
Abstract
IL-28B polymorphisms are predictors of response to therapy in adults infected with hepatitis C. We do not know whether they are markers of response to therapy in children and adolescents. The aim of this study was to determine whether single-nucleotide polymorphisms (SNPs) in the IL-28B gene could influence the probability of response to therapy compared with other known baseline prognostic factors and correlate with clinical findings in pediatric patients infected with hepatitis C virus (HCV) genotypes 1 or 4. We determined three SNPs of IL-28B (rs12979860, rs12980275, and rs8099917) in 82 patients with chronic HCV infection treated with pegylated interferon alpha and ribavirin (peg-IFNα/RBV). Treatment response and clinical data were analyzed. Overall, sustained virological response (SVR) was achieved by 45 % of patients infected with difficult-to-treat HCV genotypes 1 and 4. Except for IL-28B polymorphisms, there was no association of SVR with any other clinical data. IL-28B rs12979860 CC [odds ratio (OR), 6.81; p = 0.001] and rs8099917 TT (OR, 3.14; p = 0.013) genotypes were associated with higher SVR rates. IL-28B rs12980275 was not significantly associated with SVR (p = 0.058). Only the distribution between CC and CT–TT genotypes of rs12979860 significantly differentiated patients achieving early virological response (EVR) (OR, 10.0; p = 0.011). Children with the rs12979860 CC genotype had significantly higher baseline viral load compared with CT–TT patients (p = 0.010). In children and adolescents chronically infected with HCV genotypes 1 and 4, IL-28B rs12979860 and rs8099917 polymorphisms were the only predictors of response to peg-IFN/RBV.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of hepatitis C virus (HCV) in children in developed countries ranges between 0.1 and 0.4 %, and is generally lower than in adults. However, HCV is the most common cause of chronic liver disease of infectious etiology in children [1]. Although new, specifically targeted antiviral drugs are on the horizon, the combined therapy of pegylated interferon alpha (peg-IFNα) and ribavirin (RBV) is currently approved as the standard treatment for children. Even though most experts believe that the treatment is beneficial, due to several factors associated with treating young patients chronically infected with HCV, there is little consensus on when or how to optimally treat children with HCV infection [1–3]. According to recommendation from the European Medicines Agency (EMA), children with difficult-to-treat HCV genotypes 1 or 4 should be treated for 48 weeks, with treatment discontinued after 12 weeks if there has been no viral response. The main aim of therapy is to achieve a sustained virological response (SVR), which frequently determines the rate of therapeutic success. Identifying predictors of response to current therapy, particularly in patients infected with genotypes 1 and 4, remains as one of the main objectives of the research.
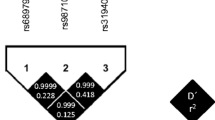
The viral factors, including HCV genotype, baseline viral load, and viral kinetics during treatment, as well as the characteristics of the host, such as age, gender, liver fibrosis, insulin resistance, and absence of adherence to therapy, have been fully studied in predicting the response to treatment [4–7]. Both host and viral factors are recognized to be important but do not adequately explain the observed variation in response to interferon alpha-based therapy for chronic HCV. Recent genome-wide association studies (GWAS) have shown that human genetic variations (single-nucleotide polymorphisms, SNPs) around the gene for interleukin 28B (IL-28B) may explain differences in the results of the treatment of adults chronically infected with HCV and that they can be useful as therapy response markers [8–11]. Among them, the most important ones seem to be rs12979860, rs8099917, and rs12980275. Currently, a large number of independent validations of the importance of IL-28B variants related to HCV treatment response in different populations of chronically infected adults is being carried out. According to these studies, patients with genotypes CC rs12979860, TT rs8099917, and AA 12980275 are statistically more likely to achieve SVR compared to patients bearing the T allele of rs12979860 (TT and CT), the G allele of rs8099917 (TG and GG), and the G allele of rs12980275 (AG and GG). Additionally, it was reported that the favorable IL-28B genotypes were independent strongest pretreatment predictors of treatment response in European patients [12]. The population of children has not yet been widely evaluated in order to determine the relationships between IL-28B polymorphisms and treatment response. Although the described variations are independent, their effects on the final therapy outcome may have a different strength in adults and children, due to the different distribution of prognostic factors that may affect the final results of the therapy, such as liver fibrosis, which seems to increase with the age of the patient and/or with the duration of the disease. Therefore, higher rates of efficacy are being observed in pediatric patients in clinical practice.
In the presented study, we defined the relationship between SNPs rs12979860, rs12980275, and rs8099917 and response to peg-IFN and RBV combined therapy in children and adolescents infected with HCV genotypes 1 and 4. This information is important for better prediction of response to therapy, and could allow for a better selection of patients for further treatment.
Materials and methods
Patients and clinical data
Overall, 82 chronic HCV patients of Caucasian ethnicity, both children and adolescents infected with viral genotypes 1 or 4, were included in the study. We retrospectively selected a cohort of naïve patients under 18 years of age who were treated with combined antiviral therapy with peg-IFNα-2a or 2b and RBV between the years 2006 and 2011 in one of the Polish academic centers. Children whose medical records allowed to obtain information on the clinical course of infection and the effectiveness of treatment were included in the analyses. Patients underwent treatment under a standard protocol with peg-IFNα (Pegasys, PegIntron) and weight-based RBV for 48 weeks. The exclusion criteria included hepatitis B or human immunodeficiency virus (HIV) coinfection, coexistent autoimmune liver diseases, hemochromatosis, or other coexistent chronic liver diseases (Wilson’s disease). Blood samples from these patients were used for genotyping.
The HCV genotype was determined using the INNO-LiPA HCV assay (Innogenetics) and chronic infection was defined as a detectable HCV RNA for at least 6 months. In assessing the effectiveness of antiviral treatment, virological response criteria were used. Baseline viral load and viral concentration at week 12 of treatment were measured by quantitative polymerase chain reaction (PCR) assay using the COBAS AmpliPrep/COBAS TaqMan HCV RNA Test (Roche Molecular Diagnostics); sensitivity > 15 IU/ml, dynamic range of quantification 43–69,000,000 IU/ml. In order to determine the treatment’s efficacy, in patients with a 48-week course of therapy, HCV RNA levels were measured by qualitative PCR at the end of treatment and 24 weeks after the completion of treatment. The primary endpoint of the study was SVR, defined as undetectable HCV RNA in serum 24 weeks after the completion of therapy. The lack of response to therapy was defined as HCV viral load decline less than 2 logs at week 12 during therapy or detectable HCV RNA in serum at any other time during the 48-week therapy. Relapse was defined as undetectable HCV RNA in serum at the end of therapy, followed by detectable HCV RNA after the completion of therapy. The secondary endpoint was early virological response (EVR), defined as a reduction of HCV RNA by at least 2 logs after the first 12 weeks of treatment compared with baseline HCV RNA levels. Patients who failed to achieve EVR were considered to be non-responders, and their therapy was discontinued. EVR with undetectable HCV RNA in serum was referred as a complete EVR (cEVR). To carry out the analysis, we divided the patients into two groups: SVR (including individuals who achieved SVR) and non-response/relapse (NR/R) (with individuals who were non-respondent or who had a relapse during therapy).
Liver histological analysis was carried out by only one pathologist using the modified Scheuer scoring system (F0–F4; A0–A4) on liver biopsies obtained no later than 18 months before therapy. Detailed results of the demographic characteristics and other standard clinical data were obtained from patients’ clinical documentation. The protocol was approved by the Ethics Committee of Collegium Medicum, Nicolaus Copernicus University, Bydgoszcz, Poland. Informed consent was provided in writing by the legal guardian of each patient before treatment was initiated.
DNA extraction and IL-28B genotyping
In order to carry out the genotyping analysis, genomic DNA was prepared by the extraction method using Igepal CA-630 detergent from peripheral blood samples collected in 0.5 M EDTA tubes. Subsequent handling of the DNA, including quality control and dilution to working concentrations, was carried out in our own laboratory. The genotyping of SNPs rs12979860, rs12980275, and rs8099917 was carried out by polymerase chain reaction and restriction fragment length polymorphism (PCR-RFLP). For rs12979860, the primer sequences were: 5′-CGC TTA TCG CAT ACG GCT AGG-3′ (sense) and 5′-AGG CTC AGG GTC AAT CAC AGA AG-3′ (antisense). For rs8099917, the oligonucleotide primers were: 5′-CAT CCC ACT TCT GGA ACA AAT C-3′ (sense) and 5′-GTA TCA ACC CCA CCT CAA ATT ATC-3′ (antisense). For rs12980275, the primer sequences were: 5′-AAG AGG AGG GAA GGA AGT TCT G-3′ (sense) and 5′-GGT CTG GTC CTA GTG GTG TTT G-3′ (antisense). The PCR conditions (20 μL) were: initial denaturation at 95 °C for 2 min, followed by 35 cycles of denaturation at 95 °C for 30 s, annealing at 60 °C for 25 s, and extension at 72 °C for 40 s. The PCR products for rs12979860, rs8099917, and rs12980275 were of 243, 400, and 293 base pairs, respectively.
In order to perform the RFLP assay for the rs12979860 genotype, 15 μL of amplicons were digested with 2 U of BstUI restriction endonuclease (Fermentas) at 37 °C for 12 h. BstUI digestion of allele CC yields fragments of 136, 82, and 25 base pairs, whereas DNA containing the allele TT polymorphism yields fragments of 161 and 82 base pairs. For the RFLP assay for the rs8099917 genotype, 15 μL of amplicons were digested with 1 U of BseMI restriction endonuclease (Fermentas) at 55 °C for 12 h. BseMI digestion of allele TT yields fragments of 400 base pairs, whereas DNA containing the allele GG polymorphism yields fragments of 234 and 166 base pairs. For the RFLP assay for the rs12980275 genotype, 20 μL of amplicons were digested with 2 U of BseLI restriction endonuclease (Fermentas) at 55 °C for 12 h. BseLI digestion of allele AA yields fragments of 178 and 115 base pairs, whereas DNA containing the allele GG polymorphism yields fragments of 148, 115, and 30 base pairs. Restriction digestion products for each were separated on agarose gel stained with ethidium bromide for visualization on a UV transilluminator.
To confirm the PCR-RFLP results, the rs12979860, rs8099917, and rs12980275 SNPs were genotyped using the ABI TaqMan SNP genotyping assays (Applied Biosystems) and predesigned commercial genotyping assays (ABI assay C_11710096_10). The real-time PCR reactions were performed in 96-well microplates with the ABI Prism 7000 Sequence Detection System (Applied Biosystems). Allele discrimination was achieved by fluorescence detection.
Statistical analyses
In this work, the patient characteristics are reported as medians (ranges) or absolute and relative frequencies, n (%), as appropriate. The genetic and clinical features [age, gender, liver histopathology (Scheuer score), viral load before treatment, serum levels of alanine aminotransferase (ALT), HCV genotype, and IL-28B SNP] were compared between patients having SVR (34 responders) and those who did not respond to peg-IFN plus ribavirin treatment or had a relapse after the end of the treatment (48 relapsers/non-responders). To identify factors predicting treatment response, we evaluated the statistical significance in the univariate analysis of the relationships between clinical characteristics and the response phenotype (responder/non-responder). Continuous variables were compared with Mann–Whitney U-tests (the distributions were not parametric). The Pearson Chi-square or Fisher’s exact test, where appropriate, were used for categorical variables. For all these tests, two-tailed p-values were used and p-values < 0.05 were considered to be statistically significant. Odds ratios (ORs) and 95 % confidence intervals (CIs) were also calculated for association tests between the IL-28B polymorphisms and the binary clinical variables. All statistical analyses were performed with SPSS software version 20 for Windows.
Results
Clinical characteristics
A total of 82 patients chronically infected with HCV, 14 (17.1 %) children (4–11 years old) and 68 (82.9 %) adolescents (12–17 years old), 34 (41.5 %) girls and 48 (58.5 %) boys, were studied. The median age at the onset of therapy was 15 years. This study recruited patients infected with HCV genotypes 1 (59.8 %) or 4 (40.2 %). The demographic and clinical characteristics of the examined patients, stratified by HCV genotype, are presented in Table 1.
All patients’ initial viral load was determined and described by the percentage of patients in each categorization of high and low initial viral load. The two limits most common in the literature, that is, 600,000 and 800,000 IU/ml, were adopted. The median baseline HCV viral load of the entire group was 3.98 × 105. For this patient characteristic, the level of ALT and GGTP activity prior to treatment was taken into account. Forty-eight (58.5 %) patients had abnormal ALT serum levels and 14 (17.1 %) patients had abnormal GGTP serum levels. For all patients, the median levels of ALT and GGTP was 36 and 60 UI/L, respectively (normal range GGTP <61 and <36 UI/L and ALT <41 and < 31 UI/L for males and females, respectively). Pretreatment liver biopsy samples were assessed from 78 (95 %) patients. The liver biopsy data showed that most patients had staging F1 (55.1 %) and F2 (26.9 %), as well as grading A1 (43.6 %) and A2 (50.0 %) (modified Scheuer score). None of these patients had cirrhosis. The groups of HCV genotype 1-infected patients and HCV genotype 4-infected patients were comparable with respect to gender, age at the start of the treatment, median serum ALT and GGTP concentration, and liver histology, but their baseline viral loads were different. Patients with HCV genotype 1 had significantly higher baseline viral loads than patients with genotype 4 (5.4 × 105 vs. 2.9 × 105 for genotypes 1 and 4, respectively; p = 0.012). There were no differences among HCV genotypes in the distribution alleles of IL-28B polymorphisms.
Overall, 34 (41.5 %) patients achieved an SVR and, in 48 cases, there was a treatment failure [41 patients (50.0 %) were non-responders and 7 (8.5 %) were relapsers]. In selected subgroups for HCV genotypes 1 or 4, the treatment efficacy was 44.9 and 36.4 %, respectively, and the observed difference was not statistically significant. HCV viral load decline of less than 2 logs at week 12 during therapy affected 31.7 % of patients, but was more frequently observed in patients infected with HCV genotype 4 [14 (42.4 %)] compared to HCV genotype 1 infection [12 (24.5 %)]. Among the 56 patients who achieved EVR, 34 (60.7 %) achieved SVR. Sixty patients with cEVR achieved SVR.
The rapid virological response (RVR), defined as an undetectable HCV RNA at week 4 after treatment initiation, was available for 34 patients. Among them, HCV RNA was undetectable in five patients (14.7 %) (data not shown).
Clinical and demographical variables associated with SVR
At first, the association between the main clinical and demographical variables known to influence HCV viral clearance and achievement of SVR was evaluated. Factors such as age, gender, liver histology, and viral load were assessed for obtaining SVR. As shown in Table 2, there were no statistically significant differences in the baseline characteristics between responders and non-responders, which may be related with the poor cardinality of the study group. Despite the lack of statistical significance, the median values of ALT and GGTP activity were lower in patients achieving SVR. In contrast, in our study, responders had a higher median baseline viral load than non-responders. In addition, the categorization of viremia in terms of 8 × 105 IU/ml value showed the greatest variation between analyzed groups, with a reduced rate in a group achieving SVR.
Relationship between treatment response and IL-28B gene polymorphisms
Among our 82 treated patients, the genotypic frequency of rs12979860 CC was 20.7 %, CT was 54.9 %, and TT was 24.4 %. The proportion for rs8099917 TT was 42.7 %, TG 50.0 %, and GG 7.3 %, and for rs12980275 AA was 19.5 %, AG 54.9 %, and GG 25.6 %. Univariate analysis (Table 2) showed no relationship of response type with either age at therapy, gender, baseline viral load, fibrosis, or viral genotype (1 vs. 4). In contrast, a significant relationship was observed between response type and the IL-28B SNP genotype. The response to treatment depending on the genotypes of IL-28B is shown in Table 3. The genotype distributions for IL-28B rs12979860 and rs8099917 polymorphisms were significantly different between responders and non-responders (p = 0.001 and p = 0.013, respectively). In our series, for rs12979860, the odds ratio of being a responder for the CC genotype as compared to genotypes CT and TT was 6.81 (95 % CI = 1.98–23.42). The SVR was achieved in 76.5 % of patients with the genotype CC of rs12979860, compared with 33.3 % in patients with the genotype CT and 30.0 % in patients with the genotype T/T. For rs8099917, the OR of being a responder for the TT genotype as compared to genotypes TG and GG was 3.14 (95 % CI = 1.26–7.85). The response rates were 57.1, 31.7, and 16.7 % for genotypes TT, TG, and GG, respectively. In contrast, no significant difference was found between the genotype distribution of rs12980275 and treatment outcome (p = 0.058). Despite the lack of statistical significance, response rates for rs12980275 indicate the relationship of this marker with SVR. The response rates were 62.5, 37.8, and 33.3 % for genotypes AA, AG, and GG, respectively.
A relationship was observed between EVR and the IL-28B SNP genotype. The distribution of genotypes CC and CT–TT rs12979860 significantly divided the patients in terms of the frequency of achieving EVR (OR = 10.0; 95 % CI = 1.25–80.14). In contrast, no significant difference was found between TT/TG–GG rs8099917 and AA/AG–GG rs12980275 genotypes among patients with and without EVR. Additionally, achieving cEVR was independent of the genotypes distribution of all the analyzed IL-28B polymorphisms.
Association between baseline viral load and IL-28B gene polymorphisms
Patient age, gender distribution, ALT, GGTP activity, and liver fibrosis stage did not differ by SNP genotype in the analyzed groups. Despite there being no significant differences between the median baseline viral load and treatment response among the analyzed groups, a significant relationship between the median baseline viral load and IL-28B rs12979860 genotypes was shown (Fig. 1). The median baseline viral load for patients with genotype CC rs12979860 was 7.1 × 105 (6.3 × 104–5.4 × 106) and for patients with genotype CT–TT, it was 2.9 × 105 (3.7 × 103–4.7 × 106) (p = 0.010). Although the median viral load was higher in patients with either the TT rs8099917 or AA rs12980275 genotypes, compared with patients with the TG–GG rs8099917 or AG–GG rs12980275 genotypes, the differences did not reach statistical significance (p = 0.087 and p = 0.053, respectively). Moreover, the viral load was analyzed as a categorical variable using known cut-off levels of 600,000 or 800,000 IU/ml (Table 4). For a cut-off of 600,000 IU/ml, we showed that favorable genotypes of all the analyzed markers were associated with high viral load (rs12979860: OR = 5.40, 95 % CI = 1.68–17.38, p = 0.003; rs8099917: OR = 2.50, 95 % CI = 1.00–6.21, p = 0.047; rs12980275: OR = 3.33, 95 % CI = 1.07–10.36, p = 0.032). However ,this association was not observed using a cut-off level of 800,000 IU/ml for all markers.

The association of the interleukin 28B (IL-28B) single-nucleotide polymorphism (SNP) with hepatitis C virus (HCV) baseline viral load in chronic HCV patients. There were significant differences in viral load between patients with rs12979860 genotype CC (median, 7.1 × 105 IU/ml; range, 6.3 × 104–5.4 × 106 IU/ml) and CT–TT (2.9 × 105 IU/ml; range, 3.7 × 103–4.7 × 106 IU/ml; p = 0.010). Statistical analysis was performed using a Mann–Whitney U-test
Discussion
This retrospective study was performed in a large unique monocentric cohort of 82 pediatric patients infected with difficult-to-treat HCV genotypes 1 and 4, who were treated with peg-IFN and RBV. Up to now, the results of several trials in children and adolescents with chronic hepatitis C using peg-IFNα-2a or 2b in combination with RBV have been reported [13–17]. As expected, based on adult studies, the rates of virological response were significantly lower in patients infected with HCV genotypes 1 and 4 than in patients infected with other genotypes. According to these studies, SVR rates in patients with HCV genotype 1 ranged from 40 to 60 %, and the relapse rate was between 7.7 and 17 %. However, data regarding the efficacy of peg-IFN and RBV for the treatment of chronic hepatitis C in children and adolescents infected with genotype 4 are limited because of the small size of test groups [18, 19]. In fact, most trials were carried out in western countries, where HCV genotype 1 is the predominant variant, followed by genotypes 2 and 3, and genotype 4 is relatively uncommon. In our study, among all the analyzed pediatric patients, the achievement of SVR was 41.5 % (44.9 % and 36.4 % for genotypes 1 and 4, respectively). Therefore, the SVR rate reported in our study is comparable to those obtained from prospective clinical trials of children and adolescents with HCV genotype 1.
In this study, we determined the role of known determinants eliminating HCV in response to treatment in children who received combined treatment with peg-IFN and RBV. We determined that age, gender, ALT or GGTP activity, and histological findings from liver biopsy do not significantly correlate with the SVR rate in combined therapy. Responders showed similar median baseline ALT and GGTP activity compared with non-responders, and patients with normal ALT or GGTP values display the same SVR rate as those with abnormal biochemistry prior to therapy. Patient age and gender do not seem to influence response; however, the group of patients <12 years old was relatively small. According to our study, the results for age, gender, ALT, and liver histology were similar to those reported in known studies among children who received combined treatment with peg-IFN and RBV. In contrast, the lack of the baseline viral load’s role in predicting SVR presented in this study is at odds with the data previously published by Wirth et al. for patients with HCV genotype 1. Wirth et al. showed that 32 % with high viral load (>600,000 IU/ml) and 73 % with low viral load (<600,000 IU/ml) achieved SVR [17]. In a second study by Sokal et al. using a cut-off value of 500,000 IU/ml, 45 % of children with HCV RNA >500,000 IU/ml and 62 % with HCV RNA <500,000 IU/ml achieved SVR [16]. Moreover, we demonstrated no predictive role when the viral load was analyzed as a categorical variable using a cut-off level of 800,000 IU/ml. In a comparative analysis of baseline characteristics, we observed significantly lower baseline viral loads in patients with HCV genotype 4 than in patients with HCV genotype 1; however, the SVR rates between these subgroups do not differ significantly. This observation confirms previously reported findings in adults [20]. Because of discontinued therapy in patients who did not achieve EVR, this study did not assess the statistical significance of EVR and cEVR on the SVR rate. According to trials, among the adult naïve patient population, less than 5 % of patients who failed to achieve an EVR ultimately achieved SVR [21]. However, similarly to other reports [13, 17], our study determined that the distribution of EVR and cEVR stratified by SVR showed an association with the SVR rate.
To the best of our knowledge, this is a unique study that specifically examines the genotype frequencies of IL-28B rs12979860, rs8099917, and rs12980275 polymorphisms in children and adolescents with chronic HCV-1/4 infection. Interestingly, the distribution of genotypes differed compared to the results of studies conducted in adult Caucasian populations [8, 9, 20, 22]. While in the European studies of the Caucasian race nearly 40 % incidence of the CC genotype is observed, the incidence rate for patients in the study population did not exceed 30 %. The reduced frequency of favorable genotypes rs12979860 CC, rs8099917 TT, and rs12980275 AA may be a result of the test group’s limited cardinality and needs to be confirmed in studies on a larger group of patients. However, in the only available study, published in abstract form, carried out by Hierro et al. on 61 children of white-Hispanic population from which 52/61 were infected with genotypes 1 and 4, the distribution of IL-28B rs12979860 genotype was as follows: CC = 14 (22.9 %), CT = 35 (57.3 %), TT = 12 (19.6 %) [23]. In our and Hierro et al.’s study, it was demonstrated that the most commonly occurring rs8099917 marker genotype was the heterozygotic variant TG, in contrast to adult patients, where the favorable TT genotype dominated. In fact, in several adult trials, it was demonstrated that the favorable IL-28B genotypes increase the chances of spontaneous elimination of the virus [9, 24]. In a recent study, Ruiz-Extremera et al. analyzed the role of IL-28B polymorphism in HCV vertical transmission (HCV-VT) and in the spontaneous clearance of HCV among infected infants [25]. They showed that rs12979860 plays no role in HCV-VT, but the IL-28B CC child polymorphism is associated independently with the spontaneous clearance of HCV genotype 1 among infected infants born to HCV-infected mothers. It was found that the CC polymorphism is the only predictor of HCV clearance in HCV genotype 1 in infants. Additionally, Hierro et al. reported an increased frequency of parenteral infection in children with the rs12979860 CC genotype [23]. Unfortunately, the mode of HCV infection in the examined patients was not determined in our study.
The main focus of this study was to determine the predictive value of IL-28B SNP in treatment outcome in children and adolescents infected with HCV genotypes 1 and 4. In this study, the IL-28B rs12979860 CT and rs8099917 TG, but not rs12980275 polymorphisms’ pivotal role in predicting the rate of SVR in the analyzed group was demonstrated. We found that children/adolescent’s IL-28B polymorphisms were the only predictors of SVR in HCV genotypes 1 and 4. A particularly strong relationship between rs12979860 and the viral clearance rate was observed. Additionally, only the IL-28B rs12979860 polymorphism affects the earliest treatment milestone, which is EVR. However, neither rs12979860 nor other markers influence cEVR. These observations suggest that viral eradication at week 12 of treatment in HCV genotypes 1 and 4 infection is partly influenced by IL-28B. The relationship between the IL-28B SNP and SVR has not been widely studied in pediatric patients. In the study by Hierro et al. performed on children with chronic HCV genotypes 1, 2, and 4, the investigators demonstrated that polymorphisms in the IL-28B gene region rs12979860 and 8099917 were the only predictors of response to peg-IFN/RBV, a finding similar to ours. Moreover, similarly to Hierro et al.’s results, we showed a significant association of the IL-28B rs12979860 CC genotype with higher baseline viral load, and, in contrast, no significant association with lower levels of ALT.
Despite promising results, this study has some limitations. First of all, this is a retrospective study. Secondly, it takes into consideration not only the patients who completed the planned treatment period (48 weeks). Furthermore, reports of adults treatment showed no difference in SVR between peg-IFNα 2a and 2b [26]; therefore, we hypothesize the same relation in patients <18 years old because of an absence of a comparison study at this point in time. In this study, we did not determine certain baseline characteristics that may help to better select candidates for therapy, such as infection mode. Studies among children showed that treatment was particularly effective in patients with parenterally acquired infections [13, 27]. However, statistical significance was not reached, probably due to the small number of enrolled patients. A prospective controlled study will be necessary in order to evaluate the influence of IL-28B polymorphisms on peg-IFN and RBV combined treatment in children and adolescents with chronic hepatitis C.
In conclusion, this study demonstrated the role of IL-28B in predicting the outcome of antiviral therapy in children and adolescents chronically infected with difficult-to-treat HCV genotypes. Thus, the determination of the IL-28B SNP, like in adults, may be useful in clinical practice in enhancing the correct prediction of SVR achievement in treating this group of young patients.
References
Jara P, Hierro L (2010) Treatment of hepatitis C in children. Expert Rev Gastroenterol Hepatol 4(1):51–61
Yeung LT, Roberts EA (2010) Current issues in the management of paediatric viral hepatitis. Liver Int 30(1):5–18
Serranti D, Buonsenso D, Ceccarelli M, Gargiullo L, Ranno O, Valentini P (2011) Pediatric hepatitis C infection: to treat or not to treat…what’s the best for the child? Eur Rev Med Pharmacol Sci 15(9):1057–1067
Shirakawa H, Matsumoto A, Joshita S, Komatsu M, Tanaka N, Umemura T, Ichijo T, Yoshizawa K, Kiyosawa K, Tanaka E; Nagano Interferon Treatment Research Group (2008) Pretreatment prediction of virological response to peginterferon plus ribavirin therapy in chronic hepatitis C patients using viral and host factors. Hepatology 48(6):1753–1760
Maekawa S, Enomoto N (2009) Viral factors influencing the response to the combination therapy of peginterferon plus ribavirin in chronic hepatitis C. J Gastroenterol 44(10):1009–1015
Asselah T, Estrabaud E, Bieche I, Lapalus M, De Muynck S, Vidaud M, Saadoun D, Soumelis V, Marcellin P (2010) Hepatitis C: viral and host factors associated with non-response to pegylated interferon plus ribavirin. Liver Int 30(9):1259–1269
Kau A, Vermehren J, Sarrazin C (2008) Treatment predictors of a sustained virologic response in hepatitis B and C. J Hepatol 49(4):634–651
Ge D, Fellay J, Thompson AJ, Simon JS, Shianna KV, Urban TJ, Heinzen EL, Qiu P, Bertelsen AH, Muir AJ, Sulkowski M, McHutchison JG, Goldstein DB (2009) Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature 461(7262):399–401
Rauch A, Kutalik Z, Descombes P, Cai T, Di Iulio J, Mueller T, Bochud M, Battegay M, Bernasconi E, Borovicka J, Colombo S, Cerny A, Dufour JF, Furrer H, Günthard HF, Heim M, Hirschel B, Malinverni R, Moradpour D, Müllhaupt B, Witteck A, Beckmann JS, Berg T, Bergmann S, Negro F, Telenti A, Bochud PY; Swiss Hepatitis C Cohort Study; Swiss HIV Cohort Study (2010) Genetic variation in IL28B is associated with chronic hepatitis C and treatment failure: a genome-wide association study. Gastroenterology 138(4):1338–1345
Suppiah V, Moldovan M, Ahlenstiel G, Berg T, Weltman M, Abate ML, Bassendine M, Spengler U, Dore GJ, Powell E, Riordan S, Sheridan D, Smedile A, Fragomeli V, Müller T, Bahlo M, Stewart GJ, Booth DR, George J (2009) IL28B is associated with response to chronic hepatitis C interferon-alpha and ribavirin therapy. Nat Genet 41(10):1100–1104
Tanaka Y, Nishida N, Sugiyama M, Kurosaki M, Matsuura K, Sakamoto N, Nakagawa M, Korenaga M, Hino K, Hige S, Ito Y, Mita E, Tanaka E, Mochida S, Murawaki Y, Honda M, Sakai A, Hiasa Y, Nishiguchi S, Koike A, Sakaida I, Imamura M, Ito K, Yano K, Masaki N, Sugauchi F, Izumi N, Tokunaga K, Mizokami M (2009) Genome-wide association of IL28B with response to pegylated interferon-alpha and ribavirin therapy for chronic hepatitis C. Nat Genet 41(10):1105–1109
Thompson AJ, Muir AJ, Sulkowski MS, Ge D, Fellay J, Shianna KV, Urban T, Afdhal NH, Jacobson IM, Esteban R, Poordad F, Lawitz EJ, McCone J, Shiffman ML, Galler GW, Lee WM, Reindollar R, King JW, Kwo PY, Ghalib RH, Freilich B, Nyberg LM, Zeuzem S, Poynard T, Vock DM, Pieper KS, Patel K, Tillmann HL, Noviello S, Koury K, Pedicone LD, Brass CA, Albrecht JK, Goldstein DB, McHutchison JG (2010) Interleukin-28B polymorphism improves viral kinetics and is the strongest pretreatment predictor of sustained virologic response in genotype 1 hepatitis C virus. Gastroenterology 139(1):120–129.e18
Jara P, Hierro L, de la Vega A, Díaz C, Camarena C, Frauca E, Miños-Bartolo G, Díez-Dorado R, de Guevara CL, Larrauri J, Rueda M (2008) Efficacy and safety of peginterferon-alpha2b and ribavirin combination therapy in children with chronic hepatitis C infection. Pediatr Infect Dis J 27(2):142–148
Pawłowska M, Pilarczyk M, Halota W (2010) Virologic response to treatment with Pegylated Interferon alfa-2b and Ribavirin for chronic hepatitis C in children. Med Sci Mon 16(12):CR616–CR621
Schwarz KB, Gonzalez-Peralta RP, Murray KF, Molleston JP, Haber BA, Jonas MM, Rosenthal P, Mohan P, Balistreri WF, Narkewicz MR, Smith L, Lobritto SJ, Rossi S, Valsamakis A, Goodman Z, Robuck PR, Barton BA; Peds-C Clinical Research Network (2011) The combination of ribavirin and peginterferon is superior to peginterferon and placebo for children and adolescents with chronic hepatitis C. Gastroenterology 140(2):450–458.e1
Sokal EM, Bourgois A, Stéphenne X, Silveira T, Porta G, Gardovska D, Fischler B, Kelly D (2010) Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection in children and adolescents. J Hepatol 52(6):827–831
Wirth S, Ribes-Koninckx C, Calzado MA, Bortolotti F, Zancan L, Jara P, Shelton M, Kerkar N, Galoppo M, Pedreira A, Rodriguez-Baez N, Ciocca M, Lachaux A, Lacaille F, Lang T, Kullmer U, Huber WD, Gonzalez T, Pollack H, Alonso E, Broue P, Ramakrishna J, Neigut D, Valle-Segarra AD, Hunter B, Goodman Z, Xu CR, Zheng H, Noviello S, Sniukiene V, Brass C, Albrecht JK (2010) High sustained virologic response rates in children with chronic hepatitis C receiving peginterferon alfa-2b plus ribavirin. J Hepatol 52(4):501–507
Al Ali J, Owayed S, Al-Qabandi W, Husain K, Hasan F (2010) Pegylated interferon alfa-2b plus ribavirin for the treatment of chronic hepatitis C genotype 4 in adolescents. Ann Hepatol 9(2):156–160
Ghaffar TY, El Naghy S, El Sebaie H, El Monaiery M, Ghaffar AY (2009) Pegylated alpha interferon 2B plus ribavirin in the treatment of HCV genotype 4 infection. Indian J Pediatr 76(9):895–898
Stättermayer AF, Stauber R, Hofer H, Rutter K, Beinhardt S, Scherzer TM, Zinober K, Datz C, Maieron A, Dulic-Lakovic E, Kessler HH, Steindl-Munda P, Strasser M, Krall C, Ferenci P (2011) Impact of IL28B genotype on the early and sustained virologic response in treatment-naïve patients with chronic hepatitis C. Clin Gastroenterol Hepatol 9(4):344–350.e2
Fried MW, Shiffman ML, Reddy KR, Smith C, Marinos G, Gonçales FL Jr, Häussinger D, Diago M, Carosi G, Dhumeaux D, Craxi A, Lin A, Hoffman J, Yu J (2002) Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med 347(13):975–982
McCarthy JJ, Li JH, Thompson A, Suchindran S, Lao XQ, Patel K, Tillmann HL, Muir AJ, McHutchison JG (2010) Replicated association between an IL28B gene variant and a sustained response to pegylated interferon and ribavirin. Gastroenterology 138(7):2307–2314
Hierro L, Alvarez L, Andueza S, Gordo-Giralt R, Lledin D, Camarena C, de la Vega A, Muñoz-Bartolo G, Frauca E, Diaz C, Jara P (2011) Influence of IL28B gene polymorphisms on sustained response to peginterferon plus ribavirin in children with chronic hepatitis C. J Hepatol 53:524
Thomas DL, Thio CL, Martin MP, Qi Y, Ge D, O’Huigin C, Kidd J, Kidd K, Khakoo SI, Alexander G, Goedert JJ, Kirk GD, Donfield SM, Rosen HR, Tobler LH, Busch MP, McHutchison JG, Goldstein DB, Carrington M (2009) Genetic variation in IL28B and spontaneous clearance of hepatitis C virus. Nature 461(7265):798–801
Ruiz-Extremera A, Muñoz-Gámez JA, Salmerón-Ruiz MA, de Rueda PM, Quiles-Pérez R, Gila-Medina A, Casado J, Belén Martín A, Sanjuan-Nuñez L, Carazo A, Pavón EJ, Ocete-Hita E, León J, Salmerón J (2011) Genetic variation in interleukin 28B with respect to vertical transmission of hepatitis C virus and spontaneous clearance in HCV-infected children. Hepatology 53(6):1830–1838
McHutchison JG, Lawitz EJ, Shiffman ML, Muir AJ, Galler GW, McCone J, Nyberg LM, Lee WM, Ghalib RH, Schiff ER, Galati JS, Bacon BR, Davis MN, Mukhopadhyay P, Koury K, Noviello S, Pedicone LD, Brass CA, Albrecht JK, Sulkowski MS; IDEAL Study Team (2009) Peginterferon alfa-2b or alfa-2a with ribavirin for treatment of hepatitis C infection. N Engl J Med 361(6):580–593
Wirth S, Pieper-Boustani H, Lang T, Ballauff A, Kullmer U, Gerner P, Wintermeyer P, Jenke A (2005) Peginterferon alfa-2b plus ribavirin treatment in children and adolescents with chronic hepatitis C. Hepatology 41(5):1013–1018
Acknowledgments
Financial support: This study was supported by the Ministry of Science and Higher Education (MNiSW, grant no. N402 584440) and Nicolaus Copernicus University (UMK, grant no. MN-4/WL-SD).
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Domagalski, K., Pawłowska, M., Tretyn, A. et al. Impact of IL-28B polymorphisms on pegylated interferon plus ribavirin treatment response in children and adolescents infected with HCV genotypes 1 and 4. Eur J Clin Microbiol Infect Dis 32, 745–754 (2013). https://doi.org/10.1007/s10096-012-1799-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-012-1799-z