
Summary
Background
Segmental non-anatomical colectomy is a current proposed minimally invasive but non-anatomical procedure. However, few studies have compared its efficacy to that of anatomical colectomy.
Objective
To evaluate the prognostic impact of anatomical vs. non-anatomical colectomy in colon cancer.
Patients
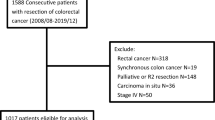
Based on the data of 1152 patients who underwent colorectal surgery, the 300 patients with pathologically proven stage II and III colon cancer were included. Patients were divided into two groups, depending on whether the anatomical colectomy (n = 161) or segmental non-anatomical colectomy (n = 139) was performed. The operative procedure was decided by preoperative imaging by taking into account the dominant vessels of the primary tumor. The overall survival and disease-free survival were analyzed.
Results
The number of harvested lymph nodes was significantly larger (p < 0.01) and the metastatic lymph node ratio was significantly lower (p < 0.01) for anatomical colectomy. Mean operation time (p = 0.13), intraoperative blood loss (p = 0.11), and complication (p = 0.70) rates did not differ significantly. The overall survival rates (89.1% vs. 76.9%, p < 0.01) and the 5‑year disease-free survival (86.2% vs. 70.5%, p < 0.01) were significantly better in the anatomical colectomy group than those in the non-anatomical group. The operative procedure (anatomical vs. non-anatomical, odds ratio: 2.65, 95% confidence interval: 1.37–5.35, p < 0.01) was the strongest predictor for overall survival.
Conclusions
Anatomical colectomy has a better prognostic impact than segmental non-anatomical colectomy in stage II and III colon cancer.


Similar content being viewed by others


References
Douillard JY, Siena S, Cassidy J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol. 2010;28:4697–705.
de Gramont A, Figer A, Seymour M, et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol. 2000;18:2938–47.
André T, Boni C, Mounedji-Boudiaf L, et al. Multicenter international study of oxaliplatin/5-fluorouracil/leucovorin in the adjuvant treatment of colon cancer (MOSAIC) investigators. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350:2343–51.
Lembersky BC, Wieand HS, Petrelli NJ, et al. Oral uracil and tegafur plus leucovorin compared with intravenous fluorouracil and leucovorin in stage II and III carcinoma of the colon: results from National Surgical Adjuvant Breast and Bowel Project Protocol C‑06. J Clin Oncol. 2006;24:2059–64.
Park IJ, Choi GS, Kang BM, Lim KH, Jun SH. Lymph node metastasis patterns in right-sided colon cancers: is segmental resection of these tumors oncologically safe? Ann Surg Oncol. 2009;16:1501–6.
Yada H, Sawai K, Taniguchi H, Hoshima M, Katoh M, Takahashi T. Analysis of vascular anatomy and lymph node metastases warrants radical segmental bowel resection for colon cancer. World J Surg. 1997;21:109–15.
Morikawa E, Yasutomi M, Shindou K, et al. Distribution of metastatic lymph node in colorectal cancer by the modified clearing method. Dis Colon Rectum. 1994;37:219–23.
Japanese Society for Cancer of the Colon and Rectum. Japanese classification of colorectal carcinoma. Tokyo: Kanehara; 2010.
Maurer CA. Colon cancer: resection standards. Tech Coloproctol. 2004;8(Suppl 1):s29–s32.
Sobin LH, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours. 7th ed. Oxford: Wiley-Blackwell; 2009.
Rouffet F, Hay JM, Vacher B, et al. Curative resection for left colonic carcinoma: hemicolectomy vs. segmental colectomy. A prospective, controlled, multicenter trial. French Association for Surgical Research. Dis Colon Rectum. 1994;37:651–9.
Wang J, Kulaylat M, Rockette H, et al. Should total number of lymph nodes be used as a quality of care measure for stage III colon cancer? Ann Surg. 2009;249:559–63.
Chen SL, Steele SR, Eberhardt J, Zhu K, Bilchik A, Stojadinovic A. Lymph node ratio as a quality and prognostic indicator in stage III colon cancer. Ann Surg. 2011;253:82–7.
Kim J, Huynh R, Abraham I, Kim E, Kumar RR. Number of lymph nodes examined and its impact on colorectal cancer staging. Am Surg. 2006;72:902–5.
Schumacher P, Dineen S, Barnett C Jr, Fleming J, Anthony T. The metastatic lymph node ratio predicts survival in colon cancer. Am J Surg. 2007;194:827–31.
Berger AC, Sigurdson ER, LeVoyer T, et al. Colon cancer survival is associated with decreasing ratio of metastatic to examined lymph nodes. J Clin Oncol. 2005;23:8706–12.
Hashiguchi Y, Hase K, Ueno H, et al. Prognostic significance of the number of lymph nodes examined in colon cancer surgery: clinical application beyond simple measurement. Ann Surg. 2010;251:872–81.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
T. Funada, S. Yamazaki, M. Kochi, and T. Takayama declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Funada, T., Yamazaki, S., Kochi, M. et al. Impact of anatomical versus non-anatomical resection for stage II and III colon cancer. Eur Surg 50, 183–188 (2018). https://doi.org/10.1007/s10353-018-0523-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10353-018-0523-3