
Abstract
Ictal hand signs manifest as dystonic, tonic, or non-convulsive rhythmic elementary motor patterns, as well as finger snapping or automatic movement patterns (e.g. fumbling), and psychogenic movements have been reported in a small number of patients. This study demonstrates the various ictal hand signs and discusses the data on lateralization and localization as reported in the literature. In addition to published reports, our case studies are presented.
Zusammenfassung
Iktale Handsymptome sind nur in geringer Zahl publiziert worden. Sie können dystonischen, tonischen, nichtkonvulsiven rhythmischen elementar-motorischen Bewegungsmustern, Fingerschnappen oder automatischen Bewegungsmustern (z. B. fummelnde Bewegungen) und psychogenen Bewegungen entsprechen. In der vorliegenden Arbeit werden die verschiedenen iktalen Handsymptome dargestellt, außerdem werden Daten zur Lateralisierung und Lokalisation unter Einschluss eigener Beobachtungen und der vorhandenen Literatur erörtert.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Akkadian texts (empire of Sargon Akkad) reported seizure signs as early as 1050–1800 Before Christ in the form of “tonic muscular tension arm, neck to the left, eyes open.” An early description of ictal semiology was later presented by Tissot in 1789 [1]. The introduction of video EEG monitoring allowed for a clinically driven precise analysis method, and the phenomenon of ictal dystonic limb posturing was subsequently described by Bleasel et al. and Kotagal et al. [2, 3]. This condition was characterized as an involuntary forced muscle contraction of the hand, forearm, and shoulder that caused an unnatural posturing of the flexed or stretched limb, flexion of the wrist and metacarpophalangeal joints, extension of fingers, or rotation of the forearm. Using an analysis method driven by video EEG monitoring, ictal semiology evolved to provide the fundamental information for diagnosis of the seizure onset zone. The century-long discussion resulted in a variety of terminologies relating to ictal signs. The glossary of descriptive terminology for ictal semiology published by Blume et al. [4] defined the terms as follows:
-
“Tonic: sustained increase in muscle contraction lasting a few seconds to minutes;
-
Postural: adoption of a posture that may be bilaterally symmetric or asymmetric;
-
Dystonic: sustained contraction of both agonist and antagonist muscles producing athetoid or twisting movements which may produce abnormal postures.”
A recently published glossary of terms and their significance has been summarized by Beniczky et al. [5].
The definition and description of ictal dystonic or tonic hand signs are incomplete and inconsistent. Rotation and unnatural elements of dystonic posturing are defined as different features compared to those of tonic posturing. Full-blown dystonic upper limb posturing ictal signs that affect only the hand or fingers were described subsequently, and snapping, tonic motor activities, and rhythmic ictal non-clonic hand (RINCH) motions extended the spectrum of hand and finger signs [6,7,8,9,10]. With regard to localization, different ictal hand postures (thumb abduction, wrist flexion, fist closure, finger hyperextension) were first classified in the temporal lobe by Holl et al. [11]. Index finger pointing was subsequently described by Siegel and Tantum [12], and the ictal signs “politician’s fist” and “pincer” were added by Ferando et al. [13]. Ictal hand posture signs include elementary movement patterns with persistent tense muscle contractions that last for several seconds. The speed and amplitude of the movements are often considered part of normal movement.
This study presents the various hand postures and discusses the localization results. In addition to published reports, our case studies are presented.
Lateralization and localization values
The thumb sign is defined as the stretched abduction of the thumb and is localized in the contralateral temporal lobe [14]. After the classification of the observed phenomenology of hand postures by Holl et al. [11], two further groups were defined by their predominant muscle reactions: sustained muscle contractions (Type I) and myoclonic jerks (Type II).
-
Type I involves sustained muscle contractions with (a) abduction of the thumb, (b) flexion of the wrist, or (c) extension of all fingers.
-
Type II consists of myoclonic dystonia with (a) abduction of the thumb, (b) flexion of the wrist and fist closure, or (c) extension of all fingers.
These groupings were used to correlate ictal phenomena with either the mesial or lateral temporal lobe origin. Although the difference in location was not statistically significant [11], a comparison of the mean latencies of contralateral sustained dystonic posturing, including flexion of the wrist and fist closure (Type IB), between seizures resulting from mesial temporal lobe epilepsy (MTLE) and those from neocortical temporal lobe epilepsy (NTLE) resulted in a statistically significant difference (mean latencies: 19 and 7 s, respectively; p = 0.001). The pathophysiological considerations differentiated between striatopallidal and thalamic dystonia [15]. A clinical analysis of flexion of the wrist hand posturing showed a significant earlier occurrence of the “striatopallidal” type in NTLE compared to MTLE seizures, suggesting rapid seizure propagation from the neocortical focus to the striatopallidal complex compared to the “delayed” spread of ictal discharges from mesial temporal structures.
Different hand signs are presented in Fig. 1, including their lateralization and localization values. The predominant lateralization and localization information of ictal hand signs has been presented in various studies [11, 13, 14, 16]. Our video EEG monitoring analysis of 145 patients revealed six patients with ictal fist, six with ictal hand extension, five with ictal cup, three with RINCH, two with ictal thumb-up, two with ictal pincer, and one each with ictal index pointers.

Ictal hand sign lateralization and/or localization values from different studies. (Concurrence with the results described by Ferando et al. [13] is indicated by the letters i–iii: i, study by Vilaseca et al. [14]; ii, study by Ferando et al. [13]; iii, our study). Cup sign points to temporal lobe (in study ii) in study c to fronto-temporal, extended hand to contralateral fronto-temporal (in study ii, iii); claw to fronto-temporal (study iii); fist to frontal (in studies ii, iii), index pointer to frontal (in studies ii, iii); thumb-up, pincer and politician’s fist to temporal (study i, iii); a the “cup” sign, contralateral fronto-temporal (ii, iii), b the thumb sign, contralateral temporal (i, iii), c the “claw” sign, contralateral, fronto-temporal (iii), d the extended hand sign, contralateral (ii, iii), e the closed fist sign, contralateral, frontal (ii, iii), f the “pincer” sign, contralateral temporal (ii), g the index pointer sign, frontal (ii, iii), h the Politician’s fist to temporal (ii)
Ictal hand signs were found in 54.5% of patients with temporal lobe seizures and 72.5% of those with frontal epilepsies by Ferando et al. [13]. The signs identified were cup, fist, pincer, politician’s fist, index pointer, and extended hand, which corresponded to some of the signs observed in this study as shown in Fig. 1. The index pointer sign in our case was combined with a fist posture of the other fingers, whereas in the report by Ferando et al., the index finger and thumb were extended while the other fingers were less flexed, resulting in a more open hand. The results of that study [13] identified a significant correlation between ictal hand posture and epileptogenic zone localization (p = 0.00001). Only seizures with temporal onsets were associated with the cup or pincer sign, while the fist, extended hand, and pointer signs were only present in frontal seizure onsets.
The ictal thumb-up sign was observed by Vilaseca et al. [14] in 5% of temporal lobe seizures. The latency to the seizure onset was 3–25 s and ipsilateral automatism was not featured in these cases.
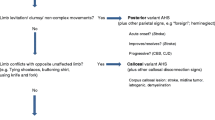
Bleasel et al. [2] recognized that dystonic posturing occurred in 35.3% of TLE patients (κ: 0.78, positive predictive value [PPV] for the sign being contralateral to seizure onset: 92%), while tonic limb posturing occurred in 17.7% (κ: 0.36, PPV 40%) and unilateral immobile limb was present in 11.8% of the patients (κ: 0.23, PPV: 100%). In patients with extratemporal epilepsy, dystonic posturing was observed in 20.0% (κ: 0.31, PPV: 100%) of the cases and tonic limb posturing occurred in 15.0% (κ: 0.08, PPV: 67%). The higher kappa indexes were significant for dystonic posturing (p < 0.001) and tonic limb posturing (p = 0.032) in TLE patients. Dystonic posturing (p = 0.034), tonic posturing (p = 0.07), and version (p = 0.0038) was reported to occur earlier in extratemporal seizures than in temporal seizures. Marashly et al. [17] stated that ictal dystonia only included dystonic posturing of the hand. These authors suggested that the rotatory component of the hand (into extreme pronation or supination), which is the hallmark of increased tonic flexion or extension in ictal dystonia, was previously included as a tonic seizure component. During the tonic phase of a focal-to-bilateral tonic–clonic seizure, a posture similar to the dystonic posture can exist. Marashly et al. [17] stressed that the similarity of these postures may cause confusion leading to the reporting of a higher prevalence of ictal dystonia in some studies: “Moreover, despite a strict definition of dystonia, this sign had the least interrater reliability, further limiting the utility of this sign. It is important to stress, however, that in this study we analyzed ictal dystonia as presence of dystonia at any point before the generalization irrespective of its association with an `automotor or dialeptic´ phase of the seizure. Because previous studies analyzed ictal dystonia specifically in association with these features, this difference may explain the discrepancy (up to 67% difference; annotation by the authors of this manuscript) of the positive predictive value of ictal dystonia between the reports in the literature and the present study.”
Ictal hand sign and epilepsy type
Hand signs may occur in focal and generalized seizures as well as in non-epileptic seizures. The index pointer sign (IPS) was more common in focal-to-bilateral tonic–clonic seizures than in generalized bilateral tonic seizures (96% vs. 56.6%; p ≤ 0.001). In addition, the IPS was less common in non-epileptic “convulsive” seizures than in bilateral tonic–clonic seizures (83.6% vs. 12.0%; p < 0.001; [16]).
Siegel and Tatum [12] showed a claw hand posture only during non-epileptic seizures, whereas our study also observed this sign in focal epileptic seizure cases.
We (i.e. H.S. the 1st author) extensively evaluated ictal hand signs in typical generalized epilepsy absences [18] and found that an absence seizure of the same patient produced the following ictal semiology: initial ocular signs with versive rhythmic eye movements to the right (5 s duration), followed by ictal flexing of the fingers up to making a fist in the left hand (beginning 2 s after seizure onset and enduring for 8.5 s), and tonic stretching of the left toe resembling a Babinski sign at 3 s after fist onset. The hand sign occurred as a single element over one spike wave and was integrated during the absence seizure in a characteristic temporal succession of ictal signs from the ocular region to the lower extremities.
Differences between hand automatisms and ictal hand signs
Hand automatisms involve complex movement patterns. The International League Against Epilepsy (ILAE) glossary states that “the term automatism is used to account for an irrepressible, discrete or excessive and repetitive single motor activity that often resembles a voluntary behavior.” Gestural automatisms are rhythmic repetitive movements of the hands. Distal automatisms (e.g., tapping, crumbling, fumbling, grasping, finger snapping, exploratory movements, manipulating movements) can be self-directed (virtually independent of environmental factors) or environmentally influenced. Hand automatisms are often RINCH (unilateral, rhythmic, non-clonic, non-tremor) hand movements (low-amplitude milking, grasping, fist clenching, or pill rolling, or larger-amplitude hand opening and closing movements) that are usually followed by dystonic posturing, sometimes with overlap [5]. Hand automatisms such as fumbling that unilaterally involve the distal segments of the upper extremities can indicate ipsilateral seizure onset, as demonstrated by Vilaseca et al. [14] in their study of temporal lobe epilepsy. The term automatism is indistinct and can be intermingled with other clear definable motor patterns (e.g., dystonia). This can cause misleading conclusions. Another characteristic ictal movement is gripping the neck with the hand at the onset of a seizure of the insula when the patient experiences an unpleasant sensation of laryngeal constriction and paresthesia [19]. Postictal nose wiping is often found ipsilateral to a seizure onset when contralateral limb posturing occurs simultaneously. A sensation in the nose can cause the ipsilateral hand to move toward the nose, while the contralateral arm is fixed by dystonic posturing. Similarly, genital automatisms are often observed in temporal lobe epilepsies [20], mostly ipsilateral to the seizure onset. Ictal grasping can be directed toward the body of the patient or the surroundings and is evoked by stimulation of the anterior cingulate cortex. This hand sign is reported as often occurring contralaterally but does not have a consistent lateralization value. The current study observed that a sudden flexing of fingers (clenching fingers similar to grasping with the left hand) was documented with the video EEG simultaneously contralaterally to a right “interictal” frontal spike.
Ictal motor phenomena can be misinterpreted as voluntary spontaneous movements or tics [18]. Masked small motor seizures could be detected and diagnoses corrected using simultaneous video EEG documentation.
Generally, pseudo-voluntary movements represent elementary or complex motor patterns (also called “motorische Schablone” [21]), and knowledge of their characteristic patterns in the context of their occurrence facilitates differential diagnostic analyses.
The specific pathophysiology of hand automatisms
An important factor in relation to automatisms is the basal ganglia network, which is a complex interconnected system that receives multiple topographically organized inputs from the neocortex, thalamus, and limbic system. In addition, this network forwards information regarding motor control and motivational behavior to the thalamus and brainstem. The involvement of specific basal ganglia subcircuits could help explain different automatic patterns and hand automatisms. According to Dhawale et al. [22], the sensorimotor arm of the basal ganglia circuit is crucial for generating the detailed movement patterns underlying motor skills: “The basal ganglia can specify and control the fine-grained details of learned motor skills through their interactions with lower-level motor circuits.” Anatomical studies indicate that the topographical organization in the striatum/thalamus and cortex operates through a loop. Similar to the basal ganglia, the cerebral cortex contains circuits that manage learned body movements (e.g. fine finger movements) in the motor cortex and control learned behaviors (e.g. context-dependent decisions) in the prefrontal cortex. Furthermore, the basal ganglia project to different brainstem regions for innate body movements (as an “pattern generation” [23]). Electrophysiology and neuroimaging, including SPECT and fMRI, could provide an improved understanding of the role of the complex network of basal ganglia and other subcortical structures in the generation of ictal hand semiology. A comparison of regional count ratios of ictal dystonia cases to patients without this disorder showed significant changes in the basal ganglia only. Specifically, ictal dystonia was associated with a relative increase in the perfusion of basal ganglia opposite the dystonic limb [24]. Striatal cholinergic dysfunction is considered a unifying theme in the pathophysiology of dystonia [25]. Dystonia with striatal and thalamic involvement was differentiated by Lehéricy [15].
Ictal hand signs and their importance in seizure propagation
Several ictal hand signs can occur in a temporal sequence during one seizure; therefore, initial and subsequent signs should be analyzed in regard to individual seizure propagation. A small cohort of our patients exhibited the following signs: One patient initially showed a cup sign and hand extension and subsequently a claw sign, all of which were contralateral to the frontal lobe involvement; two patients had seizures with an initial cup or RINCH sign, followed by a fist sign, with the latter possibly due to propagation from the temporal to frontal lobe; one patient first showed a left-hand extension and subsequently a right fist, and the seizure started in the right temporal region and spread to the left frontal area; four patients showed contralateral RINCH motions, of which two occurred after propagation from seizure onset to contralateral hemisphere; and two patients with pincer had contralateral temporal seizure onset similar to the cases described by Ferando et al. [13].
Conclusion
Ictal hand signs are rarely reported, both in relation to non-epileptic or generalized seizures as well as for focal seizures, which are the main objects of presurgical video EEG monitoring. Ictal hand signs can manifest as dystonic or tonic movements, non-convulsive rhythmic elementary motor patterns (e.g., RINCH), finger snapping, or complex automatic movement patterns (e.g., fumbling). Currently, ictal postural hand signs are not specially listed in semiological glossaries. RINCH movements should be differentiated from automatisms of the upper extremity to prevent the diagnosis of automotor seizures with incorrect localization information. Automatisms involving the distal segments of the upper extremities in cases of unilateral occurrence often indicate ipsilateral seizure onset, whereas RINCH motion is mainly contralateral to the seizure-onset hemisphere. Finger snapping could be interpreted as a temporal lobe automatism if presenting as a mild movement, but not in the case of wild movements. “The fierceness of the finger-snapping movement associated with tonic abduction of the upper limb” can indicate a focus in the supplementary motor area, as indicated by Overdijk et al. [8]. Concerning the lateralization and localization values, most of the video EEG monitoring showed ictal hand signs associated with seizure onset in the contralateral hemisphere. The ictal thumb-up phenomenon pointed to the right temporal lobe in all six cases analyzed by Vilaseca et al. [14], although it was not the first ictal sign of the seizure. The two ictal thumb cases in our study were contralaterally temporally localized. The Ictal fist and pointer were indicators of frontal lobe seizure onset [13] and this sign was observed in five of six patients with a contralateral frontal lobe seizure onset in our own study.
Localization approaches should consider more than the brain area of the seizure onset. If epilepsy is considered a network disorder, different seizure types might be attributed to the involvement of distinct cortical and subcortical networks. An analysis of the temporal succession of ictal signs provides essential information for the identification of the brain regions involved, and Bancaud et al. [26] studied this using an anatomical-electro-clinical approach for focal seizures. The ILAE-classified generalized seizures, such as in absence seizures, show a temporal evolution of discrete signs, whereby they exhibit a “cranio-caudal march” [27]. This phenomenon has been discussed in the context of the current comprehension of network involvement in “generalized” seizures [28]. The limitations of using ictal semiology for localization are the absence of initial ictal signs (such as hand postures) and the onset of epileptic discharges in the “silent brain regions.” In addition, the use of imprecise terminology may obscure diagnoses. Elementary motor signs can often be the keys to understanding distinct cortical involvement and seizure propagation, while the pathophysiology of complex motor behaviors is more difficult to comprehend. The release phenomena of networks with fixed action patterns (central pattern generators; [29]) and the transient “desynchrony” in emotion-regulation networks [30] must consider more than one specific region.
Previous concepts and future perspectives for dynamic semiology and network analyses using multiple techniques are discussed in detail by McGonigal et al. [31]. Within network analyses, a conceptual amalgamation of the focus and network concept is a challenge. Stefan and Schmitt [32] suggested a combined presentation from the epileptic nucleus to network involvement. In terms of semiology, the initial ictal sign of a seizure provides the first important information, but the temporal succession of the ictal signs during the seizure allows for an understanding of how single elements are embedded in the Gestalt of the seizure evolution. This also holds for ictal hand signs. The localization, lateralization, and seizure-type information of ictal hand signs requires several preconditions:
-
1.
Precise terminology with regard to known elementary or complex movements/postures or repetitive stereotyped movements;
-
2.
The temporal course of seizure signs;
-
3.
Co-registration with video EEG monitoring.
Continuous long-term video EEG testing can unmask pseudo-voluntary ictal movements.
In 2021, McGonigal [31] stated that a “better understanding of semiologic categorization and pathophysiological correlates is relevant to seizure classification. Systems advances in knowledge of neural mechanisms as well as anatomic correlates of different semiologic patterns could help improve knowledge of epilepsy networks and potentially contribute to therapeutic innovations.”
The recognition and analysis of ictal hand signs may participate in this proposition. The results of the different studies indicate that ictal hand signs should be more thoroughly analyzed during seizure episodes. A multicenter study could overcome the limitations of low patient numbers for assessing prevalence and lateralization and localization values.
References
Tissot S. Traité de l’epilepsie (1789), Esquirol1838 (Esquirol E. Des maladies mentales: L’epilepsie. Paris: chez J.B. Baillière, 1838
Bleasel A, Kotagal P, Kankirawatana P, Rybicki L (1997) Lateralizing value and semiology of ictal limb posturing and version in temporal lobe and extratemporal epilepsy. Epilepsia 38(2):168–174
Kotagal P, Luders H, Morris H, Dinner D et al (1989) Dystonic posturing in complex partial seizures of temporal lobe onset: a new lateralizing sign. Neurology 39:196–201
Blume W, Lüders H, Mizrrahi E, Tassinari C et al (2001) Glossary of descriptive terminology for ictal semiology: report of the ILAE task force on classification and terminology. Epilepsia 42(9):1212–1218
Beniczky S, Tatum O, Blumenfeld H, Stefan H et al (2022) Seizure semiology: ILAE glossary of terms and their significance. Epileptic Disord 24(3):447–495
Kuba R, Musilova K, Vojvodic N, Tyrlikova I et al (2013) Rhythmic ictal nonclonic hand (RINCH) motions in temporal lobe epilepsy: invasive EEG findings, incidence, and lateralizing value. Epilepsy Res 106(3):386–395
Lee GR, Arain A, Lim N, Lagrange A et al (2006) Rhythmic ictal nonclonic hand (RINCH) motions: a distinct contralateral sign in temporal lobe epilepsy. Epilepsia 47(12):2189–2192
Overdijk MJ, Zijlmans M, Gosselaar PH, Olivier A et al (2014) Finger snapping during seizures. Epilepsy Behav Case Rep 14(2):108–111
Van Ness P (1996) Invasive electroencephalography in evaluating the supplementary motor area seizures. Ach Neurol 17:319–340
Zaher N, Haas K, Sonmezturk H, Arain A et al (2020) Rhythmic ictal nonclonic hand (RINCH) motions in general EMU patients with focal epilepsy. Epilepsy Behav 103(Part A):106666
Holl A, Feichtinger AM, Körner E, Stefan H, Ott E (2005) Ictal dystonic posturing in mesial versus neocortical temporal lobe seizures. Seizure 14(4):269–273
Siegel J, Tatum O (2016) Index-finger pointing in generalized tonic-clonic seizures. Epilepsy Behav 58:18–21
Ferando I, Soss JR, Elder C, Shah V et al (2019) Hand posture as localizing sign in adult focal epileptic seizures. Ann Neurol 86(5):793–800
Vilaseca A, Fonseca E, Martin CA, Alvarez-Sabin J et al (2021) Thumb-up sign: characterization of an undescribed seizure semiology sign. Seizure 89:62–64
Lehéricy S, Vidailhet M, Dormont D, Piérot L, Chiras J et al (1996) Striatopallidal and thalamic dystonia. A magnetic resonance imaging anatomoclinical study. Arch Neurol 53(3):241–250
Siegel J, Tantum O (2016) Hand postures in primary and secondary generalized tonic-clonic seizures. Neurology 87(17):1802–1805
Marashly A, Ewida A, Agarwal R, Younes K et al (2016) Ictal motor sequences: lateralization and localization values. Epilepsia 57(3):369–375
Stefan H (1981) Pseudospontanbewegungen bei Patienten mit Petit mal Anfällen. Arch Psychiatr Nervenkrankheiten 229(4):277–290
Isnard J, Guénot M, Sindou M, Mauguière F (2004) Clinical manifestations of insular lobe seizures: a stereo-electroencephalographic study. Epilepsia 45(9):1079–1090
Voges B, Schmitt FC, House PM, Stodieck RS, Schenck HC (2019) Complex sexual behaviors during sleep as a manifestation of epilepsy: a case series. Sleep. https://doi.org/10.1093/sleep/zsy233
Kretschmer E (1953) Der Begriff motorischer Schablonen und ihre Rolle in normalen und pathologischen Lebensvorgängen. Arch Psychiatr Nervenkrankheiten 190(1):1–3
Dhawale A, Wollf St, Ko R, Ölveczky B (2021) The basal ganglia control the detailed kinematics of learned motor skills. Nat Neurosci 24(9):1256–1269
Kim HF, Hikosaka O (2015) Parallel basal ganglia circuits for voluntary and automatic behaviour to reach rewards. Brain 138(Pt 7):1776–1800
Newton MR, Berkovic SF, Austin MC, Reutens DC, McKay WJ, Bladin PF (1992) Dystonia, clinical lateralization, and regional blood flow changes in temporal lobe seizures. Neurology 42(2):371–377
Eskow Jaunarajs KL, Bonsi P, Chesselet MF, Standaert DG, Pisani A (2015) Striatal cholinergic dysfunction as a unifying theme in the pathophysiology of dystonia. Prog Neurobiol 127–128:91–107
Bancaud J, Talairach J (1965) La stéréo-électroencéphalographie dans l’épilepsie: informations neurophysiopathologiques apportées par l’investigation fonctionnelle stéreotaxique. Masson et Cie, Paris
Stefan H (1982) Epileptische Absencen: Studien zur Anfallsstruktur, Pathophysiologie und zum klinischen Verlauf. Thieme
Stefan H, Trinka E (2022) Generalized absence seizures: where do we stand today? Z Epileptol 35:56–72
Tassinari CA, Rubboli G, Gardella E, Cantalupo G, Calandra-Buonaura G, Vedovello M et al (2005) Central pattern generators for a common semiology in fronto-limbic seizures and in parasomnias. A neuroethologic approach. Neurol Sci 26(Suppl 3):s225–s232
Bartolomei F, Trébuchon A, Gavaret M, Régis J, Wendling F, Chauvel P (2005) Acute alteration of emotional behaviour in epileptic seizures is related to transient desynchrony in emotion-regulation networks. Clin Neurophysiol 116(10):2473–2479
McGonigal A, Bartolome F, Chauvel P (2021) On seizure semiology. Epilepsia 62(9):2019–2035
Stefan H, Schmitt F (2021) Epilepsie als Netzwerkerkrankung. In: Schmitt F, Stefan H, Holtkamp M (eds) Epileptische Anfälle und Epilepsien im Erwachsenenalter. Springer, pp 21–27
Acknowledgements
We would like to thank Irina Pollenskaya (drpollenskaya@gmail.com) for creating and Karen Klewer (MSc.) for preparing the illustrations for this manuscript.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
H. Stefan, A. Strzelczyk and F.C. Schmitt declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies mentioned were in accordance with the ethical standards indicated in each case.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.

Scan QR code & read article online
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Stefan, H., Strzelczyk, A. & Schmitt, F.C. Ictal hand signs: Minimal previous attention to these diagnostic indicators. Clin Epileptol 37, 144–149 (2024). https://doi.org/10.1007/s10309-023-00644-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10309-023-00644-7