
Abstract
With the outbreak of the novel coronavirus (COVID-19), the generation of a large amount of medical waste brought a rude shock to the existing solid waste management system. Since masks constitute the most common household medical waste under the COVID-19 pandemic, their effective collection and treatment can significantly reduce the potential risks for secondary transmission, and this concern has attracted worldwide attention. Taking Macau City as a case study, this research tried to identify factors that can influence residents’ behavioral intentions toward the source separation of COVID-19 waste masks. The extended theory of planned behavior (TPB) model is used to examine the influence factors of the source separation behaviors of 510 respondents. The results show that the main factors that positively affected respondents’ behavioral intentions toward waste-mask source separation are: cognitive attitude, convenience, and perceived behavioral control, and among these, cognitive attitude has the highest influence. Subjective norm is also proved to be the weak factor to improving behavioral intention. Policy advocacy, and demographic variables have no significant effect on behavioral intention. The results of this study can help decision makers and managers formulate effective strategies to increase residents’ participation in the source separation of waste masks.
Similar content being viewed by others


Introduction
Since December 2019, the sudden outbreak of a novel coronavirus (also known as COVID-19) has attracted worldwide attention. As of March 3, 2021, COVID-19 had caused 116 million infections and 26 million deaths [1]. During this crisis, most governments announced border closures and issued a series of guidelines (such as wearing masks, washing hands more frequently, and keeping socially distant) to reduce the infection risks and limit the spread of COVID-19. With these epidemic prevention and control requirements, a large amount of medical waste has been generated. Although the global blockade caused by the response to COVID-19 has brought some positive environmental impacts (such as the improvement of air quality and river water quality) [2], this is not the case for solid waste management. During the epidemic period, the composition of daily household waste has changed dramatically, and personal protective equipment (masks, disinfectant, gloves, etc.) has become common household waste, bringing great challenges to the waste treatment system [3]. In China, the daily medical waste related to the COVID-19 pandemic was about 468.9 tons [4]. It is estimated that the daily average production of COVID-19 medical waste in the world increased from 200 tons/day in February to 29,000 tons/day at the end of September 2020 [5]. The huge increase in and improper collection of medical waste contribute not only to environmental pollution, but also to the spread of COVID-19 itself [6]. The effective management of medical waste should be regarded as an urgent and important public service, to prevent negative environmental impacts and the risk of secondary transmission via the waste stream.
To prevent COVID-19 infection, masks have become indispensable protective equipment for the public [7, 8]. The role of masks is to reduce the spread of droplets from infected individuals and greatly reduce the possibility of virus waves [9]. The World Health Organization (WHO) as well as health organizations in most countries have suggested that residents need to wear masks in the communal environment [10, 11]. Wearing a mask has been considered an effective way of reducing the spread of COVID-19, and has become a community custom and an important prerequisite for social activities. However, because of the high possibility of viruses escaping outside the mask, it is not recommended to reuse a mask [3]. According to the guidelines published by the National Health Commission of China (NHCRC), the use of medical masks and disposable masks is limited in low-risk areas or among people with non-occupational exposure, and the cumulative use time (wearing) of a mask should not exceed 8 h [12]. The WHO reports that 89 million medical masks are required per month [13]. At the same time, it is estimated that the global consumption of disposable masks has reached 6.6 billion units, with a total weight of 2641 tons as of August 2020 [3]. High consumption levels of these masks lead to the generation of large amounts of solid waste. How to effectively manage the waste masks has become the top priority of municipal solid waste (MSW) management.
COVID-19 medical waste is produced not only in hospitals, but also within ordinary residential premises. Compared with the centralized treatment of medical waste in hospitals, waste masks from households are often mixed in with other MSW [14]. However, a research report pointed out that the COVID-19 virus has different survival times in different materials, such as: atomized copper, 3 h; cardboard, 4 h; plastic, 24 h; and stainless steel, 2–3 days [15]. In addition, Kampf et al. [16] indicated that the COVID-19 virus could survive for 9 days on inanimate solid surfaces such as metal, plastic and glass. As a result, mixed collection may contaminate other common MSW and even contribute to the spread of COVID-19. Identifying source separation of COVID-19 waste is extremely important during an epidemic, not only to reduce costs but also to help prevent the spread of the virus [17].
Compared with other medical wastes, most masks are designed for single use, there is a higher frequency of replacement and disposal, resulting in a large volume of waste masks being generated every day. Waste masks have become bulk wastes that must be processed or disposed of properly. A good waste-mask recycling and disposal system needs to consider not only the treatment technology and cost, but also the behavioral intentions of residents [18]. Previous studies have shown that residents’ consensus is an important prerequisite for implementing solid waste management [19]. Residents’ demographic variables, perceived behavioral control, behavioral intentions and environmental attitudes are all important factors that affect whether residents support a waste management system [18,19,20,21]. In addition, Irfan et al. [22] analyzed the factors that prompt Pakistani residents to wear masks or prevent residents from wearing masks based on the expanded TPB model. Zhao et al. [23] assessed the self-reported face mask wearing status and related perceptions, and reported that compared with the Europeans, Chinese participants showed a stronger pro-masking tendency. To prevent the secondary infection and pollution of waste masks, it is very important to identify residents’ behaviors for the source separation of waste masks. However, there have been few studies on residents’ behavioral responses to the source separation of waste masks. To fill this gap, this study attempts to construct an extended Theory of Planned Behavior (TPB) framework to understand residents’ attitudes and the influencing factors of residents’ willingness to participate in source separation. The research results can provide theoretical data for policy managers and makers, and provide a scientific basis for the rational source separation of waste masks.
Literature review the theory of planned behavior
As of March 2021, TPB had been cited nearly 90,000 times, according to a Google Academic Search. Although there are other competing behavior models, the TPB model has always been one of the most widely used frameworks to investigate individual behavior, and is also considered the most effective model for designing behavior intervention [24]. In 1975, Fishbein and Ajzen [25] put forward the rational behavior theory (TRA) on the premise that human behavior can be controlled by human consciousness. However, due to its lack of consideration of human intention, this theory has been highly controversial [26]. The TPB model was formally proposed by Ajzen [27], and a key variable (perceptual behavior control) was added to the TRA model [28]. According to the theory, three important determinants—cognitive attitude, perceived behavioral control and subjective norm—perform the analysis function of behavioral intention. These variables jointly analyze behavioral intention and speculate on human behavior [21].
TPB has been widely used to predict and explain environmental behavior [29], especially in the field of waste recovery [21, 26, 30,31,32]. TPB is also a flexible model that can be used to evaluate specific populations [24]. To better study the recycling behavior, additional variables can be added to enhance TPB’s explanatory capabilities [28]. Considering that decision makers’ intentions may be influenced by other important factors [26], this study also adopted some other key variables in the TPB model. (1) Convenience is usually considered an important variable for waste recovery [21, 33, 34]; it is described as the convenience and time available to an individual for waste management [35], and is also an assessment of whether an individual has time to collect, sort and treat waste [21]. (2) Policy advocacy is usually an important factor affecting residents’ behavioral intentions. Since source separation of waste masks is a time-consuming activity, residents’ understanding on policies can help increase their willingness, although this understanding is related to their trust in the government’s waste management policies [32]. (3) Demographic variables—especially monthly income and educational level—may also play an important role in recycling behavior [18,19,20].
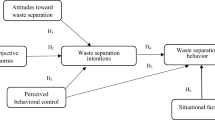
As shown in Fig. 1, this study built an extended TPB model framework to investigate six possible influencing factors of waste-mask source separation: cognitive attitudes, subjective norms, perceived behavioral control, demographic variables, convenience and policy advocacy variables.

Extended TPB model framework for waste-mask source separation
Research hypotheses
Cognitive attitudes
As a psychological characteristic, attitude is an evaluative reflection of a problem (preference or non-preference) [31]. Attitude toward a specific behavior can inspire people to specific behavioral intentions [28]. In general, the more preference a person has for a behavior, the greater the individual’s willingness to perform that behavior. Tonglet et al. [36], Wang et al. [30] and Aboelmaged [31] confirmed that attitude is a strong predictor of e-waste recycling intention. At present, cognitive attitude is considered a good predictor of pro-environment behavior, and is related to an individual’s ability to bear the risks and uncertainties caused by decisive factors [37]. However, Russell et al. [29] pointed out that attitude alone cannot successfully affect the intention to reduce food waste. Khan et al. [21] reported that attitudes did not significantly affect consumers’ behavioral intentions to deal with plastic waste. To test whether attitude is an important predictor of residents’ intention to participate in waste-mask management, this study puts forward the following cognitive-attitude hypothesis:
H1
Cognitive attitude positively affects residents’ intentions of performing waste-mask source separation.
Subjective norms
In the TPB model, social influence is represented by the concept of a subjective norm [38]. Subjective norms represent the social pressure to perform certain behaviors [28]. Many studies have reported that subjective norms are positively correlated with behavioral intentions [21, 39]. However, there is great uncertainty about how effective a subjective norm is, in influencing behavioral intentions [31, 36]. This study proposes the following subjective-norm hypothesis:
H2
Subjective norms positively affect residents’ behavioral intentions toward the source separation of waste masks.
Perceived behavioral control
Perceived behavioral control is our confidence and control over intentional behavior. Many studies have shown that perceived behavioral control has a positive effect on recycling behavior and is an important factor in predicting people’s intentions for pro-environment behavior [29, 40, 41]. Russell et al. [29] reported that the stronger a consumer’s perceived behavioral control, the stronger their intention to reduce food waste. Cao [41] proposed that the better respondents perceive the recycling conditions to be, the more likely they will participate in the recycling of express packaging waste. However, other studies have shown that there is no significant relationship between perceived behavioral control and behavioral intention [21, 31]. To verify whether residents’ intrinsic perceptual behavior control has an impact on their intention to participate in the source separation of waste masks, this study puts forward the following behavioral-control hypothesis:
H3
Perceived behavioral control has a positive effect on residents’ behavioral intentions toward waste-mask source separation.
Convenience
Convenience (including the facilities, cost, time and difficulty of operation) refers to a person’s ease of performing a certain behavior [21]. Previous studies have pointed out that convenience is an important influence on recycling behaviors [21, 33, 34]. Kochan et al. [33] believed that as the complexity of recycling storage decreases, residents’ willingness to participate in recycling may increase significantly. In this study, convenience is also considered an important factor, and this study puts forward the following convenience hypothesis:
H4
Convenience has a positive effect on residents’ behavioral intentions toward waste-mask source separation.
Policy advocacy
The formation of a perfect waste recycling channel requires not only laws and regulations, but also policy advocacy, to guide residents’ perceptions. Previous studies have shown that policy measures can change people’s perceptions and behavior [40, 42]. Wan et al. [40] reported that governmental policies and advocacy would enhance consumers’ willingness to participate in waste recycling. In general, publicizing the policy will help enhance residents’ environmental awareness. It is believed that policy advocacy is an important predictor of residents’ behavioral intentions to recycle waste masks. This study puts forward the following policy-advocacy hypothesis:
H5
Policy advocacy has a positive impact on residents’ behavioral intentions toward waste-mask source separation.
Demographic variables
In general, waste generation and recycling are mainly affected by demographic characteristics, socio-economic characteristics, structural characteristics, and governmental policies [43, 44]. Previous studies have shown that monthly income, educational level and family size are the key factors affecting residents’ recycling intentions [18, 45, 46]. Meanwhile, age and gender may also be related to waste recycling behavior. Saphores et al. [47] believed that the higher the educational level of young people, the more willing they are to support environmental protection. Therefore, we propose the following demographic hypothesis:
H6
Demographic variables have a positive impact on residents’ behavioral intentions toward waste-mask source separation.
Questionnaire design, survey and data collection
Macau has made important achievements in coping with the crisis of COVID-19 (as of February 2021, only 48 people were infected and none died from COVID-19) [48]. However, due to the small land area and the increasing COVID-19 medical waste, Macau’s solid waste management system is under great pressure [19]. Currently, medical wastes in Macao are incinerated at high temperature in Special and Hazardous Waste Treatment Station (SHWTS). However, due to insufficient treatment capacity (24 metric tons per day), the medical waste received in SHWTS exceeds the treatment capacity undre the COVID-19 pandemic (see Fig. S1). The COVID-19 medical waste must be treated without delay, thus parts of these medial waste end in the Macao Incineration Plant (MIP) for Municipal solid waste. Although China (including Macao) has not formulated a special policy on source separation of waste masks, some regions (e.g., Chongqing City, Xiamen city, Foshan City and Shandong Province) require to set up special recycling containers for waste masks in public places (residential quarters, business districts and stations, etc.) [49]. In Macao, some residential quarters, buildings and universities also spontaneously set up special waste-mask containers. Sanitation workers will regularly disinfect the waste masks every day and transfer them to the next level of processing facilities (SHWTS or MIP). However, because COVID-19 virus has strong concealment and infectivity, incorrect disposal of waste masks may actually increase the rate of viral transmission. With the normalization of epidemic prevention and control, the volume of waste masks has increased sharply. It is still necessary to formulate special management regulations, and build a system for recycling and centralized disposal of daily waste masks. A good recycling system for waste masks depends not only on the external environment (the government and the recycling enterpreise), but also on the internal environment (e.g., the public’s recycling intention). Residents’ participation is an important prerequisite for implementing solid waste management policy. However, due to the lack of policy guidance, the residents would discard waste masks directly into garbage cans at home, or public garbage cans. Whether Macao residents are willing to participate in the waste-mask source separation is still an important issue that needs to be explored urgently. Therefore, to verify the hypotheses, this study selected Macao as the case study to identify the important influence factors on the residents’ source separation behaviors of waste masks. The types of masks studied include disposable common masks, disposable medical masks, non-valve N95 masks and N95 masks with valves, etc. Meanwhile, all kinds of waste masks are considered to need source separation in this study. Figure 2 shows the main structure of the questionnaire survey.

Structure of our survey on waste masks
Questionnaire design
There were four steps to setting up the questionnaire on what affects Macau residents’ behavioral intentions toward waste masks. The first was to investigate the medical waste generated due to the epidemic in Macau, and to obtain useful information about epidemic medical waste through online information collection and consultation via postal mail. Secondly, a team of graduate students from Macau University of Science and Technology investigated the academic papers published in international journals, mainly focusing on TPB methods and solid waste management, finally obtaining a list of 40 items. Next, the items were modified and supplemented by three researchers (professors from Macau University of Science and Technology). To complete the questionnaire, a preliminary survey was organized and 31 items were finally determined for inclusion.
The questionnaire consisted of three parts. The first part refers to the demographic variables of the respondents, including age, monthly income, family size, etc. The second part refers to the use and disposal behaviors with regard to masks. In the third part, six influencing factors—cognitive attitude, subjective norms, perceived behavioral control, convenience, policy advocacy and behavioral intention—were investigated; these were adopted from Tonglet et al. [36], Ramayaht et al. [50], Saphores et al. [47], Cao [41] and Wan et al. [40]. In this study, the five-point Likert scale was adopted to describe the questionnaire, and the indicators are shown in Table S1.
Questionnaire survey and data collection
For the pre-investigation, 50 questionnaires from residents and hospital staff were processed by university students working on the study. Based on the results of the pre-investigation, the questionnaire was revised to improve its rationality and scientific integrity.
The resulting final questionnaire survey was carried out through online entry and an offline survey. The off-line survey was conducted in the Macau Peninsula area by the experienced students; the online questionnaire survey was conducted via the Questionnaire Star platform. By setting the location and pre-filling some responses via IP management, it was ensured that only Macau residents could fill in the questionnaire, and that each user could fill in it only once, thereby guaranteeing its authenticity. In addition, to ensure that respondents could clearly understand the meaning of the questions, rare words and professional and academic words were excluded from the questionnaire as much as possible. Finally, 545 questionnaires were collected, and 510 valid questionnaires were obtained—an effective rate of 93.58%.
Results and analysis
Descriptive statistical analysis
Basic information
As shown in Table 1, respondents aged 18–30 years made up the largest group, followed by those aged 31–40 years. The ratios of male to female were similar for all the participant groups. In addition, more than 50% of the respondents had a bachelor’s degree or higher. Most respondents (> 50%) had a monthly income higher than 20,000 MOP. Finally, in terms of occupation, 12.35% of the respondents were engaged in the medical profession [51]. Compared with data from the Macau statistical yearbook, the survey data are close to the average level for Macau residents (indicated in the rightmost column), except for occupation.
Data analysis
Before data analysis, each item of the respondents’ intentions and influencing factors for waste-mask treatment was coded (1–5), and exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were then carried out.
EFA is mainly used to analyze the nature of a multivariate observation structure and reduce a large number of variables into a smaller number of factors [30], verifying data validity. Since validity is a relative value rather than an absolute one, it can pass the KMO and Bartlett value tests. Through SPSS19.0 software, the validity of the initial questionnaire was tested and is shown in Table 2. The KMO value is 0.858, greater than 0.7 (the critical value), and the Chi-square value of myopia in the Bartlett spherical test is 4234.086 (P value < 0.01), which indicates that the designed factors are suitable for factor analysis. Secondly, 18 indicators were tested based on principal component analysis. By observing the key parameters such as cumulative contribution rate, common factor variance and factor load (see Table S2), it was found that the retention factor was almost the same as the initial ratio, and Cronbach’s alpha value of all variables was close to or greater than 0.7 (see Table 2), indicating that the scale has sufficient reliability.
Then, CFA was adopted to determine whether the scale data support the constructs extracted from EFA [52] using Amos 21.0 software. The convergence validity of all variables was tested, to measure the relative degree between two variables of the same structure [53, 54]; these data are shown in Table 3. Although the average extracted variance (AVE) values of most variables are greater than or equal to 0.5, the AVE values of convenience and policy advocacy are lower than 0.45, indicating that the convergence validity of the questionnaire is not ideal. To ensure the validity of the content, we re-identified, fitted and evaluated the scale data. Finally, after deleting DC1 of convenience and all topics of policy advocacy (PA1–3), the model shows good fitting degree. At the same time, the AVE values of all variables are greater than or equal to 0.5, and the composite reliabilities (CR) of all constructs are greater than 0.6, indicating that the ideal internal quality of the questionnaire meets the requirements.
In addition, discriminant validity is established to understand the difference between one construct and another [21]. The discriminant validity is mainly determined by the heterogeneity-single trait ratio and the cross load between items [21]. As shown in Table 4, the diagonal values represent the square of AVE, and other values are the correlations between the aforementioned variables. In general, the square root value of AVE should be greater than the correlation of other constructs [54]. Therefore, the results in Table 5 confirm the validity of the discriminant validity.
Structural equation model (SEM)
After EFA and CFA analysis, the structural equation model (SEM) was selected to test the theoretical model. SEM involves using some observable variables to test an unobservable variable, and reflecting the degree of model fitting based on various indicators [30]. Using AMOS 21.0 software, the maximum probability estimation method was used to evaluate the significance of the model fitting, coefficient and structural path of residents’ behavioral intentions. Policy advocacy was deleted due to low validity. As shown in Fig. 3A, the conceptual model included five potential variables (subjective norm, perceived behavior control, convenience, cognitive attitude, demographic variables and behavioral intention) and 19 items.

Structural equation model of waste-mask source separation intention (SN subjective norms, PBC perceived behavioral control, CO convenience, CA: cognitive attitude, BI behavioral intention). A initial model; B revised model
Model fitness test
Table 5 shows the evaluation criteria of the SEM adaptation index, including the main absolute adaptation statistics, value-added adaptation statistics and simple adaptation statistics. Firstly, we verify the initial model (see Fig. 3A). As shown in Table 5, it can be found that the data fitting effect of this model is not ideal, and five indexes fail. Therefore, the model is constantly revised and the final model is obtained (see Fig. 3B). It can be found that the covariance matrix of the revised model fits well with the actual data (CMIN/DF value 1.09 < 3). In addition, RMSEA, NFI, IFI, PGFI and most other indicators are consistent with the alignment judged by the SEM model, which also supports the hypothesis that the model has good adaptability. In summary, it can be considered that the theoretical hypothesis fits well with the sample data.
Path analysis and hypothesis testing
Table 6 presents the path result analysis of the structural equation model. The results show that cognitive attitudes (β = 0.659, P < 0.01), perceived behavioral control (β = 0.191, P < 0.01) and convenience (β = 0.409, P < 0.01) have significant effects on behavioral intention toward the source separation of waste masks. Thus, H1, H3 and H4 are confirmed. In addition, subjective norms (β = 0.133, P < 0.05) had a weak effect on the behavioral intention. Hence, H2 is confirmed. However, demographic variables are not significant for behavioral intention, so H6 is rejected. Previous analysis shows that policy advocacy variables is not applicable to the model, so H5 were rejected.
Discussion, conclusions and recommendations
Because of the risk of secondary infection, waste masks are a special kind of solid waste. Source separation and recycling is the most suitable way to dispose of waste masks. However, in Macau, the source separation of waste masks has not received enough attention. Identifying respondents’ behavioral intentions will help improve MSW management. This study explored the respondents’ behavioral intention for source separation of waste masks and its influencing factors, and will help policy managers design plans to promote waste-mask recycling activities.
Exploring the influence of key factors on respondents’ behavioral intentions
Based on the expanded TPB, we developed a reliable scale and surveyed more than 500 residents. After obtaining the data, the hypotheses were tested by the structural equation of AMOS 21.0 software. The results show that convenience, cognitive attitude and perceived behavioral control are the main factors affecting residents’ behavioral intentions to engage in waste-mask source separation. Meanwhile, subjective norms weak affect residents’ behavioral intentions toward waste-mask source separation. However, demographic variables (gender, occupation, monthly income, education and age) had no effect on behavioral intention.
As mentioned above, cognitive attitude has a significant positive impact on behavioral intention, and the impact coefficient reached 0.659, the highest among all the predictive factors. As cognitive attitude is the residents’ subjective evaluation of waste-mask source separation, the more positive a resident’s attitude, the stronger their willingness to recycle [31, 36]. It can be seen that the residents who pay more attention to hygiene risk have higher intentions toward waste-mask source separation. In this study, it is indicated some respondents still did not understand the significance of source separation. In general, only when residents think that the source separation of waste masks is everyone’s responsibility and obligation, their attitude will become more positive [30]. Therefore, it is very necessary to cultivate residents’ knowledge of waste-mask source separation through various channels (community lectures, advertisements or education, etc.), thereby promoting the transformation of this perception to environmental behavior. In addition, the loss of perceived benefits (lower satisfaction) will affect residents’ willingness to participate in waste-mask source separation. Thus, when implementing a waste source separation plan, policy makers and managers should also fully consider and improve residents’ acceptance or satisfaction, so as to promote the source separation behavior.
Convenience has great attraction for residents, encouraging them to participate in waste-mask source separation; its influence coefficient is 0.409, making it an important predictor. When individuals feel comfortable participating in waste source separation activities, they will actively do so [21]. Participation is also related to the availability of recycling infrastructure, distance to recycling facilities and time required to participate in recycling. Therefore, the higher the convenience, the stronger the residents’ intentions to participate in waste source separation.
At the same time, increasing individual PBC also contributes to improving residents’ behavioral intention (influence coefficient: 0.191). If residents perceive that the waste-mask source separation process is simple, they are more likely to participate in it [29]. When the government implements a waste source separation plan, it can launch an education plan to publicize the location of the recycling facilities and explain how to participate in the operation guidelines, such as classification, storage and disposal of waste masks. All these actions will help promote the source separation of waste masks.
In addition, subjective norm is also proved to be the factor to improving behavioral intention. Subjective norms are created by external pressures (i.e., the degree of influence of others) [38]. The source separation of waste masks is a pro-environment behavior. Residents’ ideas are usually influenced by their surroundings or activities, eg., changing their behavioral intention toward waste source separation. Therefore, if policy makers can turn waste source separation and resource utilization into a “trendy” activity (a social trend), and strengthen publicity to improve residents’ satisfaction, it will obviously promote waste-mask source separation.
Although this study has not confirmed the influence of policy advocacy on the source separation of waste masks, previous studies have shown that when people hold a positive view on a policy’s effectiveness, their recycling behavior will also increase [40, 55]. There is reason to believe that policy advocacy is still an important factor in the source separation of waste masks. Policy formulation will restrain and improve residents’ source separation intention. Policy makers and managers should still raise people’s awareness of the policy’s potential effectiveness through publicity activities [40, 55]. By publicizing the government’s work, progress and achievements (environmental improvement) in the recycling plan, the residents can be educated to participate in the source separation of waste masks.
In general, residents with higher educational levels should have higher willingness to participate in waste-mask source separation [18]. However, educational level is an unreliable predictor, and high educational level alone cannot improve residents’ environmental awareness [20], possibly because the management of waste masks is still in its initial stage, the responsibility for recycling is unclear, and the publicity has been insufficient, failing to arouse residents’ intentions to separate waste masks, and they do not know how to properly recycle and dispose of the masks. There is still a need to cultivate their responsibility for the environment and help them understand the importance of waste-mask source separation.
These research results are of great significance for policy makers to solve the problem of household medical waste, even though with the increasing control over the and the development of a vaccine, the number of people infected with COVID-19 can be not expected to decrease significantly in the near future.The residents’ dependence on masks will also not decrease, even increase in the short term [56]. As Tripathi et al. [3] suggests that COVID-19 will continue to be prevalent in the coming years, it is extremely important to develop a long-term management plan for solid waste (especially masks). Residents are the core stakeholders of waste classification and recycling, and it is very important to determine the factors that affect residents’ behavioral intentions, especially in a small land area like Macau [18, 19]. With the increasing number of waste masks, the environmental and social pressures will continue to increase. Therefore, the results of this study are expected to provide theoretical support and scientific basis for the management of waste masks in Macau and other counries and regions.
Implications
As of this writing, Macau has accomplished a great deal in its efforts to control the COVID-19 epidemic and prevent its further spread. Yet these prevention and control measures have brought on another problem—the generation of a large number of waste masks [3, 7]. It is of great concern that there is no special management policy on medical waste (waste masks) in Macau [57]. An increasing amount of solid waste always results in a huge challenge to an existing solid waste management system [58, 59]. Establishing a management system for waste masks will help alleviate their environmental impacts. It is worth noting that the role of residents needs to be included in the process of formulating management policies for waste masks [20, 59]. Improving residents’ behavioral intention is the key to implementing an effective waste management policy. This study can provide some practical applications for managers and decision makers, in the formulation of such a policy.
First of all, low environmental awareness and lack of knowledge about mask hygiene may be hindering residents’ ability to participate in waste-mask source separation. Therefore, Macau’s policy of carrying out more environmental protection activities and delivering health-risk lectures can improve residents’ knowledge and understanding of waste-mask source separation, and enable them to transform their environmental awareness into environmentally responsible behavior.
Secondly, convenience can positively influence residents’ intention to participate in waste-mask source separation. To facilitate the source separation of waste masks, policy makers should set up a reasonable recycling infrastructure for processing waste masks, based on actual local situations, to promote residents’ intentions to participate in waste-mask source separation.
Third, the government should cooperate with universities and other educational institutions to set up environmental protection courses to cultivate students’ environmental concern and ethics. These students can then educate their relatives and neighbors and encourage them to participate in the source separation of waste masks, eventually developing a communal environmental ethic around this issue.
The last and most critical step is the work of managers and decision makers. Establishing a sound policy or guideline will help improve the waste management system and serve as a guide for residents to participate in waste recovery. Managers and decision makers need to pay special attention to policy advocacy in the process of formulating and implementing these policies. At the same time, the current situation of waste management should be widely publicized; it would be an effective means of motivating residents to help implement the official waste-mask source separation policy, explaining the current situation and available waste-mask disposal methods to the public, and increasing public enthusiasm to participate in waste-mask source separation.
References
WHO (2021) Real-time global epidemic situation. Available at: http://www.chinanews.com/m/34/2020/0318/1388/globalfeiyan.html. Accessed 3 Mar 2021
Gardiner B (2020) Pollution made COVID-19 worse. Now, lockdowns are clearing the air. National Geographic. https://www.nationalgeographic.com/science/2020/04/pollution-made-the-pandemic-worse-but-lockdowns-clean-the-sky/. Accessed 15 May 2020
Tripathi A, Tyagi VK, Vivekanand V, Bose P, Suthar S (2020) Challenges, opportunities and progress in solid waste management during COVID-19 pandemic. Case Stud Chem Environ Eng 2:100060
Peng J, Wu X, Wang R, Li C, Zhang Q, Wei D (2020) Medical waste management practice during the 2019–2020 novel coronavirus pandemic: Experience in a general hospital. Am J Infect Control 48(8):918–921
Liang Y, Song Q, Wu N, Li J, Zhong Y, Zeng W (2021) Repercussions of COVID-19 pandemic on solid waste generation and management strategies. Front Environ Sci Eng 15(6):115
Singh N, Tang Y, Zhang Z, Zheng C (2020) COVID-19 waste management: effective and successful measures in Wuhan. China Resour Conserv Recycl 163:105071
Si H, Shen L, Liu W, Wu G (2021) Uncovering people’s mask-saving intentions and behaviors in the post-COVID-19 period: evidence from China. Sustain Cities Soc 65:102626
de Sousa FDB (2021) Plastic and its consequences during the COVID-19 pandemic. Environ Sci Pollut Res Int 28(33):46067–46078
Hartanto BW, Mayasari DS (2021) Environmentally friendly non-medical mask: an attempt to reduce the environmental impact from used masks during COVID 19 pandemic. Sci Total Environ 760:144143
WHO (2020a) In: Advice on the use of masks in the Community, during home care and in health care settings in the context of the novel Coronavirus (2019-nCoV) outbreak. World Health Organization. Interim Guidance 29 January 2020. Available at https://www.apps.who.int/iris/bitstream/handle/10665/330987/WHOnCov-IPC_Masks-2020.1-eng.pdf?. Accessed 11 Mar 2020
NHCRC (National Health Commission of the People’s Republic of China) (2020a) Face mask use guidelines for preventing against Coronavirus disease (COVID-19) transmission. Available from http://www.nhc.gov.cn/xcs/zhengcwj/202001/a3a261dabfcf4c3fa365d4eb07ddab34. Accessed 31 Jan 2020
NHCRC (National Health Commission of the People’s Republic of China) (2020b) Guidelines for the public scientific wearing of masks. Available at http://www.nhc.gov.cn/jkj/s3577/202003/0a472cc09e744144883db6a74fe6e760.shtml. Accessed 18 Mar 2020
WHO (2020b) Shortage of personal protective equipment endangering health workers worldwide. The World Health Organization. Available at https://www.who.int/news-room/detail/03-03-2020-shortage-of-personalprotective-equipment-endangering-health-workers-worldwide. Accessed 30 Apr 2020
Das AK, Islam MN, Billah MM, Sarker A (2021) COVID-19 pandemic and healthcare solid waste management strategy—a mini-review. Sci Total Environ 778:146220
Van Doremalen N, Bushmaker T, Morris D, Holbrook M, Gamble A, Williamson B, Tamin A, Harcourt J, Thornburg N, Gerber S, Lloyd-Smith J, de Wit E, Munster V (2020) Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. New Engl J Med 382(16):1564–1567
Kampf G, Todt D, Pfaender S, Steinmann E (2020) Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect 104(3):246–251
Valizadeh J, Hafezalkotob A, Seyed Alizadeh SM, Mozafari P (2021) Hazardous infectious waste collection and government aid distribution during COVID-19: a robust mathematical leader-follower model approach. Sustain Cities Soc 69:102814
Song Q, Wang Z, Li J (2012) Residents’ behaviors, attitudes, and willingness to pay for recycling e-waste in Macau. J Environ Manag 106:8–16
Song Q, Wang Z, Li J (2016) Exploring residents’ attitudes and willingness to pay for solid waste management in Macau. Environ Sci Pollut Res Int 23:16456–16462
Cai K, Song Q, Peng S, Yuan W, Liang Y, Li J (2020) Uncovering residents’ behaviors, attitudes, and WTP for recycling e-waste: a case study of Zhuhai city. China Environ Sci Pollut Res Int 27(2):2386–2399
Khan F, Ahmed W, Najmi A (2019) Understanding consumers’ behavior intentions towards dealing with the plastic waste: perspective of a developing country. Resour Conserv Recycl 142:49–58
Irfan M, Akhtar N, Ahmad M, Shahzad F, Elavarasan RM, Wu H, Yang C (2021) Assessing public willingness to wear face masks during the COVID-19 pandemic: fresh insights from the theory of planned behavior. Int J Environ 18(9):4577
Zhao X, Knobel P (2021) Face mask wearing during the COVID-19 pandemic: comparing perceptions in China and three European countries. Transl Behav Med 11(6):1199–1204. https://doi.org/10.1093/tbm/ibab043
Yuriev A, Dahmen M, Paillé P, Boiral O, Guillaumie L (2020) Pro-environmental behaviors through the lens of the theory of planned behavior: a scoping review. Resour Conserv Recycl 155:104660
Fishbein M, Ajzen I (1975) Belief, attitude, intention, and behavior: an introduction to theory and research. Addison-Wesley, Reading
Khan O, Daddi T, Slabbinck H, Kleinhans K, Vazquez-Brust D, De Meester S (2020) Assessing the determinants of intentions and behaviors of organizations towards a circular economy for plastics. Resour Conserv Recycl 163:105069
Ajzen I (1985) From intentions to actions: a theory of planned behavior action control. Springer, Berlin, pp 11–39
Ajzen I (1991) The theory of planned behavior. Organ Behav Hum Decis Process 50:179–211. https://doi.org/10.1016/0749-5978(91)90020-T
Russell SV, Young CW, Unsworth KL, Robinson C (2017) Bringing habits and emotions into food waste behaviour. Resour Conserv Recycl 125:107–114
Wang Z, Guo D, Wang X (2016) Determinants of residents’ e-waste recycling behaviour intentions: evidence from China. J Clean Prod 137:850–860
Aboelmaged M (2021) E-waste recycling behaviour: an integration of recycling habits into the theory of planned behaviour. J Clean Prod 278:124182
Echegaray F, Hansstein FV (2017) Assessing the intention-behavior gap in electronic waste recycling: the case of Brazil. J Clean Prod 142:180–190
Kochan C, Pourreza S, Tran H, Prybutok VR (2016) Determinants and logistics of e-waste recycling. Int J Logist Manag 27(1):52–70
Wan C, Zhang X, Cheung R, Qiping Shen G (2012) Recycling attitude and behaviour in university campus: a case study in Hong Kong. Facilities 30(13/14):630–646
Kianpour K, Jusoh A, Mardani A, Streimikiene D, Cavallaro F, Nor KM, Zavadskas E (2017) factors influencing consumers’ intention to return the end of life electronic products through reverse supply chain management for reuse repair and recycling. Sustainability 9(9):1665
Tonglet M, Phillips PS, Read AD (2004) Using the Theory of planned behaviour to investigate the determinants of recycling behaviour: a case study from Brixworth, UK. Resour Conserv Recycl 41(3):191–214
Liu Y, Hong Z, Zhu J, Yan J, Qi J, Liu P (2018) Promoting green residential buildings: Residents’ environmental attitude, subjective knowledge, and social trust matter. Energy Policy 112:152–161
Wan C, Shen GQ, Choi S (2017) Experiential and instrumental attitudes: Interaction effect of attitude and subjective norm on recycling intention. J Environ Psychol 50:69–79
Jiang L, Zhang J, Wang HH, Zhang L, He K (2018) The impact of psychological factors on farmers’ intentions to reuse agricultural biomass waste for carbon emission abatement. J Clean Prod 189:797–804
Wan C, Shen GQ, Yu A (2014) The role of perceived effectiveness of policy measures in predicting recycling behaviour in Hong Kong. Resour Conserv Recy 83:141–151
Cao X, Liu C (2019) Research on customers’ willingness to participate in express package recycling. IOP Conf Ser Earth Environ Sci 295
Wan C, Shen GQ, Yu A (2015) Key determinants of willingness to support policy measures on recycling: a case study in Hong Kong. Environ Sci Policy 54:409–418
Soukiazis E, Proenca S (2020) The determinants of waste generation and recycling performance across the Portuguese municipalities—a simultaneous equation approach. Waste Manag 114:321–330
Milovantseva N, Saphores J (2013) E-waste bans and US households’ preferences for disposing of their e-waste. J Environ Manag 124:8–16
Nixon H, Saphores J (2007) Financing electronic waste recycling Californian households’ willingness to pay advanced recycling fees. J Environ Manag 84(4):547–559
Ananno A, Masud M, Dabnichki P, Mahjabeen M, Chowdhury S (2021) Survey and analysis of consumers’ behaviour for electronic waste management in Bangladesh. J Environ Manag 282:111943
Saphores JDM, Ogunseitan OA, Shapiro AA (2012) Willingness to engage in a pro-environmental behavior: an analysis of e-waste recycling based on a national survey of USA households. Resour Conserv Recycl 60:49–63
NCIRC (Novel Coronavirus Infection Response Coordination Center) (2020) Anti-epidemic specialty. Available at https://www.ssm.gov.mo/apps1/PreventCOVID-19/ch.aspx#clg17046. Accessed 25 Feb 2021
People’s Daily Online (2021) Ministry of Ecology and Environment: continue to make overall arrangements for the collection, transportation and disposal of discarded masks. Available at https://m.gmw.cn/baijia/2021-09/12/1302572266.html. Accessed 12 Sept 2021
Ramayah T, Lee JW, Lim S (2012) Sustaining the environment through recycling: an empirical study. J Environ Manag 102:141–147
DSEC (Statistics and Census Service Macao SAR Government) (2019) Macau statistical yearbook. Available at https://www.dsec.gov.mo/getAttachment/a2b8aa77-3b58-4f44-b5cf-ea003a02cc4f/C_AE_PUB_2019_Y.aspx. Accessed 20 Sept 2021
Fan B, Yang W, Shen X (2019) A comparison study of ‘motivation–intention–behavior’ model on household solid waste sorting in China and Singapore. J Clean Prod 211:442–454
Hinkin T (1998) A brief tutorial on the development of measures for use in survey questionnaires. Organ Res Method 1(1):104–121
Hair JF, Ringle CM, Sarstedt M (2014) PLS-SEM: indeed a silver bullet. J Mark Theory Pract 19(2):139–152
Steg L, Vlek C (2009) Encouraging pro-environmental behaviour: an integrative review and research agenda. J Environ Psychol 29(3):309–317
Dharmaraj S, Ashokkumar V, Hariharan S, Manibharathi A, Show PL, Chong CT, Ngamcharussrivichai C (2021) The COVID-19 pandemic face mask waste: a blooming threat to the marine environment. Chemosphere 272:129601
DSPA (Direcção dos Serviços de Protecção Ambiental) (2021) Hot topic. Available at https://www.dspa.gov.mo/index.aspx. Accessed 20 Sept 2021
Song Q, Wang Z, Li J (2013) Environmental performance of municipal solid waste strategies based on LCA method: a case study of Macau. J Clean Prod 57:92–100
Song Q, Li J, Zeng X (2015) Minimizing the increasing solid waste through zero waste strategy. J Clean Prod 104:199–210
Acknowledgements
This work was funded by the Science and Technology Development Fund, Macao SAR, China (0062/2020/A; 0024/2020/AGJ),Open Fund of Guangdong Provincial Key Laboratory of Petrochemical Pollution Process and Control, Guangdong University of Petrochemical Technology (No. 2018B030322017).
Author information
Authors and Affiliations
Contributions
KC: conceptualization, methodology, software; WZ: data curation, investigation, writing—original draft preparation; QS: writing—reviewing and editing; YL: validation, supervision; SP, JH and JL: supervision.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Cai, K., Zeng, W., Song, Q. et al. What makes residents more willing to participate in source separation of waste masks under the COVID-19 pandemic?. J Mater Cycles Waste Manag 25, 103–116 (2023). https://doi.org/10.1007/s10163-022-01513-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10163-022-01513-7