
Abstract
Background
Postoperative morbidity after esophagectomy for esophageal cancer is still frequent. Tools for prediction of postoperative complications have been sought, with the estimation of physiologic ability and surgical stress (E-PASS) scoring system being one of the candidates. The aim of this study was to determine the usefulness of the E-PASS system for risk assessment of esophagectomy.
Methods
The clinical courses of 308 patients who underwent elective subtotal esophagectomy with lymph node dissection for esophageal cancer were analyzed. The incidence and severity of complication and influence of preoperative therapy were investigated using the E-PASS system.
Results
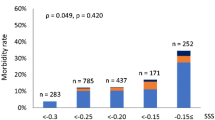
The incidence of any complication was as high as 42.2 %. The frequency of severe and critical complications was 13.0 and 6.8 %, respectively. The E-PASS system could estimate the incidence and severity of complications. Patients with a comprehensive risk score (CRS) >0.9 had a significantly higher probability of incidence of severe or critical complications. The incidence of complication and the CRS increased linearly according to preoperative treatment in the following order: no preoperative treatment < neoadjuvant chemotherapy < neoadjuvant chemoradiotherapy < definitive chemoradiotherapy. These were significantly higher after salvage esophagectomy.
Conclusion
The E-PASS scoring system was useful for risk assessment after esophagectomy. Patients with a CRS >0.9 and patients undergoing salvage esophagectomy should be treated carefully after surgery. Among two scoring systems of which the CRS consisted, the surgical stress score strongly correlated with postoperative complications after esophagectomy, but the preoperative risk score did not.




Similar content being viewed by others

References
Bakhos CT, Fabian T, Oyasiji TO, Gautam S, Gangadharan SP, Kent MS, et al. Impact of the surgical technique on pulmonary morbidity after esophagectomy. Ann Thorac Surg. 2012;93:221–6.
Schieman C, Wigle DA, Deschamps C, Nichols Iii FC, Cassivi SD, Shen KR, et al. Patterns of operative mortality following esophagectomy. Dis Esophagus. 2012;25:645–51.
Ferguson MK, Celauro AD, Prachand V. Assessment of a scoring system for predicting complications after esophagectomy. Dis Esophagus. 2011;24:510–5.
Paul DJ, Jamieson GG, Watson DI, Devitt PG, Game PA. Perioperative risk analysis for acute respiratory distress syndrome after elective oesophagectomy. ANZ J Surg. 2011;81:700–6.
Valentí V, Hernández-Lizoain JL, Marínez-Regueira F, Bellver M, Rodríguez J, Díaz González JA, et al. Transthoracic oesophagectomy with lymphadenectomy in 100 oesophageal cancer patients: multidisciplinary approach. Clin Transl Oncol. 2011;13:899–903.
Dutta S, Al-Mrabt NM, Fullarton GM, Horgan PG, McMillan DC. A comparison of POSSUM and GPS models in the prediction of post-operative outcome in patients undergoing oesophago-gastric cancer resection. Ann Surg Oncol. 2011;18:2808–17.
Grotenhuis BA, van Hagen P, Reitsma JB, Lagarde SM, Wijnhoven BP, van Berge Henegouwen MI, et al. Validation of a nomogram predicting complications after esophagectomy for cancer. Ann Thorac Surg. 2010;90:920–5.
Dhungel B, Diggs BS, Hunter JG, Sheppard BC, Vetto JT, Dolan JP. Patient and peri-operative predictors of morbidity and mortality after esophagectomy: American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP), 2005–2008. J Gastrointest Surg. 2010;14:1492–501.
Wright CD, Kucharczuk JC, O’Brien SM, Grab JD, Allen MS. Predictors of major morbidity and mortality after esophagectomy for esophageal cancer: a Society of Thoracic Surgeons General Thoracic Surgery Database risk adjustment model. J Thorac Cardiovasc Surg. 2009;137:587–95.
Lagarde SM, Reitsma JB, Maris AK, van Berge Henegouwen MI, Busch OR, Obertop H, et al. Preoperative prediction of the occurrence and severity of complications after esophagectomy for cancer with use of a nomogram. Ann Thorac Surg. 2008;85:1938–45.
Thompson AM, Rapson T, Gilbert FJ, Park KG. Hospital volume does not influence long-term survival of patients undergoing surgery for oesophageal or gastric cancer. Br J Surg. 2007;94:578–84.
Rodgers M, Jobe BA, O’Rourke RW, Sheppard B, Diggs B, Hunter JG. Case volume as a predictor of inpatient mortality after esophagectomy. Arch Surg. 2007;142:829–39.
Sunpaweravong S, Ruangsin S, Laohawiriyakamol S, Mahattanobon S, Geater A. Prediction of major postoperative complications and survival for locally advanced esophageal carcinoma patients. Asian J Surg. 2012;35:104–9.
Grotenhuis BA, Wijnhoven BP, Grüne F, van Bommel J, Tilanus HW, van Lanschot JJ. Preoperative risk assessment and prevention of complications in patients with esophageal cancer. J Surg Oncol. 2010;101:270–8.
Noble F, Curtis N, Harris S, Kelly JJ, Bailey IS, Byrne JP, et al. Risk assessment using a novel score to predict anastomotic leak and major complications after oesophageal resection. J Gastrointest Surg. 2012;16:1083–95.
Ando N, Kato H, Igaki H, Shinoda M, Ozawa S, Shimizu H, et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (JCOG9907). Ann Surg Oncol. 2012;19:68–74.
Haga Y, Ikei S, Ogawa M. Estimation of physiologic ability and surgical stress (E-PASS) as a new prediction scoring system for postoperative morbidity and mortality following elective gastrointestinal surgery. Surg Today. 1999;29:219–25.
Copeland GP, Jones D, Walters M. POSSUM: a scoring system for surgical audit. Br J Surg. 1991;78:355–60.
McMillan DC. An inflammation-based prognostic score and its role in the nutrition-based management of patients with cancer. Proc Nutr Soc. 2008;67:257–62.
Baba Y, Haga Y, Hiyoshi Y, Imamura Y, Nagai Y, Yoshida N, et al. Estimation of physiologic ability and surgical stress (E-PASS system) in patients with esophageal squamous cell carcinoma undergoing resection. Esophagus. 2008;5:81–6.
Haga Y, Wada Y, Takeuchi H, Ikejiri K, Ikenaga M, Kimura O. Evaluation of modified estimation of physiologic ability and surgical stress in gastric carcinoma surgery. Gastric Cancer. 2012;15:7–14.
Haga Y, Wada Y, Ikenaga M, Takeuchi H, Ikejiri K. Evaluation of modified estimation of physiologic ability and surgical stress in colorectal carcinoma surgery. Dis Colon Rectum. 2011;54:1293–300.
Hashimoto D, Takamori H, Sakamoto Y, Ikuta Y, Nakahara O, Furuhashi S, et al. Is an estimation of physiologic ability and surgical stress able to predict operative morbidity after pancreaticoduodenectomy? J Hepatobiliary Pancreat Sci. 2010;17:132–8.
Hashimoto D, Takamori H, Sakamoto Y, Tanaka H, Hirota M, Baba H. Can the physiologic ability and surgical stress (E-PASS) scoring system predict operative morbidity after distal pancreatectomy? Surg Today. 2010;40:632–7.
Watanabe M, Nagai Y, Kinoshita K, Saito S, Kurashige J, Karashima R, et al. Induction chemotherapy with docetaxel/cisplatin/5-fluorouracil for patients with node-positive esophageal cancer. Digestion. 2011;83:146–52.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Watanabe M, Yoshida N, Karashima R, Sato N, Hirashima K, Imamura Y, et al. Transcervical superior mediastinal lymph node dissection combined with transhiatal lower esophageal dissection before transthoracic esophagectomy: a safe approach for salvage esophagectomy. J Am Coll Surg. 2009;208:e7–9.
Nakamura M, Iwahashi M, Nakamori M, Ishida K, Naka T, Iida T, et al. An analysis of the factors contributing to a reduction in the incidence of pulmonary complications following an esophagectomy for esophageal cancer. Langenbecks Arch Surg. 2008;393:127–33.
Law S, Wong KH, Kwok KF, Chu KM, Wong J. Predictive factors for postoperative pulmonary complications and mortality after esophagectomy for cancer. Ann Surg. 2004;240:791–800.
Morita M, Kumashiro R, Hisamatsu Y, Nakanishi R, Egashira A, Saeki H, et al. Clinical significance of salvage esophagectomy for remnant or recurrent cancer following definitive chemoradiotherapy. J Gastroenterol. 2011;46:1284–91.
Takeuchi H, Saikawa Y, Oyama T, Ozawa S, Suda K, Wada N, et al. Factors influencing the long-term survival in patients with esophageal cancer who underwent esophagectomy after chemoradiotherapy. World J Surg. 2010;34:277–84.
Miyata H, Yamasaki M, Takiguchi S, Nakajima K, Fujiwara Y, Nishida T, et al. Salvage esophagectomy after definitive chemoradiotherapy for thoracic esophageal cancer. J Surg Oncol. 2009;100:442–6.
Tachimori Y, Kanamori N, Uemura N, Hokamura N, Igaki H, Kato H. Salvage esophagectomy after high-dose chemoradiotherapy for esophageal squamous cell carcinoma. J Thorac Cardiovasc Surg. 2009;137:49–54.
Chao YK, Chan SC, Chang HK, Liu YH, Wu YC, Hsieh MJ, et al. Salvage surgery after failed chemoradiotherapy in squamous cell carcinoma of the esophagus. Eur J Surg Oncol. 2009;35:289–94.
Schlag PM. Randomized trial of preoperative chemotherapy for squamous cell cancer of the esophagus. The Chirurgische Arbeitsgemeinschaft Fuer Onkologie der Deutschen Gesellschaft Fuer Chirurgie Study Group. Arch Surg. 1992;127:1446–50.
Conflict of interest
Naoya Yoshida and the other co-authors have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yoshida, N., Watanabe, M., Baba, Y. et al. Estimation of physiologic ability and surgical stress (E-PASS) can assess short-term outcome after esophagectomy for esophageal cancer. Esophagus 10, 86–94 (2013). https://doi.org/10.1007/s10388-013-0369-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10388-013-0369-5