
Abstract
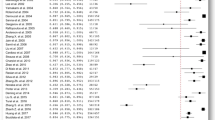
For large (≥30 mm) or giant (≥40 mm) vestibular schwannomas (VSs) for which microsurgical removal is the main treatment option, complete tumour resection and the preservation of acceptable facial nerve function can be safely and successfully achieved via the retrosigmoid approach. We performed a meta-analysis to provide a reliable estimate of functional outcome and postoperative complications for patients treated surgically for large VSs. We conducted a comprehensive search in Pubmed, Embase and the Chinese National Knowledge Infrastructure (CNKI) databases to identify publications that included only patients in whom the VSs were >3.0 cm in maximal diameter and microsurgically removed by a retrosigmoid approach. Pooled estimates of proportions with corresponding 95 % confidence intervals were calculated using the Freeman–Tukey double arcsine transformation. This meta-analysis revealed that the pooled proportion of gross total resections was 79.1 % (95 % CI, 64.2–90.8 %; I 2 = 95.4 %). By combining microsurgical techniques with continuous electrophysiological monitoring, the anatomical preservation of the facial nerve at the end of surgery was achieved in 88.8 % (95 % CI, 83.6–93.2 %; I 2 = 76.1 %) of the patients. The pooled proportion of good postoperative facial nerve function (House–Brackmann (HB) grades I–II) was 62.9 % (95 % CI, 50.0–74.9 %; I 2 = 91.1 %). Cerebrospinal fluid leakage was reported in 7.8 % (95 % CI, 4.8–11.4 %; I 2 = 49.8 %) of the patients. The mortality rate was 0.87 % (95 % CI, 0.22–1.78 %; I 2 = 4.9 %). Our meta-analysis revealed that for large VSs, very favourable results can be obtained using the retrosigmoid approach with minimal mortality, especially with respect to anatomical and functional facial nerve preservation.





Similar content being viewed by others


References
Anderson DE, Leonetti J, Wind JJ, Cribari D, Fahey K (2005) Resection of large vestibular schwannomas: facial nerve preservation in the context of surgical approach and patient-assessed outcome. J Neurosurg 102:643–649
Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50:1088–1101
Charpiot A, Tringali S, Zaouche S, Ferber-Viart C, Dubreuil C (2010) Perioperative complications after translabyrinthine removal of large or giant vestibular schwannoma: outcomes for 123 patients. Acta Otolaryngol 130:1249–1255
Chen L, Liu L, Ling F, Yuan X, Fang J, Liu Y (2009) Vestibular schwannoma microsurgery with special reference to facial nerve preservation. Clin Neurol Neurosurg 111:47–53
Darwish BS, Bird PA, Goodisson DW, Bonkowski JA, MacFarlane MR (2005) Facial nerve function and hearing preservation after retrosigmoid excision of vestibular schwannoma: Christchurch Hospital experience with 97 patients. ANZ J Surg 75:893–896
Deeks JJ (2001) Systematic reviews in health care: systematic reviews of evaluations of diagnostic and screening tests. BMJ 323:157–162
Di Maio S, Malebranche AD, Westerberg B, Akagami R (2011) Hearing preservation after microsurgical resection of large vestibular schwannomas. Neurosurgery 68:632–640, discussion 640
Freeman MF, Tukey JW (1950) Transformations related to the angular and the square root. Ann Math Stat 21:607–611
Gharabaghi A, Samii A, Koerbel A, Rosahl SK, Tatagiba M, Samii M (2007) Preservation of function in vestibular schwannoma surgery. Neurosurgery 60, ONS124-127, discussion ONS127-128
Hoffman S, Propp JM, McCarthy BJ (2006) Temporal trends in incidence of primary brain tumors in the United States, 1985–1999. Neuro Oncol 8:27–37
House JW, Brackmann DE (1985) Facial nerve grading system. Otolaryngol Head Neck Surg 93:146–147
Jain VK, Mehrotra N, Sahu RN, Behari S, Banerji D, Chhabra DK (2005) Surgery of vestibular schwannomas: an institutional experience. Neurol India 53:41–45, discussion 45
Jung S, Kang SS, Kim TS, Kim HJ, Jeong SK, Kim SC, Lee JK, Kim JH, Kim SH, Lee JH (2000) Current surgical results of retrosigmoid approach in extralarge vestibular schwannomas. Surg Neurol 53:370–377, discussion 377–378
Kobayashi M, Tsunoda A, Komatsuzaki A, Yamada I (2002) Distance from acoustic neuroma to fundus and a postoperative facial palsy. Laryngoscope 112:168–171
Lee SH, Willcox TO, Buchheit WA (2002) Current results of the surgical management of acoustic neuroma. Skull Base 12:189–195
Li JM, Yuan XR, Liu Q, Ding XP, Peng ZF (2011) Facial nerve preservation following microsurgical removal of large and huge acoustic neuroma. Zhonghua Wai Ke Za Zhi 49:240–244
Mamikoglu B, Esquivel CR, Wiet RJ (2003) Comparison of facial nerve function results after translabyrinthine and retrosigmoid approach in medium-sized tumors. Arch Otolaryngol Head Neck Surg 129:429–431
Mamikoglu B, Wiet RJ, Esquivel CR (2002) Translabyrinthine approach for the management of large and giant vestibular schwannomas. Otol Neurotol 23:224–227
Marouf R, Noudel R, Roche PH (2008) Facial nerve outcome after microsurgical resection of vestibular schwannoma. Prog Neurol Surg 21:103–107
Mehrotra N, Behari S, Pal L, Banerji D, Sahu RN, Jain VK (2008) Giant vestibular schwannomas: focusing on the differences between the solid and the cystic variants. Br J Neurosurg 22:550–556
Miller JJ (1978) The inverse of the Freeman–Tukey double arcsine transformation. Am Stat 32:138
Samii M, Gerganov VM, Samii A (2010) Functional outcome after complete surgical removal of giant vestibular schwannomas. J Neurosurg 112:860–867
Sampath P, Holliday MJ, Brem H, Niparko JK, Long DM (1997) Facial nerve injury in acoustic neuroma (vestibular schwannoma) surgery: etiology and prevention. J Neurosurg 87:60–66
Sekhar LN, Tariq F, Ferreira M (2012) Giant acoustic neuromas and their treatment. World Neurosurg 77:629–630
Seol HJ, Kim CH, Park CK, Kim DG, Chung YS, Jung HW (2006) Optimal extent of resection in vestibular schwannoma surgery: relationship to recurrence and facial nerve preservation. Neurol Med Chir (Tokyo) 46:176–180, discussion 180–181
Somers T, Offeciers FE, Schatteman I (2003) Results of 100 vestibular schwannoma operations. Acta Otorhinolaryngol Belg 57:155–166
Sterne JA, Egger M (2001) Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J Clin Epidemiol 54:1046–1055
Sterne JA, Egger M, Smith GD (2001) Systematic reviews in health care: investigating and dealing with publication and other biases in meta-analysis. BMJ 323:101–105
Sughrue ME, Yang I, Aranda D, Rutkowski MJ, Fang S, Cheung SW, Parsa AT (2011) Beyond audiofacial morbidity after vestibular schwannoma surgery. J Neurosurg 114:367–374
Sughrue ME, Yeung AH, Rutkowski MJ, Cheung SW, Parsa AT (2011) Molecular biology of familial and sporadic vestibular schwannomas: implications for novel therapeutics. J Neurosurg 114:359–366
Tos M, Stangerup SE, Caye-Thomasen P, Tos T, Thomsen J (2004) What is the real incidence of vestibular schwannoma? Arch Otolaryngol Head Neck Surg 130:216–220
Yamakami I, Uchino Y, Kobayashi E, Yamaura A, Oka N (2004) Removal of large acoustic neurinomas (vestibular schwannomas) by the retrosigmoid approach with no mortality and minimal morbidity. J Neurol Neurosurg Psychiatry 75:453–458
Zhang X, Fei Z, Chen YJ, Fu LA, Zhang JN, Liu WP, He XS, Jiang XF (2005) Facial nerve function after excision of large acoustic neuromas via the suboccipital retrosigmoid approach. J Clin Neurosci 12:405–408
Zhang X, Fei Z, Fu L (2001) Removal of large acoustic neuroma via suboccipito-retrosigmoid approach with microsurgical technique. Zhonghua Wai Ke Za Zhi 39:782–785
Zhao X, Wang Z, Ji Y, Wang C, Yu R, Ding X, Wei S (2010) Long-term facial nerve function evaluation following surgery for large acoustic neuromas via retrosigmoid transmeatal approach. Acta Neurochir (Wien) 152:1647–1652
Acknowledgments
We thank Prof. Aihua Gu and Dr. Guixiang Ji in the School of Public Health of Nanjing Medical University for statistical analysis. This work is supported by the National Natural Science Foundation of China (grant 30901534), the Jiangsu Province’s Natural Science Foundation (proj. no. BK2009444), the Grant for the 135 Key Medical Project of Jiangsu Province (no. XK201117), and the Priority Academic Program Development of Jiangsu Higher Education Institutions.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Comments
M. Samii, V. Gerganov, Hannover, Germany
Modern vestibular schwannoma (VS) surgery is safe and potentially curable. In the case of large or giant tumours, surgery is the only treatment option, and in experienced hands, it is related to very good general and functional outcome, as presented explicitly in the current meta-analysis. Excellent results can be achieved both with the retrosigmoid and the translabyrinthine approaches. The controversy over the superiority of a surgical route belongs to the history of VS surgery. The important points are that the surgeon should be most familiar with the operative technique and should have at his disposal a sufficient number of cases.
Focus of this study is the possibility to achieve a high rate of facial nerve preservation with the retrosigmoid approach. However, the main advantage of this approach, as compared to the translabyrinthine one, is that it allows for hearing preservation. From our experience as well as from published data, it is well-known that preservation of functional hearing is possible even in large and giant VS [1, 3]. Moreover, the retrosigmoid route is associated with a low rate of approach-related morbidity, such as injury to venous structures, parenchymal damage, CSF leak or postoperative headache. We were able to substantially reduce the risk of CSF leak by using pieces of subcutaneous fat tissue for sealing the opened air cells; thus, the rate in our hands is now less than 2.5 %. VS surgery is an extremely demanding procedure and requires a vast experience to achieve an optimal outcome [2]. This fact, along with numerous ethical issues, hinders the idea of multi-centre randomised trials proposed by the authors.
References
1. Di Maio S, Malebranche AD, Westerberg B, Akagami R (2010) Hearing preservation after microsurgical resection of large vestibular schwannomas. Neurosurgery 68 (3):632–640; discussion 640. doi:10.1227/NEU.0b013e31820777b1
2. Samii M, Gerganov V, Samii A (2006) Improved preservation of hearing and facial nerve function in vestibular schwannoma surgery via the retrosigmoid approach in a series of 200 patients. J Neurosurg 105 (4):527–535. doi:10.3171/jns.2006.105.4.527
3. Samii M, Gerganov VM, Samii A (2009) Functional outcome after complete surgical removal of giant vestibular schwannomas. J Neurosurg 112 (4):860–867. doi:10.3171/2009.7.JNS0989
Rights and permissions
About this article
Cite this article
Zou, P., Zhao, L., Chen, P. et al. Functional outcome and postoperative complications after the microsurgical removal of large vestibular schwannomas via the retrosigmoid approach: a meta-analysis. Neurosurg Rev 37, 15–21 (2014). https://doi.org/10.1007/s10143-013-0485-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-013-0485-7