
Abstract
Background
Although left ventricular hypertrophy (LVH) has been established as a predictor of cardiovascular events in chronic kidney disease (CKD), the relationship between the prevalence of LVH and CKD stage during the predialysis period has not been fully examined.
Methods
We measured left ventricular mass index (LVMI) in a cross-sectional cohort of participants in the Chronic Kidney Disease Japan Cohort (CKD-JAC) study in order to identify factors that are associated with increased LVMI in patients with stage 3–5 CKD. LVH was defined as LVMI > 125 g/m2 in male patients and >110 g/m2 in female patients.
Results
We analyzed baseline characteristics in 1185 participants (male 63.7 %, female 36.3 %). Diabetes mellitus was the underlying disease in 41.3 % of patients, and mean age was 61.8 ± 11.1 years. LVH was detected in 21.7 % of patients at baseline. By multivariate logistic analysis, independent risk factors for LVH were past history of cardiovascular disease (odds ratio [OR] 0.574; 95 % confidence interval [CI] 0.360–0.916; P = 0.020), systolic blood pressure (OR 1.179; 95 % CI 1.021–1.360; P = 0.025), body mass index (OR 1.135; 95 % CI 1.074–1.200; P < 0.001), and serum calcium level (OR 0.589; 95 % CI 0.396–0.876; P = 0.009).
Conclusion
Cross-sectional baseline data from the CKD-JAC study shed light on the association between LVH and risk factors in patients with decreased renal function. Further longitudinal analyses of the CKD-JAC cohort are needed to evaluate the prognostic value of LVH in CKD patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) is the leading risk factor for cardiovascular disease (CVD), a great threat to health and an economic burden [1]. In Japan, the prevalence of end-stage kidney disease (ESKD) requiring renal replacement therapy has been increasing over the last three decades. There were 38,893 new cases in 2010, bringing the total number of cases in Japan to 304,592 [2]. Since the number of patients requiring dialysis has continued to increase [3], there appear to be an enormous number of latent cases of CKD in the Japanese population. In a recent study, Imai et al. reported the prevalence of CKD by calculating the estimated glomerular filtration rate (eGFR) using an equation that estimates GFR based on data from the Japanese annual health check program in 2005 [4]. They predicted that 13 % of the Japanese adult population (approximately 13.3 million people) would have CKD in 2005. CKD frequently progresses and becomes severe over time, but the factors that are responsible for the progression of CKD need further elucidation [5].
Renal dysfunction and albuminuria in CKD patients have been established as a risk factor for cardiovascular (CV) events independent of conventional CV risk factors [6–8]. Population-based studies in Western and Asian countries have shown that the risk of CVD increases as renal function declines. Because of this finding, the National Kidney Foundation formed a task force to heighten awareness of CVD in CKD, and defined CKD using parameters such as decreased eGFR < 60 ml/min/1.73 m2. A cohort of CKD patients treated by nephrologists is required to accurately analyze renal and CV events. However, few studies have been conducted on the prevalence of left ventricular hypertrophy (LVH) in a predialysis population [9–12].
The aim of the present study was to clarify whether there is a close correlation between the prevalence of LVH and the stage of CKD classified according to eGFR and to identify factors related to LVH among the participants in the Chronic Kidney Disease Japan Cohort (CKD-JAC) [13].
Subjects and methods
Inclusion and exclusion criteria
Baseline characteristics of CKD-JAC are described elsewhere [14]. The following inclusion criteria were used at screening: (1) Japanese or Asian patients living in Japan; (2) age 20–75 years; and (3) a broad spectrum of CKD with eGFR of 10–59 ml/min/1.73 m2. eGFR was calculated using a modified three-variable equation for eGFR in Japanese patients [15]: eGFR = 194 × age−0.287 × sCr−1.094 (×0.739, if female), where sCr = serum creatinine.
All patients were classified on the basis of CKD stage as described in our previous paper [13]. The following patients were excluded from participation: (1) patients with polycystic kidney disease, human immunodeficiency virus (HIV) infection, liver cirrhosis, active cancer, and patients who had received cancer treatment within the past 2 years; (2) transplant recipients and patients who had previously been on long-term dialysis; (3) patients who refused to provide informed consent.
Information on past medical history, including hypertension, acute myocardial infarction, angina pectoris, congestive heart failure, peripheral arterial disease, cerebrovascular disease, and prescription of antihypertensive agents, including angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), diuretics, and β-blockers, statins, and antiplatelet agents, was collected from the medical records at each institution.
Blood pressure and echocardiographic measurements
Blood pressure (BP) was measured in outpatient clinics with an automated sphygmomanometer after a 5-min rest. BP in the right arm was measured three times at intervals of 1 min, and the mean values were used for analyses. A mercury sphygmomanometer was used to measure the BP of patients who had frequent premature contractions, atrial fibrillation, or atrial flutter. Pulse pressure was calculated by subtracting diastolic BP from systolic BP. A 2-dimensional guided M-mode echocardiographic study was performed at each institution. Measurements included the diastolic thickness of the interventricular septum (IVST) and left ventricular posterior wall (PWT), and the internal diameter of the left ventricle at the end of diastole (LVDd) and the end of systole (LVDs). The modified Penn cube formula was used to calculate LV mass [16]: ([1.04 × (0.1 × IVST) + (0.1 × PWT)] × 3 − [(0.1 × LVDd) × 3] × 8 + 0.6, and LV mass was adjusted for body surface area (LVMI). LVH was defined as LVMI > 125 g/m2 in men and >110 g/m2 in women [17].
Definitions of hypertension, diabetes and dyslipidemia
Hypertension was defined as systolic BP ≥ 140 mmHg and/or diastolic BP ≥ 90 mmHg or taking an antihypertensive agent. Diabetes mellitus (DM) was defined as HbA1C ≥ 6.5 % or taking an antidiabetic agent. Diabetic patients were identified as those with diabetic nephropathy as the primary cause of CKD. Dyslipidemia was defined as serum triglyceride level >150 mg/dl, or serum high-density lipoprotein (HDL) cholesterol level <40 mg/dl in men and <50 mg/dl in women.
Collection of biological samples and measurements
Whole blood, serum, and urine samples were collected for measurement of serum Cr and cystatin C, HbA1c, intact parathyroid hormone (iPTH), and urinary albumin and Cr levels at a central laboratory. Urinary albumin excretion was expressed as the albumin to Cr ratio (ACR). HbA1c was measured by the JDS method, and the value was converted to the A1C value measured by the NGSP method by adding 0.4 % as determined by the Japanese Diabetes Society. Each clinical center measured serum Cr at each visit. A 24-h urine specimen was collected from each patient once a year to measure the amount of proteinuria.
Statistical analysis
All variables are reported as mean ± SD and frequency. Descriptive statistics of baseline characteristics were calculated by CKD stage, sex, and the presence or absence of LVH. CKD stages were defined according to the patient’s eGFR. Chi-squared test and Student’s t test or one way analysis of variance (ANOVA) were used to detect between-group differences. ACR values had a skewed distribution, and were log-transformed to achieve a normal distribution. Logistic linear regression was used to investigate the relation of LVMI to eGFR, BMI, and log ACR. Univariate logistic regression analyses were performed in an attempt to identify factors related to LVH. Multivariate logistic regression analyses were used to identify independent variables related to LVH. We considered some variables that had a P value <0.10 in univariate logistic regression analyses as independent variables for multivariate logistic regression analyses. The model included the variables as follows: sex, smoking status, complications of DM, dyslipidemia and hypertension, past history of congestive heart failure, systolic and diastolic BPs, pulse pressure, BMI, eGFR, uric acid, ACR, A1C, iPTH, HDL cholesterol, triglyceride, calcium, phosphorus, and prescription of antihypertensive agents. The two-sided 95 % confidence interval (CI) and odds ratio (OR) were calculated by estimation. A two-sided probability level of 5 % was considered significant. All statistical analyses were performed using the SAS software program for Windows (SAS Inc. Japan, Tokyo, Japan).
Results
Baseline demographics and clinical characteristics of participants according to eGFR level
The baseline characteristics of the 2977 participants in the CKD-JAC study have been described previously [13]. Of them, the subjects in this study, i.e., those who were examined by echocardiography (UCG), consisted of 755 Japanese men (63.7 %) and 430 Japanese women (36.3 %), 489 (41.3 %) and 918 (77.5 %) of whom had DM and dyslipidemia, respectively. Most of the subjects had hypertension (1051, 88.7 %) and were being treated with an antihypertensive agent (1095, 92.4 %), most of them (83.1 %) with ACE inhibitors (302, 25.5 %)/ARBs (901, 76.0 %), as shown in Table 1.
CKD was stage 3a in 136 patients (11.5 %), stage 3b in 383 patients (32.3 %), stage 4 in 464 patients (39.2 %), and stage 5 in 202 patients (17.0 %) (Table 1). The prevalence of CVD comorbidity tended to be inversely proportional to eGFR, but the correlation did not reach statistical significance. The groups with stage 4–5 CKD were older, and had higher systolic BP and pulse pressure, a higher prevalence of hyperuricemia and anemia, and higher grades of proteinuria and albuminuria than the groups with stage 3a and 3b CKD, and serum levels of phosphorus, and iPTH in stage 4 and 5 CKD patients were significantly higher than those in stage 3a and 3b CKD patients. Antihypertensive agents, including ACE inhibitors and CCBs, statins, and antiplatelet agents were frequently administered in the groups of patients with stage 3b and 4 CKD.
Analysis by sex
Since the proportion of male subjects was 63.7 % in the study population, sex may have affected the results of the present study. As shown in Table 2, female subjects were younger (60.8 ± 11.7 vs. 62.4 ± 10.7 years, P = 0.0160), and had a lower prevalence of hypertension (84.9 vs. 90.9 %, P = 0.0018), DM (36.7 vs. 43.8 %, P = 0.0170), and past history of myocardial infarction (1.9 vs. 9.5 %, P < 0.0001) and stroke (8.4 vs. 14.7 %, P = 0.0015) than male subjects. In addition, female subjects had lower BMI (23.2 ± 4.1 vs. 23.9 ± 3.5 kg/m2, P = 0.0016), lower serum levels of Cr (1.84 ± 0.90 vs. 2.38 ± 1.13 mg/dl, P < 0.0001) and uric acid (6.90 ± 1.51 vs. 7.38 ± 1.49 mg/dl, P < 0.0001), and lower hemoglobin concentration (11.53 ± 1.54 vs. 12.49 ± 1.91 g/dl, P < 0.0001) than male subjects. However, there was no significant sex difference in eGFR (28.61 ± 13.00 vs. 28.61 ± 12.43 ml/min/1.73 m2, P = 0.9986). Female subjects had higher serum levels of lipids, including total cholesterol (207.6 ± 45.3 vs. 186.6 ± 40.7 mg/dl, P < 0.0001), non-HDL cholesterol (147.9 ± 44.3 vs. 136.6 ± 40.3 mg/dl, P < 0.0001), low-density lipoprotein (LDL) cholesterol (118.1 ± 35.2 vs. 106.3 ± 32.9 mg/dl, P < 0.000), and HDL cholesterol (60.8 ± 19.3 vs. 50.0 ± 16.4 mg/dl, P < 0.0001), and lower serum triglyceride level (160.5 ± 106.0 vs. 175.8 ± 119.8 mg/dl, P = 0.0358). Lower percentages of female subjects were prescribed antihypertensive agents, including CCBs and β-blockers, statins and antiplatelet agents. As shown in Table 5, menopause was not significantly associated with LVMI (OR 1.269; 95 % CI 0.858–1.877; P = 0.233) by univariate logistic regression analyses.
Comparison of study population with and without LVH according to CKD stage and sex
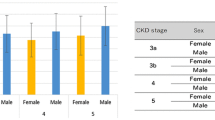
LVMI in each of the four groups of CKD patients according to eGFR is shown in Fig. 1, and tended to increase with the stage of CKD (P = 0.0005 in men, P = 0.0016 in women). The prevalence of LVH was 257 of 1185 (21.7 %) of the study population (Table 3). Men had a higher prevalence of LVH than women (15.9 vs 5.7 %).

Comparison of left ventricular mass index (LVMI) in the different subgroups of CKD patients according to their degree of renal dysfunction
The demographic and biochemical parameters of the study population are compared in Table 4. Female subjects with LVH had a higher prevalence of DM (52.9 vs. 33.7 %, P = 0.003), higher BMI (24.5 ± 4.2 vs. 22.9 ± 4.1 kg/m2, P = 0.004), higher systolic BP (135.5 ± 19.6 vs. 130.4 ± 18.5 mmHg, P = 0.043), lower eGFR (24.4 ± 10.7 vs. 29.4 ± 13.3 ml/min/1.73 m2, P = 0.003), and higher ACR (1515.4 ± 1802.7 vs. 916.0 ± 1534.2 mg/gCr, P = 0.005) than female subjects without LVH. In addition, female subjects with LVH had lower serum calcium level (8.94 ± 0.70 vs. 9.16 ± 0.50 mg/dl, P = 0.004), and higher serum levels of phosphorus (3.95 ± 0.72 vs. 3.74 ± 0.60 mg/dl, P = 0.015) and iPTH (132.4 ± 117.0 vs. 104.9 ± 80.8 mg/dl, P = 0.019) than female subjects without LVH. Moreover, higher proportions of female subjects with LVH were being treated with ACE inhibitors (33.8 vs. 22.1 %, P = 0.036), CCBs (75.0 vs. 47.5 %, P < 0.001), β-blockers (25.0 vs. 13.3 %, P = 0.013), and diuretics (51.5 vs. 29.3 %, P = 0.001).
On the other hand, higher proportions of male subjects with LVH had hypertension (97.4 vs. 88.7 %, P = 0.001) and DM (50.3 vs. 41.7 %, P = 0.04), and lower proportions had a past history of angina (6.3 vs. 11.7 %, P = 0.038) and stroke (6.9 vs. 12.0 %, P = 0.048). The group of male subjects with LVH had higher BMI (25.5 ± 3.6 vs. 23.4 ± 3.3 kg/m2, P < 0.001), higher systolic BP (138.4 ± 19.2 vs. 131.3 ± 16.8 mmHg, P < 0.001), higher pulse pressure (60.3 ± 15.4 vs. 55.4 ± 12.9 mmHg, P < 0.001), lower eGFR (26.8 ± 13.1 vs. 29.2 ± 12.1 ml/min/1.73 m2, P = 0.017), and higher ACR (1456.7 ± 1720.6 vs. 972.6 ± 1349.3 mg/gCr, P = 0.001) than female subjects without LVH. Among the lipid parameters, male subjects with LVH had significantly lower serum HDL cholesterol level (46.6 ± 13.3 vs. 51.2 ± 17.2 mg/dl, P = 0.002) and higher serum triglyceride level (202.4 ± 149.2 vs. 166.8 ± 106.9 mg/dl, P = 0.001) than female subjects without LVH. Parameters of mineral metabolism showed the same trends in female subjects as in male subjects with LVH. Moreover, higher proportions of male than female subjects with LVH were being treated with β-blockers (27.0 vs. 16.4 %, P = 0.002).
Factors related to LVH
Table 5 shows that the factors associated with LVH were female sex (OR 1.78; 95 % CI 1.308–2.416; P < 0.001), DM (OR 1.66; 95 % CI 1.254–2.186; P < 0.001), dyslipidemia (OR 1.43; 95 % CI 1.007–2.040; P = 0.045), and hypertension (OR 3.73; 95 % CI 1.487–9.376; P = 0.005). Significant clinical factors associated with LVH were systolic BP (OR 1.23; 95 % CI 1.134–1.323; P < 0.001), diastolic BP (OR 1.16; 95 % CI 1.031–1.306; P = 0.014), pulse pressure (OR 1.25; 95 % CI 1.137–1.380; P < 0.001), eGFR (OR 0.98; 95 % CI 0.968–0.9991; P = 0.0004; Fig. 2a, b), BMI (OR 1.15; 95 % CI 1.110–1.199; P < 0.0001; Fig. 3a, b), serum uric acid (OR 1.10; 95 % CI 1.002–1.202; P = 0.046), ACR (OR 1.55; 95 % CI 1.267–1.905; P < 0.001), A1C (OR 1.17; 95 % CI 1.011–1.345; P = 0.035), serum levels of iPTH (OR 1.00; 95 % CI 1.001–1.005; P < 0.001), HDL cholesterol (OR 0.98; 95 % CI 0.971–0.989; P < 0.001), triglyceride (OR 1.00; 95 % CI 1.001–1.003; P < 0.001), calcium (OR 0.56; 95 % CI 0.431–0.720; P < 0.001) and phosphorus (OR 1.23; 95 % CI 1.004–1.515; P = 0.046), and prescription of antihypertensive agents (OR 3.51; 95 % CI 1.601–7.685; P = 0.002).

Relationship between estimated glomerular filtration rate (eGFR) and left ventricular mass index (LVMI) of patients with stage 3–5 CKD. a female; b male

Relationship between body mass index (BMI) and left ventricular mass index (LVMI) of patients with stage 3–5 CKD. a Female; b male
As shown in Table 6, the variables independently associated with LVH were past history of CVD (OR 0.574; 95 % CI 0.360–0.916; P = 0.020), systolic BP (OR 1.179; 95 % CI 1.021–1.360; P = 0.025), BMI (OR 1.135; 95 % CI 1.074–1.200; P < 0.001), and serum calcium level (OR 0.595; 95 % CI 0.404–0.876; P = 0.009) by multivariate logistic regression analysis.
As shown in Table 7, the variables independently associated with LVH in diabetic patients were BMI (OR 1.110; 95 % CI 1.023–1.203; P = 0.012), serum triglyceride level (OR 1.002; 95 % CI 1.000–1.005; P = 0.043), and serum calcium level (OR 0.461; 95 % CI 0.273–0.777; P = 0.004) by multivariate logistic regression analysis.
As shown in Table 8, the variables independently associated with LVH in non-diabetic patients were male gender (OR 2.453; 95 % CI 1.241–4.849; P = 0.010), systolic BP (OR 1.355; 95 % CI 1.076–1.707; P = 0.010), and BMI (OR 1.156; 95 % CI 1.063–1.257; P = 0.001) by multivariate logistic regression analysis.
Discussion
In the present cross-sectional study, we enrolled 2977 representative Japanese outpatients, most of whom had stage 3–5 CKD. These 2977 outpatients were being treated by nephrologists and were receiving a good standard of care. UCG was performed in 1185 of them. The UCG carried out was not intended to evaluate selected patients with cardiac complications, but was performed consecutively for evaluation of cardiac function in representative participants in the CKD-JAC study, if they provided informed consent. The prevalence of LVH in the present study was much lower than that reported in previous studies in the general population. The participants in the CKD-JAC study may be better treated by nephrologists. Alternatively, cardiologists could treat more severe cases. The majority of the study subjects had hypertension and proteinuria or albuminuria on enrollment, but systolic and diastolic BP were normal (132/76 mmHg). More than 90 % of the subjects were being treated with antihypertensive agents (n = 1095, 92.4 %), including ACE inhibitors (n = 302, 25.5 %) and/or ARBs (n = 901, 76.0 %). The prevalence rates of pre-existing CVD, i.e., congestive heart failure (5.7 %), myocardial infarction (6.8 %), and stroke (12.4 %), were higher than in the general Japanese population [18]. DM was present in 41.3 % of the study subjects, and more than one-third of enrolled subjects had CKD secondary to glomerulonephritis.
The results of the present study provided information on the prevalence of LVH and factors associated with LVH in stage 3–5 CKD patients in the CKD-JAC study. In the CKD-JAC study, LVH was observed in a small population (21.7 %) of the 1185 study subjects, whereas LVMI tended to increase with the progression of CKD. CKD patients have a high prevalence of LVH, ranging from 34 to 74 % in different studies, and its prevalence increases as renal function declines [10, 12, 19, 20]. However, the relatively wide heterogeneity of the prevalence of LVH in different studies can be attributed to several differences in the characteristics of the populations studied, including differences in ethnicity, age, proportion of subjects with different stages of CKD, prevalence of hypertension, method chosen to evaluate GFR, cut-off GFR used to enroll patients, and definition of LVH.
Elevated systolic BP has a continuous, graded, and independent association with risk of coronary heart disease, stroke, and ESKD [21]. LVH might be a beneficial compensatory process in CKD patients, allowing the left ventricle to produce additional force to increase cardiac work and maintain constant wall tension [22]. Even though mean systolic BP was well controlled (132.4 ± 18.1 mmHg), systolic BP was higher in patients with LVH than in patients without LVH in the present study. According to multivariate logistic regression analysis, systolic BP was an independent variable associated with LVH. Recently, it was reported that systolic arterial hypertension and elevated pulse pressure are closely associated with LVH in pre-dialysis patients, suggesting that fluid overload and increased arterial stiffness play important roles in LVH before starting dialysis therapy [12]. Fluid volume management and maintenance of a near euvolemic state are crucial for the amelioration of LVH [23].
After adjusting for several potential confounders, multivariate logistic regression analyses showed that the presence of a previous CVD was significantly associated with LVH. The potential explanations for how the CKD state can accelerate atherosclerosis and cause CVD have been of considerable interest in clinical practice. The 4 basic explanations are: (1) uncontrolled confounding, or the impact of comorbidities that occur in CKD patients, especially older age; (2) therapeutic nihilism, meaning CKD patients receive lesser degrees of cardioprotective therapies; (3) excess treatment toxicities, intolerances, or risks such that therapy cannot be used or offers a less favorable benefit-to-risk ratio; and (4) a unique vascular pathobiology that occurs in the CKD state [24]. By using the large sample size of the Kidney Early Evaluation Program (KEEP), McCullough et al. [25] demonstrated in stratified analysis that the presence of CKD in young adults was clearly related to premature CVD. These findings suggest the biological changes that occur with CKD promote CVD at an accelerated rate that cannot be fully explained by conventional risk factors or older age.
In accordance with the theory of non-hemodynamic LVH-promoting factors in our CKD patients, BMI was found to be a factor that was independently associated with LVH. Obesity is thought to be a risk factor independent of LVH, and heart disorders in obesity include structural adaptation with LVH and functional abnormalities [26]. Kotsis et al. [27] reported that obesity and daytime pulse pressure are predictors of LVH in true normotensive individuals. In hypertensive obese patients, metabolic syndrome (MetS) maintains its role as a risk factor for LVH independently of age and systolic BP and is a useful predictor of target organ damage in clinical practice [28]. However, MetS is no longer an independent risk factor when BMI is taken into account, suggesting that the effects of MetS on LVH are mainly driven by the degree of abdominal adiposity.
Currently, information about sex differences in renal abnormalities and CVD in healthy individuals is limited and conflicting. In the Prevention of Renal and Vascular End-Stage Disease (PREVEND) study, the prevalence of microalbuminuria in men was almost double that observed in women, and for a higher value of age and BMI was greater in men than in women [29]. In addition, the presence of CKD has been found to be associated with an increased risk of cardiovascular events [30] and of cardiovascular death [31] in both women and men having different degrees of cardiovascular risk or already having CVD. A recent study has shown that logistic regression analysis demonstrated that the factors significantly associated with the prevalence of LVH were age and BMI in women and uric acid in men [32]. In the present study, men were significantly associated with LVH in non-diabetic CKD patients. In our cohort, men had higher prevalence of classical cardiovascular risk factors including hypertension, past history of previous CVD, hyperuricemia, and lower HDL cholesterol, suggesting that classical cardiovascular risk factors may be associated with LVH in men with non-diabetic CKD.
Various abnormalities of mineral–bone metabolism are common in CKD patients, and mineral metabolism disorders such as hypocalcemia, hyperphosphatemia, and vitamin D deficiency have been found to be closely associated with CVD in CKD patients [33]. The mean serum calcium and phosphorus levels in the subjects of the present study were within the normal ranges, but differed between the groups with and without LVH. Serum iPTH level was elevated in patients with LVH and differed from that in the group without LVH. Hypocalcemia was associated with LVH by multivariate logistic regression analysis. Although its mechanism is not completely known, hypocalcemia followed by vitamin D deficiency may be associated with the pathogenesis of LVH. The results of the present study suggested that disorders of mineral metabolism may be involved in the etiology of LVH.
In conclusion, the results of this study showed that the prevalence of LVH was low in stage 3–5 CKD patients treated by nephrologists in Japan. The cross-sectional baseline data from the CKD-JAC study shed light on the association between LVH and risk factors in patients with decreased renal function. Differences in the presence of previous CVD, blood pressure control, and metabolic state may lead to different outcomes of CVD in a longitudinal study. Future analysis of the CKD-JAC cohort will clarify whether the incidence of LVH varies with the causative disease during further follow-up.
Change history
09 September 2017
An erratum to this article has been published.
References
National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evidence, classification, and stratification. Am J Kidney Dis. 2002;39(suppl 1):S1–266.
Japanese Society of Dialysis Therapy. An overview of regular dialysis treatment in Japan as of Dec 31, 2010. 2011. http://docs.jsdt.or.jp/overview/. Accessed 1 Aug 2012.
Imai E, Horio M, Watanabe T, Iseki K, Yamagata K, Hara S, et al. Prevalence of chronic kidney disease in the Japanese general population. Clin Exp Nephrol. 2009;13:621–30.
Imai E, Horio M, Iseki K, Yamagata K, Watanabe T, Hara S, et al. Prevalence of chronic kidney disease (CKD) in the Japanese general population predicted by the MDRD equation modified by a Japanese coefficient. Clin Exp Nephrol. 2007;11:156–63.
Yamashita T, Yoshida T, Ogawa T, Tsuchiya K, Nitta K. Clinical outcomes in patients with chronic kidney disease: a 5-year retrospective cohort study at a University Hospital in Japan. Clin Exp Nephrol. 2011;15:831–40.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–305.
Ninomiya T, Kiyohara Y, Kubo M, Tanizaki Y, Doi Y, Okubo K, et al. Chronic kidney disease and cardiovascular disease in a general Japanese population: the Hisayama Study. Kidney Int. 2005;68:228–36.
Irie F, Iso H, Sairenchi T, Fukasawa N, Yamagishi K, Ikehara S, et al. The relationships of proteinuria, serum creatinine, glomerular filtration rate with cardiovascular disease mortality in Japanese general population. Kidney Int. 2006;69:1264–71.
Levin A, Singer J, Thompson CR, Ross H, Lewis M. Prevalent left ventricular hypertrophy in predialysis population: identifying opportunities for intervention. Am J Kidney Dis. 1996;27:347–54.
Tucker B, Fabbian F, Giles M, Thuraisingham RC, Raine AE, Baker LR. Left ventricular hypertrophy and ambulatory blood pressure monitoring in chronic renal failure. Nephrol Dial Transplant. 1997;12:724–8.
McMahon LP, Roger SD, Slimheart Investigators Group. Development, prevention, and potential reversal of left ventricular hyperterophy in chronic kidney disease. J Am Soc Nephrol. 2004;15:1640–7.
Paoletti E, Bellino D, Cassottana P, Rolla D, Cannella G. Left ventricular hypertrophy in nondiabetic predialysis patients. Am J Kidney Dis. 2005;46:320–7.
Imai E, Matsuo S, Makino H, Watanabe T, Akizawa T, Nitta K, et al. Chronic Kidney Disease Japan Cohort study: baseline characteristics and factors associated with causative diseases and renal function. Clin Exp Nephrol. 2010;14:558–70.
Imai E, Matsuo S, Makino H, Watanabe T, Akizawa T, Nitta K, et al. Chronic Kidney Disease Japan Cohort (CKD-JAC) study: design and methods. Hypertens Res. 2008;3:1101–7.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Reichek N, Devereux RB. Left ventricular hypertrophy: relationship of anatomic, echocardiographic and electrocardiographic findings. Circulation. 1981;63:1391–8.
Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, Reichek N. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986;57:450–8.
Miura K, Nakagawa H, Ohashi Y, Harada A, Taguri M, Kushiro T, et al. Four blood pressure indexes and the risk of stroke and myocardial infarction in Japanese men and women: a meta-analysis of 16 cohort studies. Circulation. 2009;119:1892–8.
Levin A, Thrompson CR, Ethier J, Carisie EJ, Tobe S, Mendelssohn D, et al. Left ventricular mass index increase in early renal disease: impact of decline in hemoglobin. Am J Kidney Dis. 1999;34:125–34.
Nardi E, Palermo A, Mule G, Cusimano P, Cotton S, Cerasola G. Left ventricular hypertrophy and geometry in hypertensive patients with chronic kidney disease. J Hypertens. 2009;27:633–41.
Locatelli F, Bommer J, London GM, Martin-Malo A, Wanner C, Yaqoob M, et al. Cardiovascular disease determinants in chronic renal failure: clinical approach and treatment. Nephrol Dial Transplant. 2001;16:459–68.
London G. Pathophysiology of cardiovascular damage in the early renal population. Nephrol Dial Transplant. 2001;16(Suppl 2):3–6.
Nitta K. Pathogenesis and therapeutic implications of cardiorenal syndrome. Clin Exp Nephrol. 2011;15:187–94.
McCullough PA. Cardiovascular disease in chronic kidney disease from a cardiologist’s perspective. Curr Opin Nephrol Hypertens. 2004;13:591–600.
McCullough PA, Li S, Jurkovitz CT, Johnson B, Shlipak MG, Obialo CI, et al. Chronic kidney disease, prevalence of premature cardiovascular disease, and relationship to short-term mortality. Am Heart J. 2008;156:277–83.
Alpert MA. Obesity cardiomyopathy: pathophysiology and evolution of the clinical syndrome. Am J Med Sci. 2001;321:225–36.
Kotsis V, Stabouli S, Toumanidis S, Tsivqoulis G, Rizos Z, Trakateli C, et al. Obesity and daytime pulse pressure are predictors of left ventricular hypertrophy in true normotensive individuals. J Hypertens. 2010;28:1065–73.
Guerra F, Mancinelli L, Angelini L, Fortunati M, Rappelli A, Dessi-Fulgheri P, et al. The association of left ventricular hypertrophy with metabolic syndrome is dependent on body mass index in hypertensive overweight or obese patients. PLoS One. 2011;6:e16630.
Verhave JC, Hillege HL, Burgerhof JG, Navis G, de Zeeuw D, de Jong PE, et al. Cardiovascular risk factors are differently associated with urinary albumin excretion in men and women. J Am Soc Nephrol. 2003;14:1330–5.
Meisinger C, Doring A, KORA Study Group. Chronic kidney disease and risk of incident myocardial infarction and all-cause and cardiovascular disease mortality in middle-aged men and women from the general population. Eur Heart J. 2006;27:1245–50.
Kurth T, de Jong PE, Cook NR, Buring JE, Ridker PM. Kidney function and risk of cardiovascular disease and mortality in women: a prospective cohort study. BMJ. 2009;338:b2392.
Muiesan ML, Ambrosioni E, Costa FV, Leonetti G, Pessina AC, Salvetti M, et al. Sex differences in hypertension-related renal and cardiovascular disease in Italy: the I-DEMAND study. J Hypertens. 2012;30:2378–86.
Covic A, Kothawala P, Nernal M, Robbins S, Chalian A, Goldsmith D. Systematic review of the evidence underlying the association between mineral metabolism disturbances and risk of all-cause mortality, cardiovascular mortality and cardiovascular events in chronic kidney disease. Nephrol Dial Transplant. 2009;24:1506–23.
Acknowledgments
This study was conducted by principal investigators at the following medical centers: Yoshio Taguma; Sendai Social Insurance Hospital (Miyagi), Yoshitaka Maeda; JA Toride Medical Center (Ibaragi), Eiji Kusano; Jichi Medical University (Tochigi), Yasuhiro Komatsu; St. Luke’s International Hospital (Tokyo), Tadao Akizawa; Showa University Hospital (Tokyo), Eriko Kinugasa; Showa University Yokohama Northern Hospital (Kanagawa), Ashio Yoshimura; Showa University Fujigaoka Hospital (Kanagawa), Hiroshige Ohashi, Hiroshi Oda; Gifu Prefectural General Medical Center (Gifu), Yuzo Watanabe; Kasugai Municipal Hospital (Aichi), Daijo Inaguma, Kei Kurata; Tosei General Hospital (Aichi), Yoshitaka Isaka; Osaka University Hospital (Osaka), Yoshiharu Tsubakihara; Osaka General Medical Center (Osaka), Masahito Imanishi; Osaka City General Hospital (Osaka), Masaki Fukushima; Kurashiki Central Hospital (Okayama), Hideki Hirakata; Fukuoka Red Cross Hospital (Fukuoka), Kazuhito Takeda; Iizuka Hospital (Fukuoka).
Author information
Authors and Affiliations
Corresponding author
Additional information
For the CKD-JAC Study Group.
The editorial board has decided to retract the above-cited article entitled “Risk factors for increased left ventricular hypertrophy in patients with chronic kidney disease”, doi:10.1007/s10157-012-0758-4, because of an inadvertent but serious error.
Upon carrying out further analyses, the authors discovered that the program used in merging their data set was not working correctly, which may have made the conclusion stated in their article questionable.
An erratum to this article is available at https://doi.org/10.1007/s10157-017-1466-x.
Appendix: Contributors
Appendix: Contributors
-
1.
Steering Committee: Akira Hishida (Yaizu City Hospital), Seiichi Matsuo (Nagoya University), Tsuyoshi Watanabe (Fukushima Medical University), Yasuo Ohashi (The University of Tokyo), Hirofumi Makino (Okayama University), Tadao Akizawa (Showa University), Kosaku Nitta (Tokyo Women’s Medical University), Enyu Imai (Nagoya University)
-
2.
Data Center: Public Health Research Foundation (Tokyo)
-
3.
Independent Cardiac Function Evaluation Committee: Kyoichi Mizuno (Nippon Medical School Hospital), Hiroshi Nishimura (The University of Tokyo), Takeo Okada (Osaka Medical Center for Health Science and Promotion), Satoshi Iimuro (The University of Tokyo)
-
4.
Biostatistics Adviser: Yasuo Ohashi (The University of Tokyo)
-
5.
Medical Economics Adviser: Takashi Fukuda (The University of Tokyo)
-
6.
Nutrition Evaluation Adviser: Satoshi Sasaki (The University of Tokyo)
-
7.
International Adviser: Harold I Feldman (University of Pennsylvania)
-
8.
General Adviser: Kiyoshi Kurokawa (National Graduate Institute for Policy Study)
-
9.
Sponsor: Kyowa-Hakko-Kirin Co. Ltd.
Rights and permissions
About this article
Cite this article
Nitta, K., Iimuro, S., Imai, E. et al. RETRACTED ARTICLE: Risk factors for increased left ventricular hypertrophy in patients with chronic kidney disease. Clin Exp Nephrol 17, 730–742 (2013). https://doi.org/10.1007/s10157-012-0758-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-012-0758-4