
Abstract
Background
The best surgical strategy for the management of perforated diverticulitis with generalized peritonitis of the sigmoid colon is not clearly defined. The aim of this retrospective cohort study was to evaluate the value of a damage control strategy.
Methods
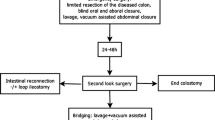
All patients who underwent emergency laparotomy for perforated diverticular disease of the sigmoid colon with generalized peritonitis between 2010 and 2015 were included. The damage control strategy (study group), included a two- stage procedure: limited resection of the diseased colonic segment, closure of proximal colon and distal stump, and application of an abdominal vacuum at the initial surgery followed by second-look laparotomy 24–48 h later At this point a choice was made between anastomosis and Hartmann’s procedure. The control group consisted of patients receiving definitive reconstruction (anastomosis or Hartmann’s procedure) at the initial operation.
Results
Thirty-seven patients were included in the study. Damage control strategy was applied in 19 patients and the control group consisted of 18 patients. Both groups were comparable in terms of demographics, severity of peritonitis, and comorbidities. The overall postoperative mortality was 11 % (n = 4). There were no statistically significant differences between both groups regarding postoperative morbidity and mortality; however, a significantly higher proportion of patients in the control group had a stoma after the initial hospital stay (83 vs. 47 %, p = 0.038). This difference was still significant after adjustment for sex, age, Mannheim Peritonitis Index, American Society of Anesthesiologists class and presence of septic shock at presentation. At the end of the follow-up period, 15 of 17 survivors in the study group and 13 of 16 survivors in the control group had their intestinal continuity restored (p = 0.66).
Conclusions
Damage control strategy in patients with generalized peritonitis due to perforated diverticulitis leads to a significantly reduced stoma rate after the initial hospital stay without an increased risk of postoperative morbidity.




Similar content being viewed by others

References
Holmer C, Kreis ME (2014) Diverticular disease—choice of surgical procedure. Chirurg 85:308–313
Aydin HN, Remzi FH, Tekkis PP, Fazio VW (2005) Hartmann’s reversal is associated with high postoperative adverse events. Dis Colon Rectum 48:2117–2126
Vermeulen J, Coene PPLO, Van Hout NM et al (2009) Restoration of bowel continuity after surgery for acute perforated diverticulitis: should Hartmann’s procedure be considered a one-stage procedure? Colorectal Dis 11:619–624
Oberkofler CE, Rickenbacher A, Raptis DA et al (2012) A multicenter randomized clinical trial of primary anastomosis or Hartmann’s procedure for perforated left colonic diverticulitis with purulent or fecal peritonitis. Ann Surg 256:819–826 (discussion 826–827)
Vermeulen J, Lange JF (2010) Treatment of perforated diverticulitis with generalized peritonitis: past, present, and future. World J Surg 34:587–593
Kafka-Ritsch R, Birkfellner F, Perathoner A et al (2012) Damage control surgery with abdominal vacuum and delayed bowel reconstruction in patients with perforated diverticulitis Hinchey III/IV. J Gastrointest Surg 16:1915–1922
Perathoner A, Klaus A, Mühlmann G, Oberwalder M, Margreiter R, Kafka-Ritsch R (2010) Damage control with abdominal vacuum therapy (VAC) to manage perforated diverticulitis with advanced generalized peritonitis—a proof of concept. Int J Colorectal Dis 25:767–774
Cirocchi R, Arezzo A, Vettoretto N et al (2014) Role of damage control surgery in the treatment of Hinchey III and IV sigmoid diverticulitis: a tailored strategy. Medicine 93:e184
Langenfeld SJ (2013) Mandatory exploration is not necessary for patients with acute diverticulitis and free intraperitoneal air. J Trauma Acute Care Surg 74:1376
Rogy M, Függer R, Schemper M, Koss G, Schulz F (1990) The value of 2 distinct prognosis scores in patients with peritonitis. The Mannheim Peritonitis Index versus the Apache II score. Chirurg 61:297–300
Függer R, Rogy M, Herbst F, Schemper M, Schulz F (1988) Validation study of the Mannheim Peritonitis Index. Chirurg 59:598–601
Demmel N, Muth G, Maag K, Osterholzer G (1994) Prognostic scores in peritonitis: the Mannheim Peritonitis Index or APACHE II? Langenbecks Arch Chir 379:347–352
Dindo D, Demartines N, Clavien P-A (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Binda GA, Karas JR, Serventi A, Study Group on Diverticulitis et al (2012) Primary anastomosis vs nonrestorative resection for perforated diverticulitis with peritonitis: a prematurely terminated randomized controlled trial. Colorectal Dis 14:1403–1410
Cirocchi R, Trastulli S, Desiderio J et al (2013) Treatment of Hinchey stage III-IV diverticulitis: a systematic review and meta-analysis. Int J Colorectal Dis 28:447–457
O’Sullivan GC, Murphy D, O’Brien MG, Ireland A (1996) Laparoscopic management of generalized peritonitis due to perforated colonic diverticula. Am J Surg 171:432–434
Myers E, Hurley M, O’Sullivan GC, Kavanagh D, Wilson I, Winter DC (2008) Laparoscopic peritoneal lavage for generalized peritonitis due to perforated diverticulitis. Br J Surg 95:97–101
Toorenvliet BR, Swank H, Schoones JW, Hamming JF, Bemelman WA (2010) Laparoscopic peritoneal lavage for perforated colonic diverticulitis: a systematic review. Colorectal Dis 12:862–867
Angenete E, Thornell A, Burcharth J et al (2014) Laparoscopic lavage is feasible and safe for the treatment of perforated diverticulitis with purulent peritonitis: the first results from the randomized controlled trial DILALA. Ann Surg 263:117–122
Swank HA, Vermeulen J, Lange JF, Dutch Diverticular Disease (3D) Collaborative Study Group et al (2010) The ladies trial: laparoscopic peritoneal lavage or resection for purulent peritonitis and Hartmann’s procedure or resection with primary anastomosis for purulent or faecal peritonitis in perforated diverticulitis (NTR2037). BMC Surg 10:29
Vennix S, Musters GD, Mulder IM, Ladies trial colloborators et al (2015) Laparoscopic peritoneal lavage or sigmoidectomy for perforated diverticulitis with purulent peritonitis: a multicentre, parallel-group, randomised, open-label trial. Lancet 386:1269–1277
Schultz JK, Yaqub S, Wallon C, SCANDIV Study Group et al (2015) Laparoscopic lavage vs primary resection for acute perforated diverticulitis: the SCANDIV randomized clinical trial. JAMA 314:1364–1375
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was conducted according to ethical standards.
Informed consent
Due to the retrospective character, informed consent was not accomplished.
Rights and permissions
About this article

Cite this article
Sohn, M., Agha, A., Heitland, W. et al. Damage control strategy for the treatment of perforated diverticulitis with generalized peritonitis. Tech Coloproctol 20, 577–583 (2016). https://doi.org/10.1007/s10151-016-1506-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-016-1506-7