
Abstract
Purpose
Complete mesocolic excision (CME) has been associated with improved oncological outcomes in treatment of colon cancer. However, widespread adoption is limited partly because of the technical complexity and perceived risks of the approach. The aim of out study was to evaluate the safety of CME compared to standard resection and to compare robotic versus laparoscopic approaches.
Methods
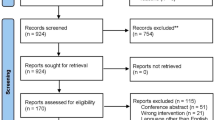
Two parallel searches were undertaken in MEDLINE, Embase and Web of Science databases 12 December 2021. The first was to evaluate IDEAL stage 3 evidence to compare complication rates as a surrogate marker of perioperative safety between CME and standard resection. The second independent search compared lymph node yield and survival outcomes between minimally invasive approaches.
Results
There were four randomized control trials (n = 1422) comparing CME to standard resection, and three studies comparing laparoscopic (n = 164) to robotic (n = 161) approaches. Compared to standard resection, CME was associated with a reduction in Clavien–Dindo grade 3 or higher complication rates (3.56% vs. 7.24%, p = 0.002), reduced blood loss (113.1 ml vs. 137.6 ml, p < 0.0001) and greater mean lymph node harvest (25.6 vs. 20.9 nodes, p = 0.001). Between the robotic and laparoscopic groups, there were no significant differences in complication rates, blood loss, lymph node yield, 5-year disease-free survival (OR 1.05, p = 0.87) and overall survival (OR 0.83, p = 0.54).
Conclusions
Our study demonstrated improved safety with CME. There was no difference in safety or survival outcomes between robotic and laparoscopic CME. The advantage of a robotic approach may lie in the reduced learning curve and an increased penetration of minimally invasive approach to CME. Further studies are required to explore this.
Prospero ID
CRD42021287065.


Similar content being viewed by others


Data availability
Data archiving is not mandated but data will be made available on reasonable request.
References
Bülow S, Harling H, Iversen LH et al (2010) Improved survival after rectal cancer in Denmark. Colorectal Dis 12:e37-42
Hohenberger W, Weber K, Matzel K et al (2009) Standardized surgery for colonic cancer: complete mesocolic excision and central ligation–technical notes and outcome. Colorectal Dis 11:354–364
Kong JC, Prabhakaran S, Choy KT et al (2021) Oncological reasons for performing a complete mesocolic excision: a systematic review and meta-analysis. ANZ J Surg 91:124–131
Wang C, Gao Z, Shen K et al (2017) Safety, quality and effect of complete mesocolic excision vs non-complete mesocolic excision in patients with colon cancer: a systemic review and meta-analysis. Colorectal Dis 19:962–972
McCulloch P, Altman DG, Campbell WB et al (2009) No surgical innovation without evaluation: the IDEAL recommendations. Lancet 374:1105–1112
De Simoni O, Barina A, Sommariva A et al (2021) Complete mesocolic excision versus conventional hemicolectomy in patients with right colon cancer: a systematic review and meta-analysis. Int J Colorectal Dis 36:881–892
Ow ZGW, Sim W, Nistala KRY et al (2021) Comparing complete mesocolic excision versus conventional colectomy for colon cancer: a systematic review and meta-analysis. Eur J Surg Oncol 47:732–737
McCulloch P, Cook JA, Altman DG et al (2013) IDEAL framework for surgical innovation 1: the idea and development stages. BMJ 346:f3012
Jayne DG, Guillou PJ, Thorpe H et al (2007) Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC trial group. J Clin Oncol 25:3061–3068
Buunen M, Veldkamp R, Hop WC et al (2009) Survival after laparoscopic surgery versus open surgery for colon cancer: long-term outcome of a randomised clinical trial. Lancet Oncol 10:44–52
Tekkis PP, Senagore AJ, Delaney CP et al (2005) Evaluation of the learning curve in laparoscopic colorectal surgery: comparison of right-sided and left-sided resections. Ann Surg 242:83–91
Ruurda JP, Draaisma WA, van Hillegersberg R et al (2005) Robot-assisted endoscopic surgery: a four-year single-center experience. Dig Surg 22:313–320
Ng KT, Tsia AKV, Chong VYL (2019) Robotic versus conventional laparoscopic surgery for colorectal cancer: a systematic review and meta-analysis with trial sequential analysis. World J Surg 43:1146–1161
Liao G, Zhao Z, Lin S et al (2014) Robotic-assisted versus laparoscopic colorectal surgery: a meta-analysis of four randomized controlled trials. World J Surg Oncol 12:122
Moher D, Shamseer L, Clarke M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4:1
Higgins JPT, Altman DG, Gøtzsche PC et al (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928
Higgins JP, Thompson SG, Deeks JJ et al (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Wan X, Wang W, Liu J et al (2014) Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 14:135
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13
Xu L, Su X, He Z et al (2021) Short-term outcomes of complete mesocolic excision versus D2 dissection in patients undergoing laparoscopic colectomy for right colon cancer (RELARC): a randomised, controlled, phase 3, superiority trial. Lancet Oncol 22:391–401
Yan D, Yang X, Duan Y et al (2020) Comparison of laparoscopic complete mesocolic excision and traditional radical operation for colon cancer in the treatment of stage III colon cancer. J BUON 25:220–226
Di Buono G, Buscemi S, Cocorullo G et al (2021) Feasibility and safety of laparoscopic complete mesocolic excision (CME) for right-sided colon cancer: short-term outcomes. A randomized clinical study. Ann Surg 274:57–62
Karachun A, Panaiotti L, Chernikovskiy I et al (2020) Short-term outcomes of a multicentre randomized clinical trial comparing D2 versus D3 lymph node dissection for colonic cancer (COLD trial). Br J Surg 107:499–508
Park JS, Kang H, Park SY et al (2019) Long-term oncologic after robotic versus laparoscopic right colectomy: a prospective randomized study. Surg Endosc 33:2975–2981
Spinoglio G, Bianchi PP, Marano A et al (2018) Robotic versus laparoscopic right colectomy with complete mesocolic excision for the treatment of colon cancer: perioperative outcomes and 5-year survival in a consecutive series of 202 patients. Ann Surg Oncol 25:3580–3586
Ceccarelli G, Costa G, Ferraro V et al (2021) Robotic or three-dimensional (3D) laparoscopy for right colectomy with complete mesocolic excision (CME) and intracorporeal anastomosis? A propensity score-matching study comparison. Surg Endosc 35:2039–2048
Park JS, Choi GS, Park SY et al (2012) Randomized clinical trial of robot-assisted versus standard laparoscopic right colectomy. Br J Surg 99:1219–1226
Watanabe T, Itabashi M, Shimada Y et al (2012) Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2010 for the treatment of colorectal cancer. Int J Clin Oncol 17:1–29
Widmar M, Keskin M, Strombom P et al (2017) Lymph node yield in right colectomy for cancer: a comparison of open, laparoscopic and robotic approaches. Colorectal Dis 19:888–894
D’Annibale A, Pernazza G, Morpurgo E et al (2010) Robotic right colon resection: evaluation of first 50 consecutive cases for malignant disease. Ann Surg Oncol 17:2856–2862
Kang J, Park YA, Baik SH et al (2016) A comparison of open, laparoscopic, and robotic surgery in the treatment of right-sided colon cancer. Surg Laparosc Endosc Percutan Tech 26:497–502
Rawlings AL, Woodland JH, Vegunta RK et al (2007) Robotic versus laparoscopic colectomy. Surg Endosc 21:1701–1708
Yozgatli TK, Aytac E, Ozben V et al (2019) Robotic complete mesocolic excision versus conventional laparoscopic hemicolectomy for right-sided colon cancer. J Laparoendosc Adv Surg Tech A 29:671–676
Author information
Authors and Affiliations
Contributions
All listed authors contributed to the conception and design, acquisition of data, analysis and interpretation of data, drafting and revision of article and approval of final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest or source of funding.
Ethic approval
Not applicable.
Informed consent
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Xu, J., Mohan, H.M., Fleming, C. et al. Complete mesocolic excision versus standard resection for colon cancer: a systematic review and meta-analysis of perioperative safety and an evaluation of the use of a robotic approach. Tech Coloproctol 27, 995–1005 (2023). https://doi.org/10.1007/s10151-023-02838-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-023-02838-7