
Abstract
The aim of this study was to investigate the association between caffeine consumption and headache type and frequency in the general adult population. The results were based on cross-sectional data from 50,483 (55%) out of 92,566 invited inhabitants aged ≥20 years who participated in the Nord-Trøndelag Health Survey. In the multivariate analyses, adjusting for age, gender, smoking, and level of education as confounding factors, a weak but significant association (OR = 1.16, 95% CI 1.09–1.23) was found between high caffeine consumption and prevalence of infrequent headache. In contrast, headache >14 days/month was less likely among individuals with high caffeine consumption compared to those with low caffeine consumption. The results may indicate that high caffeine consumption changes chronic headache into infrequent headache due to the analgesic properties of caffeine. Alternatively, chronic headache sufferers tend to avoid intake of caffeine to not aggravate their headaches, whereas individuals with infrequent headache are less aware that high caffeine use can be a cause.
Similar content being viewed by others


Introduction
Caffeine is probably the most commonly consumed stimulant worldwide, generating increased wellbeing, happiness, energy, alertness, and sociability [1]. Caffeine also has acute analgesic properties and promotes headache relief [2]. On the other hand, among habitual caffeine users, abrupt cessation may results in time-limited withdrawal symptoms such as headache [1]. In a placebo-controlled double-blind study, as many as 52% of the participants had a moderate or severe headache within the first 2 days of cessation of coffee intake, whereas only 6% had similar headache among those who continued the coffee intake [3]. However, more recently, a controlled, blinded study reported a lower prevalence (33%) of caffeine-withdrawal headache [4].
Conflicting results have also been found in population-based studies evaluating the association between caffeine and headache. Some studies have reported a positive relationship between high caffeine consumption and prevalence of headache [5], migraine [6], and chronic migraine [7]. Furthermore, high caffeine consumption has been found to be a modest risk factor for onset of chronic daily headache [8].
In contrast, no clear relationship has been found between current caffeine consumption and headache [9] or chronic headache [8, 10]. The prevalence of caffeine-withdrawal headache in a Norwegian population-based survey was only 0.4% [11]. In previous case-control studies the total number of participants has been <900 [7, 8, 10], and <6,000 in previous cross-sectional studies [5, 6, 9, 11]. Recent reviews of headache epidemiology and health economy have showed that headache constitutes considerable burden on individuals and society [12, 13]. The high prevalence of both headache and caffeine consumption means that even if caffeine is a weak causal factor for headache, this could be of great importance for the public health. Because of divergent results and limited number of participants in previous studies, a study including >50,000 participants should be of interest.
The aim of this large-scale cross-sectional population-based survey was to evaluate the association between caffeine consumption and headache type and frequency.
Materials and methods
Study population
The 1995–1997 HUNT (HUNT 2) study covered a wide range of topics in two questionnaires. The first questionnaire (Q1) was enclosed with the invitation letter and completed at home and delivered during attendance at the health examination. Q1 included three questions about caffeine consumption. The second questionnaire (Q2), which also included questions about headache and ergotamine intake, was filled in after the examination and returned by mail. Of the 92,566 invited inhabitants, a total of 51,383 subjects (56%) completed the headache questionnaire [14], whereof 50,483 (55%) answered the question about caffeine consumption. Details of the non-participants are described elsewhere [14, 15].
The study was approved by the Regional Committee for Ethics in Medical Research, and the HUNT Study is also approved by the Norwegian Data Inspectorate.
Estimation of caffeine consumption
The participants were asked to report the number of cups of brew coffee, other types of coffee (i.e. instant coffee and drip coffee), and tea per day. Based on previous data from Norway [16], the estimated caffeine content per cup was 90 mg for brew coffee, 80 mg for other types of coffee, and 50 mg for tea [16]. Headache patients were asked to report the number of ergotamine tablets and suppositories (Cafergot® and Anervan®) used during the past month. The caffeine content for Cafergot was 100 mg, for Anervan suppository 100 mg, and for Anervan tablets 50 mg. The caffeine consumption per day due to use of ergotamine medication was calculated by dividing the total amount of caffeine due to ergotamine intake by 30. Total overall caffeine consumption (mg/day) was the sum of caffeine per day due to brew coffee, other types of coffee, tea, and ergotamine-containing medication.
Information regarding caffeine consumption due to caffeinated soda, hot chocolate, and other caffeine-containing medications (OTC or prescribed) were not available.
Headache diagnosis
The headache questions in Q2 and the prevalence of headache are published elsewhere [14, 15]. The headache questions were designed mainly to determine whether or not the person had headache, and the frequency of headache, and to diagnose migraine according to a modified version of the migraine criteria of the Headache Classification Committee of the IHS [17]. Subjects who answered “yes” to the question “Have you suffered from headache during the last 12 months?” were classified as headache sufferers. Based on data from the subsequent 12 headache questions, they were classified into two groups of either migraine or non-migrainous headache. The diagnoses were mutually exclusive. A headache which did not fulfil the criteria for migraine was classified as a non-migrainous headache. Based on a question about headache frequency during the last year, headache frequency was divided in three categories; <7, 7–14, and >14 days/month.
The classification of the subjects has been described in detail previously, and has been validated by interview diagnoses [18]. In short, for migraine, the positive predictive value (PPV) was 84% and the negative predictive value (NPV) was 78%; for non-migrainous headache, the PPV was 68% and the NPV was 76% [16]. For the questionnaire-based diagnosis of migraine with aura, the PPV and specificity were 100%, whereas the NPV was 91% and sensitivity was 42% [18].
Statistics
Differences between continuous variables were tested with one-way analyses of variance and between proportions by Chi-squared test. In the multivariate analyses, using logistic regression, we estimated the prevalence odds ratio (OR) with 95% confidence interval (CI) for the association between headache and caffeine consumption. The participants were categorized into quartiles based on individual values of total caffeine consumption. High caffeine consumption was defined as the top quartile (>540 mg/day), whereas low caffeine consumption was defined at the low quartile (0–240 mg/day). Separate analyses for dietary caffeine consumption (excluding caffeine due to use of ergotamine-containing medication) were also done. A large number of confounders were evaluated, e.g. current smoking as it reduces the halftime of caffeine with 30–50% [19], and use of oral contraceptives in women because they increase the level of caffeine with as much as 50% [20]. In the final analyses we adjusted for age, gender, smoking, and education level as confounders. Other potential confounding factors like physical activity, previous myocardial infarction, alcohol consumption, body mass index, and mean systolic blood pressure were also evaluated, but were excluded from the final analyses because they changed the OR by <5%. When appropriate, caffeine consumption was also treated as a continuous variable and was incorporated in a two sided test for trend to evaluate the probability of a linear relationship between caffeine consumption and headache. We also investigated potential interaction between age and caffeine consumption by including the product of the two variables into the logistic regression analyses. The interaction coefficient was tested using Wald χ2 statistics. Data analyses were performed with the Statistical Package for the Social Sciences, version 15.0 (SPSS, Chicago, IL, USA).
Results
Among the 50,483 participants answering questions about caffeine consumption and headache, 19,577 (38.8%) suffered from headache past year; 6,131 (12.1%) from migraine, and the remaining 13,446 (26.6) from non-migrainous headache. A total of 1,163 reported headache >14 days/month, whereof 511 (1.0%) probably had medication overuse headache (MOH) as defined in a previous paper [21].
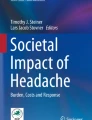
Average dietary caffeine consumption in the general population was 426 mg/day (median 400 mg/day), whereas the average caffeine consumption due to ergotamine intake was 1.4 mg/day (median 0 mg/day) among migraineurs. As demonstrated by Fig. 1, average total caffeine consumption was higher among men than women both in headache sufferers and headache-free individuals.

Mean daily caffeine consumption with 95% confidence interval (CI) among men and women related to headache frequency
Table 1 presents the demographic data and clinical characteristics for the caffeine consumption groups. Among individuals with the lowest caffeine consumption, educational level, level of physical activity, proportion of alcohol abstainers, and proportion of women were significantly higher (P < 0.001) compared to those with higher consumption, whereas, age, proportion of smokers, and prevalence of chronic musculoskeletal complaints were significantly lower (P < 0.001, Table 1). In particular, a low mean age (36.1 years) was found among the minor group of 2,646 (5.2% out of the 50,483 participants) who did not report intake of coffee or tea.
The unadjusted headache prevalence varied with daily caffeine consumption being highest for the group of individuals using >500 mg caffeine daily (Fig. 2). In the multivariate analyses, adjusting for age, gender, smoking, and level of education as confounding factors, the prevalence of headache was higher among individuals with the highest caffeine consumption than among individuals with the lowest consumption (OR = 1.13, 95% CI 1.07–1.20) (Table 2), evident for both men (OR = 1.17, 95% CI 1.06–1.28) and women (OR = 1.13, 95% CI 1.03–1.23) (data not shown). The results were more marked for non-migrainous headache (OR = 1.14, 95% CI 1.07–1.21) than migraine (OR = 1.10, 95% CI 1.01–1.20) (Table 2). No interaction between age and caffeine consumption was found (P = 0.66). Our results did not change if only dietary caffeine consumption was evaluated (data not shown).

Unadjusted headache prevalence (%) related to daily caffeine consumption
As displayed in Table 3, individuals with high caffeine consumption were more likely to have headache <7 days/month than those with low caffeine consumption, and there was a linear trend (P < 0.001) of increasing prevalence of headache <7 days/month with increasing caffeine consumption (Table 3). Non-migrainous headache <7 days/month was 18% more common (OR = 1.18, 95% CI 1.10–1.26) among individuals with high caffeine consumption than among individuals with lowest consumption, evident for both men (OR = 1.21, 95% CI 1.09–1.34) and women (OR = 1.16, 95% CI 1.06–1.28). In contrast, headache >14 days/month was less likely among individuals with intermediate or high caffeine consumption compared to those with low caffeine consumption (Table 3). Because information about use of caffeine-containing OTC medication was not available, we repeated our analyses adjusting for the diagnosis of probable MOH, but these adjustments did not change the results substantially (data not shown).
Discussion
In this large-scale cross-sectional population-based study a weak but significant association was found between high caffeine consumption and migraine and non-migrainous headache, most evident among individuals with infrequent headache. Surprisingly, chronic headache was more prevalent among individuals with low caffeine consumption.
Mean estimated daily caffeine consumption of 426 mg/day was nearly identical with the figures found previously in Sweden (407 mg/day) and in Norway (400 mg/day) [22]. Because the mean daily caffeine consumption in Scandinavian countries is approximately twice as high as in other countries in Europe and in the US, direct comparison of our results with other studies should be done with some caution. However, in the present study headache, including migraine, was 1.1 times more likely (i.e. 10% increased prevalence) among individuals with high caffeine consumption. Somewhat stronger associations were reported in the cross-sectional studies from Australia (headache 1.3 times more likely) and Japan (migraine 2.4 times more likely) [5, 6]. On the other hand, no clear relationship was found between current caffeine consumption and headache in a cross-sectional study from England [9] and in two case-control studies focusing on chronic headache [8, 10]. However, the high prevalence of headache and caffeine consumption means that even if the effect of caffeine consumption on headache prevalence is modest, a reduction could potentially have a large impact on the absolute number of individuals with headache. Thus, based on our results, well designed studies should address the hypothesis that a decrease in caffeine consumption alleviates headache complaints.
Interestingly, when headache frequency was considered, we found that non-migrainous headache <7 days/month was 18% more likely among individuals with high caffeine consumption than among those with lowest consumption. Since the study is cross-sectional, it cannot be concluded that high caffeine consumption causes infrequent headache. There may be a reverse causation, i.e. that some use caffeine to relieve their headache. In addition, although we adjusted for many known confounders, some residual confounding can never be totally excluded. There may be other incompletely registered factors, like sleep disorders, anxiety and other psychological problems which could influence our findings. However, if the association is a causal one, it seems that high caffeine consumption has a higher impact on headache prevalence than previously reported in Vågå in Norway, indicating a prevalence of caffeine-withdrawal headache of only 0.4% [11]. One interpretation of this difference is that caffeine may cause headache not only in connection with withdrawal.
Surprisingly, chronic headache was most likely among individuals with low caffeine consumption. It should be emphasized that the great majority (78%) of these reported intake of coffee and/or tea on a daily basis, and the mean caffeine consumption being 125 mg/day in this group. This low value is of relevance because withdrawal of a maintenance dose of 100 mg caffeine has been shown to induce headache in a double-blind experiment [23]. Similarly, significant reduction of caffeine consumption is also associated with headache [23] which may be of relevance because the low caffeine consumption group may partly consist of individuals who recently had reduced their caffeine consumption. Thus, one can not rule out the possibility that caffeine intake may be a contributing factor for chronic headache in this group.
However, there is no obvious reason why chronic headache was less likely among individuals with intermediate or high caffeine consumption. A possible explanation could be that medium and high caffeine consumption change chronic headache into infrequent headache due to the analgesic properties of caffeine [2]. On the other hand, another quite opposite explanation could be that many chronic headache sufferers had experienced the headache precipitating properties of coffee and therefore reduced their intake, whereas individuals with infrequent headache were less aware that high caffeine consumption can be the cause. This may be analogous to the findings that migraineurs tend to avoid alcohol, to avoid its headache-triggering effect [24].
A potential weakness of the present study is that information regarding caffeine consumption due to caffeinated soda, chocolate, and caffeine-containing OTC medication was not available. Our results are probably most valid for individuals with headache <7 days/month, because use of analgesics containing caffeine was most likely relatively low in this group, whereas such use was probably relatively high among individuals with chronic headache. In the period between 1995 and 1997, the sale of analgesics containing caffeine was approximately five defined daily doses/1,000 inhabitants/day in Norway [25]. Although our results did not change when adjusting for the diagnosis MOH, we cannot rule out that information about caffeine containing analgesics could have changed our results for headache >6 days/month. The caffeine consumption due to caffeinated soda and chocolate in Nord-Trøndelag County was not estimated. It should be emphasized that the chocolate consumption per inhabitants is higher in Norway than in most other countries. However, the caffeine content in caffeinated soda and chocolate is much lower than in e.g. coffee [26], and has been reported to be below 5% of the total caffeine consumption in other studies from Norway and Sweden [22]. Thus, most likely, our questionnaire captured >90% of the total caffeine consumption in Nord-Trøndelag County.
The questionnaire-based headache diagnoses were not optimal compared with the interview diagnosis [18]. The bias caused by misclassification can either exaggerate or underestimate the true difference between headache groups. Most likely, any real difference between migraine and non-migrainous headache sufferers with regard to caffeine consumption will be underestimated because of the presence of migraineurs in the non-migrainous headache group and vice versa, making the two groups more similar than they really are. The impact of non-participants has been discussed in more details previously, and the fact that neither headache nor caffeine consumption questions were the primary objectives of the study makes selective participation unlikely.
Conclusions
In this large cross-sectional study high caffeine consumption was associated with increased prevalence of infrequent headache, whereas chronic headache surprisingly was less likely among individual with high caffeine consumption. The results may indicate that high caffeine consumption changes chronic headache into infrequent headache due to the analgesic properties of caffeine. Alternatively, chronic headache sufferers have reduced the intake of coffee and tea to avoid worsening, whereas individuals with infrequent headache may be less aware that high caffeine use can cause headache.
References
Juliano LM, Griffiths RR (2004) A critical review of caffeine withdrawal: empirical validation of symptoms and signs, incidence, severity, and associated features. Psychopharmacology 176:1–29
Zhang WY (2001) A benefit-risk assessment of caffeine as an analgesic adjuvant. Drug Saf 24:1127–1142
Silverman K, Evans SM, Strain EC, Griffiths RR (1992) Withdrawal syndrome after the double-blind cessation of caffeine consumption. N Engl J Med 327:1109–1114
Dews PB, Curtis GL, Hanford KJ, O’Brian CP (1999) The frequency of caffeine withdrawal in a population-based survey and in a controlled, blinded pilot experiment. J Clin Pharmacol 39:1221–1232
Shirlow MJ, Mathers CD (1985) A study of caffeine consumption and symptoms: indigestion, palpitations, tremor, headache and insomnia. Int J Epidemiol 14:239–248
Takeshima T, Ishizaki K, Fukuhara Y, Ijri T, Kusumi M, Wakutani Y, Mori M, Kawashima M, Kowa H, Adachi Y, Urakami K, Nakashima K (2004) Population-based door-to-door survey of migraine in Japan: the Daisen study. Headache 44:8–19
Bigal ME, Sheftell FD, Rapoport AM, Tepper SJ, Lipton RB (2002) Chronic daily headache: identification of risk factors associated with induction and transformation. Headache 42:575–581
Scher AI, Stewart WF, Lipton RB (2004) Caffeine as a risk factor for chronic daily headache. Neurology 63:2022–2027
Boardman HF, Thomas E, Millson DS, Croft PR (2005) Psychological, sleep, lifestyle, and comorbid associations with headache. Headache 45:657–669
Wiendels NJ, Knuistingh Neven A, Rosendaal FR, Spinhoven P, Zitman FG, Assendelft WJ, Ferrari MD (2006) Chronic frequent headache in the general population: prevalence and associated factors. Cephalalgia 26:1434–1442
Sjaastad O, Bakketeig LS (2004) Caffeine-withdrawal headache. The Vågå study of headache epidemiology. Cephalalgia 24:241–249
Stovner LJ, Hagen K, Jensen R, Katsarava Z, Lipton R, Scher AI, Steiner T, Zwart JA (2007) Headache prevalence and disability worldwide: a documentation of headache prevalence and disability worldwide. Cephalalgia 27:191–210
Stovner LJ, Hagen K (2006) Prevalence, burden and cost of headache disorders. Curr Opin Neurol 19:281–285
Hagen K, Stovner LJ, Zwart JA (2007) Potentials and pitfalls in analytical headache epidemiological studies. Lessons to be learned from the Head-HUNT Study. Cephalalgia 27:403–413
Hagen K, Zwart JA, Vatten L, Stovner LJ, Bovim G (2000) Prevalence of migraine and non-migrainous headache—Head-HUNT, a large population-based study. Cephalalgia 20:900–906
Spigset O (2001) Pharmacological effects of caffeine. Tidsskr Nor Laegeforen 121:3080–3081
Headache Classification Committee of the International Headache Society (1988) Classification and diagnostic criteria for headache disorders, cranial neuralgias, and facial pain. Cepahalalgia 8(Suppl 7):19–28
Hagen K, Zwart JA, Vatten L, Stovner LJ, Bovim G (2000) Head-HUNT: Validity and reliability of a headache questionnaire in a large population-based study in Norway. Cephalalgia 20:244–251
Nastase A, Ioan S, Braga RI, Zagrean L, Moldovan M (2007) Coffee drinking enhances the analgesic effect of cigarette smoking. Neuroreport 18:921–924
Carrillo JA, Benitez J (2000) Clinically significant pharmacokinetic interactions between dietary caffeine and medications. Clin Pharmacokinet 39:127–153
Zwart J-A, Dyb G, Hagen K, Svebak S, Stovner LJ, Holmen J (2004) Analgesic overuse among subjects with headache, neck and low-back pain. Neurology 62:1540–1544
Fredholm BB, Bättig K, Holmén J, Nehlig A, Zvartau E (1999) Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol Rev 51:83–133
Evans SM, Griffiths (1999) Caffeine withdrawal: a parametric analysis of caffeine dosing conditions. J Pharmacol Exp Ther 289:285–294
Aamodt AH, Hagen K, Bråthen G, Zwart J-A, Stovner LJ (2006) Headache prevalence related to smoking and alcohol use. The Head-HUNT Study. Eur J Neurol 13:1233–1238
Rønning M, Strøm H, Blix HS, Litlekare I, Harbø BT, Ullerud TG (1999) Sales per county of other analgesics and antipyretics. In: Øydvin K (ed) Drug consumption in Norway 1994–1998. Norsk Medisinaldepot (NMD), Oslo, pp 167–169
Barone JJ, Roberts R (1996) Caffeine consumption. Food Chem Toxicol 34:119–129
Acknowledgments
The Nord-Trøndelag Health Study (The HUNT Study) is a collaboration between The HUNT Research Centre, Faculty of Medicine, The Norwegian University of Science and Technology (NTNU); Norwegian Institute of Public Health; and the Nord-Trøndelag County Council.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Hagen, K., Thoresen, K., Stovner, L.J. et al. High dietary caffeine consumption is associated with a modest increase in headache prevalence: results from the Head-HUNT Study. J Headache Pain 10, 153–159 (2009). https://doi.org/10.1007/s10194-009-0114-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10194-009-0114-6