
Abstract
Background
The usefulness of magnifying gastroscopy has been reported in differentiating between benign and malignant gastric mucosal lesions. However, there have been no studies of the usefulness of magnifying endoscopy with narrow-band imaging (M-NBI) in the diagnosis of superficial (non-polypoid) elevated lesions of the stomach. In this study, we investigated the ability of M-NBI to differentiate between cancer and adenoma in superficial elevated lesions of the stomach.
Methods
We examined 93 consecutive superficial elevated lesions of the stomach. We defined the endoscopic criteria for early cancer as red coloring using conventional white light imaging (C-WLI), and an irregular microvascular pattern with a demarcation line, or irregular microsurface pattern with a demarcation line, using M-NBI. We determined the sensitivity, specificity and accuracy of C-WLI and M-NBI in the diagnosis of these 93 lesions.
Results
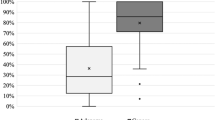
The sensitivity, specificity, and accuracy (95 % confidence interval) of C-WLI versus M-NBI were 64 % (52–76 %) versus 95 % (90–100 %), 94 % (86–100 %) versus 88 % (77–99 %), and 74 % (66–83 %) versus 92 % (86–98 %), respectively. Sensitivity and accuracy were significantly higher for M-NBI than C-WLI.
Conclusions
M-NBI appears to be useful in differentiating between cancerous and adenomatous superficial elevated lesions of the stomach.
Similar content being viewed by others


Introduction
Superficial (non-polypoid) elevated epithelial neoplasias of the stomach can be broadly divided into cancerous and adenomatous lesions. Differentiation between cancer and adenoma is difficult using conventional endoscopy with white-light imaging (C-WLI) alone, and biopsy is considered essential in making the differential diagnosis [1–4]. Red coloration is the only indicator of malignancy when examining superficial elevated lesions of the stomach using C-WLI [1–3, 5]; that is to say, adenomas have been reported to often be pale in color, whereas early gastric cancers of the superficial elevated type tend to be red in color. Previously, we reported that magnifying endoscopy is useful in differentiating between focal gastritis and small flat or depressed gastric cancers [6–15]. However, the usefulness of magnifying endoscopy with narrow-band imaging (M-NBI) in differentiating between cancer and adenoma in superficial elevated lesions of the stomach remains unclear.
In this study, we investigated the ability of M-NBI to differentiate between cancerous and adenomatous superficial elevated lesions of the stomach.
Methods
Subjects
We analyzed superficial elevated lesions of the stomach in consecutive subjects who underwent preoperative C-WLI and subsequent M-NBI, followed by endoscopic resection, between January 2006 and March 2010, with exhaustive histopathological examination of the resected specimen. Subject demographic characteristics are given in Table 1. All study participants provided informed consent, and the study design was approved by an ethics review board of Fukuoka University Chikushi Hospital.
Endoscopy procedures and endoscopic analyses
The endoscopy procedures described and illustrated in this article were performed by two experienced endoscopists (K.Y. and T.N.), as described previously, using a high-resolution magnifying upper gastrointestinal (GI) endoscope (GIF-Q240Z, Olympus, Tokyo) or a high-definition magnifying upper GI endoscope (GIF-H260Z, Olympus), and an electronic endoscopy system (Evis Lucera Spectrum, Olympus). This system incorporates both a structure enhancement function and an NBI function. The structure enhancement function of the video processor is set at a level of 4, 6, or 8 (level 4 or 6 for nonmagnified observation and level 8 for magnified observation). Before the procedure, a soft black hood (MB-162 for the GIF-Q240Z, MB-46 for the GIF-H260Z) is mounted at the tip of the endoscope to enable a constant distance of 3 mm between the tip of the endoscope zoom lens and the mucosal surface, at which distance maximal magnification of the endoscopic image can be obtained.
In practice, when a mucosal lesion is found during nonmagnified observation with white light imaging (WLI), the endoscopic findings include the color of the lesion. Subsequently magnification of the lesion is zoomed up to maximal, and the tip of the endoscope is then allowed to contact the mucosa immediately after the maximal magnification level has been reached. The magnified endoscopic findings are then interpreted using the vessel plus surface (VS) classification system.
Immediately after each endoscopic examination, the endoscopic findings using both C-WLI and M-NBI were recorded on the database by the aforementioned two experienced endoscopists (K.Y. and T.N.).
We reviewed the recorded endoscopic findings and collected the data. We retrospectively analyzed the endoscopic findings of the target lesions as follows. Initially, we classified the color of lesions as observed using C-WLI, in comparison with the surrounding mucosa, into red-color group (red-colored lesions) and not-red-color group (the same color, or paler than the surroundings) (Fig. 1a, b). The criterion for cancer was red coloration of the lesion and the criterion for non-cancer was not-red coloration of the lesion.

Conventional endoscopy with white light imaging (C-WLI) findings for superficial elevated lesions. a Red-color group. b Not-red-color group. C-WLI conventional endoscopy with white light imaging. Arrows indicate lesions
We then analyzed the M-NBI findings using the VS classification system proposed by Yao et al. [15, 16]. First, we determined whether a clear demarcation line (DL) was present at the border between the lesion and the surrounding mucosa. Then, we classified the lesion’s microvascular (MV) pattern as regular, irregular, or absent. Similarly, we classified the lesion’s microsurface (MS) pattern as regular, irregular, or absent. Finally, we defined lesions as cancers according to the following criteria: “the presence of an irregular MV pattern with a DL, or the presence of an irregular MS pattern with a DL, or both” [15–19]. If the M-NBI findings did not meet these criteria, we classified lesions as noncancerous lesions (Fig. 2).

Magnified endoscopic findings showing vessel plus surface (VS) classification (arrows, DL). DL demarcation line
Histopathological findings
We used the revised Vienna classification for histopathological diagnoses [20]. For the purposes of this study, we defined the revised Vienna classification Category 3 as low-grade adenoma (LGA), and the revised Vienna classification Categories 4 and 5 as early cancer (EC), reclassifying all lesions into LGA and EC groups.
Using the histopathological findings from the endoscopically resected specimens as the gold standard, we performed the following analyses. We determined the sensitivity, specificity, and accuracy of C-WLI in diagnosing cancer; we determined the sensitivity, specificity, and accuracy of M-NBI in diagnosing cancer; and we compared the sensitivity, specificity, and accuracy of the two methods in diagnosing cancer.
Statistical analyses
We determined the 95 % confidence interval (CI) for comparisons of the sensitivity, specificity, and accuracy of C-WLI and M-NBI. Student’s t test was used to compare mean values between groups and the χ2 test to compare frequencies between groups. A P value <0.05 was considered significant.
Results
Between January 2006 and March 2010, 340 epithelial gastric neoplasias were resected by either endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD). Following histopathological investigation of the resected specimens, 307 lesions were diagnosed as EC and 33 as LGA. The number of ECs with each macroscopic type (Paris classification) was as follows: 16 lesions were 0 I type, 4 were 0 I + IIa type, 61 were 0 IIa type, 1 was 0 IIa + I type, 7 were 0 IIa + IIb type, 25 were 0 IIa + IIc type, 11 were 0 IIb type, 3 were 0 IIb + IIc type, 152 were 0 IIc type, 15 were 0 IIc + IIa type, and 12 were 0 IIc + IIb type. The number of LGAs with each macroscopic type (Paris classification) was as follows: 32 were 0 IIa type and 1 was 0 IIc type. Accordingly, in total 93 superficial elevated lesions (61 EC and 32 LGA) were included in the analysis.
After examination of the 93 target lesions using C-WLI, 41 were classified into the red-color group and 52 into the not-red-color group (Figs. 3a, 4a). Of the 41 lesions in the red-color group, 39 were EC and 2 were LGA. Of the 52 in the not-red-color group, 22 were EC and 30 LGA (Table 2).

A representative case of early cancer (EC). a C-WLI findings. This lesion (arrow) was classified as not red colored (pale) using C-WLI. b Magnifying endoscopy with narrow-band imaging (M-NBI) findings (arrows, DL). Using the vessel plus surface (VS) classification system, this lesion was diagnosed as cancer by the presence of an irregular MV pattern plus an irregular MS pattern. c The histopathological diagnosis of the resected specimen was EC. C-WLI conventional endoscopy with white light imaging, M-NBI magnifying endoscopy with narrow-band imaging, VS vessel plus surface, MV microvascular, MS microsurface, EC early cancer, LGA low-grade adenoma, DL demarcation line

A representative case of low-grade adenoma (LGA). a C-WLI findings. This lesion (arrow) was classified as not red colored (pale) using C-WLI. b M-NBI findings (arrows, DL). Using the vessel plus surface (VS) classification system, this lesion was diagnosed as non-cancer by the presence of a regular MV pattern plus a regular MS pattern, with a DL. c The histopathological diagnosis of the resected specimen was LGA. C-WLI conventional endoscopy with white light imaging, M-NBI magnifying endoscopy with narrow-band imaging, VS vessel plus surface, MV microvascular, MS microsurface, EC early cancer, LGA low-grade adenoma, DL demarcation line
Using M-NBI, 62 of the 93 target lesions were classified as cancer (Fig. 3b) and 31 as noncancerous lesion in appearance (Fig. 4b). Of the 62 lesions classified as cancers using M-NBI, 58 were EC (Fig. 3c) and 4 were LGA on histopathological examination. Of the 31 lesions classified as noncancerous lesions by M-NBI, 3 were EC and 28 were LGA (Fig. 4c) on histopathological examination (Table 3).
The sensitivity, specificity, and accuracy, with their 95 % CI, for the identification of EC using C-WLI (with red color vs. not-red color as the marker) and M-NBI are shown in Table 4. Diagnostic sensitivity and accuracy were significantly higher for M-NBI than C-WLI.
Discussion
Until now, C-WLI and application of indigo carmine dye have been used to differentiate between adenoma and cancer in superficial elevated lesions of the stomach. In other words, a variety of endoscopic findings have been reported to be useful in the differential diagnosis of superficial elevated lesions of the stomach, such as the size of the lesion, changes in coloration when observed using C-WLI, and, following application of indigo carmine, the characteristics of superficial elevated lesions [1–4]. However, there have few objective studies of the usefulness of these endoscopic findings. Takemura et al. reported the endoscopic findings of coloration in superficial elevated lesions of the stomach (32 EC, 26 LGA). Red coloration was seen in 24 of 32 (75 %) EC lesions and in only 3 of 26 (11.5 %) LGA lesions. In other words, red coloration was significantly more common in malignant lesions. They reported lesion coloration to be the only objective marker to assist in differentiating between cancer and adenoma [5]. On the other hand, the results of this study showed that 22 lesions of 52 classified into the not-red-color group using C-WLI were in fact diagnosed as EC histopathologically. Accordingly, the distinction between LGA and EC is particularly difficult for superficial elevated lesions of the stomach that do not show red coloration when examined using C-WLI.
In recent years, advances in magnifying endoscopic technology allow observation down to the capillary level, and we previously reported the characteristics of EC as visualized using magnifying endoscopy and the usefulness of magnifying endoscopy in distinguishing EC from gastritis [9, 12, 13]. Combining M-NBI led to the proposal of a VS classification system, using the microvascular pattern (V) and the microsurface pattern (S), reported to be clinically useful in detecting early gastric cancers [15, 16, 18, 21, 22]. However, our search of the literature revealed no reports of the usefulness of M-NBI in diagnosing superficial elevated lesions of the stomach.
In this study, the sensitivity, specificity, and accuracy of M-NBI in diagnosing superficial elevated lesions of the stomach were 95 %, 88 %, and 92 %, respectively. Sensitivity, specificity, and accuracy were all higher for M-NBI than for C-WLI, the difference being significant for sensitivity and accuracy. In other words, when a lesion shows red coloration using C-WLI, the diagnostic specificity for cancer is sufficiently high that an accurate diagnosis of cancer can be made with C-WLI alone. On the other hand, when a lesion does not show red coloration using C-WLI, the diagnostic sensitivity for cancer is insufficient with conventional endoscopy. M-NBI should be performed, allowing differentiation between malignant and benign lesions with a high diagnostic accuracy.
Accordingly, we set out a diagnostic strategy for superficial elevated lesions of the stomach in Fig. 5. M-NBI is particularly useful for superficial elevated lesions that do not show red coloration using C-WLI.

Endoscopic diagnostic algorithm for differential diagnosis of superficial elevated lesions of the stomach. C-WLI conventional endoscopy with white light imaging, M-NBI magnifying endoscopy with narrow-band imaging, VS vessel plus surface, MV microvascular, MS microsurface, EC early cancer, LGA low-grade adenoma
The main limitation of this study is that it was a retrospective study. There is also the possibility of bias, such as a carrying-over effect. To avoid bias, we need to conduct a randomized controlled trial in the near future in which endoscopy procedures are randomly allocated to C-WLI or M-NBI. The findings of this study should now be tested in such a well-designed prospective study. Furthermore, because assessments of lesion color appear to be descriptive and subjective, we should quantify the degree of color using image analysis [23].
In conclusion, we conducted a retrospective study of M-NBI in diagnosing superficial elevated lesions of the stomach. Our results suggest that M-NBI could be useful in the diagnosis of early gastric cancer, in not only flat and superficial depressed, but also in superficial elevated lesions.
References
Hamada T, Kondou K, Simoya M, et al. Clinical management to gastric flat elevated lesion. Stomach Intest. 1999;34:1513–20. (in Japanese with English abstract).
Nakamura S, Matsumoto T, Ishikawa T, et al. Long term clinical course of gastric adenoma: a retrospective analysis of tumors with enlargement and those with malignant transformation. Stomach Intest. 2003;38:1389–400. (in Japanese with English abstract).
Toyozumi H, Tajiri H. Magnifying endoscopy diagnosis for elevated early gastric cancer and adenoma. Stomach Intest. 2011;46:853–65. (in Japanese with English abstract).
Motohiko K, Tsutomu N, Shusaku T, et al. Endoscopic submucosal dissection as a treatment for gastric noninvasive neoplasia: a multicenter study by Osaka University ESD study group. J Gastroenterol. 2011;46:325–31.
Takemura S, Iwashita A, Yao K, et al. The correlation between the quantified microvascular density and the endoscopic color in elevated type of gastric neoplastic lesions. Gastroenterol Endosc. 2002;44:745–54. (in Japanese with English abstract).
Yao K, Oishi T. Microgastroscopic findings of mucosal microvascular architecture as visualized by magnifying endoscopy. Dig Endosc. 2001;13:S27–33.
Yao K, Yao T, Iwashita A. Determining the horizontal extent of early gastric carcinoma: two modern techniques based on differences in the mucosal microvascular architecture and density between carcinomatous and non carcinomatous mucosa. Dig Endosc. 2007;14:S83–7.
Yao K, Oishi T, Matsui T, et al. Novel magnified endoscopic findings of microvascular architecture in intramucosal gastric cancer. Gastrointest Endosc. 2002;56:279–84.
Yao K, Iwashita A, Matsui T, et al. Microvascular architecture in gastric flat reddened lesions visualized by magnified endoscopy: usefulness for differentiating between gastritis and gastric cancer. Gastrointest Endosc. 2003;57:AB156.
Yao K, Kikuchi Y, Tanabe H, et al. Novel zoom-endoscopy technique for visualizing the microvascular architecture of early gastric cancer enables the precise margin of the cancer to be determined thereby allowing successful resection by the endoscopic submucosal dissection method. Endoscopy. 2004;36:A6.
Yao K, Iwashita A, Tao T. Early gastric cancer: proposal for a new diagnostic system based on micro vascular architecture as visualized by magnified endoscopy. Dig Endosc. 2004;16:S110–7.
Yao K, Iwashita A, Kikuchi Y, et al. Novel zoom endoscopy technique for visualizing the microvascular architecture in gastric mucosa. Clin Gastroenterol Hepatol. 2005;3:S23–6.
Yao K, Iwashita A, Tanabe H, et al. Novel zoom endoscopy technique for diagnosis of small flat gastric cancer: a prospective, blind study. Clin Gastroenterol Hepatol. 2007;5:869–78.
Yao K, Takaki Y, Matsui T, et al. Clinical application of magnification endoscopy and narrow-band imaging in the upper gastrointestinal tract: new imaging techniques for detecting and characterizing gastrointestinal neoplasia. Gastrointest Endosc Clin N Am. 2008;18:415–33.
Yao K, Anagnostopoulos GK, Ragunath K. Magnifying endoscopy for diagnosing and delineating early gastric cancer. Endoscopy. 2009;41:462–7.
Yao K, Iwashita A, Matsui T. A new diagnostic classification system by magnification endoscopy and narrow-band imaging in the stomach: microvascular architecture and microsurface structure. In: Niwa H, Tajiri H, Nakajima M, et al., editors. New challenges in gastrointestinal endoscopy. Heidelberg: Springer; 2008. p. 169–76.
Anagnostopoulos GK, Yao K, Kaye P, et al. Novel endoscopic observation in Barrett’s oesophagus using high resolution magnification endoscopy and narrow band imaging. Gut. 2006;55:A105.
Yao K, Nagahama T, Hirai F, et al. Clinical application of magnification endoscopy with NBI in the stomach and the duodenum. In: Cohen J, editor. Comprehensive atlas of high resolution endoscopy and narrow band imaging. Oxford: Blackwell; 2007. p. 169–176.
Yao K, Iwashita A, et al. White opaque substance within superficial elevated gastric neoplasia as visualized by magnification endoscopy with narrow-band imaging: a new optical sign for differentiating between adenoma and carcinoma. Gastrointest Endosc. 2008;68:574–9.
Schlemper RJ, Riddell RH, Borchard F, et al. The Vienna classification of gastrointestinal epithelial neoplasia. Gut. 2000;47:251–5.
Nagahama T, Yao K, Maki S, et al. Usefulness of magnifying endoscopy with narrow-band imaging for determining the horizontal extent of early gastric cancer when there is an unclear margin by chromoendoscopy (with video). Gastrointest Endosc. 2011;74:1259–67.
Ezoe Y, Muto M, Uedo N, et al. Magnifying narrowband imaging is more accurate than conventional white-light imaging in diagnosis of gastric mucosal cancer. Gastroenterology. 2011;141:2017–25.
Yao K, Yao T, Matsui T, et al. Hemoglobin content in intramucosal gastric carcinoma as a marker of histological differentiation: a clinical application of quantitative electronic endoscopy. Gastrointest Endosc. 2000;52:241–5.
Acknowledgments
Financial support for this study was provided by a grant-in-aid for Scientific Research (C) from the Japan Society for the Promotion of Science (# 21590882).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Maki, S., Yao, K., Nagahama, T. et al. Magnifying endoscopy with narrow-band imaging is useful in the differential diagnosis between low-grade adenoma and early cancer of superficial elevated gastric lesions. Gastric Cancer 16, 140–146 (2013). https://doi.org/10.1007/s10120-012-0160-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-012-0160-7