
Abstract
Personal values are broad motivational goals that have been found to have systematic relations with subjective wellbeing in adults. Values that promote higher subjective wellbeing are considered healthy while those that hamper it are considered unhealthy (Schwartz & Sortheix, 2018). However, little is known about these relations in children. This pre-registered study examined (1) whether the values of children (6 to 12 years of age) relate to their subjective wellbeing and (2) whether these relations are moderated or mediated by perceived social support from parents, teachers, classmates, and close friends. These research questions were examined with a sample of 738 primary school students (50% female). Our results show that healthy growth values were positively related to subjective wellbeing overall, and for the subgroups of girls and children 9 to 12 years but not boys and children 6 to 8 years; however, unhealthy anxiety values were only negatively associated with subjective wellbeing for girls. While perceived social support partially mediated relations between growth values and subjective wellbeing, the direct values-wellbeing relations accounted for over half the variance. Interestingly, this study also found that growth values positively, and anxiety values negatively, influenced perceived social support from all referents. While perceived social support did not moderate values-wellbeing relations in the overall sample, differences were found in the way perceived social support moderated these relations in some age and gender subgroups. Taken together, these findings suggest that healthy growth values positively influence subjective wellbeing in middle childhood, even after accounting for perceived social support.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is growing evidence of mental health problems among school aged children (4 to 17 years), globally. For instance, in Australia, 14% of primary school aged children (4 to 11 years) experienced a diagnosable mental health disorder, including behavior and anxiety disorders (e.g., AIHW, 2020; Goodsell et al., 2017). In England, mental health disorders increased from 11% in 2017 to 16% in 2020 in children aged 5 to 16 years (Newlove-Delgado et al., 2021) and in India, 23% of school children are said to have a psychiatric disorder (see meta-analysis, Malhotra & Patra, 2014). Internalizing problems (e.g., depressive and anxiety symptoms, somatic complaints, and withdrawn behavior) have also been reported to have increased in childhood in Australia (Wang et al., 2018). Evidence of an increase in mental health problems in childhood has resulted in a greater interest in increasing wellbeing in the school context (Dix et al., 2020a; 2020b; OECD, 2019d).
Subjective wellbeing, which relates to how individuals evaluate their own lives, including cognitive appraisals of life, and domains of life, as well as positive and negative affect (e.g., emotions and moods; Diener et al., 2017), is a key aspect of wellbeing. In this paper, the focus is on how happy and satisfied individuals are with the life they are leading (see Schwartz & Sortheix, 2018). Understanding subjective wellbeing is important in the school context, as it has been found to predict changes in students’ academic functioning and outcomes (e.g., Suldo et al., 2011). In addition, subjective wellbeing has been found to be reciprocally associated with academic engagement (e.g., Datu & King, 2018).
Brockevelt et al. (2019) suggested that subjective wellbeing is a transformative interaction between the child (i.e., their self-concept, beliefs and values, personal competence, attitudes, and personality), their context (i.e., home, family, community, school, and peers), and their engagement in meaningful activity (i.e., habits, routines, rituals, and role fulfilment). However, most previous research on subjective wellbeing in childhood has focused on the influence of context, primarily social context. For instance, the wellbeing of adolescents in a classroom context has been shown to be related to the wellbeing of their classmates King and Datu (2017). Specifically, adolescents in classes with high levels of positive affect and life satisfaction were also more likely to have high levels of positive affect and life satisfaction themselves. In younger children (aged 7 years), relationships with friends/family, issues of safety, and bullying and social exclusion during school play were important factors in predicting subjective wellbeing (Rees, 2019). While social context is clearly an important aspect of wellbeing in school children, little is known about the impact of individual differences in personality characteristics on their wellbeing.
There has been a great deal of interest in how different aspects of personality, especially traits and values, relate to subjective wellbeing in adults. In support of this, meta-analytic studies have found that personality traits are one of the better predictors of subjective wellbeing in adults (Anglim et al., 2020; Steel et al., 2008). Studies have also found that personal values have both a direct and indirect impact on subjective wellbeing in adults (e.g., Schwartz & Sortheix, 2018). However, no studies were found to examine whether or how personal values are associated with subjective wellbeing in middle childhood.
The current, pre-registered study (see link https://aspredicted.org/7VS_JM3) aimed to help fill this gap by examining whether and how personal values, defined as broad motivational life goals (Schwartz, 1992), relate to subjective wellbeing in middle childhood. However, rather than studying these relations in isolation, as is the case in much of the adult literature, this study examined how personal values relate to subjective wellbeing in light of perceived social support from important referents (i.e., parents, teachers, classmates, and close friends), as good interpersonal relationships with those who are close are fundamental to wellbeing (e.g., Baumeister & Leary, 1995).
Personal values, perceived social support, and subjective wellbeing
Personal values are broad motivational goals that transcend situations and reflect what is important to people in their lives (Rokeach, 1973; Schwartz, 1994). They serve as guiding principles that direct beliefs, attitudes, and behavior (e.g., Allport et al., 1960; Rokeach, 1973; Schwartz, 1992) and have been associated with subjective wellbeing in adults (e.g., Sagiv & Schwartz, 2000; Schwartz & Sortheix, 2018; Sortheix & Schwartz, 2017).
The most commonly cited personal values theory today is the Schwartz (1992) theory of human values. This theory identified the circular structure of a set of near-universal values, based on a motivational continuum that underlies the conflicts and compatibilities among values. Schwartz (1992) divided this circular structure into ten basic values (see Fig. 1, inner circle), and summarized the conflicts and compatibilities among these basic values with four higher order values, organized along two dimensions (Fig. 1, second circle). The first dimension opposes self-transcendence values (i.e., benevolence and universalism), emphasizing concern for the welfare of close and distant others, with self-enhancement values (i.e., power, achievement, and sometimes hedonism), emphasizing the pursuit of self-interests over the interests of others. The second dimension opposes conservation values (i.e., tradition, conformity, and security), emphasizing maintenance of the status quo, with openness-to-change values (i.e., self-direction, stimulation, and sometimes hedonism), emphasizing the pursuit of autonomy and novelty. The ten basic and four higher order values can also be collapsed into different dimensions (Fig. 1, outer circles), including the contrast between anxiety avoidance and growth values and the contrast between person-focused and social-focused values (Schwartz et al., 2012). This theory allows researchers to examine relations between values and constructs of interest at different levels of specificity.

Schwartz theory of human values. Source: Adapted from Schwartz, S. H. (2016, Ch4, p.68) ‘Basic individual values: Sources and consequences’. Handbook of value. Perspectives from Economics, Neuroscience, Philosophy, Psychology and Sociology. Oxford University Press
Empirical support for the Schwartz (1992) theory has been found in hundreds of adult samples in more than 80 countries (Sagiv et al., 2017). There is also growing evidence that childrens’ values are similar, in both structure and function, to those found in adult samples (e.g., Collins et al., 2017; Döring et al., 2010; Lee et al., 2017).
Childrens’ values have been found to relate to antecedents (e.g., age and gender) in a similar way to adults’ values. Specifically, in terms of gender, boys have been found to place higher importance on self-enhancement values than girls, whereas girls have been found to place higher importance on the opposing self-transcendence values than boys (e.g., Bilsky et al., 2015; Döring et al., 2015; Lee et al., 2017; Tulviste et al., 2018). These gender-based patterns are similar to those found in adult (e.g., Borg, 2019) and adolescent samples (e.g., Elizarov et al., 2023). Similarly, age has been positively associated with self-transcendence and negatively associated with self-enhancement values in middle childhood (Daniel et al., 2020; Tamm & Tulviste, 2022). However, in contrast to adults, openness-to-change have been positively, and conservation values negatively, associated with age in children (Cieciuch et al., 2016; Tulviste et al., 2018). Childrens’ values have also been found to relate to potential consequences (e.g., value-expressive behavior; Vecchione et al., 2016) in a similar way to adults’ values.
While no studies were found to relate personal values to subjective wellbeing in middle childhood (defined as around 6 to 12 years of age, Collins, 1984; DelGiudice, 2018), mixed results have been found in adult and adolescent samples. In an effort to shed some light on why there may be inconsistencies in relations between values and subjective wellbeing, Schwartz and Sortheix (2018) suggest that inconsistencies may reflect different perspectives on how personal values influence subjective wellbeing. They point out that previous research considered these relations from three different perspectives: (1) a (un)healthy values perspective, (2) a goal attainment perspective, and (3) a value-congruence perspective. Specifically, subjective wellbeing may be influenced by values directly, due to the content of healthy versus unhealthy values and their underlying motivations, or indirectly, due to the potential for value attainment and/or the alignment of values with the prevailing culture or environment (i.e., value-congruence). The current study focuses on the (un)healthy values perspective in examining relations between values and subjective wellbeing in middle childhood, based on the previous adult research. This (un)healthy perspective of the content of values is grounded in self-determination theory (Deci & Ryan, 1985). This theory proposed that people experience higher wellbeing with three basic psychological needs are met (i.e., autonomy, relatedness and competence; Ryan, 2009).
Drawing on self-determination theory, Sagiv et al. (2015) argued that those values with intrinsically motivating content (e.g., self-direction) are healthy in that they promote wellbeing, whereas those values with extrinsically motivating content (e.g., conformity) are unhealthy in that they thwart or frustrate wellbeing. Bilsky and Schwartz (1994) originally argued that healthy values (i.e., hedonism, stimulation, self-direction, universalism, benevolence, and sometimes achievement) facilitate an individual’s growth needs, while unhealthy values (i.e., conformity, tradition, security, power and sometimes achievement) facilitate an individual’s self-protective needs. Sagiv and Schwartz (2000) later proposed that pursuing healthy values is more likely to lead to positive attitudes and behaviors that promote positive subjective wellbeing, whereas pursuing unhealthy values is more likely to lead to negative attitudes and behaviors that undermine subjective wellbeing. More recently, Schwartz and Sortheix (2018), proposed that healthy growth values promote subjective wellbeing as they motivate self-expansion, through self-actualization, free-expression, or a focus on the welfare of others.
While no studies were found to examine relations between childrens’ values and subjective wellbeing, other aspects of wellbeing have been examined, with mixed results. For instance, growth values were positively associated with psychological wellbeing in adolescents (Bojanowska & Piotrowski, 2018) and global self-worth in children (Collins et al., 2022), but not self-esteem in adolescents (Benish-Weisman et al., 2019). Thus, it is not obvious whether relations between healthy values and subjective wellbeing will be the same in children as they are for adults or adolescents. Therefore, this study examined whether the expected (un)healthy values-wellbeing relations are evident in middle childhood. Specifically, this study examined the pre-registered hypothesis that, in middle childhood:
-
H1: Growth values will be positively related to wellbeing.
In contrast, Schwartz and Sortheix (2018) also proposed that unhealthy anxiety values should undermine subjective wellbeing as they motivate the need to avoid threat and anxiety, through self-restriction, order and avoiding change or asserting control and dominance, to overcome anxiety. In adolescent and children’s samples, self-enhancement values located in the anxiety values region, were negatively associated with psychological wellbeing (Bojanowska & Piotrowski, 2018), psychological adjustment (Tamm et al., 2020), and self-esteem (Benish-Weisman et al., 2019; Collins et al., 2022); however, conservation values, which are also located in the anxiety values region, were positively associated with self-esteem and global self-worth (Benish-Weisman et al., 2019; Collins et al., 2022). Given this, the role of unhealthy values in explaining subjective wellbeing in middle childhood needs further investigation. Thus, this study examined the pre-registered hypothesis that, in middle childhood:
-
H2: Anxiety values will be negatively related to wellbeing.
Further, this study also examined age and gender differences in value-subjective wellbeing relations, as previous research found gender and age differences in the importance of specific values (Döring et al., 2015), As such, this study explored whether the hypothesized relations (H1 and H2) held across subsamples of (a) girls and (b) boys and (c) older and (d) younger children.
Values, and relations with potential consequences, are often examined in isolation. It is possible that one of the reasons for previous research finding mixed results in values and subjective wellbeing relations is due to other factors influencing these relations. One important factor in children’s wellbeing research is the role of social support. As such, this study examined the role of childrens’ perceptions of social support in value-wellbeing relations.
Perceived social support, which is defined as “an individual's perceptions of general support or specific supportive behaviors (available or enacted on) from people in their social network, which enhances their functioning or may buffer them from adverse outcomes” (Demaray & Malecki, 2002, p. 215), has been found to have a significant positive influence on subjective wellbeing (Goodwin et al., 2004). A meta analysis found that childrens’ perceptions of social support, including teacher support, were positively related to their wellbeing, and that the association between social support and wellbeing increased with age (see meta-analaysis, Chu et al., 2010). Further, relations between social support and self-esteem (Ikiz & Cakar, 2010), victimization and aggression (Jenkins & Demaray, 2012), and depression (Rueger et al., 2016) have also been found in adolescence. Specifically, perceived social support from parents, teachers, and friends were all positively related to self-esteem (Ikiz & Cakar, 2010), and negatively related to peer victimization and aggression (Jenkins & Demaray, 2012). Perceived social support from family (i.e., parents, grandparents/ siblings), teacher, classmate, and close friend also had a significant negative association with depression (see Rueger et al., 2016).
Social support has also been found to moderate relations between a range of different constructs and aspects of wellbeing. For instance, perceived social support moderated relations between social acceptance and wellbeing (Tian et al., 2015), bullying and wellbeing (Davidson & Demaray, 2007), and negative environmental factors (i.e., medically ill family member, abuse, trauma, low income) and wellbeing (see meta-analytic review; Rueger et al., 2016). Thus, this study examined the role of perceived social support on relations between values and subjective wellbeing in middle childhood. Therefore, this pre-registered hypothesis stated that in middle childhood:
-
H3: Social support will have a positive effect on the relationship between values and wellbeing.
This study also examined whether H3 held across subsamples of (a) girls and (b) boys and (c) older and (d) younger children. Past research has found girls perceived higher levels of classmate support than boys in perceptions of classmate social support (Danielsen et al., 2009; Rueger et al., 2010).
Perceived social support has also been found to mediate relations between different constructs and wellbeing. For instance, perceived social support has been found to mediate relations between problems in childhood/adolescence and wellbeing (Sánchez-Sandoval et al., 2019) and between parent involvement and psychological wellbeing (Hao et al., 2019). Thus, this study also explored whether perceived social support mediated relations between values and subjective wellbeing.
The current study
Despite growing evidence that individual differences in personal values influence subjective wellbeing in adolescents (e.g., Benish-Weisman et al., 2021; Bojanowska & Piotrowski, 2018; Solomon & Knafo, 2010; Tamm et al., 2021), little attention has been paid to these relations in middle childhood. Therefore, this pre-registered study sought to address important gaps in the literature by examining values and subjective wellbeing relations in middle childhood. Specifically, this study examined relations between personal values and subjective wellbeing from an (un)healthy values perspective, and whether perceived social support from parents, teachers, classmates, and close friends mediates, or moderates, values-wellbeing relations in middle childhood.
Method
Participants and procedures
As part of a larger study, participants were recruited from a convenience sample of two metropolitan primary schools in Western Australia. These were in areas with relatively high socioeconomic status (i.e., in the 10th decile for economic advantage vs. disadvantage, education, and occupation in Australia), and with 39% to 43% having both parents born overseas compared with the national average of 28% (Australian Bureau of Statistics, 2021). As data was collected over a two-week period, some participants were absent or unavailable for subsequent surveys. In total, 738 children, aged 6 to 12 years, first completed the personal values survey (50% female; Mage = 9.00, SD = 1.79). Of these, 718 completed the subjective wellbeing scale (50% female; Mage = 9.04, SD = 1.77) and 697 completed the social support scale (51% female; Mage = 9.00, SD = 1.79). These sample sizes were considered adequate for all analyses (see power analyses in Supplemental Materials S1). Ethics approval for this study was granted by The University of Western Australia, with opt-out consent. In total, the five children that were opted out by their parents, and children with neurotypical disorders (e.g., Autism), were excluded from the analysis.
After a brief introduction, children completed the values survey on iPads and at subsequent sessions, they completed the wellbeing and social support scales in their home classroom. Consideration was given for children’s phonological processing ability (i.e., ability to decode and read with understanding) for both paper surveys. Specifically, year 1 and 2 children (typically aged 5.5 to 7.5) were read the questionnaire in small groups or as a class, whereas in year 3 to 6 (typically aged 7.5 to 11.5), only those identified as having reading difficulties by their teachers, were read the questions.
Measures
Personal values were measured using the revised Animated Values Instrument (AVI-r; Lee et al., 2017). This measure is based on best–worst scaling theory (Louviere et al., 2015), which extends paired comparisons to the multiple-choice context. Specifically, participants were asked to choose which value animation is “most like you” and which is “least like you” from sets of five animations presented in each of 21 subsets (see Figures S1 & S2 in Supplemental materials for thumbnail animations/screen shot). These subsets were formed from a balanced Youden experimental design, where each animation was seen five times and each pair of animations was seen together once, across 21 subsets.
Values scores were calculated by the simple count method. The number of times a value was chosen as “least like you” was subtracted from the number of times the same value was chosen as “most like you” (see Louviere, et al., 2015). This score was then divided by the number of times the item appeared across the survey (i.e., 5 times), resulting in an 11-point scale (-1 to + 1), where higher scores reflect higher value importance and zero is the mid-point. Following Collins et al. (2017) this study found consistency of choice was a good marker of reliability in this sample (see Supplemental Materials S2).
Higher order values subscales were calculated by first averaging value items for the basic values scores and then averaging the basic values scores that reflect each higher-order value (see Benish-Weisman et al., 2019; Schwartz et al., 2012). Scores for growth values were computed by averaging scores for the higher order self-transcendence (i.e., universalism, benevolence) and openness-to-change values (i.e., self-direction, stimulation). Scores for anxiety values were computed by averaging scores for the higher order self-enhancement (i.e., power, achievement) and conservation values (i.e., tradition, conformity, security). Given that achievement can be considered either a healthy or an unhealthy value, this study examined the correlations between the 10 basic values in this sample (see Supplemental Materials Table S1). As achievement was positively correlated with power (an unhealthy value) and negatively with self-direction (a healthy value), achievement was included in the computation of anxiety values. Further, as hedonism was positively correlated with achievement values and negatively with self-direction values in this sample, its position as being healthy or unhealthy was uncertain, as such it was not included in scoring of either growth or anxiety values.
Subjective wellbeing was measured using the Personal Wellbeing Index – School Children (PWI-SC: Cummins & Lau, 2005). This is an established 8-item scale with good reliability and validity (Tomyn & Cummins, 2011; Tomyn et al., 2020). This scale includes the 7-item Personal Wellbeing Index (PWI) and an optional item about overall happiness in life. This study used only the 7-item PWI as multi-item scales are considered more reliable for measuring subjective wellbeing than a single item. Respondents are asked to indicate their level of happiness in seven life domains (i.e., standard of living, health, achievements, relationships, safety, future security, and community), on an 11-point scale with anchors at 0 (very sad), 5 (not happy or sad), and 10 (very happy). These are then combined to form the PWI. Cronbach’s alpha for the 7-item PWI was acceptable (α = 0.69).
Perceived social support was measured using the Social Support Scale for Children (SSSC: Harter, 2012), which has been reported as having good internal consistency, reliability, and validity (e.g., Gordon-Hollingsworth et al., 2015). The SSSC uses 6 items to measure perceived support for each of four categories: parents, classmates, teachers, and close friends. It uses a ‘structured alternative format’, where two opposing alternatives are presented (e.g., Some kids have parents who don’t seem to hear about their children’s problems BUT other kids have parents who do want to listen to their children’s problems), with the chosen alternative being rated as either Really True for me or Sort of True for me (see Harter, 2012). The most positive statement in each pair was scored as 4 (really true for me) or 3 (sort of true for me) and the least positive in each pair was scored as 1 (really true for me) or 2 (sort of true for me). Cronbach’s alpha was reasonable for each category: Parent support (α = 0.79); teacher support (α = 0.83); classmate support (α = 0.72); close friend support (α = 0.84).
Analytic strategy
Multidimensional scaling (MDS) PROXSCAL procedure (SPSSv29) with an initial theory driven custom configuration, ordinal proximity transformations, Euclidian distance measures, and Z-score transformations (following Schwartz et al., 2012), were used to examine whether the Schwartz (1992) theorized structure of basic values (see Fig. 1) was reflected in this sample. As both values and subjective wellbeing data were non-normally distributed, as is often found with values and subjective wellbeing (see Supplemental Materials Table S2, Figures S3-S5), Spearman’s rank order correlations were used to estimate relations between values and subjective wellbeing. Finally, to examine whether social support moderated or mediated these relations, this study used the SPSS PROCESS v3.4 macro (Hayes, 2018), with standardized variables, using the heteroscedasticity-consistent standard error estimator (HC3), and examining one standard deviation above and below the mean for the dependent variable. To determine whether the effects in the models were significant, this study used bootstrapping and 95% confidence intervals (CI). For moderation, Hayes Model 1 was used to examine each type of perceived social support separately (i.e., parent, teacher, classmate, close friend). For mediation, Hayes Model 4 was used to examine all four types of perceived social support in the one model.
Results
Descriptive statistics
The two-dimensional MDS map (see Fig. 2) supports the theoretical order of the Schwartz (1992) basic values, with the exception of benevolence and universalism, with benevolence being located closer to the center of the map. This has been found in other samples and is considered a minor deviation (e.g., Döring et al., 2015).

MDS for year 1 to 6 children. Note. N = 738 (Stress 1 = .092, DAF = .992); lines represent higher-order value regions
Descriptive statistics and correlations for all study variables are presented in Table 1. The means for subjective wellbeing and all four types of perceived social support were relatively high and positively related. In line with previous research (e.g., Mannerström et al., 2023; Ungvary et al., 2018), growth values were more important and anxiety values were less important on average in the sample.
Hypothesis testing
In support of Hypothesis 1 (pre-registered), the correlation between healthy growth values (i.e., self-transcendence, openness-to-change) and subjective wellbeing was positive overall (r = 0.14, p < 0.001). This was also the case for girls (r = 0.20, p < 0.001) and for older children (r = 0.16, p = 0.001), supporting H1a and c. However, these relations were not significant for boys (r = 0.10, p = 0.072), or for younger children (r = 0.09, p = 0.115), thus H1b and d were rejected.
Hypothesis 2 (pre-registered) was not supported at the sample level. That is, the correlation between unhealthy anxiety values (i.e., self-enhancement, conservation) and subjective wellbeing was not significant (r = -0.05, p = 0.185). At the subgroup level these relations were significant for girls (r = -0.14, p = 0.009), supporting H2a, but not for boys (r = -0.01, p = 0.841) or for older (r = -0.03, p = 0.511) or younger (r = -0.05, p = 0.405) children. Thus, H2b-d were rejected.Footnote 1
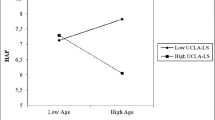
Hypothesis 3 (pre-registered) was not supported overall, with none of the four types of perceived social support (i.e., parent, teacher, classmate, or close friend) moderating relations between either growth values and subjective wellbeing or anxiety values and subjective wellbeing (see Table S3 in the supplemental materials). However, when this study explored whether perceived social support moderated relations between values and subjective wellbeing for gender and age subgroups, five significant results were found. For boys, perceived parent support positively moderated relations between growth values and subjective wellbeing (β = 2.68, 95% CIs [0.8, 4.6], p = 0.007) and negatively moderated relations between anxiety values and subjective wellbeing (β = -1.23, 95% CIs [-2.4, -0.1], p = 0.038), partially supporting H3b. For younger children, perceived classmate support negatively moderated relations between anxiety values and subjective wellbeing (β = -1.31, 95% CIs [-2.6, -0.16], p = 0.041), as did perceived friend support (β = -1.58, 95% CIs [-2.8, -0.3], p = 0.013). In contrast, for older children, perceived classmate support positively moderated relations between anxiety values and subjective wellbeing (β = 1.51, 95% CIs [0.2, 2.8], p = 0.024). For detailed results see Table S4a-d Supplemental Materials.
The significant moderation effects at the subsample level were probed further to test the significance of the slopes for three levels of perceived social support (− 1 SD, the mean, + 1 SD, respectively). Figure 3a, b shows how perceived parent support moderated relations between values and subjective wellbeing relations for boys. These results show that perceived parent support significantly increased subjective wellbeing for boys with higher, but not lower, growth values (see Fig. 3a). In contrast, perceived parent support significantly increased subjective wellbeing for boys with lower, but not higher, anxiety values (see Fig. 3b).

Moderation by perceived parent support for boys. a Moderation of relations between growth values (i.e., self-transcendence & openness-to-change) and subjective wellbeing relations by perceived parent support for boys. b Moderation of relations between anxiety values (i.e., self-enhancement & conservation) and subjective wellbeing by perceived parental support for boys. Red dots show relations between values and subjective wellbeing at the mean levels of parent support, with blue dots showing these relations at 1SD below the mean and green dots showing 1SD above the mean. Note. n's = 338
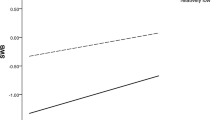
Figure 4a, b shows the different ways in which perceived classmate support moderated relations between values and subjective wellbeing for older and younger children. For older children, perceived classmate support significantly increased subjective wellbeing for those with higher, but not lower, anxiety values (see Fig. 4a). In contrast, for younger children, perceived classmate support significantly increased subjective wellbeing for those with lower, but not higher, anxiety values (see Fig. 4b). Similarly, for younger children, perceived close friend support significantly increased subjective wellbeing for those with lower, but not higher, anxiety values (see Fig. 4c).

Moderation by perceived social support by age. a Moderation of relations between anxiety values (i.e., self-enhancement & conservation) and subjective wellbeing by perceived classmate support for older children. Note. n = 398. b Moderation of relations between anxiety values (i.e., self-enhancement & conservation) and subjective wellbeing by perceived classmate support for younger children. Note. n = 287. c Moderation of relations between anxiety values (i.e., self-enhancement & conservation) and subjective wellbeing by perceived close friend support for younger children. Note: n = 287; Red dots show relations between values and subjective wellbeing at the mean levels of parent support, with blue dots showing these relations at 1SD below the mean and green dots showing 1SD above the mean
Social support as a possible mediator for values-subjective wellbeing relations
This study explored whether perceived social support mediated relations, either fully or partially, between childrens’ values and subjective wellbeing. This was done to see whether social support acts as a protective factor that nullifies the hypothesized relations between growth values and subjective wellbeing (H1), and anxiety values and subjective wellbeing relations (H2). The positive relations between growth values and subjective wellbeing (H1) were partially mediated by some, but not all, types of social support (see Fig. 5). Of the total effect (β = 1.73, p < 0.001), over half was accounted for by the direct effect of growth values on subjective wellbeing (β = 0.97, p = 0.031). However, significant indirect effects were also found through perceived parent and perceived classmate support, but this was not the case for perceived teacher or perceived close friend support. Further, growth values had a positive effect on perceived social support from parents, teachers, classmates, and close friends. This suggests that children who prioritise growth values perceive they have social support from their parents, teachers, classmates, and close friends, (See Fig. 5).

Mediation of relations between growth values (i.e., self-transcendence and openness-to-change) and subjective wellbeing by perceived social support. Note. N = 684; ns = not significant; *p < .05; **p < .01; ***p < .001
For anxiety values, neither the direct (β = 0.11) nor total effects (β = -0.36) on subjective wellbeing were significant (see Fig. 6). Again significant, but different, indirect effects were found for anxiety values on subjective wellbeing through perceived parent and perceived classmate support, but not for perceived teacher or perceived close friend support. However, anxiety values had negative effects on all four types of perceived social support. This suggests that children who prioritise anxiety values perceive they do not have social support from their parents, teachers, classmates, and close friends.

Mediation of relations between anxiety values (i.e., self-enhancement and conservation) and subjective wellbeing by perceived social support. Note. N = 684; ns = not significant; *p < .05; **p < .01; ***p < .001
Discussion
Previous research suggests early life experiences (e.g., Denny et al., 2004), social relationships (Heady et al., 2013), social support (e.g., Henderson, 1981), coping styles (Matud, 2004; Parker et al., 1998), and personality characteristics (Lucas, 2018) can help to shape responses to life stressors that impact mental health. Most of the research examining factors influencing childrens’ wellbeing have focused on contextual factors. Thus, the current study sought to examine whether children’s personal values are related to their subjective wellbeing, and whether these relations are moderated or mediated by perceived social support from parents, teachers, classmates, and close friends.
Findings from the current study suggest that some, but not all, personal values related to childrens’ subjective wellbeing. Specifically, healthy growth values were found to positively influence subjective wellbeing in middle childhood. It appears that children who place higher importance on healthy growth values (i.e., values that promote pursuit of autonomy and novelty or caring for the welfare of others) may have better wellbeing outcomes than those who place lower importance on these values. However, these findings were less clear for the proposition that unhealthy anxiety values being negatively associated with subjective wellbeing, as this was not found in the overall sample, but was found in the subsample of girls.
The finding that healthy growth values were related to higher levels of subjective wellbeing in middle childhood, extends findings from adult studies of values and subjective wellbeing (Sagiv and Schwartz (2000) and adolescent studies of values and psychological wellbeing (Bojanowska & Piotrowski, 2018). Thus, it appears that personal values relations with subjective wellbeing begin much earlier than previously thought.
While there is evidence that prioritizing unhealthy anxiety values are negatively associated with subjective wellbeing in adults (Sagiv & Schwartz, 2000), in the current study this was only the case for girls, but not for boys or younger and older children. This result reflects Schwartz and Sortheix (2018) finding that anxiety values were more strongly negatively associated with subjective wellbeing in females than males in adolescent and adult samples. However, more research is needed to understand reasons for these gender-based differences and to see whether they extend to other types of values-wellbeing relations (see Diener et al. 2017).
Past research has shown that girls tend to prioritize conservation values more than boys (e.g., Bilsky et al., 2015; Döring et al., 2015). Further, the school environment tends to promote and reward specific values, such as conformity, which encourage compliance with rules and the smooth functioning of social relations. Positive reinforcement of these motivational goals at school may, in turn, have a positive influence on subjective wellbeing. Given that a positive school climate is linked to a greater sense of life meaning when a stronger sense of belonging is felt (OECD, 2019c), future research might examine how value congruence with teachers and peers (i.e., value attainment and/or the alignment of values with the prevailing culture or environment) influences subjective wellbeing.
To move beyond examining the influence of values on subjective wellbeing in isolation, this study explored whether perceived social support would mediate relations between values and wellbeing, as social support is viewed as a protective factor in the field of mental health (Baumeister & Leary, 1995). These findings extend the literature by showing that healthy growth values are not only directly related to subjective wellbeing, but that perceived social support only partially mediates these relations. While it might be argued that actual social support might influence value development, past findings show that values are at least in part heritable (Twito & Knafo-Noam, 2020) and that they influence perceptions (Sagiv et al., 2017). Given that perceived social support is positively related to subjective wellbeing (Goodwin et al., 2004), the current research examined whether these perceptions mediate or moderate relations between personal values and subjective wellbeing.
This study found that children who prioritize healthy growth values perceived that they had greater social support from (a) parents, (b) teachers, (c) classmates, and (d) close friends. In contrast, children who prioritize unhealthy anxiety values perceived they had less social support from (a) parents, (b) teachers, (c) classmates, and (d) close friends. It may be the case that children who prioritize growth values have more of a growth mindset (i.e., a belief that your ability and intelligence can develop over time; Dweck, 2006), thus viewing social support from parents, teachers, classmates, and close friends as beneficial. Whereas those who prioritize anxiety values, may have more of a fixed mindset (i.e., your ability and intelligence cannot be altered by experience; Dweck, 2006) and thus do not see as much benefit from the social support of their parents, teachers, classmates, and close friends. However, more research is required to examine these ideas.
While this study did not find an overall (preregistered) moderation effect for perceived social support on values-subjective wellbeing relations, it found some interesting patterns of moderation within subgroups. Specifically, the study found that for boys, perceived parent support increased subjective wellbeing for those with higher, but not lower growth values, and conversely, it increased subjective wellbeing for those with lower, but not higher anxiety values. Future research should test the independence of these effects, as those high on growth values may be lower on anxiety values and vice versa. However, it is also possible that children who are high on growth values have parents who are more likely to reinforce their values, whereas those who are higher on anxiety values do not feel the same level of reinforcement. Previous research suggests parent–child value similarity may be reciprocal (Grusec & Goodnow, 1994; Knafo & Galansky, 2008; Knafo & Schwartz, 2009) and when values align subjective wellbeing is higher (Flurry et al., 2021). This might suggest that value congruence between parents and children is important to their perceptions of social support. However, further research is required to examine these ideas.
Interestingly, this study found contrasting moderation effects for perceived classmate support on relations between anxiety values and subjective wellbeing for older versus younger children. Specifically, for older children with higher anxiety values, their perceived classmate support was associated with greater subjective wellbeing, whereas for younger children with lower anxiety values, their perceived classmate and friend support was positively associated with subjective wellbeing. These contrasting effects between older and younger children may explain why this study did not find direct associations between anxiety values and subjective wellbeing at the sample level. Further research is needed to understand whether this is due to an increase in peer influence in older children, as social support has been found to be more important with age in childhood (Chu et al., 2010).
Practical implications, limitations, and future directions
Schools are not only expected to improve the academic outcomes of their students, but increasingly their wellbeing (OECD, 2019a, b, c, d). This emphasis on student wellbeing is reflected in the high number of wellbeing programs being offered in schools (Dix et al., 2020a). However, even though some research suggests small but positive outcomes (Fenwick-Smith et al., 2018; Ferreira Lima & Araujo de Morais, 2018; Goldberg et al., 2019; Kumar & Mohideen, 2019; Tomé et al., 2021), criticism of school-based wellbeing programs has focused on their ‘one size fits all’ approach (e.g., Street, 2017; Weare & Nind, 2011), and the lack of robust research designs or high quality empirical evidence (see review Dix et al., 2020a; 2020b). This highlights the need for schools to match wellbeing programs with specific problems, including intrapersonal (e.g., internalizing behavior) and interpersonal domains (e.g., bullying), as well as student competencies, such as self-awareness (i.e., insight building) and problem solving (see meta-analysis, Mertens et al., 2020). The current research may help practitioners to think about ways of individualizing their programs. Future studies could compare the effectiveness of 'one size fits' programs with more individualized programs.
As with all research, this study had some limitations. First, as with almost all values research, this study relied on self-reports for values, perceived social support and subjective wellbeing. While self-reporting can be subject to social desirability bias, Schwartz et al. (1997) argue that social desirability is a personality trait that is meaningfully related to value importance. While motivational goals, happiness and perceptions are not directly observable, prompting researchers to ask respondents directly (using self-reports), behaviors may indicate propensity toward these factors. As such, future research should examine peer and teacher reports of behaviors that can reflect these constructs. To further ameliorate possible biases associated with self-reports, this study administered each of the surveys separately using an online survey for values and paper-based surveys for other constructs, over a two-week timeframe. Future studies could also consider direct measures of actual social support, as a possible protective factor (Lyell et al., 2020), as well as different indicators of wellbeing (Rueger, et al., 2016).
Second, participants were recruited from schools located in areas with relatively high socioeconomic status (i.e., 10th decile for economic advantage vs. disadvantage, education, and occupation; Australian Bureau of Statistics, 2021). Additionally, this study was undertaken in just one country, Australia. However, the sample could be considered to be culturally diverse, as schools were located in areas with relatively high proportions of adults born overseas (i.e., 39–43% having both parents born overseas compared with the national average of 28%; Australian Bureau of Statistics, 2021). Despite this, future research should examine values-wellbeing relations in more diverse school populations.
Conclusion
Improving the wellbeing of school children is a clear aim around the world, with countries, like Australia, producing wellbeing frameworks (i.e., Education Council, 2018; Goodhue et al., 2021), and the Council of Europe (2023) and OECD countries endorsing the PISA 2018 Wellbeing Framework (OECD, 2019d). While institutions focusing on wellbeing in childhood recognize the importance of values (OECD, 2019a), our study is the first to show clear associations between personal values, subjective wellbeing and perceived social support in middle childhood. Thus, this study paves the way for a deeper understanding of how such individual differences in childhood can inform the practice of wellbeing support in schools.
Data Availability
Data sharing is not possible due to confidentiality in our ethics application.
Notes
As suggested by a reviewer, relations between person- and social-focused values and subjective wellbeing were also tested at the sample level; however, the results were less compelling see Supplemental materials S3.
References
AIHW. (2020). Australia's Children. Australian Institute of Health and Welfare. Retrieved March 20, 2021 from https://www.aihw.gov.au/getmedia/6af928d6-692e-4449-b915-cf2ca946982f/aihw-cws-69-print-report.pdf.aspx?inline=true
Allport, G. W., Vernon, P. E., & Lindsey, G. (1960). Study of values (3rd ed.). Houghton Mifflin.
Anglim, J., Horwood, S., Smillie, L. D., Marrero, R. J., & Wood, J. K. (2020). Predicting psychological and subjective well-being form personality: A meta-Analysis. Psychological Bulletin, 146(4), 279–323. Retrieved July 2, 2021 from https://doi.apa.org/doiLanding?doi=10.1037%2Fbul0000226
Australian Bureau of Statistics. (2021). Data by region summary. Australian Bureau of Statistics. Retrieved July 20, 2022 from https://www.abs.gov.au/
Baumeister, R. F., & Leary, M. R. (1995). The need to belong: Desire for interpersonal attachments as a fundermental human motivation. Psychological Bulletin, 117(3), 497–529.
Benish-Weisman, M., Daniel, E., & McDonald, K. L. (2019). Values and adolescents’ self-esteem: The role of value content and congruence with classmates. European Journal of Social Psychology, 50(1), 207–223. https://doi.org/10.1002/ejsp.2602
Benish-Weisman, M., Oreg, S., & Berson, Y. (2021). The contribution of peer values to children’s values and behavior. Personality and Social Psychology Bulletin. https://doi.org/10.1177/01461672211020193
Bilsky, W., & Schwartz, S. H. (1994). Values and personality. European Journal of Personality, 8, 163–181. https://doi.org/10.1002/per.2410080303
Bilsky, W., Doring, A. K., & Groenen, P. J. F. (2015). Assessing the fit of each item of the 'Pictured-Based Survey for Children' into the theoretical structure of values 15th International Facet Theory Conference, Fordham University NY. https://www.researchgate.net/publication/317182170_Assessing_the_fit_of_each_item_of_the_'Picture_based_Value_Survey_for_Children'_into_the_theoretical_structure_of_values
Bojanowska, A., & Piotrowski, K. (2018). Values and psychological well-being among adolescents - are some values “healthier” than others? European Journal of Developmental Psychology. https://doi.org/10.1080/17405629.2018.1438257
Borg, I. (2019). Age-and gender-related differences in the structure and the meaning of personal values. Personality and Individual Differences, 138, 336–343. https://doi.org/10.1016/j.paid.2018.10.013
Brockevelt, B. L., Cerny, S. L., Newland, L. A., & Lawler, M. J. (2019). Activities within an ecological, relationship-based model of children’s subjective well-being. Child Indicators Research, 12, 589–608. https://doi.org/10.1007/s12187-018-9563-2
Chu, P. S., Saucier, D. A., & Hafner, E. (2010). Meta-analysis of the relationships between social support and well-being in children and adolescents. Journal of Social and Clinical Psychology, 29(6), 624–645. https://doi.org/10.1521/jscp.2010.29.6.624
Cieciuch, J., Davidov, E., & Algesheimer, R. (2016). The stability and change of value structure and priorities in childhood: A longitudinal study. Social Development, 25(3), 503–527. https://doi.org/10.1111/sode.12147
Collins, A. W. (1984). The status of basic research on middle childhood: The years from six to twelve. In A. W. Collins (Ed.), Development during middle childhood: The years from six to twelve (pp. 398–421). National Academy Press.
Collins, P. R., Lee, J. A., Sneddon, J. A., & Döring, A. K. (2017). Examining the consistency and coherence of values in young children using a new animated values instrument. Personality and Individual Differences, 104, 279–285. https://doi.org/10.1016/j.paid.2016.08.024
Collins, P. R., Sneddon, J. A., & Lee, J. A. (2022). Do Personal Values have an effect on self-esteem in middle childhood? Personality and Individual Differences, 199. https://doi.org/10.1016/j.paid.2022.111861
Council of Europe. (2023). Improving well-being at school. Retrieved 12 June 2023 from https://www.coe.int/en/web/campaign-free-to-speak-safe-to-learn/improving-well-being-at-school
Cummins, R. A., & Lau, A. L. D. (2005). Manual of the Personal Wellbeing Index: School Children (PWI-SC) (English) (3rd ed.). School of Psychology, Deakin University.
Daniel, E., Benish-Weisman, M., Sneddon, J. A., & Lee, J. A. (2020). Value profiles during middle childhood: Developmental processes and social behavior. Child Development. https://doi.org/10.1111/cdev.13362
Danielsen, A. G., Samdal, O., Hetland, J., & Wold, B. (2009). School-related social support and students’ perceived life satisfaction. The Journal of Educational Research, 102(4), 303–320. https://doi.org/10.3200/JOER.102.4.303-320
Datu, J. A. D., & King, R. B. (2018). Subjective well-being is reciprocally associated with academic engagement: A two-wave longitudinal study. Journal of School Psychology, 69, 100–110. https://doi.org/10.1016/j.jsp.2018.05.007
Davidson, L. M., & Demaray, M. K. (2007). Social support as a moderator between victimization and internalizing-externalizing distress from bullying. School Psychology Review, 36(3), 383–405. https://doi.org/10.1080/02796015.2007.12087930
Deci, E. L., & Ryan, R. M. (1985). Intrinsic motivation and self-determination theory in human behavior. Plenum.
DelGiudice, M. (2018). Middle childhood: An evolutionary-developmental synthesis. In N. Halfon, C. B. Forrest, R. M. Lerner, & E. M. Faustman (Eds.), Handbook of life course health development. Springer Nature. https://doi.org/10.1007/978-3-319-47143-3
Demaray, M. K., & Malecki, C. K. (2002). Critical levels of perceived social support associated with student adjustment. School of Psychology Quarterly, 17, 213–241. https://doi.org/10.1521/scpq.17.3.213.20883
Denny, S., Clark, T., Fleming, T., & Wall, M. (2004). Emotional resilience: Risk and protective factors for depression among alternative education students in New Zealand. American Journal of Orthopsychiatry, 74, 137–149. https://doi.org/10.1037/0002-9432.74.2.137
Diener, E., Pressman, S. D., Hunter, J., & Delgadillo-Chase, D. (2017). If, why, and when subjective well-being influences health, and future needed research. Applied Psychology, Health and Well-Being, 9(2), 133–167. https://doi.org/10.1111/aphw.12090
Dix, K., Ahmed, S. K., Carslake, T., Sniedze-Gregory, S., O’Grady, E., & Trevitt, J. (2020a). Student health and wellbeing: A systematic review of intervention research examining effective student wellbeing in schools and their academic outcomes. Evidence for Learning, Issue. Retrieved July 2, 2021 from https://www.evidenceforlearning.org.au/assets/Uploads/Main-Report-Student-Health-and-Wellbeing-Systematic-Review-FINAL-25-Sep-2020.pdf
Dix, K., Kashfee, S. A., Carslake, T., Sniedze-Gregory, S., O’Grady, E., & Trevitt, J. (2020b). A systematic review of intervention research examining effective student wellbeing in schools and their academic outcomes. Addendum: Wellbeing Programs in Australia. Evidence for Learning, Issue. Retrieved May 7, 2021 from https://d288jieqo2x7eq.cloudfront.net/documents/pages/Addendum-Student-Health-and-Wellbeing-Systematic-Review-FINAL-25-Sep-2020.pdf?v=1648704187
Döring, A. K., Blauensteiner, A., Aryus, K., Drogekamp, L., & Bilsky, W. (2010). Assessing values at an early age: The picture-based value survey for children (PBVS-C). Journal of Personality Assessment, 92(5), 439–448. https://doi.org/10.1080/00223891.2010.497423
Döring, A. K., Schwartz, S. H., Cieciuch, J., Groenen, P., Glatzel, G., Harasimczuk, J., ... Bilsky, W. (2015). Cross-cultural evidence of value structures and priorities in childhood. British Journal of Psychology, 106, 675–699. https://doi.org/10.1111/bjop.12116
Dweck, C. S. (2006). Mindset: The new psychology of success. Random House.
Education Council. (2018). Australian student wellbeing framework. Education Services Australia. Retrieved August 20, 2021 from https://studentwellbeinghub.edu.au/educators/resources/australian-student-wellbeing-framework/
Elizarov, E., Benish-Weisman, M., & Ziv, Y. (2023). Teacher–child relational conflict and maladaptive social behaviors: The moderating role of children’s values. Journal of Experimental Child Psychology, 233, 105689. https://doi.org/10.1016/j.jecp.2023.105689
Fenwick-Smith, A., Dahlberg, E. E., & Thompson, S. C. (2018). Systematic review of resilience-enhancing, universal, primary school-based mental health promotion programs. BMC Psychology, 6(30), 6. https://doi.org/10.1186/s40359-018-0242-3
Ferreira Lima, R. F., & Araujo de Morais, N. (2018). Subjective well-being of children and adolescents: integrative review. Ciencias Psicológicas (Psychological Sciences), 12(2), 249–260. https://doi.org/10.22235/cp.v12i2.1689
Flurry, L. A., Swimberghe, K., & Allen, J. (2021). Exposing the moderating impact of parent-child value congruence on the relationship between adolescents’ materialism and subjective wellbeing. Journal of Business, 128, 290–302. https://doi.org/10.1016/j.jbusres.2021.02.005
Goldberg, J. M., Sklad, M., Elfrink, T. R., Schreurs, K. M. G., Bohlmeijer, E. T., & Clarke, A. M. (2019). Effectiveness of interventions adopting a whole school approach to enhancing social and emotional development: A meta-analysis. European Journal of Psychology of Education, 34(4), 755–782. https://doi.org/10.1007/s10212-018-0406-9
Goodhue, R., Dakin, P., & Noble, K. (2021). What's in the nest? Exploring Australia's wellbeing framework for children and young people. Canberra: ARACY Retrieved August 20, 2021 from https://www.aracy.org.au/documents/item/700
Goodsell, B., Lawrence, D., Ainley, J., Sawyer, M., Zubrick, S., & Maratos, J. (2017). Child and adolescent metal health and educational outcomes. An analysis of educational outcomes from Young Minds Matter: the scecond Australian Child and Adolescent Survey of Mental Health and Wellbeing. G. S. o. E. Perth, The University of Western Australia. Retrieved September 29, 2019 from https://youngmindsmatter.telethonkids.org.au/siteassets/media-docs---young-minds-matter/childandadolescentmentalhealthandeducationaloutcomesdec2017.pdf
Goodwin, R., Costa, P., & Adonu, J. (2004). Social support and its consequences: “Positive” and “deficiency” values and their implications for support and selfesteem. British Journal of Social Psychology, 43, 465–474. https://doi.org/10.1348/0144666042038006
Gordon-Hollingsworth, A. T., Thompson, J. E., Geary, M. A., Schexnaildre, M. A., S., L. B., & Kelley, M. L. (2015). Social support questionnaire for children: development and initial validation. Measurement and Evaluation in Counseling and Development, 1–23. https://doi.org/10.1177/0748175615596780
Grusec, J. E., & Goodnow, J. J. (1994). Impact of parental dicipline methods on the child’s internalization of values: A reconceptualization of current points of view. Developmental Psychology, 30, 4–19.
Hao, K. Y., Aqeel, K., & Siang, T. J. (2019). Social support as mediating effect of psychological well-being amongst emerging adolescents Indian Journal of Public Health Research & Development, 10(6). https://doi.org/10.5958/0976-5506.2019.01487.6
Harter, S. (2012). Social support scale for children: Manual and Questionnaires. University of Denver.
Hayes, A. F. (2018). Introduction to mediation, moderation, and conditional process analysis: A regression based approach. The Guildford Press.
Heady, B., Muffels, R., & Wagner, G. G. (2013). Choices Which Change Life Satisfaction: Similar Results for Australia, Britain and Germany. Social Indicators Research, 112, 725–748. https://doi.org/10.1007/s11205-012-0079-8
Henderson, S. (1981). Social relationships, adversity and neurosis: An analysis of prospective observations. British Journal of Psychiatry, 138, 391–398. https://doi.org/10.1192/bjp.138.5.391
Ikiz, F. E., & Cakar, F. S. (2010). Perceived social support and self-esteem in adolescence. Procedia Social and Behavioral Sciences, 5, 2338–2342. https://doi.org/10.1016/j.sbspro.2010.07.460
Jenkins, L. N., & Demaray, M. K. (2012). Social support and self-concept in relation to peer victimization and peer aggression. Journal of School Violence, 11(1), 56–74. https://doi.org/10.1080/15388220.2011.630958
King, R. B., & Datu, J. A. (2017). Happy classes make happy students: Classmates’ well-being predicts individual student well-being. Journal of School Psychology, 65, 116–128. https://doi.org/10.1016/j.jsp.2017.07.004
Knafo, A., & Galansky, N. (2008). The influence of children on their parents’ values. Social and Personality Psychology Compass, 2(3), 1143–1161. https://doi.org/10.1111/j.1751-9004.2008.00097.x
Knafo, A., & Schwartz, S. H. (2009). Accounting for parent-child value congruence: Theoretical considerations and empirical evidence. In U. Schonpflug (Ed.), Culteral transmission: Psychological, developmental, social, and methodological aspects (pp. 240–268). Cambridge University Press.
Kumar, A., & Mohideen, F. (2019). Strengths-based positive schooling interventions: A scoping review. Contemporary School Psychology. https://doi.org/10.1007/s40688-019-00260-1
Lee, J. A., Ye, S., Sneddon, J. A., Collins, P. R., & Daniel, E. (2017). Does the intra-individual structure of values exist in young children? Personality and Individual Differences, 110, 125–130. https://doi.org/10.1016/j.paid.2017.01.038
Louviere, J., Flynn, T. N., & Marley, A. A. J. (2015). Best-Worst Scaling: Theory. Cambridge University Press.
Lucas, R. E. (2018). Exploring the associations between personality and subjective well-being. DEF Publishers. https://doi.org/Noblascholar
Lyell, K. M., Coyle, S., Malecki, C. K., & Santuzzi, A. M. (2020). Parent and peer social support compensation and internalizing problems in adolescence. Journal of School Psychology, 83, 25–49. https://doi.org/10.1016/j.jsp.2020.08.003
Malhotra, S., & Patra, B. N. (2014). Prevalence of child and adolescent psychiatric disorders in India: a systematic review and meta-analysis. Child and Adolescent Psychiatry and Mental Health, 8, 22. https://doi.org/10.1186/1753-2000-8-22
Mannerström, R., Hietajärvi, L., Kuusisto, A., Salmela-Aro, K., & Kallioniemi, A. (2023). Value Profles among Finnish adolescents and their associations with subjective and social well-being. Child Indicators Research, 16, 509–531. https://doi.org/10.1007/s12187-022-09992-8
Matud, M. (2004). Gender differences in stress and coping styles. Personality and Individual Differences, 37, 1401–1415. https://doi.org/10.1016/j.paid.2004.01.010
Mertens, E., Dekovic, M., Leijten, P., Van Londen, M., & Reitz, E. (2020). Components of school-based interventions stimulating students’ intrapersonal and interpersonal domains: a meta-analysis. Clinical Child and Family Psychology Review, 23(4), 605–631. https://doi.org/10.1007/s10567-020-00328-y
Newlove-Delgado, T., McManus, S., Sadler, K., Thandi, S., Vizard, T., Cartwright, C., & Ford, T. (2021). Child mental health in England before and during the COVID-19 lockdown. Lancet Psychiatry, 8(5), 353–354. https://doi.org/10.1016/S2215-0366(20)30570-8
OECD. (2019a). OECD Future of education and skills 2030: OECD learning compass 2030. OECD. Retrieved November, 26, 2021 from https://www.oecd.org/education/2030-project/teaching-and-learning/learning/learning-compass-2030/OECD_Learning_Compass_2030_concept_note.pdf
OECD. (2019b). PISA 2018 assessment and analytical framework. OECD Publishing. https://doi.org/10.1787/b25efab8-en
OECD. (2019c). PISA 2018 results (Volume III): What school life means for students’ lives. OECD Publishing. https://doi.org/10.1787/acd78851-en
OECD. (2019d). PISA 2018 Well-being Framework. PISA 2018 Assessment and Analytical Framework (pp. 257–298). OECD Publishing. https://doi.org/10.1787/38a34353-en
Parker, G., Roy, K., Wilhelm, K., Austin, M., Mitchell, P., & Hadzi-Pavlovic, D. (1998). “Acting out” and “acting in” as behavioral responses to stress: A qualitative and quantitative study. Journal of Personality Disorder, 12, 338–350. https://doi.org/10.1521/pedi.1998.12.4.338
Rees, G. (2019). Variations in children's affective subjective well-being at seven years old: An analysis of current and historical factors. Child Indicators Research, 12, 141–160. Retrieved July 2, 2021 from https://link.springer.com/article/10.1007%2Fs12187-017-9516-1
Rokeach, M. (1973). The nature of human values. Free Press.
Rueger, S. Y., Malecki, C. K., Pyun, Y., Aycock, C., & Coyle, S. (2016). A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychological Bulletin. https://doi.org/10.1037/bul0000058
Rueger, S. Y., Malecki, C. Y., & Demaray, M. K. (2010). Relationship between multiple sources of perceived social support and psychological and academic adjustment in early adolescence: Comparisons across gender. Journal of Youth Adolescence, 39, 47–61. https://doi.org/10.1007/s10964-008-9368-6
Ryan, R. (2009). Self determination theory and well being. Social Psychology, 84(822), 848.
Sagiv, L., Roccas, S., Cieciuch, J., & Schwartz, S. H. (2017). Personal values in human life. Nature. https://doi.org/10.1038/s41562-017-0185-3
Sagiv, L., Roccas, S., & Oppenheim-Weller, S. (2015). Values and Well-being. In S. Joseph (Ed.), Positive psychology in practice: Promoting human flourishing in work, health, education, and everyday life (2nd ed.). Wiley. https://doi.org/10.1002/9781118996874.ch7
Sagiv, L., & Schwartz, S. H. (2000). Value priorities and subjective well-being: Direct relations and congruity effects. European Journal of Social Psychology, 30, 177–198. https://doi.org/10.1002/(SICI)1099-0992(200003/04)30:2%3c177::AID-EJSP982%3e3.0.CO;2-Z
Sánchez-Sandoval, Y., Melero, S., & López-Jiménez, A.-M. (2019). Mediating effects of social support in the association between problems in childhood and adolescence and well-being in adult domestic adoptees. Journal of Happiness Studies. https://doi.org/10.1007/s10902-019-00124-8
Schwartz, S. H. (1992). Universals in the content and structure of values: Theoretical advances and empirical tests in 20 countries. In M. P. Zanna (Ed.), Advances in Experimental Social Psychology (Vol. 25, pp. 1–25). Elsevier. https://doi.org/10.1016/S0065-2601(08)60281-6
Schwartz, S. H. (1994). Are there universal aspects in the structure and contents of human values? Journal of Social Issues, 50(4), 19–45. https://doi.org/10.1111/j.1540-4560.1994.tb01196.x
Schwartz, S. H., Cieciuch, J., Vecchione, M., Davidov, E., Fisher, R., C., B., ... Konty, M. (2012). Refining the theory of basic individual values: New concepts and measurements. Journal of Personality and Social Psychology, 103(4), 663-668.https://doi.org/10.1037/a0029393
Schwartz, S. H., & Sortheix, F. M. (2018). Values and subjective well-being. In E. Diener, S. Oishi, & L. Tay (Eds.), Handbook of well-being. DEF Publishers. Nobascholar.com.
Schwartz, S. H., Verkasalo, M., Antonovsky, A., & Sagiv, L. (1997). Value priorities and social desirability: Much substance, some style. British Journal of Social Psychology, 36, 3–18. https://doi.org/10.1111/j.2044-8309.1997.tb01115.x
Solomon, S., & Knafo, A. (2010). Value similarity in adolescent friendships. In J. C. Toller (Ed.), Friendships: Types, Cultural, Psychological and Social Aspects (6th ed.). Nova Science Publishers Inc.
Sortheix, F. M., & Schwartz, S. H. (2017). Values that underlie and undermine well-being: Variability across countries. European Journal of Personality, 31, 181–201. https://doi.org/10.1002/per.2096
Steel, P., Schmidt, J., & Shultz, J. (2008). Refining the relationship betwen personality and subjective well-being. Psychological Bulletin, 134(1), 138–161. Retrieved June 28, 2021 from http://hdl.handle.net/1880/47915
Street, H. (2017). Measures of success: Exploring the inportance of context in the delivery of well-being and social and emotional learning programs in Australian primary and secondary schools. In E. Frydenberg, A. J. Martin, & R. J. Collie (Eds.), Social and emotional learning in Australia and the Asia-Pacific. Springer Nature.
Suldo, S., Thalji, A., & Ferron, J. (2011). Longitudinal academic outcomes predicted by early adolescents’ subjective well-being, psychopathology, and mental health status yielded from a dual factor model. The Journal of Positive Psychology, 6(1), 17–30. https://doi.org/10.1080/17439760.2010.536774
Tamm, A., & Tulviste, T. (2022). Children's values in early childhood: Age differences in structure and priorities. Personality and Individal Differences, 184. https://doi.org/10.1016/j.paid.2021.111196
Tamm, A., Tulviste, T., & Tonissaar, M. (2020). Values of adolescents and values prevailing in the classroom are related to adolescents' psychological adjustment. European Journal of Developmental Psychology, 18(1), 54–74. Retrieved July 21, 2021 from https://www.tandfonline.com/doi/full/10.1080/17405629.2020.1755250
Tian, L., Zhao, J., & Huebner, E. S. (2015). School-related social support and subjective well-being in school among adolescents: The role of self-system factors. Journal of Adolescence, 45, 138–148. https://doi.org/10.1016/j.adolescence.2015.09.003
Tomé, G., Almeida, A., Ramiro, L., Gaspar, T., & Gaspar de Matos, M. (2021). Intervention in Schools promoting mental health and wellbeing: a systematic review. Global Journal of Community Psychology Practice, 12(1), 1–23. Retrieved May 17, 2021 from http://www.gjcpp.org/
Tomyn, A. J., & Cummins, R. A. (2011). The subjective wellbeing of high-school students: validating the personal wellbeing index—school children. Social Indicators Research, 101, 405–414. https://doi.org/10.1007/s11205-010-9668-6
Tomyn, A. J., Stokes, M. A., Cummins, R. A., & Dias, P. C. (2020). A rasch analysis of the personal wellbeing index in school children. Evaluation & the Health Professions, 43(2), 110–119. https://doi.org/10.1177/0163278718819219
Tulviste, T., Harro, H., & Tamm, A. (2018). Values structure and priorities in Estonian children: Using the picture-based value survey for children (PBVS-C). Child Indicators Research, 11, 1817–1829. https://doi.org/10.1007/s12187-017-9512-5
Twito, L., & Knafo-Noam, A. (2020). Beyond culture and the family: Evidence from twin studies on the genetic and environmental contribution to values. Neuroscience and Biobehavioral Reviews, 112, 135–143. https://doi.org/10.1016/j.neubiorev.2019.12.029
Ungvary, S., McDonald, K. L., & Benish-Weisman, M. (2018). Identifying and distinguishing value profiles in American and Israeli adolescents. Journal of Research on Adolescence, 28(2), 294–309. https://doi.org/10.1111/jora.12330
Vecchione, M., Döring, A. K., Alessandri, G., Marsicano, G., & Bardi, A. (2016). Reciprocal relations across time between basic values and value-expressive behaviors: A longitudinal study among children. Social Development, 25(3), 528–547. https://doi.org/10.1111/sode.12152
Wang, C., Williams, K. E., Shahaeian, A., & Harrison, L. J. (2018). Early predictors of escalating internalizing problems across middle childhood. School Psychology Quarterly, 33(2), 200–212. https://doi.org/10.1037/spq0000218
Weare, K., & Nind, M. (2011). Mental health promotion and prevention in schools: What does the evidence say? Health Promation International, 26(S1), 29–69. https://doi.org/10.1093/heapro/dar075
Acknowledgements
We acknowledge The University of Western Australia for funding this research and we also thank the students and staff at our participating schools.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. This project was supported by research grant funding awarded to Prof. Julie Lee from the University of Western Australia.
Author information
Authors and Affiliations
Contributions
Patricia Collins: Conceptualization, Data curation, Formal analyses, Methodology, Writing – original draft.
Joanne Sneddon: Conceptualization, Writing – review & editing.
Julie Lee: Conceptualization, Funding acquisition, Data curation, Formal Analysis, Methodology, Writing – review & editing.
Corresponding author
Ethics declarations
Research involving human participants
This research has Human Research Ethics Committee Approval #: RA/4/1/5188 from The University of Western Australia.
Informed consent
Opt-out parent consent was used in this research. School principals representing both government and private school systems gave consent before the research project began.
Disclosure of potential conflicts of interest
There are no relevant financial or nonfinancial competing interests for any of the authors. Data sharing is not possible due to confidentiality in our ethics application.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Patricia R. Collins. School of Education, Edith Cowan University, Perth, Australia.
Current themes of research:
Values and their impact on wellbeing. Behavior & friendships in children; and the values of preservice teachers and teachers and value congruence in the classroom.
Joanne Sneddon. Centre for Human and Cultural Values, UWA Business School, The University of Western Australia, Perth, Australia.
Current themes of research:
Values and prosocial behavior in adults and children.
Julie Anne Lee. Centre for Human and Cultural Values, UWA Business School, The University of Western Australia, Perth, Australia.
Current themes of research:
Values theory. Methodology and expression in adults and children.
Most relevant publications:
Benish-Weisman, M., Daniel, E., Sneddon, J., & Lee, J. (2019). The relations between values and prosocial behavior among children: The moderating role of age. Personality and Individual Differences, 141, 241-247.
Collins, P. R., Lee, J. A., Sneddon, J. N., & Döring, A. K. (2017). Examining the consistency and coherence of values in young children using a new Animated Values Instrument. Personality and Individual Differences, 104, 279-285.
Collins, P. R., Sneddon, J., & Lee, J. A. (2022). Do personal values have an effect on self-esteem in middle childhood? Personality and Individual Differences, 199, 111861.
Daniel Ella, Benish‐Weisman Maya, Sneddon Joanne N, & Lee Julie A. (2020). Value profiles during middle childhood: Developmental processes and social behavior. Child Development, 91, 5: 1615-1630.
Lee, J. A., Ye, S., Sneddon, J. N., Collins, P. R., & Daniel, E. (2017). Does the intra-individual structure of values exist in young children? Personality and Individual Differences, 110, 125-130.
Pre-registration: The current, study was pre-registered in 2021 https://aspredicted.org/7VS_JM3.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Collins, P.R., Sneddon, J. & Lee, J.A. Personal values, subjective wellbeing, and the effects of perceived social support in childhood: A pre-registered study. Eur J Psychol Educ (2024). https://doi.org/10.1007/s10212-024-00800-1
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10212-024-00800-1