
Abstract
Purpose
Real-world experience with meropenem/vaborbactam (M/V) is limited. Our aim is to report a clinical experience of M/V in the treatment of resistant Gram-negative bacilli.
Methods
This is a prospective observational study including patients hospitalized in the University Hospital of Pisa (March 2021–Jan 2023) with infections by both extended-spectrum β-lactamases (ESBL)-producing Enterobacterales and carbapenem-resistant Klebsiella pneumoniae (Kp) treated with M/V. The primary outcome measure was clinical success, defined as a composite of survival, resolution of signs and symptoms and absence of microbiological failure at day 30 from infection onset. A multivariable regression analysis was performed to identify factors associated with clinical failure. Odds ratio (OR) with 95% confidence intervals (CI) was calculated.
Results
A total of 104 patients who received M/V were included: 24/104 (23.1%) infections were caused by ESBL non-hypervirulent Enterobacterales, 17/104 (16.3%) by ESBL-producing hypervirulent Klebsiella pneumoniae (hvKp) and 63/104 (60.6%) by CRE. The most common infections were bloodstream infections, followed by urinary tract infections, hospital-acquired pneumonia, intra-abdominal infections and others. Septic shock occurred in 16/104 (15.4%) patients. Clinical success was achieved in 77% of patients, and 30-day mortality rate was 15.4%. In patients with KPC-producing Kp infections, clinical success and 30-day mortality rates were 82% and 11.5%, respectively. On multivariable analysis, SOFA score (OR 1.32, 95% CI 1.02–1.7, p=0.032) was independently associated with clinical failure, while source control (OR 0.16, 95% CI 0.03–0.89, p=0.036) was protective.
Conclusions
M/V is a promising therapeutic option against infections caused by difficult-to-treat ESBL-producing Enterobacterales and CR-Kp.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gram-negative bacilli represent one of the greatest challenges for health care system worldwide [1]. In the last decades the armamentarium against carbapenem-resistant Enterobacterales (CRE) has been expanded with the marketing authorization of ceftazidime/avibactam (CZA) and, more recently, meropenem/vaborbactam (M/V) and imipenem/relebactam (I/R). While clinical experience of CZA has been consolidated in the last years, the knowledge about the clinical use of M/V and I/R is still limited [2, 3].
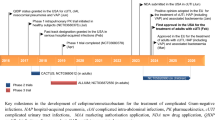
Current guidelines on the management of infections by multidrug-resistant Gram-negative bacilli recommend CZA or M/V as first line therapy in patients with infections by CRE if in vitro active or when KPC carbapenemase is detected [4,5,6]. Two randomized controlled trials (RCTs) evaluating the efficacy and safety of M/V are available: the TANGO I, which documented the non-inferiority of M/V compared to piperacillin/tazobactam in complicated urinary tract infections (UTIs), and the TANGO II, which demonstrated that M/V is associated with higher clinical cure compared to the best available therapy in patients with infections by CRE [7, 8]. Observational studies confirmed the efficacy of M/V in the treatment of CRE infections, but they are limited by small sample size and report data from compassionate use or early clinical experiences with M/V [9,10,11,12].
In this study we report a real-world experience with M/V for the treatment of infections caused by difficult-to-treat expanded-spectrum beta-lactamases (ESBL)-producing Enterobacterales and carbapenem-resistance K. pneumoniae (CR-Kp) after 2 years from the marketing authorization of this antibiotic in a clinical setting with high prevalence of multidrug-resistant bacteria.
Methods
This is a prospective observational study conducted in the University Hospital of Pisa (Italy) including patients who received M/V between March 2021 and January 2023. Patients were eligible for inclusion in the study if they (1) received M/V for at least 48 h, (2) were ≥ 18 years old, (3) had a documented infection by Enterobacterales. Polymicrobial infections were excluded.
Infections were classified according to CDC/NHSN definitions, as previously reported [13]. The probable source of bloodstream infections (BSI) was classified according to the available clinical and microbiological information, according to the NHSN/CDC definitions as detailed in Supplementary materials [14]. Low-respiratory tract as source of infection included both HAP/VAP without bacteremia and BSI secondary to a lower respiratory tract infection.
Demographic data, comorbidities, ward of hospitalization, clinical characteristics at infection onset and outcome were collected. To assess comorbidity burden, the age-adjusted Charlson Comorbidity Index was calculated. Severity of infection was assessed using the SOFA score. All patients were followed up until 30 days from infection onset. Occurrence of adverse events was prospectively evaluated.
The study was conducted in accordance with the Declaration of Helsinki. The study was approved by local ethical committee (IRB number 61185), and informed consent was obtained from study participants.
Study objective and outcomes
The primary objective of the study was to describe clinical features and outcome of patients treated with M/V. The primary outcome measure was clinical success, defined as a composite of survival, resolution of signs and symptoms and absence of recurrent infection or microbiological failure at 30-days from infection onset. Microbiological failure was defined as isolation of the same bacterial species following ≥7 days of M/V end of treatment. Persistent isolation of the same isolate from respiratory and urinary site was not considered a microbiological failure unless eradicated during M/V treatment.
The secondary objective was to identify factors independently associated with clinical failure, defined as lack of achieving clinical success.
Microbiological methods
On all microbiological samples, isolate identification was performed using matrix-assisted laser desorption ionization time of flight mass spectrometry (MALDI-TOF Biotyper, Bruker Daltonics). Antimicrobial susceptibility tests were performed with the SensiTitre™ system (Thermo Fisher Scientific, Waltham, MA, USA) according to the manufacturer’s instructions. Minimum inhibitory concentrations (MICs) were classified according to breakpoints established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST v.13) [15]. Among all the CRE isolates, the presence of a bla gene was determined with polymerase chain reaction assay using the GeneXpert System (Cepheid) as previously reported [16]. The hypermucoviscous phenotype was determined by the ‘string test’, a positive reaction being defined as a bacteriological loop being able to generate a viscous filament ≥5 mm in length by stretching bacterial colonies growth at 37 °C by 18–24 h on a blood agar plate, as previously reported [17]. Among hvKp, molecular typing was performed on three strains (according to Bioproject PRJNA746575) representative of three different time periods (one isolated in November 2020, one in January 2021 and one in March 2021), as previously reported [17]. A proportion of CRE isolates representative of the clones circulating in our hospital were subjected to whole-genome sequencing with an Illumina MiSeq platform (Illumina Inc., San Diego, CA, USA).
Sinergy between M/V and aztreonam against New Delhi metallo-beta-lactamases (NDM)-producing isolates was evaluated in real time for patients care, as previously reported [18]. It was explored using checkerboard analysis in MH broth and defined as a fractional inhibitory concentration (FIC) index≤0.5. FIC indices were 0.26 and 0.07, respectively [18].
Statistical analysis
Continuous variables were reported as median with interquartile ranges and categorical variables as numbers and percentages. Continuous variables were compared using the Student t test and Mann–Whitney U test as appropriate. Analysis of variance was used to analyze the differences of continuous variables among multiple groups. Categorical variables were evaluated using the χ2 or two-tailed Fisher exact test, as appropriate.
A multivariable logistic regression analysis was performed to identify factors independently associated with clinical failure. Variables with statistical significance at the univariate analysis (p < .05) and those with clinical relevance were entered into the multivariable model. The final multivariable model was chosen according to the Akaike information criterion. Odds ratio (OR) and 95% confidence intervals (95% CI) were reported.
Statistical significance was established at p ≤ .05. All reported p values are two tailed. The results obtained were analyzed using commercially available statistical software packages (IBM SPSS version 27, Armonk, NY).
Results
A total of 104 patients treated with M/V were included: 63 (60.6%) had infections caused by CRE (61 KPC-producing and 2 NDM-producing Klebsiella pneumoniae) and 41 (39.4%) by ESBL-producing Klebsiella pneumoniae (Fig. 1).

Study flow chart.
Microbiological isolates
Among 41 ESBL-producing Enterobacterales, 24 were non-hv Enterobacterales (n=17 Kp, n=6 E. coli, n=1 K. aerogenes), while 17 were hvKp. The three sequenced hvKp belonged to ST147, and their plasmid carried three replicons of the IncFIB (Mar), IncR and IncHI1B types and several resistance genes, including the rmpADC genes encoding enhancers of capsular synthesis [16]. CRE isolates included 61 KPC-producing and 2 NDM-producing Klebsiella pneumoniae. Sequenced KPC belonged to ST512 and carried the blaKPC-3 gene. The NDM-Kp belonged to ST147. Susceptibility patterns for all tested antibiotics are detailed in Supplementary Table 1. All hvKp were resistant to third-generation cephalosporins, aminoglycosides, fluoroquinolones, piperacillin/tazobactam, ceftolozane/tazobactam, ertapenem and trimethoprim/sulfamethoxazole and remained susceptible to meropenem, ceftazidime/avibactam and M/V. All KPC-Kp were susceptible to M/V, and 4/61 (6.5%) were resistant to ceftazidime/avibactam. The 2 NDM-Kp were resistant to both ceftazidime/avibactam and M/V.
Study population
The median age was 60 (IQRs 63–79) years. Thirty-one (29.8%) patients were cared for in intensive care unit (ICU). Three patients were hospitalized due to COVID-19. The most common types of infection were BSIs (n=41/104 [39.4%]), followed by UTIs (n=21/104 [20.2%]), hospital-acquired pneumonia (HAP, n=20/104 [19.2%]), intra-abdominal infections (IAIs, n=14/104 [13.5%]) and other type of infections (n=10/104, [9.6%]), including five osteoarticular infections, three surgical site infections, one orbital cellulitis, one orchiepididymitis and one central nervous system infection. Median time from infection onset to M/V therapy was 2 (IQRs 1–3) days. The vast majority of patients received M/V as monotherapy (n=90/104, 86.5%), while 14/104 (13.5%) received M/V in combination with other antibiotics (n=6 M/V plus tygecicline, n=6 M/V plus fosfomycin, n=2 M/V plus aztreonam). Median duration of treatment was 9 (6–14) days. Only one patient with sternal osteomyelitis received more than 30 days of M/V. Adverse events were reported in three patients (2.8%): one had a skin reaction, one increase in transaminases values (2xULN) and one thrombocytopenia.
Comparison of patients with infections by ESBL-producing non-hv Kp, ESBL-producing hv Kp and CRE is reported in Supplementary Table 2. The prevalence of HAP was higher in patients with infections by CRE (17/63, 27%) compared to ESBL-producing non-hv-Kp and ESBL-producing hv-Kp (2/24, 8.3% and 1/17, 5.9%, respectively, p=0.04).
Outcomes
Clinical success was achieved in 77% of cases (n=80 patients). Failures were due to death (n=16), worsening symptoms (n=3), recurrent infection (n=5). Among recurrent isolates, three were KPC-Kp and two were hv-Kp. All recurrent isolates remained susceptible to M/V. Overall thirty-day mortality rate was 15.4%.
Comparison of patients who achieved clinical success and those who did not is reported in Table 1. On multivariable analysis (Table 2), SOFA score (OR 1.32, 95% CI 1.02–1.7, p=0.032) was independently associated with clinical failure, while source control (OR 0.16, 95% CI 0.03–0.89, p=0.036) was protective.
Subgroup analysis in patients with KPC-producing Klebsiella pneumoniae infections
Sixty-one patients had infections by KPC-producing Klebsiella pneumoniae. Clinical features of patients with KPC-producing Klebsiella pneumoniae infections are reported in Table 3. Clinical success rate was 81.9%, and 30-day mortality rate was 11.5%.
Figure 2 shows outcome according to infection types. The highest mortality rates occurred in patients with HAP/VAP (17.6%), followed by IAI (14.3%), UTI (11.1%) and BSI (10.5%, p ns). Clinical success and 30-day mortality rates of all patients with low-respiratory tract infections (without bacteremia plus those with BSI secondary to low-respiratory tract infections) were 70% and 20%, respectively.

Outcome of patients with KPC-Kp infections treated with M/V according to type of infection.
Discussion
Our study reports a real-world experience with M/V in the specific setting of severe infections by both ESBL-producing and CR Enterobacterales, and suggests a good safety profile of the drug associated with a high rate of clinical success.
The peculiarity of our study is that we described the clinical profile of patients who receive M/V in the clinical practice. In our experience M/V use was not limited to CRE since we also cared for patients with non-hv ESBL-producing Kp, as well as patients with allergy to β-lactams and NDM-producing Kp infections. Moreover, we used M/V in some patients with infections by ESBL-producing hv-Kp strains, which are typically resistant to piperacillin/tazobactam, ceftolozane/tazobactam, ertapenem and had high MIC values to meropenem [17].
Overall, clinical success rate of patients with KPC-producing Klebsiella pneumoniae infections treated with M/V observed in our real-life experience (81.7%) is slightly higher than that reported by an early experience with M/V in 20 critically ill patients (70% of whom ICU patients) with CRE infections (clinical success 65%) [9] and in 37 patients with KPC-producing Klebsiella pneumoniae infections who received M/V as compassionate use (clinical success 55.6%) [12]. Moreover, the 30-day mortality rates of patients with KPC-producing Klebsiella pneumoniae infections in our study were low (11.7%), similar to that reported in these two studies (10% and 24.2%, respectively) [9, 12] and by a further study including 99 patients infected by CRE (19.2%) [10]. Of note, in our study mortality rates in patients with KPC producing Klebsiella pneumoniae treated with M/V did not differ from that of patients with ESBL-producing Kp. This finding is remarkable considering that more than one third of patients with KPC-Kp infections were cared for in ICU and HAP/VAP were more common in this group than in the ESBL one. In a recent study, excess mortality was lower in patients with KPC- than in those with MBL-producing CRE and carbapenem-resistant Pseudomonas aeruginosa and Acinetobacter baumannii [19]. This finding may be explained with the higher clinical success rates achieved by patients with KPC-producing Kp infections with the new BLBLI combinations compared to colistin [20,21,22,23]. However, studies comparing the three new BLBLI combinations (CZA, M/V and I/R) are lacking, and real-world experience are warranted to better understand the optimal place-in-therapy of these three drugs.
Of interest, in our study the vast majority of patients received M/V as monotherapy, while several published articles suggest that CZA is used in combination with other antibiotics in the majority of cases [23, 24]. Given the potential toxicity of some antibiotics usually associated with CZA (such as fosfomycin or aminoglycosides) and the risk associated with the unnecessary use of antibiotics in general, the fact that M/V can be used as monotherapy also in difficult-to-treat infections (pneumonia, infections with not achievable source control) should not be overlooked.
Our study provides new data about efficacy of M/V in 20 cases of KPC-producing Kp pneumonia (17 HAP/VAP without bacteremia and three BSI secondary to pneumonia), an underrepresented infection type in the Phase 3 RCT TANGO-II. In our study, we found a 30-day mortality rate of 20% in the subgroup of HAP/VAP caused by KPC producing Kp. This finding may suggest a good activity of the drug in patients with low-tract respiratory infections, as also suggested by PK/PD studies showing a significant penetration of M/V in the epithelial lining fluid (ELF) (ELF/plasma concentrations ratios were 65% and 79% for meropenem and vaborbactam, respectively [25]). Surprisingly, 30-day mortality rates in patients with KPC-Kp pneumonia was similar than mortality rates observed in the group of hvKp and non-hpKP ESBL infections, in which there were only two pneumonia cases. This may be mainly due to the limited sample size of our study that cannot allow comparison among different etiologies. Moreover, it should be considered that the ESBL hv-Kp in our hospital belong to the ST147, a recognized high risk clone that may be associated with high risk of clinical failure.
Our study is not without limitations. First, real-world studies are subject to inherent biases and limitations related to their observational design. Second, we are not able to perform genome sequencing of all strains; although the most common ESBL circulating in our hospital is CTX-M, we did not perform genome sequencing in all strains included in the present study. Third, our study lacks a comparator arm, hindering our ability to interpret the effectiveness and safety of M/V compared with other anti-CRE agents.
Conclusions
In conclusions, M/V use is associated with low mortality rates in infections caused by both difficult-to-treat ESBL-producing Enterobacterales and CR-Kp. Although in the real-world practice M/V is mostly used in patients with KPC-producing Kp infections, it may represent a therapeutic option in selected patients with infections by ESBL-producing Kp, such as hvKp, which are resistant to piperacillin/tazobactam, ceftolozane/tazobactam and ertapenem. Clinical success in patients with HAP/VAP by KPC-producing Klebsiella pneumoniae infections is promising. Further studies are needed to explore differences in the clinical profiles of patients who can beneficiate from the now available combinations active against CRE.
Data availability
The hypervirulent Klebsiella pneumoniae genomes have been released under Bioproject PRJNA746575, as previously reported [17].
References
Falcone M, Tiseo G, Dentali F et al (2018) Predicting resistant etiology in hospitalized patients with blood cultures positive for Gram-negative bacilli. Eur J Intern Med 53:21–28. https://doi.org/10.1016/j.ejim.2018.01.029
Carattoli A, Arcari G, Bibbolino G et al (2021) Evolutionary trajectories toward ceftazidime-avibactam resistance in Klebsiella pneumoniae clinical isolates. Antimicrob Agents Chemother 65:e0057421. https://doi.org/10.1128/AAC.00574-21
Tiseo G, Falcone M, Leonildi A et al (2021) Meropenem-vaborbactam as salvage therapy for ceftazidime-avibactam-, cefiderocol-resistant ST-512 Klebsiella pneumoniae-producing KPC-31, a D179Y variant of KPC-3. Open Forum Infect Dis 8:ofab141. https://doi.org/10.1093/ofid/ofab141
Paul M, Carrara E, Retamar P et al (2022) European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European Society of Intensive Care Medicine). Clin Microbiol Infect 28:521–547. https://doi.org/10.1016/j.cmi.2021.11.025
Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ (2022) Infectious Diseases Society of America 2022 Guidance on the treatment of extended-spectrum β-lactamase producing Enterobacterales (ESBL-E), carbapenem-resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa). Clin Infect Dis 75:187–212. https://doi.org/10.1093/cid/ciac268
Tiseo G, Brigante G, Giacobbe DR et al (2022) Diagnosis and management of infections caused by multidrug-resistant bacteria: guideline endorsed by the Italian Society of Infection and Tropical Diseases (SIMIT), the Italian Society of Anti-Infective Therapy (SITA), the Italian Group for Antimicrobial Stewardship (GISA), the Italian Association of Clinical Microbiologists (AMCLI) and the Italian Society of Microbiology (SIM). Int J Antimicrob Agents 60:106611. https://doi.org/10.1016/j.ijantimicag.2022.106611
Kaye KS, Bhowmick T, Metallidis S et al (2018) Effect of meropenem-vaborbactam vs piperacillin-tazobactam on clinical cure or improvement and microbial eradication in complicated urinary tract infection: the TANGO I randomized clinical trial. JAMA 319:788–799. https://doi.org/10.1001/jama.2018.0438
Wunderink RG, Giamarellos-Bourboulis EJ, Rahav G et al (2018) Effect and safety of meropenem-vaborbactam versus best-available therapy in patients with carbapenem-resistant Enterobacteriaceae infections: the TANGO II randomized clinical trial. Infect Dis Ther 7:439–455. https://doi.org/10.1007/s40121-018-0214-1
Shields RK, McCreary EK, Marini RV et al (2020) Early experience with meropenem-vaborbactam for treatment of carbapenem-resistant Enterobacteriaceae infections. Clin Infect Dis 71:667–671. https://doi.org/10.1093/cid/ciz1131 Erratum in: Clin Infect Dis. 70:1265
Alosaimy S, Jorgensen SCJ, Lagnf AM et al (2020) Real-world multicenter analysis of clinical outcomes and safety of meropenem-vaborbactam in patients treated for serious Gram-negative bacterial infections. Open Forum. Infect Dis 19(7):ofaa051. https://doi.org/10.1093/ofid/ofaa051
Alosaimy S, Lagnf AM, Morrisette T et al (2021) Real-world, multicenter experience with meropenem-vaborbactam for Gram-negative bacterial infections including carbapenem-resistant Enterobacterales and Pseudomonas aeruginosa. Open Forum Infect Dis 8:ofab371. https://doi.org/10.1093/ofid/ofab371
Tumbarello M, Raffaelli F, Cascio A et al (2022) Compassionate use of meropenem/vaborbactam for infections caused by KPC-producing Klebsiella pneumoniae: a multicentre study. JAC Antimicrob Resist 4:dlac022. https://doi.org/10.1093/jacamr/dlac022
CDC/NHSN Surveillance Definitions for Specific Types of Infections. 2023. https://www.cdc.gov/nhsn/pdfs/pscmanual/17pscnosinfdef_current.pdf. Accessed on 11 Nov 2023
CDC/NHSN bloodstream infection event (central line-associated bloodstream infection and non-central line associated bloodstream infection). https://www.cdc.gov/nhsn/pdfs/pscmanual/4psc_clabscurrent.pdf. Accessed on 11 Nov 2023
European Committee on Antimicrobial Susceptibility Testing Breakpoint tables for interpretation of MICs and zone diameters, version 13.0, 02 Jan 2023. EUCAST breakpoints. https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_13.0_Breakpoint_Tables.pdf. Accessed on 5April 2023.
Falcone M, Tiseo G, Galfo V et al (2022) Bloodstream infections in patients with rectal colonization by Klebsiella pneumoniae producing different type of carbapenemases: a prospective, cohort study (CHIMERA study). Clin Microbiol Infect 28:298.e1–298.e7. https://doi.org/10.1016/j.cmi.2021.06.031
Falcone M, Tiseo G, Arcari G et al (2022) Spread of hypervirulent multidrug-resistant ST147 Klebsiella pneumoniae in patients with severe COVID-19: an observational study from Italy, 2020-21. J Antimicrob Chemother 77:1140–1145. https://doi.org/10.1093/jac/dkab495
Tiseo G, Suardi LR, Leonildi A et al (2023) (2023) Meropenem/vaborbactam plus aztreonam for the treatment of New Delhi metallo-β-lactamase-producing Klebsiella pneumoniae infections. J Antimicrob Chemother 78:2377–2379
Falcone M, Tiseo G, Carbonara S et al (2023) Mortality attributable to bloodstream infections caused by different carbapenem-resistant Gram negative bacilli: results from a nationwide study in Italy (ALARICO Network). Clin Infect Dis 76:2059–2069. https://doi.org/10.1093/cid/ciad100
Falcone M, Bassetti M, Tiseo G et al (2020) Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae. Crit Care 24:29. https://doi.org/10.1186/s13054-020-2742-9
Shields RK, Nguyen MH, Chen L et al (2017) Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob Agents Chemother 61:e00883–e00817. https://doi.org/10.1128/AAC.00883-17
van Duin D, Lok JJ, Earley M et al (2018) Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin Infect Dis 66:163–171. https://doi.org/10.1093/cid/cix783
Karaiskos I, Daikos GL, Gkoufa A et al (2021) Ceftazidime/avibactam in the era of carbapenemase-producing Klebsiella pneumoniae: experience from a national registry study. J Antimicrob Chemother 76:775–783. https://doi.org/10.1093/jac/dkaa503
Balandín B, Ballesteros D, Pintado V et al (2022) Multicentre study of ceftazidime/avibactam for Gram-negative bacteria infections in critically ill patients. Int J Antimicrob Agents 59:106536. https://doi.org/10.1016/j.ijantimicag.2022.106536
Wenzler E, Gotfried MH, Loutit JS et al (2015) Meropenem-RPX7009 concentrations in plasma, epithelial lining fluid, and alveolar macrophages of healthy adult subjects. Antimicrob Agents Chemother 59:7232–7239. https://doi.org/10.1128/AAC.01713-15
Acknowledgements
Preliminary results of this study have been presented as oral communication in the 33rd European Congress of Clinical Microbiology and Infectious Diseases (ECCMID) (Abstract number 05661).
Funding
Open access funding provided by Università di Pisa within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Contributions
GT and MF are responsible for conceptualization. GT created the case report form, developed the database, coordinated the data collection, analyzed and interpreted data, wrote the manuscript. VG, NR, LRS, MP recruited patients and/or collected clinical data. CG, AL, SB performed microbiological analyses. All authors revised and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki. The study was approved by local ethical committee (IRB number 61185), and informed consent was obtained from study participants.
Competing interests
MF received unconditional grants from MSD and grants/or speaker honoraria from Angelini, Shionogi, Pfizer, Menarini, Gilead and Nordic Pharma. GT received honoraria for educational meetings by Shionogi. Declared conflicts of interest are outside the submitted work and did not affect the scientific objectivity of this study. The other authors have none to declare.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(PDF 460 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tiseo, G., Galfo, V., Riccardi, N. et al. Real-world experience with meropenem/vaborbactam for the treatment of infections caused by ESBL-producing Enterobacterales and carbapenem-resistant Klebsiella pneumoniae. Eur J Clin Microbiol Infect Dis (2024). https://doi.org/10.1007/s10096-024-04758-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10096-024-04758-2