
Abstract
Rheumatoid arthritis (RA) might lead to atlantoaxial instability requiring transpedicular or transarticular fusion. High-riding vertebral artery (HRVA) puts patients at risk of injuring the vessel. RA is hypothesized to increase a risk of HRVA. However, to date, no relative risk (RR) has been calculated in order to quantitatively determine a true impact of RA as its risk factor. To the best of our knowledge, this is the first attempt to do so. All major databases were scanned for cohort studies combining words “rheumatoid arthritis” and “high-riding vertebral artery” or synonyms. RA patients were qualified into the exposed group (group A), whereas non-RA subjects into the unexposed group (group B). Risk of bias was explored by means of Newcastle-Ottawa Scale. MOOSE checklist was followed to ensure correct structure. Fixed-effects model (inverse variance) was employed. Four studies with a total of 308 subjects were included in meta-analysis. One hundred twenty-five subjects were in group A; 183 subjects were in group B. Mean age in group A was 62,1 years, whereas in group B 59,9 years. The highest risk of bias regarded “comparability” domain, whereas the lowest pertained to “selection” domain. The mean relative risk of HRVA in group A (RA) as compared with group B (non-RA) was as follows: RR = 2,11 (95% CI 1,47–3,05), I2 = 15,19%, Cochrane Q = 3,54 with overall estimate significance of p < 0,001. Rheumatoid arthritis is associated with over twofold risk of developing HRVA, and therefore, vertebral arteries should be meticulously examined preoperatively before performing craniocervical fusion in every RA patient.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rheumatoid arthritis (RA) is an inflammatory autoimmune disease affecting synovial joints as well as other organs with high morbidity and increased mortality [6]. Among many skeletal regions, cervical spine is also often disturbed possibly resulting in atlantoaxial instability [19]. However, little has been written about the immediate surroundings of the vertebral artery at the level of C2 in RA patients (Fig. 1). Mainly, its anomalies are rather congenital than acquired [20]. However, recent data suggests that one of its variants, namely high-riding vertebral artery, might be more common in patients with RA [8]. High-riding vertebral artery (HRVA) is defined as internal height of C2 ≤ 2 mm and/or C2 isthmus height ≤ 5 mm measured at the level 3 mm lateral to the border of spinal canal [16]. Identification of HRVA is crucial before approaching craniocervical junction fusion, as it determines a surgical method [8]. Modality of imaging used to diagnose HRVA is usually computed tomography angiograms (CTA). The overall prevalence of HRVA in general population is 25,3% [8]. It is speculated that in RA it might be higher, approximately 42,9% [8]. The literature, though, is not unanimous, with some papers stating to the contrary [10], and relative risk (RR) has not been estimated yet. Therefore, a timely meta-analysis appears to be contributory. To the best of our knowledge, this is the first attempt in the literature to provide RR of HRVA for patients with RA. The null hypothesis is that the 95% confidence interval RR includes 1, meaning the risk is not increased for RA patients.

Sagittal section of atlantoaxial facetal joint. High-riding vertebral artery is defined as isthmus height < 5 mm or/and internal C2 height < 2 mm measured at the level 3 mm lateral to the lateral border of spinal canal. SAF, superior articular facet. IAF, inferior articular facet. VA, vertebral artery. *Internal height. **Isthmus height. Ant., anterior. Post., posterior. Sup., superior. Inf., inferior
Methods
Search strategy
Two researchers (neurosurgical resident TK & JC) scanned the following databases: PubMed MEDLINE, Web of Science, EMBASE, SciELO, and China National Knowledge Infrastructure. Search terms included “rheumatoid arthritis” AND “high-riding vertebral artery,” “high-riding vertebral groove,” “axial isthmus,” “high-riding transverse foramen,” “C2 isthmus,” “high-ride vertebral artery,” “HRVA,” “axis isthmus,” and “vertebral artery.” Time span was not restricted. The authors strictly followed MOOSE checklist (Electronic Supplementary Material 1). Titles were imported into Mendeley Desktop 1.19.4, which was also used for creation of the bibliographic data. Next, de-duplication was conducted. References of the included articles were tracked in order to identify any potentially missed papers.
Eligibility
The following inclusion criteria were imposed: (1) cohort studies with exposed and unexposed groups, (2) patients with rheumatoid arthritis as an exposed group, (3) subjects without rheumatoid arthritis as an unexposed group, (4) information on incidence of HRVA per person, and (5) Neo’s and Bloch’s definition of HRVA (internal height ≤ 2 mm and/or C2 isthmus height ≤ 5 mm measured at the level 3 mm lateral to the border of spinal canal). Of note, the above-mentioned measurements incorporated into the definition of the HRVA had to be taken in sagittal section of computed tomography (either classic or CTA). Exclusion criteria were determined as (1) groups who were operated on by means of unilateral C1-C2 transarticular fixation (in order to avoid a possible bias due to a high risk of unilateral HRVA), (2) papers with overlapping data, (3) case reports, (4) cohort studies with a total number of patients less than 10, (5) letters to the editors, (6) commentaries, (7) conference abstracts, (8) insufficient data, (9) no definition of HRVA, (10) reviews, (11) surveys, and (12) errata. English language was not a condition—articles in other languages were translated by proficient speakers of the given language and then evaluated by the authors. In order to avoid data overlap, studies of the same authors were given a particular attention so as to identify any overlapping recruitment timeline or inclusion criteria.
Data extraction
Two authors did the data extraction independently into the spreadsheet of Microsoft Excel 2016 (Redmond, USA). Pieces of information aimed to be extracted were as follows: (1) number of subjects without RA, (2) number of subjects with RA, (3) number of non-RA subjects with HRVA, (4) number of RA patients with HRVA, (5) geographical location, (6) age, and (7) sex. If an article was lacking important data, corresponding authors were communicated with.
Risk of bias assessment
Quality check and risk of bias assessment of the studies included in this meta-analysis were conducted by means of Newcastle-Ottawa Scale (NOS) as well as by evaluation of the funnel plot symmetry. Two researchers (neurosurgical resident TK & JC) assessed each of the included studies separately. In case of discrepancy, a senior neurosurgeon (LS) was called in so as to reach consensus. All articles were evaluated based on three domains: (1) selection, (2) comparability, and (3) outcome. A maximum of stars that could have been awarded for each domain was as follows: for “selection” four stars, for “comparability” two stars, and for “outcome” three stars. Lack of any stars in a given domain meant the risk of bias was high. At least one star but shy of a maximum meant the risk of bias of moderate. A maximum number of stars meant the risk of bias was low. For the sake of “outcome” domain in NOS, an adequate period of the established diagnosis of RA was arbitrarily set to at least 2 years.
Statistics
Meta-analysis was conducted by means of MetaXL 5.3, EpiGear International Pty Ltd. (Brisbane, Australia) and Statistica 13.3.0, TIBCO Software Inc. (Palo Alto, CA, USA). Relative risk (risk ratio; RR) was calculated with corresponding confidence interval of 95%. Heterogeneity was assessed based on I2 and chi2. I2 value was interpreted with general accordance: 0 to 40%, not important; 30 to 60%, moderate heterogeneity; 50 to 90%, substantial heterogeneity; and 75 to 100%, considerable heterogeneity. Level of significance for Cochrane Q p value was arbitrarily set to < 10% (< 0,10). Level of significance for p value of comparative tests was arbitrarily set to < 5% (< 0,05). For heterogeneity lower than 40%, fixed-effects model was planned. In case of heterogeneity ≥ 40%, random-effects model would be adapted.
Results
Selection process and study characteristics
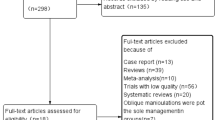
A flow diagram shows steps of the selection process (Fig. 2). Of 346 studies yielded by the initial search (344 from search engines, 2 from relevant references), 193 left once de-duplication process was completed. One hundred eighty-four records are eliminated at the level of title and abstract screening (182 from the search engines, along with 2 articles that were found through references—exclusionary reasons are shown in Fig. 2). Nine full-text articles were assessed for eligibility criteria. Finally, 4 studies were deemed eligible for meta-analysis comprising a total of 308 subjects. One hundred twenty five were in group A (the exposed arm of RA patients), whereas 183 were in group B (the unexposed arm of non-RA subjects) [4, 5, 10, 15]. One study [14] was included in qualitative, but not in quantitative synthesis due to an unacceptable risk of bias; therefore, it is addressed separately in discussion. Mean age in group A was 62,1 years, whereas in group B 59,9 years. All four studies were of Asian origin. Details are presented in Table 1.

A flow diagram depicting the study selection process
Risk of bias and quality assessment
Summary of the Newcastle-Ottawa Scale for each study included in the meta-analysis is shown in Table 2. In “selection” and “outcome” domains, all studies presented a moderate risk of bias. On the other hand, within the “comparability” domain, most of the studies presented a high risk of bias. Demonstration that outcome of interest (HRVA) was not present at the beginning of the studies was not feasible as it would have required CT scans prior to establishing diagnosis of RA. The funnel plot (Fig. 3) indicates that quantitatively only one study [10] strongly deviated from the rest, yet it had the least impact upon the mean RR.

A funnel plot illustrating quantitative assessment of the risk of bias
Estimated pooled effect
The combined relative risk estimate was RR = 2,11 (95% CI 1,47–3,05), I2 = 15,19%, Cochrane Q = 3,54, p = 0,32. Test for overall effect was significant with p < 0,001. The forest plot indicates mean distribution of RR across the studies along with the pooled effect (Fig. 4).

A forest plot of the analyzed studies indicating that rheumatoid arthritis is a risk factor for high-riding vertebral artery
Discussion
Although several papers indicated that RA might pose a risk of developing HRVA, some small studies stated to the contrary. In a small study of Lee J et al., none of three RA patients had HRVA [10]. Their study had little impact upon the overall pooled estimate, though. Studies of larger samples and lower risk of bias state that HRVA are clearly more common in RA patients. This meta-analysis confirms that, according to the current data, the relative risk is increased approximately twofold.
Presumed pathophysiology explaining the findings
Findings of this meta-analysis might be elucidated by progressive reduction of volumetric bone mineral density [18]. RA is known to induce osteoporosis in multiple ways [11]. It might be either systemic, periarticular, or focal. Thinning of the isthmus appears to combine all these three types of osteoporosis. Periarticularly, there is significant loss of trabeculae in number and in size stemming from prolonged secretion of pro-inflammatory cytokines, such as tumor-necrosis factor and interleukin 6. Systemically, disturbed osteoblastogenesis and enhanced osteoclastogenesis lead to generalized resorption of both cortical and trabecular bone. Locally, weak and demineralized bone of C2 vertebra, with transverse foramen located close to the superior articular facet, is being constantly thrusted into by the pulsating VA, over time creating a local effect of furrowing. This erodes the isthmus, rendering it insufficient in terms of screw placement. Evident cervical erosions in conventional radiographs are noticed in 16% of RA patients at 9-year follow-up [2] but much more often in CT scans [8].
Craniocervical fusion in RA patients
Rheumatoid patients’ atlantoaxial joints are prone to inflammation, subluxation, and dislocation [13, 21]. Formation of pannus around the dens of C2 as well as dens invagination into the foramen magnum might lead to craniocervical stenosis and subsequently to myelopathy of the bulbospinal junction. Many approaches are available for dens pathologies in rheumatoid arthritis including transoral release or extreme lateral [1]. Currently, treatment shifts from transoral release and posterior fusion toward solely posterior fusion, as it has been proven that craniocervical fixation leads to pannus resolution at follow-up visits [9]. As craniocervical dislocation in RA patients is often precipitated by trauma, its management shares some similarities with post-traumatic patients: for both, levels of fusion are most often C1-C2, followed by occiput-C2 [3, 7]. Precise insertion of the screws is of a paramount importance. Failure to notice a high-riding vertebral artery preoperatively at the planning stage may lead to choosing a risky method of craniocervical fusion, ultimately ending up in injuring the VA, massive blood loss, and neurological deficits. Recently, a detailed guide for clinical decision-making was provided, which facilitates choice of fusion method depending on the side of dominance of VA and whether HRVA is unilateral or bilateral [8]. In ipsilateral HRVA and dominant VA, it is recommended to either avoid transarticular/transpedicular screw or proceed only with spinal navigation.
Limitations
A small number of studies are a limitation of the present meta-analysis. One potentially contributory cohort study of Miyata et al. [14] had to be rejected from quantitative meta-analysis at the level of eligibility evaluation due to imprecise definition of HRVA, as it would have possibly introduced an unacceptable risk of bias (“the maximum screw diameter that could be inserted through the isthmus of the axis without breaching the cortex”). This peculiar definition was followed by oddly high incidence of HRVA (70,2% in RA vs 15% in non-RA); therefore, the authors of the present meta-analysis decided not to include it quantitatively but only consider it in qualitative pondering. Regional differences in HRVA definition are prominent. For instance, Paramore et al. [17] from North America named vertebral arteries high-riding if the transverse foramen was on the path of ideal transarticular screw trajectory. As useful as it might appear in day-to-day clinical practice, it is not optimal for comparative research studies due to lack of standardization. European studies are also not unanimous. Meyer et al. [12] listed 7 patients with HRVA but did not provide any definition of it, whereas Czech study of Vaněk et al. [20] adhered to the Asian definition (internal height ≤ 2 mm and/or C2 isthmus height ≤ 5 mm measured at the level 3 mm lateral to the border of spinal canal). Besides, among other limitations, all four studies coming from Asia may question validity of the results in other populations. Therefore, more studies in the future are necessary exploring relationship between rheumatoid arthritis and high-riding vertebral artery in the remaining continents. Acknowledging this issue, the authors of this meta-analysis have commenced a CT-based cohort study on HRVA of the East European population. Moreover, it is worth mentioning that 2 of the studies had relatively wide range of 95% CI, putting significant weight of the pooled RR into the other 2 studies with narrow 95% CI (Fig. 4). This weakens the findings of the meta-analysis highlighting the need for more studies. Additionally, as shown in the tabular display of NOS (Table 2), the currently available data, although the best we have now, is flawed with methodological bias, especially in terms of comparability.
Conclusion
Rheumatoid arthritis is associated with an increased risk (RR = 2,11 [95% CI 1,47–3,05]) of developing a high-riding vertebral artery. Therefore, VAs should be thoroughly examined on CT angiograms before performing craniocervical fusion in these patients. The presence of HRVA might influence choice of approach. More research studies with better methodology encompassing subjects outside Asia are needed in order to extrapolate the results.
References
Alshafai NS, Klepinowski T (2019) Extreme lateral approach to the craniovertebral junction: an update. In: Acta Neurochirurgica, Supplementum. Springer, Verlag Wien, pp 171–174. https://doi.org/10.1007/978-3-319-62515-7_25
Blom M, Creemers MCW, Kievit W, Lemmens JAM, Van Riel PLCM (2013) Long-term follow-up of the cervical spine with conventional radiographs in patients with rheumatoid arthritis. Scand J Rheumatol 42:281–288. https://doi.org/10.3109/03009742.2012.747625
Christensson D, Sáveland H, Rydholm U (2000) Cervical spine surgery in rheumatoid arthritis: a Swedish nation-wide registration of 83 patients. Scand J Rheumatol 29:314–319. https://doi.org/10.1080/030097400447705
Chung SS, Lee CS, Kim SH (2005) Analysis of the rate of high riding vertebral artery using sagittal reformatted computed tomography. J Korean Orthop Assoc 40:453. https://doi.org/10.4055/jkoa.2005.40.4.453
Higashino K, Sairyo K, Katoh S, Nakano S, Enishi T, Yasui N (2009) The effect of rheumatoid arthritis on the anatomy of the female cervical spine: a radiological study. J Bone Jt Surg - Ser B 91:1058–1063. https://doi.org/10.1302/0301-620X.91B8.22300
Kiadaliri AA, Kristensen LE, Englund M (2018) Burden of rheumatoid arthritis in the Nordic region, 1990–2015: a comparative analysis using the global burden of disease study 2015. Scand J Rheumatol 47:1–101. https://doi.org/10.1080/03009742.2017.1314002
Klepinowski T, Limanówka B, Sagan L (2020) Management of post-traumatic craniovertebral junction dislocation: a PRISMA-compliant systematic review and meta-analysis of casereports. Neurosurg Rev. https://doi.org/10.1007/s10143-020-01366-4
Klepinowski T, Pala B, Cembik J, Sagan L (2020) Prevalence of high-riding vertebral artery: a meta-analysis of the anatomical variant affecting choice of craniocervical fusion method and its outcome. World Neurosurg. https://doi.org/10.1016/j.wneu.2020.07.182
Lagares A, Arrese I, Pascual B, Gòmez PA, Ramos A, Lobato RD (2006) Pannus resolution after occipitocervical fusion in a non-rheumatoid atlanto-axial instability. Eur Spine J 15:366–369. https://doi.org/10.1007/s00586-005-0969-4
Lee JH, Jahng TA, Chung CK (2007) C1-2 transarticular screw fixation in high-riding vertebral artery: suggestion of new trajectory. J Spinal Disord Tech 20:499–504. https://doi.org/10.1097/BSD.0b013e318031af51
Lodder MC, Bakker SM, Dijkmans BAC, Kvien TK, Woolf AD, Lems WF (2000) Osteoporosis in patients with rheumatoid arthritis: tip of the iceberg? Scand J Rheumatol 29:203. https://doi.org/10.1080/030097400750002148
Meyer D, Meyer F, Kretschmer T, Börm W (2012) Translaminar screws of the axis-an alternative technique for rigid screw fixation in upper cervical spine instability. Neurosurg Rev 35:255–261. https://doi.org/10.1007/s10143-011-0358-x
Miyamoto H, Sumi M, Uno K (2013) Outcome of surgery for rheumatoid cervical spine at one institute over three decades. Spine J 13:1477–1484. https://doi.org/10.1016/j.spinee.2013.05.023
Miyata M, Neo M, Ito H, Yoshida M, Miyaki K, Fujibayashi S, Nakayama T, Nakamura T (2008) Is rheumatoid arthritis a risk factor for a high-riding vertebral artery? Spine (Phila Pa 1976) 33:2007–2011. https://doi.org/10.1097/BRS.0b013e31817c6bf7
Moon BJBJ, Choi KHKH, Shin DADA, Yi S, Kim KNKN, Yoon DHDH, Ha Y (2018) Anatomical variations of vertebral artery and C2 isthmus in atlanto-axial fusion: consecutive surgical 100 cases. J Clin Neurosci 53:147–152. https://doi.org/10.1016/j.jocn.2018.04.058
Neo M, Sakamoto T, Fujibayashi S, Nakamura T (2005) A safe screw trajectory for atlantoaxial transarticular fixation achieved using an aiming device. Spine (Phila Pa 1976) 30:E236–E242. https://doi.org/10.1097/01.brs.0000160998.53282.3f
Paramore C, Dickman C, Sonntag V (1996) The anatomical suitability of the C1-2 complex for transarticular screw fixation. J Neurosurg 85:221–224. https://doi.org/10.3171/jns.1996.85.2.0221
Perez-Edo L, Díez-Pérez A, Mariñoso L, Vallés A, Serrano S, Carbonell J (2002) Bone metabolism and histomorphometric changes in rheumatoid arthritis. Scand J Rheumatol 31:285–290. https://doi.org/10.1080/030097402760375188
Shen FH, Samartzis D, Jenis LG, An HS (2004) Rheumatoid arthritis: evaluation and surgical management of the cervical spine. Spine J 4:689–700. https://doi.org/10.1016/j.spinee.2004.05.001
Vaněk P, Bradáč O, de Lacy P, Konopková R, Lacman J, Beneš V (2017) Vertebral artery and osseous anomalies characteristic at the craniocervical junction diagnosed by CT and 3D CT angiography in normal Czech population: analysis of 511 consecutive patients. Neurosurg Rev 40:369–376. https://doi.org/10.1007/s10143-016-0784-x
Vu Nguyen H, Ludwig SC, Silber J, Gelb DE, Anderson PA, Frank L, Vaccaro AR (2004) Rheumatoid arthritis of the cervical spine. Spine J 4:329–334. https://doi.org/10.1016/j.spinee.2003.10.006
Funding
Open access funding provided by Pomeranian Medical University in Szczecin..
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
For this kind of study no ethics approval was required.
Consent to participate
As this was a retrospective analysis of the studies that had been published in the past, no consent to participate was necessary.
Consent for publication (include appropriate statements)
Authors of this study grant the Publisher the sole and exclusive license of the full copyright.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOC 71 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Klepinowski, T., Cembik, J. & Sagan, L. Risk of the high-riding variant of vertebral arteries at C2 is increased over twofold in rheumatoid arthritis: a meta-analysis. Neurosurg Rev 44, 2041–2046 (2021). https://doi.org/10.1007/s10143-020-01425-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-020-01425-w