
Abstract
Inhalation of hyperbaric oxygen has been used as an experimental treatment for migraine and pure oxygen is an established treatment for cluster headache. Intravenous glyceryl trinitrate (GTN) is an established headache model. In the present study the possibility of decreasing the headache by inhalation of pure oxygen was explored in a double-blind crossover design in 18 healthy subjects. Inhalation of air served as placebo. The subjects received intravenous GTN (0.25 µg/kg/min) for 20 min. Headache was scored for 85 min. Sixteen of 18 (89%) subjects experienced GTN-induced headache after O2-inhalation and 17/18 (94%) experienced GTN-induced headache after air. The mean peak headache scores were 1.9 and 2.4, respectively, on a numerical scale of 0–10. Oxygen inhalation did not have effect on GTN-induced headache, most likely because the theoretical decrease in NO levels, due to faster metabolism of NO, is too small to be detected in the GTN headache model.
Similar content being viewed by others

Introduction
The intravenous glyceryl trinitate (GTN) headache model is well established [1, 2]. It causes a short-lasting headache in healthy volunteers and in migraine and cluster headache patients, the so-called immediate GTN headache [1, 2]. In addition, GTN causes a delayed headache in cluster headache [3] and migraine patients [4]. The immediate GTN headache is most likely due to a vasodilator effect of GTN on the extracerebral circulation [5] whereas the delayed headache/migraine is elicited by other mechanisms.
Administration of N-acetylcysteine, a sulfhydryl group donor, enhanced the headache-inducing effect of a GTN infusion in healthy volunteers [6]. This effect of N-acetylcysteine is most likely due to enhanced formation of NO from GTN.
In a recent Cochrane review [7] it was concluded that there was some evidence that hyperbaric oxygen was effective for the termination of acute migraine, and weak evidence that normobaric oxygen was similarly effective in cluster headache.
In the present study we tried to decrease the levels of NO in our GTN headache model by administering pure oxygen in a dose, 7 l/min which has been shown to be effective in the treatment of cluster headache in a double-blind trial [8, 9] and in clinical practice [8, 10]. Increased oxygen concentration most likely decreases NO concentration by oxidization of NO to NO3 and NO2.
Healthy volunteers were investigated in a crossover design.
Methods
Subjects
The study followed a randomized, double-blind, placebo-controlled, and cross-over design. The 2 study days were scheduled at least 7 days apart and included 18 healthy volunteers who had no prior history of migraine and who did not experience tension-type headache more than once a month. Their median age was 23 years (range 20–33 years), the male:female ratio was 1:1, and the median body weight 65 kg (range 52–86 kg). Prior to entry the subjects were challenged with 0.25 mg of GTN sublingually and were included only if they experienced headache. The participants gave informed consent prior to inclusion, and it was emphasized that they were free to withdraw at any time. The study was approved by The Ethics Committee of Copenhagen County.
Procedure
No caffeine containing beverages, alcohol, tobacco, or medication were allowed for the preceding 12 h prior to the study, and all had to be headache-free at start. After 30 min of rest, either pure oxygen or placebo (atmospheric air), 7 l/min, was inhaled for 35 min through a line fastened to an inflatable anesthesia mask. The gas bottles were hidden to the investigator and the participants. The proper gas was connected to the mask by a laboratory technician. GTN, 0.25 µg/kg/min, was infused for 20 min through a i.v. line in the right cubital vein using a volume-directed infusion pump (Braun Perfusor, Secura). Headache was rated on a verbal 0–10 numerical scale; 1 representing pre-pain, 5 a moderate headache, and 10 the worst possible headache. At pain scores above 0 the headache and accompanying symptoms were characterized according to a standardized questionnaire covering the IHS criteria for migraine without aura (IHS-classification, 12). The study ended 85 min after the start of the oxygen/placebo inhalation.
Statistics
Statistical analyses were performed with Statgraphic 7.0. Randomization and Wilcoxon–Pratt statistics were performed using Medstat, p < 0.05 was chosen as the statistical level of significance. Differences in the total, summed, and peak headache scores between the two study days were analyzed using Wilcoxon–Pratt’s test.
Results
All subjects completed the study. No serious adverse events were seen during or after the infusion of GTN.
Sixteen of 18 (89%) subjects experienced headache after the O2 inhalation and 17/18 (94%) on the day with air. The mean peak headache score in was 1.9 (O2) and 2.4 (air).
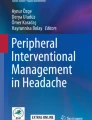
Oxygen did not significantly alter the summed headache scores or the peak headache scores (Wilcoxon–Pratt; summed p = 0.11, peak p = 0.25; Fig. 1).

Individual headache scores in the laboratory, 0–85 min after glyceryl trinitrate (with means in bold), n = 18. There was no difference between oxygen and air inhalation1
The headache showed similar characteristics in the majority of the subjects. It was mild, bilateral, pressing, mainly fronto-temporal headache of short duration without accompanying symptoms. No subject fulfilled the diagnostic criteria for migraine without aura [11].
Discussion
The rationale for this study was the fact that increased oxygen tension will tend to increase the metabolism of NO. In an aqueous solution NO reacts rapidly and spontaneously with oxygen to produce mainly nitrite via the intermediary formation of nitrogen dioxide and dinitrogen trioxide [12].
A reduction in pO2 causes an increase in NO in some [13, 14] but not all [15, 16] studies. Theoretically, hypoxia could cause an increase in the effect of glyceryl trinitrate (GTN). This effect cannot be explored experimentally in humans outside a hypobaric chamber. In contrast, an increase in pO2 causes a shortening of the half-life of NO [17] due to increased metabolism and most likely a decrease in the effect of GTN. This possible effect of pure oxygen was explored in the present study.
The major result of the present study was that a therapeutic dose of oxygen inhalation (7 l/min) [8], did not reduce the headache induced by GTN infusion (0.25 µg/kg/min) in healthy volunteers.
Theoretically, this “negative” result could be due either to the fact that the GTN headache model is not sensitive enough to detect changes in NO levels or to a lack of oxygen to counteract the effect of GTN/NO.
That the GTN model is sensitive to changes in NO is demonstrated by the fact that a dose–response curve for the headache effect of GTN could be constructed [2] and by the fact that the sulfhydryl donor, N-acetylcysteine, increased the NTG-induced headache [6].
The dose of oxygen by inhalation was 7 l/min [8] but there was no effect on NTG-induced headache, most likely because the obtained increase of pO2 was not large enough to counteract the effect of GTN. Thus, in isolated guinea pig hearts increasing oxygen tension in aqueous solutions from 150 to 700 mmHg decreased NO half-life (5.2 s) by 32% [17]. Hundred percent oxygen inhalation in normal adults increases pO2 to about 600 mmHg [18]. Based on the in vitro in guinea pig study [17] this pO2 (600 mmHg) in humans may result in too small a decrease in NO levels to be detected in our headache model.
Our results suggest that the effect of pure oxygen in cluster headache may not be mediated via a reduction of NO.
References
Kruuse C, Afridi SK (2006) Human models of the headaches. In: Olesen J, Goadsby PJ, Ramadan NM, Tfelt-Hansen P, Welch KMA (eds) The headaches, 3rd edn. Lippincott Williams & Wilkins, Philadelphia, pp 221–229
Iversen HK, Olesen J, Tfelt-Hansen P (1989) Intravenous nitroglycerin as an experimental model of vascular headache. Basic characteristics. Pain 38:17–24 10.1016/0304-3959(89)90067-5, 1:CAS:528:DyaL1MXltlWru7o%3D, 2506503
Ekbom K (1968) Nitroglycerin as a provocative agent in cluster headache. Arch Neurol 19:487–493 1:STN:280:DyaF1M%2FhtlCnsQ%3D%3D, 4971733
Thomsen LL, Kruuse C, Iversen HK, Olesen J (1994) A nitric oxide donor (nitroglycerin) triggers genuine migraine attacks. Eur J Neurol 1:73–80
Christiansen I, Iversen HK, Olesen J, Tfelt-Hansen P (2008) Nitric oxide-induced headache may arise from extracerebral arteries as judged from tolerance to isosorbide 5-mononitrate. J Headache Pain 9:215–220 10.1007/s10194-008-0043-9, 1:CAS:528:DC%2BD1cXpsVGjsrY%3D, 18521538
Iversen HK (1992) N-acetylcysteine enhances nitroglycerin-induced headache and cranial arterial responses. Clin Pharmacol Ther 52:125–133 1:CAS:528:DyaK38Xls1yru7g%3D, 1505148
Bennett MH, French C, Schnabel A, Wasiak J, Kranke P (2008) Normobaric and hyperbaric oxygen therapy for migraine and cluster headache. Cochrane Database Syst Rev 3:CD005219 18646121
Sandrini G, Ward TN (2006) Acute treatment of cluster headache. In: Olesen J, Goadsby PJ, Ramadan NM, Tfelt-Hansen P, Welch KMA (eds) The headaches, 3rd edn. Lippincott Williams & Wilkins, Philadelphia, pp 803–807
Fogan L (1985) Treatment of cluster headache. A double-blind comparison of oxygen v air inhalation. Arch Neurol 42:362–363 1:STN:280:DyaL2M7ntl2itA%3D%3D, 3885921
Kudrow L (1981) Response of cluster headache attacks to oxygen inhalation. Headache 21:1–4 10.1111/j.1526-4610.1981.hed2101001.x, 1:STN:280:DyaL3M7hs1KitA%3D%3D, 7007285
Headache Classification Committee of the International Headache Society (2004) Classification and diagnostic criteria for headache disorders, cranial neuralgia and facial pain, 2nd edn. Cephalalgia 24(Suppl 1):1–164
Purwanti E, Mukhopadhyay B (2009) Conversion of NO2 to NO by reduced coenzyme F420 protects mycobacteria from nitrosactive damage. PNAS 106:6333–6338 10.1073/pnas.0812883106
Hampl V, Cornfield DN, Cowan NJ, Archer SL (1995) Hypoxia potentiates nitric oxide synthesis and transiently increases cytosolic calcium levels in pulmonary artery endothelial cells. Eur Respir J 8:515–522 1:CAS:528:DyaK2MXmslSnsbk%3D, 7664847
Xu XP, Pollock JS, Tanner MA, Myers PR (1995) Hypoxia activates nitric oxide synthase and stimulates nitric oxide production in porcine coronary resistance arteriolar endothelial cells. Cardiovasc Res 30:841–847 1:CAS:528:DyaK28Xht1CgsLc%3D, 8746197
Shaul PW, Wells LB, Horning KM (1993) Acute and prolonged hypoxia attenuate endothelial nitric oxide production in rat pulmonary arteries by different mechanisms. J Cardiovascul Pharmacol 22:819–827 1:CAS:528:DyaK2cXnsVGhug%3D%3D, 10.1097/00005344-199312000-00007
Whorton AR, Simonds DB, Piantadosi CA (1997) Regulation of nitric oxide synthesis by oxygen in vascular endothelial cells. Am J Physiol 272:L1161–L1166 1:CAS:528:DyaK2sXktlKnsLY%3D, 9227518
Kelm M, Schrader J (1990) Control of coronary vascular tone by nitric oxide. Circ Res 66:1561–1575 1:CAS:528:DyaK3cXktlyisb4%3D, 2160870
Koeff ST, Tsao MU, Vadnay A, Wilson TO, Wilson JL (1962) Continuous measurements of intravascular oxygen tension in normal adults. J Clin Invest 41:1125–1133 10.1172/JCI104564, 1:CAS:528:DyaF38XksFylt7o%3D, 14457653
Acknowledgments
The study was supported by The Migraine Trust, UK, by the Danish Headache Society, and by the Lundbeck Foundation via the Lundbeck Foundation Center for Neurovascular Signaling (LUCENS), Denmark. Statistical advice was provided by statistician Lene Theil Skovgaard, Department of Biostatistics, University of Copenhagen, Denmark. We are grateful for the assistance of laboratory technicians Bente Leisner and Kirsten Enghave.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Daugaard, D., Tfelt-Hansen, P., Thomsen, L.L. et al. No effect of pure oxygen inhalation on headache induced by glyceryl trinitrate. J Headache Pain 11, 93–95 (2010). https://doi.org/10.1007/s10194-010-0190-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10194-010-0190-7