
Abstract
Background
Around 2 million people in the UK suffer from Long COVID (LC). Of concern is the disease impact on productivity and informal care burden. This study aimed to quantify and value productivity losses and informal care receipt in a sample of LC patients in the UK.
Methods
The target population comprised LC patients referred to LC specialist clinics. The questionnaires included a health economics questionnaire (HEQ) measuring productivity impacts, informal care receipt and service utilisation, EQ-5D-5L, C19-YRS LC condition-specific measure, and sociodemographic and COVID-19 history variables. Outcomes were changes from the incident infection resulting in LC to the month preceding the survey in paid work status/h, work income, work performance and informal care receipt. The human capital approach valued productivity losses; the proxy goods method valued caregiving hours. The values were extrapolated nationally using published prevalence data. Multilevel regressions, nested by region, estimated associations between the outcomes and patient characteristics.
Results
366 patients responded to HEQ (mean LC duration 449.9 days). 51.7% reduced paid work hours relative to the pre-infection period. Mean monthly work income declined by 24.5%. The average aggregate value of productivity loss since incident infection was £10,929 (95% bootstrap confidence interval £8,844-£13,014) and £5.7 billion (£3.8-£7.6 billion) extrapolated nationally. The corresponding values for informal caregiving were £8,726 (£6,247-£11,204) and £4.8 billion (£2.6-£7.0 billion). Multivariate analyses found significant associations between each outcome and health utility and C19-YRS subscale scores.
Conclusion
LC significantly impacts productivity losses and provision of informal care, exacerbated by high national prevalence of LC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
The term ‘Long COVID’ (LC) covers two conditions: (i) ‘ongoing symptomatic COVID-19’ for signs and symptoms of acute COVID-19 between 4 and 12 weeks after the incident COVID-19 infection; and (ii) ‘post-COVID-19 syndrome’ for signs and symptoms beyond 12 weeks not explained by an alternative diagnosis [1]. As of 5th March 2023, around 1.9 million people in the UK had self-reported LC, 41% of whom self-reported the condition 2 years or more after the incident COVID-19 infection [2]. Symptoms of LC include fatigue, breathlessness, pain, neurocognitive dysfunction, exercise intolerance, and functional disability [3,4,5,6]. The condition is characterised by clusters of symptoms that change over time, including fluctuations in severity and sudden relapses [1, 7].
Of particular concern is the impact of LC on work status and productivity of patients and, in turn, on the national workforce. The 2022 All-Party Parliamentary Group report on Long COVID, for example, estimated that the 219 NHS trusts in England lost around 1.8 million working days to LC absences between March 2020 and September 2021 [8]. The report goes on to classify LC as an occupational disease and calls for the establishment of a compensation scheme for key frontline workers (e.g. healthcare workers, teachers) who contract the disease [8]. The substantial impact of LC on productivity has likewise been confirmed by numerous UK and non-UK studies of general or general working populations [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28] and specific professions including healthcare workers, teachers, and athletes [29,30,31,32,33]. Productivity in employment not only increases national income, but is also a determinant of health and well-being [34, 35]. Productivity loss due to sickness begets further ill health via mediators including financial instability [36], lack of cognitive stimulation [37], and loss of social identity [38]. Voluntary activities, particularly by retired older persons, likewise contributes to local and wider communities [39]. It is therefore of national and individual interest that LC care strategies place adequate emphasis on vocational rehabilitation to help LC patients return to work or usual activities [40].
Of equal concern is the informal care burden on family members and other caregivers imposed by LC, which has not been a subject of recent research, even as the impact of the COVID-19 pandemic on informal caregivers in general becomes better known [41]. It is important to value the ‘invisible’ contributions of informal caregivers in providing services, which would otherwise result in unmet care needs, incur substantial private care expenditures, and/or place additional strains on the health and social care sectors [42, 43]. A recent study set in Italy, for example, has shown that increased availability of female informal caregivers in a region is negatively associated with the level of public expenditure on long-term care [44]. Productivity losses are incurred when caregivers reduce or give up their employment [42]. Moreover, informal caregivers are often ill-equipped to handle the care burden associated with complex multimorbidity and/or they themselves may be frail and at risk of emotional and physical burnout from caregiving [45, 46]. Overall, there is a strong rationale for the inclusion of productivity and informal caregiver impacts within cost-of-illness studies and economic evaluations to account for the full range of costs incurred by the disease and alleviated by prevention and/or care strategies [42, 47,48,49].
LOng COvid Multidisciplinary consortium Optimising Treatments and servIces acrOss the NHS (LOCOMOTION) is a mixed-methods study that aims to optimise all aspects of LC care in the UK [50]. A core objective of LOCOMOTION is to promote the vocational rehabilitation of LC patients. Accordingly, the economic evaluation planned for the study will adopt a societal perspective to consider how specialist LC clinics impact productivity losses and informal caregiver burden. Such evaluation requires reliable data on the productivity and caregiving impacts of the condition. So would any further evaluations outside of LOCOMOTION that develop decision-analytic models to examine the cost-effectiveness of prevention and care strategies targeting acute and/or Long COVID [51,52,53]. Monetary values concerning the productivity and caregiving impacts, stratified by factors such as age group, sex, and duration of LC, would help parameterise such models [54,55,56]. They also offer a resource for extrapolating from the study sample to the wider LC population. None of the previous studies of LC productivity loss [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33], however, have estimated its monetary value, presenting a gap in the literature. Likewise, none has estimated the economic value of informal caregiving attributable to LC.
Moreover, associations between the type and magnitude of productivity loss and caregiving impact and sociodemographic (e.g. socioeconomic deprivation, ethnicity) and health-related (e.g. duration of LC since the incident infection) factors should clarify where adverse impacts are concentrated and focus policy and care attention accordingly. Likewise, associations between productivity and caregiving impacts and validated patient-reported outcome measures (PROMs) such as the COVID-19 Yorkshire Rehabilitation Scale (C19-YRS), the first validated PROM for LC [3, 57, 58], should facilitate rehabilitation planning for LC patients, clinicians, and employers.
Therefore, this study aims to describe, measure, and value productivity losses and informal care receipt among LC patients referred to specialist LC care clinics as part of LOCOMOTION. The objectives are to: present the productivity and caregiving impacts for a cross-sectional sample of patients and across its subgroups; estimate the monetary value of those impacts; and identify patient characteristics that are associated with those impacts.
Methods
Ethics approval for the LOCOMOTION study was obtained from the Bradford and Leeds Research Ethics Committee on behalf of Health Research Authority and Health and Care Research Wales on 6th January 2022 (reference: 21/YH/0276) [50]. Patients provided informed consent for research participation, patient-reported data collection, data analysis, and research publication through the ELAROS digital system (https://www.elaros.com/) when they enrolled into the study and registered on the system.
Target population and data collection
The target population comprised LC patients newly referred to specialist LC clinics participating in the LOCOMOTION study and subsequently registered on the ELAROS system. The cross-sectional sample drawn for this particular study comprised newly referred patients recruited between 8th August 2022 (when the health economic questionnaire went live on the ELAROS system) and 13th February 2023, a recruitment period of six months. The ELAROS system includes several digital patient-reported outcome measures (DPROMs), administered using the app- and web-based interfaces within ELAROS.
Health economics questionnaire (baseline version)
The health economics questionnaire (HEQ) contained questions on: (i) service(s) received at initial contact with the specialist LC clinic (phone/online consultation, face-to-face doctor consultation, physiotherapy, occupational therapy, speech and language therapy, fatigue management, counselling, peer support network, dietitian, welfare advice, multidisciplinary session, other) and private expenses; (ii) secondary, community health and social service utilisation, medications prescribed, and private care expenditures for LC symptoms in the month preceding the survey (henceforth, ‘previous month’); (iii) productivity in the period prior to the incident COVID-19 infection that resulted in LC (henceforth, ‘pre-infection period’) and in the previous month (further described below); and (iv) informal care receipt in the previous month (further described below). The HEQ was co-developed with lead patient advisory group members (RM, CR, Ms Karen Cook) and piloted on further patient advisory group members (N = 8). The time to completion ranged between 15 and 25 min. The full HEQ is available in the Supplementary Material.
Outcomes related to productivity and informal care receipt
Table 1 lists the outcomes related to productivity and informal care receipt analysed in this study, which were generated from the relevant questions included in the HEQ. The HEQ question D1 also provided free-text space for participants to describe any other ways in which LC symptoms had affected their work status. This generated qualitative data on productivity impacts and, where available, helped internally validate the productivity outcomes. Specifically, counterintuitive responses were identified (e.g. participant described having moved from full- to part-time work, but reported higher weekly work hours), which were subsequently counted as missing and dropped from analysis.
Covariates
As noted above, the HEQ contained variables other than the outcomes related to productivity and informal care receipt: e.g. secondary, community health, and social service utilisation. These served as covariates in the multivariate analyses described below. The following variables were likewise collected digitally in ELAROS (using separate questionnaires from the HEQ) and served as further covariates:
EQ-5D-5L
The EQ-5D-5L health-related quality of life measure covers five dimensions, namely mobility, self-care, usual activities, pain and discomfort, and anxiety and depression, each with five levels of severity [59]. These are used to measure the respondent’s health ‘today’, i.e. the day of survey response. No EQ-5D-5L preference-based value set is currently recommended in the UK to convert the EQ-5D-5L dimension responses into health utility scores. The dimension responses were therefore converted into EQ-5D-3L (an earlier version of the EQ-5D with three response levels for each of the five dimensions) utility scores using an established algorithm [60]. The utility scores are anchored on a scale where 0 = dead and 1 = full health or no problem on all dimensions; utility scores below 0 are available to describe health states deemed worse than death. The EQ-5D-5L health status descriptive system is supplemented by the EQ-VAS, which measures the respondent’s self-rated health on a vertical visual analogue scale (range 0–100) [59].
COVID-19 Yorkshire Rehabilitation Scale (C19-YRS/m)
The C19-YRS is the first validated PROM in the literature for LC symptom type and severity [57]. Its 22 items produce four subscale scores: (i) symptom severity (range 0–100, higher score more severe); (ii) functional disability (0–50, higher score more disabled); (iii) overall health (0–10, higher score better health); and (iv) other symptoms (0–60, higher score more severe). The modified version (C19-YRSm) [3] has 17 items and a 4-point (rather than 11-point) response category for the items related to symptom severity and functional disability. It has the same four subscales as the original version but score ranges of 0–30, 0–15, 0–10, and 0–25, respectively. For subscales (i)–(iii) in both versions, participants were asked to describe their state ‘now’ and their state in the pre-infection period by recall. This enabled the measurement of changes to these subscale scores from the pre-infection period to the survey date.
For multivariate analyses (see below), a binary variable was created for each subscale to indicate participants who were in the highest quartile for the score change (score level for (iv)). The variables thus indicated quartiles who experienced the highest increases in symptom severity, the highest increases in functional disability, the best improvements in overall health (or the least decline in it), and the highest levels of other symptoms, respectively.
Sociodemographic and COVID-19 history variables
Participants reported their sociodemographic characteristics and COVID-19 history, including: age (integer in years), sex (male, female), ethnicity (White, Asian, Black, mixed, or other), region (Birmingham, Cardiff, Hertfordshire, Leeds, Leicester, London, Newcastle, Oxford, or Salford), postcode from which area-based index of multiple deprivation (IMD) decile was derived [61], occupation (free-text response, subsequently categorised by the 2007 UK Standard Industry Classification (SIC) codes [62]), date(s) of COVID-19 infection(s), whether a given infection led to LC (i.e. the incident infection, from the date of which the duration of LC was derived), positive COVID-19 test history, history of hospitalisation(s) due to acute COVID-19, history of intensive care unit (ICU) admission(s) due to acute COVID-19, and COVID-19 vaccination receipt(s) and their date(s) and brand(s).
Analytic methods
Descriptive statistics for each outcome were estimated. Monetary values of productivity losses and informal care receipt were then estimated. For productivity losses, the human capital approach was used for valuation wherein each paid work hour loss was valued at the hourly wage [47]. For participants that reported their monthly work income and weekly paid work hours in the pre-infection period, this information was used to estimate their pre-infection hourly wage, assuming constant weekly work hours and four working weeks over the income-earning month. For those not reporting their pre-infection monthly income, this was predicted using linear regression adjusted for age, sex, IMD quintile, industry code, and region, with coefficients bootstrapped over 1,000 replications. To estimate the aggregate loss over the whole duration of LC, it was assumed that the weekly loss remained constant from the date of incident infection to the survey date. The mean aggregate losses bootstrapped over 1,000 replications were then reported by subgroups of sex, age group, ethnicity, IMD quintile, duration of LC, and industry group – (i) health and education, (ii) financial, information and communication technology (ICT), and professional, and (iii) other – alongside their respective bootstrapped standard error (SE) and 95% confidence interval (CI). Separate mean values were calculated across the subset who had been engaged in paid work in the pre-infection period and across the whole sample. The bootstrapped mean monthly losses were likewise reported.
For informal care, each hour of informal caregiving was valued using the proxy goods method [42]: i.e. it was assumed that in the absence of informal care, individuals would purchase private care as a substitute at the average hourly cost of £20 [63]. Like productivity impacts, the aggregate value of informal care was estimated by assuming the weekly cost remained constant from the date of incident infection. For those who reported receiving any informal care but did not specify the hours of informal care received, the latter was predicted using linear regression adjusted for IMD quintile and EQ-5D-3L utility score (there was no significant association between care hours and other potential covariates such as age, sex, and C19-YRS(m) subscales), with bootstrapped coefficients. The bootstrapped mean aggregate and monthly values were reported by sex, age group, ethnicity, IMD quintile, and duration of LC. Separate mean values were calculated across the subset who received any informal care and across the whole sample.
Economic values of productivity losses and informal care receipt were extrapolated to the national level in the UK using the LC prevalence data provided by the Office for National Statistics (ONS) [2]. Specifically, as of 5th March 2023, 381,000 individuals in the UK self-reported having LC symptoms that impacted their daily activities ‘a lot’. It was assumed that the study sample of LC patients referred to LC specialist clinic is representative of this national sub-population with severe disability due to LC. Of this sub-population, 175,000 individuals reported contracting the incident COVID-19 infection at least 2 years previously, 90,000 between 1 and 2 years previously, 99,000 less than 1 year previously, and 17,000 of unknown LC duration [2]. The bootstrapped mean values (for the whole study sample) by LC duration were applied to these prevalence estimates to estimate the national level impacts; those with unknown LC duration were not included in the extrapolation.
Multilevel logistic regressions, with participants nested by region, were estimated to identify factors significantly associated with the binary outcomes (B) and (G) in Table 1, namely whether the participant returned to pre-infection paid work status/h and whether the participant received any informal care. Multilevel linear regressions were likewise estimated for continuous outcomes (C), (E), and (F) in Table 1, namely change in paid work hours, change in work performance, and change in monthly income, respectively.
All regressions adjusted for duration of LC. In addition, four covariate sets of explanatory variables were used for each regression:
-
(1)
Demographic variables – sex, age group, ethnicity (white vs. minority ethnic), and IMD quintile.
-
(2)
COVID-19-related variables – hospitalisation for acute infection, single- vs. double-vaccinated, secondary and primary/social care use for LC symptoms in the previous month, and number of services receiving at initial LC clinic contact – plus variables in covariate set (1).
-
(3)
PROMs – EQ-5D-3L utility score multiplied by 100 for greater granularity (the coefficient now represents the impact of a score change of magnitude 0.01) and the quartiles of C19-YRS(m) subscale scores defined above – plus variables in covariate set (2).
-
(4)
Variables in covariate set (3) that had P values less than 0.1 for their coefficients being significantly different from zero.
Where the EQ-5D-3L utility score was included as an explanatory variable in covariate set (4), additional regressions were estimated with individual EQ-5D-5L dimension responses as explanatory variables instead of the EQ-5D-3L utility score. It was hypothesised that there are statistically significant and positive associations between higher severity of LC as measured by the PROMs (e.g. lower EQ-5D-3L utility score) and magnitude of the disease impacts on productivity and informal caregiving. All statistical analyses were implemented in STATA version 17 [64].
Results
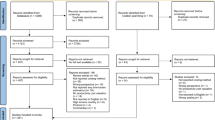
There were 714 new registrations on the ELAROS system from 9th August 2022 to 14th February 2023. Of these, 366 (51.3%) completed the HEQ and constituted the study sample. There was no statistically significant difference between the respondents and non-respondents to the HEQ in terms of mean age, sex, ethnicity (white vs. minority ethnic), IMD quintile, and hospitalisation due to acute COVID-19: see Table A1 in the Supplementary Material. See also “Discussion” for issues around representativeness of the study sample to the general LC patient population (comprising LC patients who are yet to be diagnosed and/or referred to LC specialist clinics) in the UK in terms of its ethnic and socioeconomic mix.
Sample characteristics
Table 2 describes the sample characteristics, delineated by duration of LC in terms of the number of years since the incident COVID-19 infection that resulted in LC. Table A2 in the Supplementary Material reports the EQ-5D-5L dimension responses by duration of LC. Only a minority of the sample (10.9%) reported having been hospitalised for acute COVID-19.
ICT information and communication technology, IMD index of multiple deprivation; LC Long COVID, N/A: not applicable; OT occupational therapy; PT physiotherapy; SD standard deviation; SIC UK Standard Industry Classification code, SLT speech and language therapy
Impact on productivity
Figure 1 displays the proportions of participants by the change in their paid work status/h from the pre-infection period to the previous month. Over half (189 of 366; 51.7%) of the sample had reduced paid work hours or no longer engaged in paid work with or without income. The proportion that returned to pre-infection paid work status/h or increased their paid work hours was 30.0% (110 of 366). Figures A1–A3 in the Supplementary Material display the respective proportions by duration of LC.

Change in paid work status/h from the pre-infection period to the previous month
Data on the change in unpaid work status/h was available from 53 participants. Of these, 13 (24.5%) reduced unpaid work hours, 26 (49.1%) stopped unpaid work, 7 (13.2%) maintained the same hours as the pre-infection period, and another 7 (13.2%) increased their work hours.
Figure 2 shows the average work performance by duration of LC. All subgroups experienced marked worsening in work performance from the pre-infection period to the previous month.

Change in health impact on work performance. LC Long COVID
Figure 3 similarly summarises average monthly work income by duration of LC. In proportional terms, monthly income declined by 24.5% for the whole sample and by 18.5%, 24.1%, and 41.5% for the three respective subgroups defined by duration of LC.

Change in monthly work income, LC Long COVID
Table 3 shows the bootstrapped mean monetary values of the aggregate and monthly productivity losses from paid work hour reduction by sex, age group, ethnicity, IMD quintile, duration of LC, and industry group. Due primarily to their longer disease duration, those with LC duration longer than 2 years incurred the largest aggregate loss relative to those with LC for less than 2 years. Those working in the health and education sectors incurred larger aggregate and monthly losses (£13,864 and £1,000) relative to those working in financial, ICT, and professional services (£10,300 and £792) and in other industries (£9,341 and £761).
Extrapolating from the mean values by LC duration (whole sample), the national aggregate productivity loss due to LC for those whose LC symptoms affected their daily activities ‘a lot’ amounted to £5.7 billion (95% CI: £3.8 to £7.6 billion) and the monthly loss to £277.7 million (95% CI: £196.3 to £359.2 million).
Impact on informal care receipt
Table 4 shows the pattern of informal care support received by participants by duration of LC. Around a third (31.7%) of participants received some informal care. Most (58.8%) of the primary caregivers were partners or spouses of participants. Almost a quarter (22.8%) of caregivers were reported as having reduced paid or unpaid work hours to accommodate their caregiving.
Table 5 shows the bootstrapped mean aggregate and monthly monetary values of informal care receipt by sex, age group, ethnicity, IMD quintile, and duration of LC. Like productivity loss, the aggregate value of informal care received was greater for those who spent more than 2 years with LC relative to those who spent less, owing primarily to their LC duration.
Extrapolating from the mean values by LC duration, the national aggregate informal care value for those whose LC symptoms impacted their daily activities ‘a lot’ amounted to £4.8 billion (95% CI: £2.6 to £7.0 billion) and the monthly value to £218.2 million (95% CI: £122.4 to £314.2 million).
Multivariate analyses
Table 6 shows the results of multilevel logistic regressions on the likelihood of returning to the same or increased paid work hours as the pre-infection period, adjusted for alternative sets of covariates. In covariate set (4), which included covariates with P-values less than 0.10 in set (3), there was a significant positive association between LC duration and return to the same or increased paid work hours. Those who spent 1–2 years with LC had 2.668 times increased odds of returning than those who spent less than one year (P = 0.007). The odds ratio was 2.571 (P = 0.040) for those who spent longer than 2 years. Those who used any community health or social care service in the previous month were less likely to have returned to the same or increased paid work hours (OR 0.477; P = 0.027). A 0.01-unit improvement in the EQ-5D-3L utility score was associated with 1.026 increased odds (P = 0.002). Being in the highest quartile for the increase in C19-YRS(m) functional disability was associated with lower odds (OR 0.236; P = 0.009). The latter two findings support the a priori hypothesis of significant associations between LC severity as measured by the two PROMs and the productivity impact of LC.
Tables A3–A5 in the Supplementary Material show, respectively, the results of multilevel linear regressions on the change in paid work hours relative to the pre-infection period, the change in work performance having returned to paid/unpaid work, and the change in monthly work income, adjusted for each of four alternative sets of covariates. A higher EQ-5D-3L utility score was significantly and positively associated with all three changes as hypothesised, indicating higher positive change (or lesser decline) in the three outcomes. Being in the highest quartile for the improvement (or lesser decline) in C19-YRS(m) overall health was significantly associated with higher work hours and less health issues affecting work performance. By contrast, no C19-YRS(m) subscale was significantly associated with change in monthly income.
Table 7 shows the results of multilevel logistic regressions on the likelihood of receiving any informal care, adjusted as above. Based on covariate set (4), a higher EQ-5D-3L utility score was significantly associated with lower odds of receiving informal care (OR 0.979; P < 0.001), while being in the highest quartile for the increase in C19-YRS(m) symptom severity (OR 2.866; P = 0.001) was significantly associated with increased odds of receiving informal care. Those who spent more than 1 year with LC were less likely to require informal care, but the association was statistically significant only for those who spent 1–2 years with LC (OR 0.438; P = 0.035).
The EQ-5D-3L utility score was included as an explanatory variable in covariate set (4) in each of Tables 6, 7 and A3-A5. Accordingly, Tables A6–A10 in the Supplementary Material show the results of multivariate regressions for the same dependent variables where the EQ-5D-3L utility score has been replaced by individual EQ-5D-5L dimension responses as covariates. The EQ-5D-5L dimensions differed in their associations with the dependent variables. For example, the odds of returning to same or increased paid work hours (Table A6) was significantly and negatively associated with having moderate problems (relative to having no problems) for mobility (OR 0.201; P < 0.001), self-care (OR 0.181; P = 0.012), and usual activities (OR 0.361; P = 0.042), but not for pain/discomfort (OR 0.678; P = 0.396) and anxiety/depression (OR 0.563; P = 0.178).
The multivariate analyses found no evidence of variation in productivity losses and informal care receipt by key sociodemographic variables, including sex, ethnicity, and IMD quintile, though there was some evidence that individuals working in the financial, ICT, and professional sectors were better shielded from paid work hour and monthly work income reductions than those working in the health and education sectors (Tables A3 and A5, respectively, and see “Discussion”).
Discussion
This study estimated and valued productivity losses and informal care receipt within a cross-sectional sample of LC patients referred to specialist LC care clinics in the UK. These economic impacts were found to be substantial, with 23.5% of the sample reducing their paid work status/h, 28.2% no longer engaging in paid work, the average monthly income falling by 24.5%, and 31.7% of the sample requiring informal care. The monetary value of the productivity loss since the incident infection amounted to around £277.7 million per month and £5.7 billion in aggregate amongst those whose LC symptoms impacted their daily activities ‘a lot’, when extrapolated nationally across the UK. The respective estimates for the value of informal care were £218.2 million and £4.8 billion. As hypothesised, the EQ-5D-3L utility score and at least one C19-YRS(m) subscale were shown to be significantly associated with all productivity and informal care outcomes, except for change in monthly income, assessed in multivariate analyses.
The substantial productivity loss associated with LC estimated by this study is broadly consistent with those of previous UK-based studies. Walker and colleagues [10] found that among LC patients referred to LC specialist clinics in the UK (n = 3,754), 50.8% had lost one or more working days in the previous month and 20.3% lost between 20 and 28 working days. Ziauddeen and colleagues [28] found that 19.1% of an online sample of LC patients in the UK (n = 2,550) reported being unable to work and 66.4% taking time off sick. In comparison, 51.7% in this sample had reduced work hours or stopped employment. Reuschke and Houston [11] estimated that around 80,000 persons in the UK whose daily activities had been affected ‘a lot’ by LC had left employment by March 2022. Extrapolating nationally using the same ONS data source [2] as Reuschke and Houston, this study estimates that 102,648 LC patients of similar disease severity had left employment by March 2023.
The substantial productivity impact of LC is clear when the labour market activity of LC patients is compared to that of the general UK population. According to the UK Department for Work & Pensions [65], the proportion economically inactive or unemployed in 2022 was 14.5% for those aged 35–49 years (9.4% for men, 19.4% for women) and 30.0% for those aged 50–64 years (26.0%, 33.9%). The corresponding proportions in our study sample were 36.8% for those aged 35–49 years (38.7%, 36.3%) and 43.2% for those aged 50–64 years (31.7%, 51.1%). Proportionally, therefore, the productivity impact has been most acute for male LC patients aged 35–49 years whose rate of economic inactivity or unemployment is 411.7% of that of their UK general population peers [65]. It should be noted that the highest rate of LC incidence in the UK has been found among the older working age population aged 45–69 years [66]. This study hence finds that the younger working age population has been disproportionately affected in terms of labour market participation.
The high volume of non-UK (mainly European) research on the productivity impacts of LC [9, 12,13,14,15,16,17,18,19,20, 22,23,24,25,26] allows international comparison of the impacts, though a comprehensive synthesis is beyond the scope of this paper. A multinational cohort study of 3,762 LC patients found that 45.2% of patients had reduced work hours and 22.3% no longer engaged in paid work [9]. In comparison, the current study sample comprised a higher proportion (28.2%) of those dropping out of the labour market but a much lower proportion (23.5%) returning to work at reduced schedules. A Swiss study of a sample containing 120 LC patients found 1.6% dropping out of employment and 5.8% having work ability being affected by LC [12]. Relative to the UK studies, this represents a much lower proportion of LC patients whose productivity has been adversely affected. The difference could primarily be attributed to the lower disease severity in the Swiss sample with only 6.7% of the patients having severe health impairment [12]. It is nevertheless feasible that between-country variation in occupational support structures have played a role [67]. A mixed-methods study in the UK, for example, identified key enablers to work return such as line management competency [21], and further research is warranted on whether and to what extent such environmental factors explain the between-country and between-sector differences in productivity outcomes.
Further comparisons can be made to other serious chronic diseases. The UK employment rates for patients with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) [68], multiple sclerosis [68], and non-metastatic breast cancer [69] have been estimated to be 35%, 60%, and 50.9% (women only), respectively. The rate for the current sample was 53.5% (52.8% women only), suggesting that the employment loss from LC is similar to those from multiple sclerosis and non-metastatic breast cancer, though less severe than that from ME/CFS. That said, the higher prevalence of LC relative to ME/CFS means that the total productivity loss from LC is likely much greater. A previous study estimated the annual UK-wide productivity cost due to discontinued employment after ME/CFS onset to be £102.2 million in 2009 prices (£143.6 million in 2022 prices) [70]. This compares to the annual national cost of £3.3 billion (95% CI £2.4 to £4.3 billion) when the current sample’s monthly estimate is extrapolated, although this figure includes the value of all paid work hour reductions, not only of discontinued employment. The annual cost of productivity loss from incident cases of early breast cancer has been estimated at £141.4 million (£168.5 million in 2022 prices) [71]. Overall, the productivity impact of LC can be seen to be as significant as those of other major chronic diseases.
As hypothesised, the multivariate analyses found significant associations between the EQ-5D-3L utility score derived from EQ-5D-5L dimension responses and all productivity-related dependent variables and receipt of any informal care. By contrast, not all EQ-5D-5L dimension responses were significantly associated with the dependent variables, and it may be feasible to infer from the significant associations which of the dimensions are most strongly related with vocational difficulties and care needs. Mobility, for instance, was significantly associated with all dependent variables, and this may motivate increased focus on mobility rehabilitation. Another key finding was the consistent association between one or more C19-YRS(m) subscale score and dependent variables after adjusting for the EQ-5D-3L utility score. The C19-YRS(m) symptom severity subscale, for example, was independently associated with receipt of any informal care. This suggests that better care strategies and professional support tailored to LC-specific symptoms may significantly alleviate the informal caregiver burden. It also suggests that the generic EQ-5D-5L and disease-specific C19-YRS(m) outcome measures should be used in tandem in clinical practice and research.
There was some evidence from the multivariate analyses that the longer the time since the incident infection, the higher the likelihood of returning to the pre-infection work status/h and the lower the likelihood of receiving any informal care, after adjusting for one’s health status measured by the EQ-5D-3L utility score, community health or social care service use in the previous month, and C19-YRS(m) symptom severity or functional disability. However, given that those with LC duration longer than 2 years (the ‘long-haulers’) have significantly worse health status than those with shorter durations as measured by EQ-5D-3L utility score (difference of -0.115 compared to those with LC duration less than 2 years; t test P value of 0.0078), the finding suggests that the long-haulers are returning to work and/or managing without care support despite their worse health status. Financial pressure could be a reason for the work return, as could a desire to limit the care burden on families. More detailed research on this subset of LC long haulers is warranted, particularly regarding their employment, financial, and care support situations.
The substantial magnitude of productivity loss and informal caregiver burden in this patient sample strongly suggest that economic evaluations of LC intervention strategies conducted from a societal perspective should include these outcomes. Such an approach has been previously recommended for ME/CFS, a disease which in some respects may be similar in aetiology and symptoms to LC [72], as well as for a broader family of complex public health interventions [49, 73, 74]. The prevalence data on productivity change and informal care receipt from this study, as well as their final valued outcomes, should serve as important inputs into model-based economic evaluations of LC interventions. Nevertheless, it is likely that equity concerns are particularly relevant for economic evaluations conducted from a societal perspective: the disadvantage of those with the most severe impairments and/or from socially deprived or marginalised backgrounds may be further highlighted when outcomes such as productivity changes are considered in addition to health [75].
Considering such equity concerns, it is noteworthy that the multivariate analyses failed to find any significant evidence of variation in productivity loss and informal care receipt by indicators of social vulnerability, including ethnicity (white vs. minority ethnic) and IMD quintile. A likely issue is the unrepresentativeness of the study sample (comprising LC patients who are diagnosed and referred to LC specialist clinics) to the general LC patient population in the UK in terms of its ethnic and socioeconomic mix. A larger UK study that used primary care records found that Black, mixed ethnicity and other ethnic minority groups comprised around 7.0% of the patients infected with SARS-CoV-2 between January 2020 and April 2021 and had between 6 and 21% increased risks of developing LC [76]. By contrast, these minority ethnic groups comprised just 4.7% of the current study sample, suggesting that the minority ethnic LC patients are underrepresented as was the case in previous UK COVID-19 trials [77]. Analyses of ethnically unrepresentative samples, including multivariate analyses and national extrapolations of productivity and caregiving values, may produce misleading results [78]. There was no statistically significant difference between the respondents and non-respondents to the HEQ in terms of their ethnicity and IMD quintile. This suggests that improved representation of marginalised groups requires broadening the target population to those who are not yet referred to LC specialist clinics and/or have LC symptoms yet no LC diagnosis. Defining diverse ethnic groups, rather than treating them as a homogenous population, would also avoid masking inequities that affect specific groups.
This study has several further limitations. First, it did not use one of established productivity questionnaires such as the Work Productivity and Activity Impairment questionnaire (WPAI), which would have allowed comparisons with economic estimates for other diseases [79,80,81]. That said, the study questionnaire was designed with extensive PPI input from LC patients, including discussions on existing questionnaires such as the WPAI. Second, it was unclear how the survey respondents accounted for inflation in reporting their work incomes in the pre-infection period and previous month. This issue has been encountered in a previous study [68], which noted that if inflation was factored in, the income loss would be even greater in real terms. Third, the study did not explore alternative ways of valuing productivity and informal care [42, 47]. For productivity, an alternative method is friction costing [47], which limits the productivity cost to that related to the time to hire and train a replacement worker. In the absence of accurate estimates of this friction cost, a heuristic method might have been to apply a deflator to the annual income used under the human capital approach [82]. For caregiving, the valuation should ideally account also for the health and wellbeing impact on the caregivers [42]. Finally, the cross-sectional study design meant that the direction of association in the multivariate analyses could not be assessed. The EQ-5D-5L anxiety/depression dimension, for example, was significantly associated with higher reduction in monthly work income (Table A8), but it was unclear whether anxiety impaired income-earning or the lower income resulted in greater anxiety (or both). It was likewise not feasible to estimate any impact that LC specialist services might have had on the various outcomes.
Some caveats to the productivity loss valuation should also be noted. First, the values only incorporate losses from paid work hour reductions. They hence exclude the value of unpaid work hour reduction and of poorer work performance due to LC symptoms (i.e. presenteeism). They also exclude the value of informal caregivers’ work reductions. Second, the change in paid work status/h from the pre-infection period to the month preceding the survey may not strictly be due to LC symptoms; external firm-level and macroeconomic factors (e.g. lower economic activity in lockdowns inducing layoffs) may be at play. Third, it was assumed that the extent of paid work status/h change from the pre-infection period to the previous month was constant to calculate the aggregate loss value. The same assumption was made to calculate the aggregate informal care value. If, however, the paid work status at the survey date represents an improvement relative to earlier stages of LC, then the aggregate value may represent an underestimate, and if a decline an overestimate. Further prospective analyses based on longitudinal cohort studies are warranted to understand the individual trajectories in work status/h and care burden from the incident infection and LC diagnosis. Fourth, the loss values were extrapolated only to those whose LC symptoms limited their daily activities ‘a lot’. In addition to the 381,000 individuals in this group, there were 1,075,000 in the UK who reported LC symptoms limiting their daily activities ‘a little’ (323,000 with LC duration < 1 year, 307,000 1–2 years, and 445,000 > 2 years) [2]. Those with unknown LC duration were also excluded from the extrapolation. Accounting for these groups’ losses would likely enlarge the aggregate burden.
Further research is warranted to analyse the qualitative data obtained from the free-text responses (available from 187 of 366 participants; 51.1%) regarding further personal and environmental factors influencing the productivity of LC patients which are only imperfectly captured by the quantitative data. Box A1 in the Supplementary Material presents a selected sample of quotes organised under the themes ‘Pressure to maintain work performance’, ‘Concern over career prospects’, and ‘Financial pressure even in employment’. Finally, further research can use the full set of information in the HEQ to measure and value the disease impact on health and social care utilisation and patient out-of-pocket expenditures. This will enable a comprehensive evaluation of the economic impact of LC delineated by sectors as done previously for similar diseases [82,83,84].
Conclusion
LC has major impacts on productivity and informal care needs. The high national prevalence of LC likely implies substantial monetary values of over £5.7 billion from productivity losses and £4.8 billion from informal caregiving costs. Patient-reported outcome measures, including outputs from the generic EQ-5D-5L health-related quality of life measure and condition-specific C19-YRS(m) measure, are significantly associated with productivity- and care-related outcomes, such that the measures can be used for rehabilitation planning and evaluation. Our economic values for productivity changes and informal care receipt can inform model-based economic evaluations of LC interventions. The cross-sectional design is a limitation of this study, and a key future research direction is to understand the longitudinal trajectories of productivity patterns and informal care needs of LC patients. This would facilitate causal inferences on how the symptoms of LC affect these outcomes and enable more accurate estimation and extrapolation of their monetary values. Mixed-methods research identifying the environmental determinants of productivity and care needs would help inform the design of vocational rehabilitation and labour regulation suited to LC patients. Further research is also needed with a more representative sample of people with LC, including those not yet referred to LC specialist clinics and those with LC symptoms but no diagnosis, to identify whether inequalities in productivity loss and informal care receipt affect marginalised groups such as deprived and specific minority ethnic populations.
Abbreviations
- C19-YRS:
-
COVID-19 Yorkshire Rehabilitation Scale
- C19-YRSm:
-
COVID-19 Yorkshire Rehabilitation Scale modified
- CI:
-
Confidence interval
- DPROM:
-
Digital patient-reported outcome measure
- HEQ:
-
Health economics questionnaire
- ICT:
-
Information and communication technology
- ICU:
-
Intensive care unit
- IMD:
-
Index of multiple deprivation
- LC:
-
Long COVID
- ONS:
-
Office for National Statistics
- SE:
-
Standard error
- SIC:
-
Standard industry classification
- WPAI:
-
Work Productivity and Activity Impairment questionnaire
References
National Institute for Health and Care Excellence, Scottish Intercollegiate Guidelines Network, Royal College of General Practitioners. COVID-19 rapid guideline: managing the long-term effects of COVID-19. In: NICE R, and SIGN, editor. 2022.
Office for National Statistics. Prevalence of ongoing symptoms following coronavirus (COVID-19) infection in the UK: 30 March 2023. 2023.
Sivan, M., Preston, N., Parkin, A., Makower, S., Gee, J., Ross, D., et al.: The modified COVID-19 Yorkshire rehabilitation scale (C19-YRSm) patient-reported outcome measure for long covid or post-COVID-19 syndrome. J. Med. Virol. 94(9), 4253–4264 (2022)
Pierce, J.D., Shen, Q., Cintron, S.A., Hiebert, J.B.: Post-COVID-19 syndrome. Nurs. Res. 71(2), 164–174 (2022)
Michelen, M., Manoharan, L., Elkheir, N., Cheng, V., Dagens, A., Hastie, C., et al.: Characterising long COVID: a living systematic review. BMJ Glob. Health 6(9), e005427 (2021)
Ayoubkhani D, Bermingham C, Pouwels KB, Glickman M, Nafilyan V, Zaccardi F, et al. Trajectory of long covid symptoms after covid-19 vaccination: community based cohort study. Bmj. 2022; 377.
Brown, D.A., O’Brien, K.K.: Conceptualising long COVID as an episodic health condition. BMJ Glob. Health 6(9), e007004 (2021)
All-Party Parliamentary Group. Long COVID Report March 2022. In: Group A-PP, editor. 2022.
Davis, H.E., Assaf, G.S., McCorkell, L., Wei, H., Low, R.J., Re’em, Y., et al.: Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine. 38, 101019 (2021)
Walker, S., Goodfellow, H., Pookarnjanamorakot, P., Murray, E., Bindman, J., Blandford, A., et al.: Impact of fatigue as the primary determinant of functional limitations among patients with post-COVID-19 syndrome: a cross-sectional observational study. BMJ Open 13(6), e069217 (2023)
Reuschke D, Houston D. The impact of Long COVID on the UK workforce. Applied Economics Letters. 2022:1–5.
Kerksieck P, Ballouz T, Haile SR, Schumacher C, Lacy J, Domenghino A, et al. Post COVID-19 condition, work ability and occupational changes in a population-based cohort. The Lancet Regional Health–Europe. 2023.
Delgado-Alonso, C., Cuevas, C., Oliver-Mas, S., Díez-Cirarda, M., Delgado-Álvarez, A., Gil-Moreno, M.J., et al.: Fatigue and cognitive dysfunction are associated with occupational status in post-COVID syndrome. Int. J. Environ. Res. Public Health 19(20), 13368 (2022)
Magnavita, N., Arnesano, G., Di Prinzio, R.R., Gasbarri, M., Meraglia, I., Merella, M., et al.: Post-COVID symptoms in occupational cohorts: effects on health and work ability. Int. J. Environ. Res. Public Health 20(9), 5638 (2023)
Vaes AW, Goërtz YM, Van Herck M, Machado FV, Meys R, Delbressine JM, et al. Recovery from COVID-19: a sprint or marathon? 6-month follow-up data from online long COVID-19 support group members. ERJ open research. 2021;7 (2).
Westerlind, E., Palstam, A., Sunnerhagen, K.S., Persson, H.C.: Patterns and predictors of sick leave after COVID-19 and long COVID in a national Swedish cohort. BMC Public Health 21(1), 1–9 (2021)
Buonsenso, D., Gualano, M.R., Rossi, M.F., Valz Gris, A., Sisti, L.G., Borrelli, I., et al.: Post-acute COVID-19 sequelae in a working population at one year follow-Up: a wide range of impacts from an italian sample. Int. J. Environ. Res. Public Health 19(17), 11093 (2022)
Diem, L., Schwarzwald, A., Friedli, C., Hammer, H., Gomes-Fregolente, L., Warncke, J., et al.: Multidimensional phenotyping of the post-COVID-19 syndrome: a swiss survey study. CNS Neurosci. Ther. 28(12), 1953–1963 (2022)
Dryden, M., Mudara, C., Vika, C., Blumberg, L., Mayet, N., Cohen, C., et al.: Post-COVID-19 condition 3 months after hospitalisation with SARS-CoV-2 in South Africa: a prospective cohort study. Lancet Glob. Health 10(9), e1247–e1256 (2022)
Kisiel MA, Janols H, Nordqvist T, Bergquist J, Hagfeldt S, Malinovschi A, et al. Predictors of post-COVID-19 and the impact of persistent symptoms in non-hospitalized patients 12 months after COVID-19, with a focus on work ability. Upsala Journal of Medical Sciences. 2022; 127.
Lunt J, Hemming S, Burton K, Elander J, Baraniak A. What workers can tell us about post-COVID workability. Occupational Medicine (Oxford, England). 2022.
Mazer B, Feldman DE. Functional limitations in individuals with long COVID. Archives of Physical Medicine and Rehabilitation. 2023.
Miskowiak, K., Pedersen, J., Gunnarsson, D., Roikjer, T., Podlekareva, D., Hansen, H., et al.: Cognitive impairments among patients in a long-COVID clinic: Prevalence, pattern and relation to illness severity, work function and quality of life. J. Affect. Disord. 324, 162–169 (2023)
Perlis RH, Trujillo KL, Safarpour A, Santillana M, Ognyanova K, Druckman J, et al. Association of post–COVID-19 condition symptoms and employment status. JAMA network open 2023; 6 (2): e2256152-e.
Sansone, D., Tassinari, A., Valentinotti, R., Kontogiannis, D., Ronchese, F., Centonze, S., et al.: Persistence of symptoms 15 months since COVID-19 diagnosis: prevalence, risk factors and residual work ability. Life. 13(1), 97 (2022)
Yelin, D., Margalit, I., Nehme, M., Bordas-Martínez, J., Pistelli, F., Yahav, D., et al.: Patterns of long COVID symptoms: a multi-center cross sectional study. J. Clin. Med. 11(4), 898 (2022)
Van Wambeke, E., Bezler, C., Kasprowicz, A.-M., Charles, A.-L., Andres, E., Geny, B.: Two-years follow-up of symptoms and return to work in complex post-COVID-19 patients. J. Clin. Med. 12(3), 741 (2023)
Ziauddeen, N., Gurdasani, D., O’Hara, M.E., Hastie, C., Roderick, P., Yao, G., et al.: Characteristics and impact of long covid: findings from an online survey. PLoS ONE 17(3), e0264331 (2022)
Fischer, K., Reade, J.J., Schmal, W.B.: What cannot be cured must be endured: the long-lasting effect of a COVID-19 infection on workplace productivity. Labour Econ. 79, 102281 (2022)
Fouad MM, Zawilla NH, Maged LA. Work performance among healthcare workers with post COVID-19 syndrome and its relation to antibody response. Infection. 2022: 1–11.
Nehme, M., Vieux, L., Kaiser, L., Chappuis, F., Chenaud, C., Guessous, I.: The longitudinal study of subjective wellbeing and absenteeism of healthcare workers considering post-COVID condition and the COVID-19 pandemic toll. Sci. Rep. 13(1), 10759 (2023)
Levkovich, I., Kalimi, E.: Long COVID-19 symptoms among recovered teachers in israel: a mixed-methods study. COVID. 3(4), 480–493 (2023)
Peters, C., Dulon, M., Westermann, C., Kozak, A., Nienhaus, A.: Long-term effects of COVID-19 on workers in health and social services in Germany. Int. J. Environ. Res. Public Health 19(12), 6983 (2022)
Dahlgren G, Whitehead M. European strategies for tackling social inequities in health: Levelling up Part 2. WHO Regional office for Europe Copenhagen; 2006.
Department of Health. Healthy lives, healthy people: Our strategy for public health in England: The Stationery Office; 2010.
Mureșan, G.-M., Văidean, V.-L., Mare, C., Achim, M.V.: Were we happy and we didn’t know it? a subjective dynamic and financial assessment pre-, during and post-COVID-19. Eur. J. Health Econ. 24(5), 749–768 (2023)
Rohwedder, S., Willis, R.J.: Mental retirement. J. Econ. Perspect. 24(1), 119–138 (2010)
National Institute for Health and Care Excellence. Older people: independence and mental wellbeing. NICE guideline [NG32] 2015 [updated 17 December 2015]. Available from: https://www.nice.org.uk/guidance/ng32.
Cook J. The socio‐economic contribution of older people in the UK. Working with Older People. 2011.
NHS England. National Commissioning Guidance for Post COVID Services. In: England N, editor. Version 3, July 20222022.
Cohen, S.A., Kunicki, Z.J., Drohan, M.M., Greaney, M.L.: Exploring changes in caregiver burden and caregiving intensity due to COVID-19. Geront Geriatric Med. 7, 2333721421999279 (2021)
Koopmanschap, M.A., van Exel, N.J.A., van den Berg, B., Brouwer, W.B.: An overview of methods and applications to value informal care in economic evaluations of healthcare. Pharmacoeconomics 26(4), 269–280 (2008)
Van Exel, J., Bobinac, A., Koopmanschap, M., Brouwer, W.: The invisible hands made visible: recognizing the value of informal care in healthcare decision-making. Expert Rev. Pharmacoecon. Outcomes Res. 8(6), 557–561 (2008)
Cepparulo, A., Giuriato, L.: The residential healthcare for the elderly in Italy: some considerations for post-COVID-19 policies. Eur. J. Health Econ. 23(4), 671–685 (2022)
Osborn, R., Moulds, D., Squires, D., Doty, M.M., Anderson, C.: International survey of older adults finds shortcomings in access, coordination, and patient-centered care. Health Aff. 33(12), 2247–2255 (2014)
Mello, Jd.A., Macq, J., Van Durme, T., Cès, S., Spruytte, N., Van Audenhove, C., et al.: The determinants of informal caregivers’ burden in the care of frail older persons: a dynamic and role-related perspective. Aging Mental Health. 21(8), 838–843 (2017)
Krol, M., Brouwer, W.: How to estimate productivity costs in economic evaluations. Pharmacoeconomics 32(4), 335–344 (2014)
Tong T. Broadening the perspective of economic evaluation in health care - A case study in dementia care in the UK: University of Sheffield; 2017.
Squires, H., Chilcott, J., Akehurst, R., Burr, J., Kelly, M.P.: A systematic literature review of the key challenges for developing the structure of public health economic models. Int. J. Public Health 61(3), 289–298 (2016)
Sivan, M., Greenhalgh, T., Darbyshire, J.L., Mir, G., O’Connor, R.J., Dawes, H., et al.: LOng COvid Multidisciplinary consortium optimising treatments and servIces acrOss the NHS (Locomotion): protocol for a mixed-methods study in the UK. BMJ Open 12(5), e063505 (2022)
European Burden of Disease Network. Burden of disease of COVID-19: Protocol for country studies. In: Technology ECiS, editor. 2020.
Wyper G, Assunção R, Colzani E, Grant I, Haagsma JA, Lagerweij G, et al. Burden of disease methods: a guide to calculate COVID-19 disability-adjusted life years. International Journal of Public Health. 2021:4.
Angeles, M.R., Wanni Arachchige Dona, S., Nguyen, H.D., Le, L.K.-D., Hensher, M.: Modelling the potential acute and post-acute burden of COVID-19 under the Australian border re-opening plan. BMC Public Health 22(1), 1–13 (2022)
Drummond MF, Sculpher MJ, Claxton K, Stoddart GL, Torrance GW. Methods for the economic evaluation of health care programmes: Oxford university press; 2015.
Briggs A, Sculpher M, Claxton K. Decision modelling for health economic evaluation: Oup Oxford; 2006.
Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al. Review of guidelines for good practice in decision-analytic modelling in health technology assessment. 2004.
Sivan, M., Parkin, A., Makower, S., Greenwood, D.C.: Post-COVID syndrome symptoms, functional disability, and clinical severity phenotypes in hospitalized and nonhospitalized individuals: A cross-sectional evaluation from a community COVID rehabilitation service. J. Med. Virol. 94(4), 1419–1427 (2022)
Straudi, S., Manfredini, F., Baroni, A., Milani, G., Fregna, G., Schincaglia, N., et al.: Construct validity and responsiveness of the COVID-19 Yorkshire rehabilitation scale (C19-YRS) in a cohort of Italian hospitalized COVID-19 Patients. Int. J. Environ. Res. Public Health 19(11), 6696 (2022)
Herdman, M., Gudex, C., Lloyd, A., Janssen, M., Kind, P., Parkin, D., et al.: Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 20(10), 1727–1736 (2011)
Hernández Alava M, Pudney S, Wailoo A. Estimating the relationship between EQ-5D-5L and EQ-5D-3L: results from an English Population Study. In: York UoSa, editor. Policy Research Unit in Economic Evaluation of Health and Care Interventions2020.
Ministry of Housing CaLG. English indices of deprivation 2019 2019. Available from: https://imd-by-postcode.opendatacommunities.org/imd/2019.
Office for National Statistics. UK SIC 2007 2022 [updated 24 January 2022]. Available from: https://www.ons.gov.uk/methodology/classificationsandstandards/ukstandardindustrialclassificationofeconomicactivities/uksic2007.
UK Care Guide. How Much Does in Home Care Cost in April 2023 2023 [updated 1 April 2023]. Available from: https://ukcareguide.co.uk/home-care-costs/.
StataCorp. Stata Statistical Software: Release 17. In: College Station TSL, editor. 2019.
Department for Work & Pensions. Economic labour market status of individuals aged 50 and over, trends over time: September 2022 2022 [updated 8 September 2022]. Available from: https://www.gov.uk/government/statistics/economic-labour-market-status-of-individuals-aged-50-and-over-trends-over-time-september-2022/economic-labour-market-status-of-individuals-aged-50-and-over-trends-over-time-september-2022#economic-inactivity.
Thompson, E.J., Williams, D.M., Walker, A.J., Mitchell, R.E., Niedzwiedz, C.L., Yang, T.C., et al.: Long COVID burden and risk factors in 10 UK longitudinal studies and electronic health records. Nat. Commun. 13(1), 3528 (2022)
Babnik, K., Staresinic, C., Lep, Ž: Some of the workforce face post COVID after the acute phase of the illness: the employer’s supportive role. Hum. Syst. Manag. 41(2), 257–275 (2022)
Kingdon, C.C., Bowman, E.W., Curran, H., Nacul, L., Lacerda, E.M.: Functional status and well-being in people with myalgic encephalomyelitis/chronic fatigue syndrome compared with people with multiple sclerosis and healthy controls. PharmacoEconomics-open. 2(4), 381–392 (2018)
Verrill, M., Wardley, A.M., Retzler, J., Smith, A.B., Bottomley, C., Ní Dhochartaigh, S., et al.: Health-related quality of life and work productivity in UK patients with HER2-positive breast cancer: a cross-sectional study evaluating the relationships between disease and treatment stage. Health Qual. Life Outcomes 18, 1–12 (2020)
Collin SM, Crawley E, May MT, Sterne JA, Hollingworth W, Database UCMNO. The impact of CFS/ME on employment and productivity in the UK: a cross-sectional study based on the CFS/ME national outcomes database. BMC health services research. 2011; 11:1–8.
Parsekar, K., Wilsher, S.H., Sweeting, A., Patel, A., Fordham, R.: Societal costs of chemotherapy in the UK: an incidence-based cost-of-illness model for early breast cancer. BMJ Open 11(1), e039412 (2021)
Cochrane, M., Mitchell, E., Hollingworth, W., Crawley, E., Trépel, D.: Cost-effectiveness of interventions for chronic fatigue syndrome or Myalgic encephalomyelitis: a systematic review of economic evaluations. Appl. Health Econ. Health Policy 19, 473–486 (2021)
Weatherly, H., Drummond, M., Claxton, K., Cookson, R., Ferguson, B., Godfrey, C., et al.: Methods for assessing the cost-effectiveness of public health interventions: key challenges and recommendations. Health Policy 93(2–3), 85–92 (2009)
Kelly, M.P., McDaid, D., Ludbrook, A., Powell, J.: Economic appraisal of public health interventions. Health Development Agency, London (2005)
Norheim, O.F., Baltussen, R., Johri, M., Chisholm, D., Nord, E., Brock, D., et al.: Guidance on priority setting in health care (GPS-Health): the inclusion of equity criteria not captured by cost-effectiveness analysis. Cost Effect Resource Allocation. 12(1), 18 (2014)
Subramanian, A., Nirantharakumar, K., Hughes, S., Myles, P., Williams, T., Gokhale, K.M., et al.: Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 28(8), 1706–1714 (2022)
Murali, M., Gumber, L., Jethwa, H., Ganesh, D., Hartmann-Boyce, J., Sood, H., et al.: Ethnic minority representation in UK COVID-19 trials: systematic review and meta-analysis. BMC Med. 21(1), 1–18 (2023)
Mir, G., Salway, S., Kai, J., Karlsen, S., Bhopal, R., Ellison, G.T., et al.: Principles for research on ethnicity and health: the Leeds Consensus Statement. European J Public Health. 23(3), 504–510 (2013)
Beck, A., Crain, A.L., Solberg, L.I., Unützer, J., Glasgow, R.E., Maciosek, M.V., et al.: Severity of depression and magnitude of productivity loss. Annals Family Med 9(4), 305–311 (2011)
Chen, J., Taylor, B., Palmer, A.J., Kirk-Brown, A., van Dijk, P., Simpson, S., Jr., et al.: Estimating MS-related work productivity loss and factors associated with work productivity loss in a representative Australian sample of people with multiple sclerosis. Mult. Scler. J. 25(7), 994–1004 (2019)
Algamdi, M., Sadatsafavi, M., Fisher, J.H., Morisset, J., Johannson, K.A., Fell, C.D., et al.: Costs of workplace productivity loss in patients with fibrotic interstitial lung disease. Chest 156(5), 887–895 (2019)
Sabes-Figuera, R., McCrone, P., Hurley, M., King, M., Donaldson, A.N., Ridsdale, L.: The hidden cost of chronic fatigue to patients and their families. BMC Health Serv. Res. 10(1), 1–7 (2010)
Lin, J.M.S., Resch, S.C., Brimmer, D.J., Johnson, A., Kennedy, S., Burstein, N., et al.: The economic impact of chronic fatigue syndrome in Georgia: direct and indirect costs. Cost Effectiveness Resou Allocation 9(1), 1–12 (2011)
Close S, Marshall-Gradisnik S, Byrnes J, Smith P, Nghiem S, Staines D. The economic impacts of myalgic encephalomyelitis/chronic fatigue syndrome in an Australian cohort. Frontiers in Public Health. 2020: 420.
Funding
This work is independent research funded by the National Institute for Health and Care Research (NIHR) (Long COVID grant, Ref: COV-LT2-0016). The views expressed in this publication are those of the author(s) and not necessarily those of NIHR or the Department of Health and Social Care.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing financial and non-financial interests to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kwon, J., Milne, R., Rayner, C. et al. Impact of Long COVID on productivity and informal caregiving. Eur J Health Econ 25, 1095–1115 (2024). https://doi.org/10.1007/s10198-023-01653-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10198-023-01653-z