
Abstract
Recent studies investigating pituitary function after non-sellar brain tumor surgery showed that up to 38.2% of patients have pituitary insufficiency (PI). It has been assumed that the operation causes the PI, but preoperative hormone testing, which would have been necessary to prove this assumption, was not performed. The objective of this study is to answer the question if indeed microsurgery is the culprit of PI in patients with operatively treated non-sellar brain tumors. In this prospective trial, 54 patients with supratentorial non-sellar tumors were included. The basal levels of cortisol, prolactin, testosterone, estrogen, IGF-1, fT3, fT4, STH, TSH, ACTH, FSH, and LH were recorded preoperatively on days 1 and 7 after surgery. If basal hormone screening revealed an abnormality, a releasing hormone assay was performed. Before surgery, 24 of the 54 patients (44.4%) already had PI. Additional 25 patients showed either hypocortisolism or hypothyreoidism. As those patients had been pre-treated with dexamethasone and l-thyroxine, these findings were considered not to represent PI but drug effects. Hormone testing on days 1 and 7 after surgery revealed no changes. With 44.4% PI is a frequent finding in brain tumor patients already before surgery. The factors causing preoperative PI remain yet to be identified. The endocrine results after surgery are unchanged which rules out that surgery is the cause of PI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pituitary insufficiency (PI) is a well-known sequel of the surgical management of intra- and parasellar tumors [1–13]. Surprisingly, PI also has been described in 38.2% to 43.2% of the patients who underwent surgery for gliomas, meningiomas, and neurinomas in distance to the sellar region [5, 14, 15]. Those deficits have been proposed to be a result of the surgical intervention. The authors assumed that brain damage at the tumor site and brain damage on the way to the tumor causes PI [15]. However, the assumption of surgery-related PI has to be questioned, because hormone testing was only done after surgery, which precludes the identification of PI-inducing factors not related to surgery and possibly already existing preoperatively. Apart of this, damage of healthy brain is not common in tumor surgery today, especially when dealing with extraaxial tumors. To finally answer the question if PI in brain tumor patients is caused indeed by surgery, we performed a prospective clinical trial in which the hormone status was tested before and twice after surgery. As it is known from the studies of PI after brain trauma and aneurysmal subarachnoid hemorrhage that reduced quality of life (QoL) could be a subtle indicator of PI, SF-36 testing was additionally performed [6, 8, 12, 16–21].
Material and methods
Study design
This prospective study protocol was approved by the medical ethic committee of the University of Giessen and Marburg GmbH. Fifty-four patients were enrolled in this prospective clinical study. An informed consent was obtained from all patients to participate. Exclusion criteria consisted of the following: (1) age <18 years; (2) cognitive or speech problems; (3) missing legal competence; (4) pituitary adenomas, craniopharyngeomas, and tumors close to or infiltrating into hypothalamus and hypophyseal stalk; and (5) infratentorial tumors.
Patients (Table 1)
The study comprised 54 patients (28 men, 26 women, median age 56.8 years) with supratentorial intra- and extraaxial tumors undergoing microsurgery. There were 29 patients (53.7%) with malignant glioma (WHO grades III and IV), three (5.6%) with low-grade glioma (WHO grade II), 15 (27.8%) with meningioma, four (7.4%) with metastases, two (3.7%) with non-Hodgkin’s lymphoma, and one patient (1.9%) with ganglioglioma. In seven patients, a recurrent tumor was treated.
Preoperative medication, pretreatment
The following drugs with potential effect on pituitary function or the patient’s cognitive status were taken by the patients prior to surgery: dexamethasone in 33 (61.1%), thyroxine in 11 (20.4%), antiepileptic medication (valproic acid, carbamazepine, and lamotrigine) in 12 (22.2%), neuroleptic medication in three (5.6%), antidepressants in four (7.4%), benzodiazepines in three (5.6%), l-dopamine in one (1.9%), and anti-diabetic medication (insulin or glibenclamide) in five (9.3%) cases. In 21 patients, more than one drug was given. Nine patients were admitted without any pre-medication.
Five patients underwent prior combined radio-chemotherapy, two patients underwent radiation, and one patient underwent chemotherapy only. One patient was treated with combined radio-chemotherapy for acute lymphatic leukemia during childhood.
Endocrine evaluation
Venous blood samples (10 ml) drawn in a lithium-heparinized syringe and EDTA syringe, between 8 and 10 a.m., were analysed for basal hormone concentrations. We determined the basal concentrations of cortisol, insulin-like growth factor 1 (IGF-1), prolactin (PRL), testosterone, estrogen, free thyroxine (fT3, fT4), follicle-stimulating hormone (FSH), leuteinizing hormone (LH), thyroid-stimulating hormone (TSH), adrenocorticotropic hormone (ACTH), and growth hormone (GH). Patients who had an abnormal basal hormonal value underwent a stimulation test.
Pituitary stimulation tests were conducted in a standard manner using releasing hormones in the following order: 100 μg growth hormone-releasing hormone (GHRH), 100 μg luteinizing hormone-releasing hormone, 100 μg corticotropin-releasing hormone (CRH), and 200 μg thyrotropin-releasing hormone. Blood samples were drawn at 0, 15, 30, 60, and 90 min after injection through a permanent venous catheter. Further blood samples (basal hormone concentrations) were drawn on the first and seventh postoperative day.
Normal reference values were: prolactin 60–525 μLU/ml for women and 20–350 μLU/ml for men, testosterone 300–1,000 ng/dL, estrogen for women aged 14–55 years 18–571 pg/ml, estrogen for women older than 55 years 7–44 pg/ml, fT3 2.2–4.5 pg/ml, fT4 0.8–1.8 ng/dL, age-adjusted IGF-1 55–483 ng/ml, cortisol 5–20 μg/dL, luteinizing hormone in the follicular phase 2–13 mU/ml, midcycle peak 15–79 mU/ml, luteal phase 1–19 mU/ml and postmenopausal 11–61 mU/ml, FSH in the follicular phase 3–12 mU/ml, midcycle peak 8–23 mU/ml, luteal phase 2–12 mU/ml and postmenopausal 36–157 mU/ml, ACTH 18–55 pg/ml, growth hormone <6 ng/ml, and TSH 0.4–4.0 mU/L.
Definition of hormonal impairment
Secondary hypothyroidism was defined as low fT4 or fT3 concentrations with normal or low normal TSH levels. Secondary hypogonadism was defined as low testosterone or estrogen levels with low or normal FSH or LH levels. Primary hypogonadism was diagnosed if gonadotropins were elevated with low testosterone levels in men and amenorrhea in premenopausal women. Postmenopausal women could not be evaluated in this regard. Pituitary GH deficiency was defined as low IGF-1 and STH combined with an insufficient GHRH stimulation test. Secondary adrenal insufficiency was diagnosed if patients presented with low morning cortisol concentrations and insufficient stimulation to CRH. Patients pre-treated with dexamethasone were excluded.
Evaluation of cranial magnetic resonance imaging scans
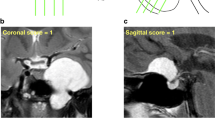
The preoperative magnetic resonance imaging (MRI) scans were evaluated for the localization of the lesion, corresponding lesion size (in cubic centimeters), potential midline shift (in millimeters), and the minimal distance between the tumor and the pituitary stalk.
Quality of life assessment
The SF-36 health questionnaire was used to evaluate the patient’s QoL. The transformed scores were used for further analysis.
Statistical analysis
All statistical tests were performed using Statistica 8 (Statsoft, Hamburg, Germany). Univariate analyses were performed with Student’s t test for continuous parameters and the chi-square test for categorical parameters. A p value < 0.05 was considered significant.
Results
Preoperative pituitary function
Before surgery, 24 of the 54 patients (44.4%) showed PI. Twenty of the 24 patients with PI had a deficiency in one (secondary hypogonadism in 13, secondary hypothyroidism in six, and growth hormone deficiency in one patient) and four in two pituitary axes (hypothyroidism and secondary hypogonadism in two patients, secondary hypogonadism and growth hormone deficiency and secondary hypogonadism and secondary adrenal insufficiency in one patient each). In addition to the 17 patients with secondary hypogonadism, five patients had primary hypogonadism with either increased levels of both FSH and LH (n = 1) or increased levels of FSH or LH (n = 2 each). The median age of the patients with primary hypogonadism was 62.8 years and that of patients with secondary hypogonadism was 56.6 years. Six patients were diagnosed with primary hyperthyroidism, three with hypercortisolism, four with excessive release of either FSH, LH, or both. Two patients showed an increased ACTH level and eight patients an increased IGF-1.
Another four patients had secondary hypothyroidism, and two patients revealed increased levels of fT3 or fT4. However, these patients were pre-treated with l-thyroxine. Hypocortisolism was found in 19 patients, which were pre-treated with dexamethasone. Therefore, these endocrine findings were considered not to be related to PI but to drug intake. All patients who received prior chemotherapy, radiotherapy, or combined treatment showed normal basal hormonal screening.
Eleven patients (45.8%) underwent pituitary stimulation test due to abnormal basal hormone levels. The remaining patients refused stimulation. Stimulation test did not detect new insufficiencies. Increased levels of PRL, LH, FSH, cortisol, and TSH in 7, 7, 1, 1, and 6 cases, respectively, were found.
Postoperative pituitary function
Regarding the blood samples drawn on the first and seventh postoperative day, we did not find any abnormalities that differed from the preoperative laboratory analyses (Table 2).
Pituitary function and neuroradiological findings
In patients with PI, a frontal tumor location was seen in eight, fronto-parietal in one, temporal in seven, parietal in three, parieto-occipital in two patients, and occipital, intraventricular, and an intraorbital location in one patient each. In patients without PI, a frontal location was found in seven, fronto-parietal in four, temporal in seven, temporo-occipital in two, parietal in three, parieto-occipital in two, and at the sphenoid wing in two patients. In one patient each, the tumor location was found in the basal ganglia, falcine, and at the tentorium. In patients with PI, the predominant tumor location was frontal. The finding did not reach statistical significance since 12 patients without PI also presented with tumors located predominantly in the frontal lobe (p = 0.925). Median tumor size was 30.1 mm3 (range, 0.4–130.7 mm3). Dichotomizing tumor volume into less and more than 30.1 mm3, no statistical significant relation between tumor volume and PI (sensitivity, 0.52; specificity, 0.32; p = 0.394) could be seen. Midline shift was found in 19 cases with a median shift of 5.8 mm (range, 2.2–7.8 mm). The midline shift was shown in 12 patients with PI and seven patients without PI. Statistical analysis did not reveal significance (p = 0.153) regarding the correlation of PI and midline shift with a sensitivity of 0.48 and a specificity of 0.29. The median distance between the tumor and the pituitary stalk was 63.1 mm (range, 26.4–90.0 mm). Dichotomizing into a distance of less and more than 63.1 mm, no significant correlation between tumor or pituitary stalk distance and PI (p = 0.210; sensitivity, 0.61; specificity, 0.61) could be seen.
Pituitary function and QoLs
According to the standardized transformed scales of the SF-36 mean values (in percentage) regarding emotional role, physical role, body pain, vitality, social function, physical function, general health, and mental health were 27.4%, 27.3%, 60.6%, 43.0%, 59.8%, 47.9%, 46%, and 53.3%, respectively. The results demonstrate that the emotional and physical roles as well as vitality are the values that are being most affected in brain tumor patients.
As demonstrated in Table 3, patients without PI had higher mean values according to the SF-36 test results, but only in the subgroup “physical functioning” a statistically significant difference could be found (p = 0.01). Neuropsychological complaints were primarily associated with glioblastoma multiforme (GBM), which did not reach statistical significance.
Discussion
PI after aneurysmal subarachnoid hemorrhage and brain trauma
Pituitary function is well investigated in patients after aneurysmal subarachnoid hemorrhage and brain trauma, and PI is a frequent finding. The majority of these patients suffer from GH deficiency. The attempt was made to explain the cause of the endocrine dysfunction. As in non-survivors, necrosis, infarction, and bleedings were often seen in the hypothalamus and the pituitary gland, PI in the survivors was believed to be related to similar but less severe lesions. Furthermore, neurosurgical clipping was attributed to contribute to PI at least in aneurysms of the anterior circulation [22, 23].
PI and brain surgery—previous studies
De Marinis et al. showed that 16 of 37 patients (43.2%) who underwent neurosurgical intervention for benign tumors, not involving the hypothalamic–pituitary region, also had PI [5]. These data have been confirmed by Schneider and co-workers who examined the endocrine function in 68 patients with non-pituitary intracranial tumors, among which had been benign and non-benign intraaxial tumors, even in the posterior fossa. 38.2% of the patients had PI after the neurosurgical intervention in combination with radiotherapy, chemotherapy, or both treatments [15]. Another 20% suffered from peripheral endocrine alterations. In both studies, secondary hypogonadism was the most common finding of PI. Second most common finding was GH deficiency. The fact that PI was more common in patients who underwent neurosurgical treatment only than in those with additional other treatments leads to the assumption that the neurosurgical procedure plays a major role in the development of PI [15]. It was believed that surgical trauma at the tumor site and on the way to the tumor causes PI. Other potential factors of PI, which had been considered by the authors, were tumor infiltration of and metastases in the hypothalamic–hypophyseal area.
Unfortunately, both studies have substantial flaws. First, hormonal testing was only performed after the operation. Thus, the conclusion that surgery is the culprit of the diagnosed PI cannot be drawn. Second, damage to normal brain is rare in extraaxial tumors, not the rule in intraaxial tumors, and is not explainable in tumors of the fourth ventricle. Third, tumor infiltration or metastases do not remain unrecognized in times of advanced MR imaging. The immature study design of the two studies stimulated the initiation of the present prospective trial.
PI and brain surgery—present study
The major finding of the present study is that more than 40% of the patients of our study population already presented with PI before neurosurgical treatment, which leads to the conclusion that factors other than the operation itself cause the pituitary dysfunction. As there are no statistically significant differences, concerning tumor volume, midline shift, and localization had been seen between the group of patients with and without PI, the authors even do not believe that tumor-related effects to surrounding brain tissue are causative for PI. To further support this assumption, a study including other cancer patients undergoing surgery outside the brain and patients with the need for brain surgery other than cancer could serve as control groups in a second study trial. Secondary, hypogonadism was the most common finding in pre- and postoperative testing in the present study, which is somewhat in line with the postoperative findings of Schneider et al. and de Marinis et al. [5, 15] but which is in contrast to the results in aneurysmal subarachnoid hemorrhage (SAH) and brain trauma with GH deficiency predominance. Possibly, this discrepancy could be explained by the fact that patients with brain tumors are older than those with SAH and head injury. The prevalence of hypogonadism in healthy males aged 45 years or more has been estimated to be 38.7%, and hypogonadism could be more the result of advanced age than of tumor growth or tumor surgery [24]. If this holds true and if all male patients aged 45 years or more with secondary hypogonadism in the present study population would be excluded, the rate of PI in brain tumor patients would drop from 44.4% to only 20.4%. Furthermore, risk factors such as obesity, diabetes, hypertension, rheumatoid arthritis, hyperlipidemia, osteoporosis, chronic obstructive pulmonary disease, and chronic pain have been identified in the development of hypogonadism [24]. Thirteen of the 22 patients of our study population with primary or secondary hypogonadism had one or more of these risk factors, which mean that the possibility that hypogonadism is linked to PI is further being reduced.
If so, an even higher proportion of patients with PI would have underlined our results even more. Concerning patients with supratentorial extrasellar tumors, further studies are warranted to define the amount of patients suffering from surgery-induced PI or improvement of PD.
QoL and PI
Reduced mental health as well as disturbed emotional and social functioning, resulting in reduced QoL, are quite common in patients with PI and mostly are related to GH deficiency [15]. Thus, posttraumatic and posthemorrhagic mental, emotional, and social disorders are very similar to those of adult onset GH deficiency [25, 26]. As mentioned above, PI is frequent after head trauma and SAH, which means that not all these disorders in those patients could be related to the trauma or the bleeding. Subnormal vigor scores in multiple pituitary hormone deficiency are attributed to reduced testosterone levels [17]. As reduced QoL could be a subtle sign of PI, we performed SF-36 testing prior to surgery. We identified only a trend to a higher mean values in patients with PI reduced QoL in brain tumor patients is well described. We therefore believe that more the brain tumor and less PI contribute to the identified disorders.
Limitations of the study
We assumed that hypocortisolism and hypothyreoidism in the 25 patients, which had been pre-treated with either dexamethasone or l-thyroxine, represent drug effect and not PI. In those patients, no stimulation test was performed, which might have the potential to underestimate PI. As reported by Hartman et al., the insulin tolerance test is the classical test for the diagnosis of GH deficiency [27]. Since we only registered basal IGF-1 and performed pituitary stimulation with GHRH, we might have underestimated the proportion of patients with GH deficiency. We only examined blood samples preoperatively and on the first and seventh postoperative day. We did not perform follow-up investigations, which might have added further information about the possible impact of adjuvant radio- and chemotherapy on pituitary dysfunction as described by Schneider et al. and other investigators [4, 12, 28–30].
Conclusion
PI is not infrequent in patients undergoing surgery for brain tumors in distance to the hypothalamic–hypophyseal region. As PI could already be diagnosed prior to surgery, PI is not related to surgery but to other not yet identified factors.
Reduced QoL in patients with supratentorial tumors are more frequent than PI. Organic brain tissue changes seem to play a more important role for the development of QoL reduction than PI.
References
Agha A, Sherlock M, Brennan S et al (2005) Hypothalamic-pituitary dysfunction after irradiation of nonpituitary brain tumors in adults. J Clin Endocrinol Metab 90:6355–6360
Arlt W, Hove U, Müller B et al (1997) Frequent and frequently overlooked: treatment-induced endocrine dysfunction in adult long-term survivors of primary brain tumors. Neurology 49:498–506
Da Silva AN, Schiff D (2007) Adrenal insufficiency secondary to glucocorticoid withdrawal in patients with brain tumor. Surg Neurol 67:508–510
Darzy KH, Shalet SM (2005) Hypopituitarism as a consequence of brain tumours and radiotherapy. Pituitary 8:203–211
De Marinis L, Fusco A, Bianchi A et al (2006) Hypopituitarism findings in patients with primary brain tumors 1 year after neurosurgical treatment: preliminary report. J Endocrinol Investig 29:516–522
Dusick JR, Fatemi N, Mattozo C et al (2008) Pituitary function after endonasal surgery for nonadenomatous parasellar tumors: Rathke's cleft cysts, craniopharyngiomas, and meningeomas. Surg Neurol 70:482–491
Dziurzynski K, Delashaw JB, Gultekin SH et al (2009) Diabetes insipidus, panhypopituitarism, and severe mental status deterioration in a patient with chordoid glioma: case report and literature review. Endocr Pract 15:240–245
Fatemi N, Dusick JR, Mattozo C et al (2008) Pituitary hormonal loss and recovery after transsphenoidal adenoma removal. Neurosurgery 63:709–718
Jayasena CN, Gadhvi KA, Gohel B et al (2009) Day 5 morning serum cortisol predicts hypothalamic–pituitary–adrenal function after transsphenoidal surgery for pituitary tumors. Clin Chem 55:972–977
Kristof RA, Wichers M, Haun D et al (2008) Peri-operative glucocorticoid replacement therapy in transsphenoidal pituitary adenoma surgery: a prospective controlled study. Acta Neurochir (Wien) 150:329–335
Martinez R, Honegger J, Fahlbusch R, Buchfelder M (2003) Endocrine findings in patients with optico-hypothalamic gliomas. Exp Clin Endocrinol Diabetes 111:162–167
Marx M, Beck JD, Müller H et al (2000) Late hormonal complications after brain tumor treatment in childhood and adolescence: literature review and a model of integrated hormone aftercare. Klin Pädiatr 212:224–228
Oberfield SE, Garvin JH Jr (2000) Thalamic and hypothalamic tumors of childhood: endocrine late effects. Pediatr Neurosurg 32:264–271
Corneli G, Baldelli R, Di Somma C et al (2003) Occurrence of GH deficiency in adult patients who underwent neurosurgery in the hypothalamus-pituitary area for non-functioning tumour masses. Growth Horm IGF Res 13:104–108
Schneider HJ, Rovere S, Corneli G et al (2006) Endocrine dysfunction in patients operated on for non-pituitary intracranial tumors. Eur J Endocrinol 155:559–566
Daniel P (1959) Traumatic infarction of the anterior lobe of the pituitary gland. Lancet 2:927–930
Deijen JB, de Boer H, Blok GJ, van der Veen EA (1996) Cognitive impairments and mood disturbances in growth hormone deficient men. Psychoneuroendocrinology 21:313–322
Lippert-Gruner M, Lefering R, Svestkova O (2007) Functional outcome at 1 vs. 2 years after severe traumatic brain injury. Brain Inj 21:1001–1005
Popovic V, Pekic S, Pavlovic D et al (2004) Hypopituitarism as a consequence of traumatic brain injury (TBI) and its possible relation with cognitive disabilities and mental distress. J Endocrinol Investig 27:1048–1054
Wachter D, Gündling K, Oertel MF et al (2009) Pituitary insufficiency after traumatic brain injury. J Clin Neurosci 16:202–208
Hellawell DJ, Taylor RT, Pentland B (1999) Cognitive and psychosocial outcome following moderate or severe traumatic brain injury. Brain Inj 13:489–504
Kreitschmann-Andermahr I, Hoff C, Niggemeier S et al (2003) Pituitary deficiency following aneurysmal subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry 74:1133–1135
Vernet M, Rapenne T, Beaurain J et al (2001) Hypopituitarism after surgical clipping of a ruptured cerebral aneurysm. Crit Care Med 29:2220–2222
Mulligan T, Frick MF, Zuraw QC et al (2006) Prevalence of hypogonadism in males aged at least 45 years: the HIM study. Int J Clin Pract 60:762–769
Kelly DF, McArthur DL, Levin H et al (2006) Neurobehavioral and quality of life changes associated with growth hormone insufficiency after complicated mild, moderate, or severe traumatic brain injury. J Neurotrauma 23:928–942
Lieberman SA, Oberoi AL, Gilkison CR et al (2001) Prevalence of neuroendocrine dysfunction in patients recovering from traumatic brain injury. J Clin Endocrinol Metab 86:2752–2756
Hartman ML, Crowe BJ, Biller BM et al (2002) Which patients do not require a GH stimulation test for the diagnosis of adult GH deficiency? J Clin Endocrinol Metab 87:477–485
Constine LS, Woolf PD, Cann D et al (1993) Hypothalamic-pituitary dysfunction after radiation for brain tumors. N Engl J Med 328:87–94
Nishioka H, Hirano A, Haraoka J, Nakajima N (2002) Histological changes in the pituitary gland and adenomas following radiotherapy. Neuropathology 22:19–25
Taphoorn MJ, Heimans JJ, van der Veen EA, Karim AB (1995) Endocrine functions in long-term survivors of low-grade supratentorial glioma treated with radiation therapy. J Neurooncol 25:97–102
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Alvaro Campero, Tucumán, Argentina
Nachter et al. performed a prospective trial in 54 patients with supratentorial non-sellar tumor surgery. They studied the function of the pituitary gland preoperatively and on days 1 and 7 after the surgery. The authors found out that before the surgery, 44.4% of the patients already had pituitary insufficiency. They also realized that after the surgery, on days 1 and 7, the hormone profile showed no changes. Thus, the authors rule out that the cause of pituitary insufficiency in the postoperative period in patients operated on supratentorial non-sellar tumors is the surgery itself. Further research should be carried out in order to state if the percentage of biochemical pituitary insufficiency in patients with brain tumors (outside the sellar and parasellar region) is similar, greater, or lower, in relationship with the general population or, perhaps, with other pathologies. Moreover, further research should clarify the factors causing preoperative pituitary insufficiency in brain tumors. Beyond the fact that some questions still remain unanswered, the article of Watcher et al. is original and contributes to the understanding of this most important topic.
Ilonka Kreitschmann-Andermahr, Erlangen, Germany
The present study aimed to investigate if operations of brain tumors distant to the hypothalamo-pituitary region actually cause hypopituitarism. This is an important topic with potentially far reaching implications for post-surgical patient care. The prospective study design chosen by the authors is definitely the superior approach to the few cross-sectional studies which have only assessed hormone status after the intervention. However, the readers of this journal with a predominantly neurosurgical and not endocrinological background deserve to be assured about the soundness of the chosen methods and the meaningful interpretation of laboratory results in relationship to clinical parameters. To collect a range of basal hormone values in an inhomogeneous and in part severely ill and heavily medicated patient group before and after surgery, to combine these only in selected circumstances with endocrine function tests, and to diagnose pituitary insufficiency by imprecisely defined cut-off values is a questionable methodological choice. Making an endocrine diagnosis this way carries the risk of oversimplification and misinterpretation.
The authors acknowledged that many patients in the study group received drugs with known influence on central and peripheral hormone secretion and that numerous clinical conditions may impact upon the pituitary and peripheral hormone secretion. Furthermore, severe illness of any etiology is known to be accompanied by low T3 and low TSH levels. Opioids, antidepressants, neuroeptics, and antiepileptics as well as epilepsy itself, but also obesity may have a negative impact on the hypopituitary–gonadal axis. Insulin-like growth factor I (IGF-I) can at best be considered a marker of impaired GH secretion if, i.e., malnutrition, liver failure, poorly controlled diabetes mellitus, or uremia are ruled out. Patients with current dexamethasone therapy were precluded from evaluation of the corticotroph axis, but also pretreatment with corticosteroids in the weeks prior to the study might still corrupt the evaluation of the pituitary–adrenal axis. Hyperprolactinemia is well known to be caused by psychiatric medication as well as mental or physical stress.
It appears questionable to label the abnormal hormone values found as “pituitary insufficiency”. The eight patients with elevated IGF-I levels in the study population would in analogy have to be defined as having acromegaly. Whether it is meaningful to set these hormone levels in relation to neuroradiological findings or quality of life, results must remain open. The present study tells us that elderly, severely ill, and medicated patients may have abnormal hormone laboratory results prior to and after neurosurgery, but conclusions beyond that finding should be drawn cautiously and would have to be substantiated further.
Jens Schittenhelm, Tübingen, Germany
Wachter et al. demonstrate that pituitary insufficiency is frequently (44.8%) seen preoperatively in brain tumor patients and that hormone levels remain stable within the first week after surgery. This is important because several studies have drawn the conclusion that surgery distant from the sellar region might be causative for pituitary insufficiency. Their results warrant future studies examining other cancer patients undergoing surgery outside the brain and patients without cancer undergoing brain surgery as control groups as the factors that are causative remain to be identified. In patients with recurrent malignant brain tumors, attention on previous radiation therapy is needed. It is known that adults may demonstrate pituitary deficiencies even in cases where the focus is outside hypothalamic–pituitary axis [1, 2]. The high rate of preoperative medication with potential effect on pituitary function might also account for the preoperative insufficiency rate. The findings in this study also emphasize that the presence of pituitary insufficiency further influences quality of life and are in line with other observations in this field [3].
References
1. Borson-Chazot F, Brue T (2006) Pituitary deficiency after brain radiation therapy. Ann Endocrinol (Paris) 67:303–309
2. Bhandare N, Kennedy L, Malyapa RS, Morris CG, Mendenhall WM (2008) Hypopituitarism after radiotherapy for extracranial head and neck cancers in pediatric patients. Am J Clin Oncol 31:567–572
3. Psaras T, Milian M, Hattermann V, Will BE, Tatagiba M, Honegger J (2011) Predictive factors for neurocognitive function and quality of life after surgical treatment for Cushing's disease and acromegaly. J Endocrinol Invest (in press)
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Wachter, D., Gondermann, N., Oertel, M.F. et al. Pituitary insufficiency after operation of supratentorial intra- and extraaxial tumors outside of the sellar–parasellar region?. Neurosurg Rev 34, 509–516 (2011). https://doi.org/10.1007/s10143-011-0326-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-011-0326-5