
Abstract
Purpose
This study was performed to evaluate the risk factors of parastomal hernia after abdominoperineal rectal amputation.
Methods
This was a retrospective study of consecutive patients who underwent abdominoperineal rectal amputation for rectal cancer between January 1999 and August 2006. The effects of age, sex, surgical approach, chemotherapy, waist circumference, and body mass index on the development of a parastomal hernia were analyzed.
Results
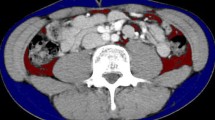
Forty-one patients underwent 19 open and 22 laparoscopic abdominoperineal rectal amputations. A parastomal hernia developed in 19 patients (46 percent) after a median follow-up period of 31 (range, 5–80) months. We observed ten hernias in the open group and nine in the laparoscopic group (P = 0.453). There were no significant differences in the type of surgical approach, age, sex, or adjuvant therapy in patients who developed a parastomal hernia compared with those who did not. Waist circumference proved to be an independent risk factor (P = 0.011). When the waist circumference exceeds the calculated threshold of 100 cm, there is a 75 percent probability to develop a parastomal hernia.
Conclusions
Abdominal obesity increases the risk of developing a parastomal hernia, therefore, it might be advisable to place a prophylactic mesh during colostomy formation when the patient’s waist exceeds 100 cm.
Similar content being viewed by others

References
Carne PW, Robertson GM, Frizelle FA. Parastomal hernia. Br J Surg 2003;90:784–93.
Kouba E, Sands M, Lentz A, Wallen E, Pruthi RS. Incidence and risk factors of stomal complications in patients undergoing cystectomy with ileal conduit urinary diversion for bladder cancer. J Urol 2007;178:950–4.
Sjödahl R, Anderberg B, Bolin T. Parastomal hernia in relation to site of the abdominal stoma. Br J Surg 1988;75:416–8.
Londono-Schimmer EE, Leong AP, Phillips RK. Life table analysis of stomal complications following colostomy. Dis Colon Rectum 1994;37:916–20.
Etherington RJ, Williams JG, Hatward MW, Hughes LE. Demonstration of para-ileostomy herniation using computed tomography. Clin Radiol 1990;41:333–6.
de Ruiter P, Bijnen AB. Successful local repair of paracolostomy hernia with a newly developed prosthetic device. Int J Colorectal Dis 1992;7:132–4.
Allen-Mersh TG, Thomson JP. Surgical treatment of colostomy complications. Br J Surg 1988;75:416–8.
Cheung MT, Chia NH, Chiu WY. Surgical treatment of parastomal hernia complicating sigmoid colostomies. Dis Colon Rectum 2001;44:266–70.
Rubin MS, Schoetz DJ Jr, Matthews JB. Parastomal hernia. Is stoma relocation superior to fascial repair? Arch Surg 1994;129:413.
Janes A, Cengiz Y, Israelsson LA. Preventing parastomal hernia with a prosthetic mesh. Arch Surg 2004;139:1356–8.
Steele SR, Lee P, Martin MJ, Mullenix PS, Sullivan ES. Is parastomal hernia repair with polypropylene mesh safe? Am J Surg 2003;185:436–40.
de Ruiter P, Bijnen AB. Ring-reinforced prosthesis for paracolostomy hernia. Dig Surg 2005;22:152–6.
Longman RJ, Thomson WH. Mesh repair of parastomal hernias: a safety modification. Colorectal Dis 2005;7:292–4.
Hofstetter WL, Vukasin P, Ortega AE, Anthone G, Beart RW Jr. New technique for mesh repair of paracolostomy hernias. Dis Colon Rectum 1998;41:1054–5.
Stelzner S, Hellmich G, Ludwig K. Repair of paracolostomy hernias with a prosthetic mesh in the intraperitoneal onlay position: modified Sugarbaker technique. Dis Colon Rectum 2004;47:185–91.
van Sprundel TC, Gerritsen van der Hoop A. Modified technique for parastomal hernia repair in patients with intractable stoma-care problems. Colorectal Dis 2005;7:445–9.
Berger D, Bientzle M. Laparoscopic repair of parastomal hernias: a single surgeon’s experience in 66 patients. Dis Colon Rectum 2007;50:1668–73.
Mancini GJ, McClusky 3rd, Khaitan L, et al. Laparoscopic parastomal hernia repair using a nonslit mesh technique. Surg Endosc 2007;21:1487–91.
Author information
Authors and Affiliations
Corresponding author
Additional information
Reprints are not available.
About this article
Cite this article
De Raet, J., Delvaux, G., Haentjens, P. et al. Waist Circumference is an Independent Risk Factor for the Development of Parastomal Hernia After Permanent Colostomy. Dis Colon Rectum 51, 1806–1809 (2008). https://doi.org/10.1007/s10350-008-9366-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10350-008-9366-5