite the double control by the nurses.
Conclusions
Few of the traditional risk factors stood out as significant for stroke. The risk factors that did reach significance after multivariable testing were age and diabetes. Opposite to MI, earlier studied in the same cohort, stroke did not show the same association with traditional risk factors. This finding may be due to low statistical power but does not contradict the theory that many traditional risk factors have a lower specific weight for stroke compared to CHD. However, for death, most of the well-established risk factors reached statistical significance. Additional research is needed to further investigate whether the traditional risk factors for CVD really are applicable for stroke to the same extent.
Availability of data and material
Data would be available upon request.
References
Agewall S, Gottsäter A, Svensson P J (2017) Ateroskleros och trombogenes. In Medicin (2nd edn., pp 24–27). Studentlitteratur AB, Lund
Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T (1980) Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ 58(1):113–130
Anderson KM, Wilson PW, Odell PM, Kannel WB (1991) An updated coronary risk profile. A statement for health professionals. Circulation 83(1):356–362. https://doi.org/10.1161/01.cir.83.1.356
Babkair LA (2017) Cardioembolic stroke: a case study. Crit Care Nurse 37(1):27–39. https://doi.org/10.4037/ccn2017127
Batty GD, Shipley MJ, Jarrett RJ, Breeze E, Marmot MG, Davey Smith G (2006) Obesity and overweight in relation to disease-specific mortality in men with and without existing coronary heart disease in London: the original Whitehall study. Heart 92(7):886–892. https://doi.org/10.1136/hrt.2005.072637
Breslow RA, Graubard BI (2008) Prospective study of alcohol consumption in the United States: quantity, frequency, and cause-specific mortality. Alcohol Clin Exp Res 32(3):513–521. https://doi.org/10.1111/j.1530-0277.2007.00595.x
Chen R, Ovbiagele B, Feng W (2016) Diabetes and stroke: epidemiology, pathophysiology, pharmaceuticals and outcomes. Am J Med Sci 351(4):380–386. https://doi.org/10.1016/j.amjms.2016.01.011
Collaboration SUT (1997) How do stroke units improve patient outcomes? A collaborative systematic review of the randomized trials. Stroke Unit Trialists Collaboration. Stroke 28(11):2139–2144. https://doi.org/10.1161/01.str.28.11.2139
Dawson DA (2000) Alcohol consumption, alcohol dependence, and all-cause mortality. Alcohol Clin Exp Res 24(1):72–81
Dimberg L, Eriksson B, Hashem M (2019) Myocardial infarction and death findings from a 22-year follow-up of a cohort of 980 employed Swedish men. Public Health 175:148–155. https://doi.org/10.1016/j.puhe.2019.07.006
Donkor ES (2018) Stroke in the 21(st) century: a snapshot of the burden, epidemiology, and quality of life. Stroke Res Treat 2018:3238165. https://doi.org/10.1155/2018/3238165
Ghatnekar O, Persson U, Glader EL, Terent A (2004) Cost of stroke in Sweden: an incidence estimate. Int J Technol Assess Health Care 20(3):375–380
Giang KW, Björck L, Novak M, Lappas G, Wilhelmsen L, Torén K, Rosengren A (2013) Stroke and coronary heart disease: predictive power of standard risk factors into old age--long-term cumulative risk study among men in Gothenburg, Sweden. Eur Heart J 34(14):1068–1074. https://doi.org/10.1093/eurheartj/ehs458
Glynn RJ, Rosner B (2005) Comparison of risk factors for the competing risks of coronary heart disease, stroke, and venous thromboembolism. Am J Epidemiol 162(10):975–982. https://doi.org/10.1093/aje/kwi309
Grau AJ, Weimar C, Buggle F, Heinrich A, Goertler M, Neumaier S, Glahn J, Brandt T, Hacke W, Diener HC (2001) Risk factors, outcome, and treatment in subtypes of ischemic stroke: the German stroke data bank. Stroke 32(11):2559–2566. https://doi.org/10.1161/hs1101.098524
Hallstrom B, Jonsson AC, Nerbrand C, Norrving B, Lindgren A (2008) Stroke incidence and survival in the beginning of the 21st century in southern Sweden: comparisons with the late 20th century and projections into the future. Stroke 39(1):10–15. https://doi.org/10.1161/strokeaha.107.491779
Hashem M (2017) Heart attacks, mortality, and cardiovascular risk factors - a 22 year follow-up of 1,000 men of the Swedish cohort of the Volvo-Renault Coeur project looking into the French paradox. University of Gothenburg, Masters Dissertation
Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD, Finkelstein EA, Hong Y, Johnston SC, Khera A, Lloyd-Jones DM, Nelson SA, Nichol G, Orenstein D, Wilson PW, Woo YJ (2011) Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation 123(8):933–944. https://doi.org/10.1161/CIR.0b013e31820a55f5
Hill MD (2014) Stroke and diabetes mellitus. Handb Clin Neurol 126:167–174. https://doi.org/10.1016/b978-0-444-53480-4.00012-6
Hofgren C, Björkdahl A, Esbjörnsson E, Sunnerhagen KS (2007) Recovery after stroke: cognition, ADL function and return to work. Acta Neurol Scand 115(2):73–80. https://doi.org/10.1111/j.1600-0404.2006.00768.x
Indredavik B, Slordahl SA, Bakke F, Rokseth R, Haheim LL (1997) Stroke unit treatment. Long-term effects. Stroke 28(10):1861–1866. https://doi.org/10.1161/01.str.28.10.1861
Kannel WB, McGee DL (1979) Diabetes and cardiovascular disease. The Framingham study. Jama 241(19):2035–2038. https://doi.org/10.1001/jama.241.19.2035
Kohler IV, Martikainen P, Smith KP, Elo I. T (2008) Educational differences in all-cause mortality by marital status - evidence from Bulgaria, Finland and the United States. Demogr Res 19(10):2011–2042. https://doi.org/10.4054/demres.2008.19.60
Lackland DT, Roccella EJ, Deutsch AF, Fornage M, George MG, Howard G, Kissela BM, Kittner SJ, Lichtman JH, Lisabeth LD, Schwamm LH, Smith E, Towfighi A (2014) Factors influencing the decline in stroke mortality: a statement from the American Heart Association/American Stroke Association. Stroke 45(1):315–353. https://doi.org/10.1161/01.str.0000437068.30550.cf
Lambrinos A, Schaink AK, Dhalla I, Krings T, Casaubon LK, Sikich N, Lum C, Bharatha A, Pereira VM, Stotts G, Saposnik G, Kelloway L, Xi X, Hill MD (2016) Mechanical Thrombectomy in acute ischemic stroke: a systematic review. Can J Neurol Sci 43(4):455–460. https://doi.org/10.1017/cjn.2016.30
Li W, Jin C, Vaidya A, Wu Y, Rexrode K, Zheng X, Gurol ME, Ma C, Wu S, Gao X (2017) Blood pressure trajectories and the risk of intracerebral hemorrhage and cerebral infarction: a prospective study. Hypertension 70(3):508–514. https://doi.org/10.1161/hypertensionaha.117.09479
Lin WY, Tsai SL, Albu JB, Lin CC, Li TC, Pi-Sunyer FX, Sung PK, Huang KC (2011) Body mass index and all-cause mortality in a large Chinese cohort. Cmaj 183(6):E329–E336. https://doi.org/10.1503/cmaj.101303
Lindberg T, Wimo A, Elmståhl S, Qiu C, Bohman DM, Sanmartin Berglund J (2019) Prevalence and Incidence of Atrial Fibrillation and Other Arrhythmias in the General Older Population: Findings From the Swedish National Study on Aging and Care. Gerontol Geriatr Med 5:2333721419859687. https://doi.org/10.1177/2333721419859687
Mukamal KJ, Chen CM, Rao SR, Breslow RA (2010) Alcohol consumption and cardiovascular mortality among U.S. adults, 1987 to 2002. J Am Coll Cardiol 55(13):1328–1335. https://doi.org/10.1016/j.jacc.2009.10.056
O'Donnell MJ, Chin SL, Rangarajan S, Xavier D, Liu L, Zhang H, Rao-Melacini P, Zhang X, Pais P, Agapay S, Lopez-Jaramillo P, Damasceno A, Langhorne P, McQueen MJ, Rosengren A, Dehghan M, Hankey GJ, Dans AL, Elsayed A et al (2016) Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet 388(10046):761–775. https://doi.org/10.1016/s0140-6736(16)30506-2
Pappas G, Queen S, Hadden W, Fisher G (1993) The increasing disparity in mortality between socioeconomic groups in the United States, 1960 and 1986. N Engl J Med 329(2):103–109. https://doi.org/10.1056/nejm199307083290207
Simon A, Dimberg L, Levenson J, Lanoiselee C, Massonneau M, Eriksson B, Jern S, Kumlin L, Marin P, Dahlof B, Hansson L, Bjorntorp P (1997) Comparison of cardiovascular risk profile between male employees of two automotives companies in France and Sweden. The Coeur project group. Eur J Epidemiol 13(8):885–891. https://doi.org/10.1023/a:1007428624757
Sun YP, Homma S (2016) Patent foramen Ovale and stroke. Circ J 80(8):1665–1673. https://doi.org/10.1253/circj.CJ-16-0534
Wester P (2017) Cerebrovaskulära sjukdomar. In Medicin (2nd edn., pp 50, 52, 62, 65, 66, 68–71 ). Studentlitteratur AB, Lund
Xi B, Veeranki SP, Zhao M, Ma C, Yan Y, Mi J (2017) Relationship of alcohol consumption to all-cause, cardiovascular, and Cancer-related mortality in U.S. adults. J Am Coll Cardiol 70(8):913–922. https://doi.org/10.1016/j.jacc.2017.06.054
Yew KS, Cheng EM (2015) Diagnosis of acute stroke. Am Fam Physician 91(8):528–536
Zhong Y, Rosengren A, Fu M, Welin L, Welin C, Caidahl K, Mandalenakis Z, Dellborg M, Svärdsudd K, Hansson PO (2017) Secular changes in cardiovascular risk factors in Swedish 50-year-old men over a 50-year period: the study of men born in 1913, 1923, 1933, 1943, 1953 and 1963. Eur J Prev Cardiol 24(6):612–620. https://doi.org/10.1177/2047487316676905
Acknowledgments
We appreciate the qualified help with the statistical calculations by Thomas Karlsson, Biostatistics, School of Public Health and Community Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden. This work stands on the shoulders of previous work by the Coeur project group (appendix 1), and more recently by the much-appreciated work by Mohammed Hashem.
The eminent Gunnar L Johansson, former president of the Volvo Corporation supported the Coeur project from its inception in 1993 and secured the finances for the Swedish branch of this bilateral project through 1998.
Our gratitude also extends to Ms. Rosemary Perry at the Mayo clinic for her quick response and the permission to use their picture (Fig. 1) in this article.
Funding
The Volvo branch of the original Renault-Volvo Coeur project was financed by a grant from the Volvo Research Foundation in 1992 H92:37. The enterprises had no influence on the interpretation of the data.
Author information
Authors and Affiliations
Contributions
IT conceived of the study and drafted the first manuscript.
LD supervised the project continually, read and critiqued the manuscript. Both authors formulated the statistical analyses plan in close collaboration with a hired statistics consultant and discussed the results based on the processed data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. The Research Ethics Committee of Gothenburg University approved the original study protocol and the consent to participate form on 11 February 1993 (Dnr. 23-93). The Research Ethics Committee of Gothenburg University renewed their approval of an amended study protocol on 19 February 2019 (Dnr1212-18/2019-00316).
Consent to participate
This study builds on register data so the Ethics Committee waived specific consent.
Consent for publication
All participants of the baseline study in 1993 were informed that only aggregated data would be published and agreed upon publication.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 15 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Torenfält, I., Dimberg, L. Stroke and death-findings from a 25-year follow-up of a cohort of employed Swedish middle-aged men of the Coeur study. J Public Health (Berl.) 30, 1713–1724 (2022). https://doi.org/10.1007/s10389-021-01667-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-021-01667-y