
Abstract
Posterior reversible encephalopathy syndrome (PRES) is an acute neurological condition associated with different etiologies, including antibiotic therapy. To date, most data regarding antibiotic-related PRES are limited to case reports and small case series. Here, we report a novel case description and provide a systematic review of the clinico-radiological characteristics and prognosis of available cases of PRES associated with antibiotic therapy. We performed a systematic literature search in PubMed and Scopus from inception to 10 January 2024, following PRISMA guidelines and a predefined protocol. The database search yielded 12 subjects (including our case). We described the case of a 55-year-old female patient with PRES occurring one day after administration of metronidazole and showing elevated serum neurofilament light chain protein levels and favorable outcome. In our systematic review, antibiotic-associated PRES was more frequent in female patients (83.3%). Metronidazole and fluoroquinolones were the most reported antibiotics (33.3% each). Clinical and radiological features were comparable to those of PRES due to other causes. Regarding the prognosis, about one third of the cases were admitted to the intensive care unit, but almost all subjects (90.0%) had a complete or almost complete clinical and radiological recovery after prompt cessation of the causative drug. Antibiotic-associated PRES appears to share most of the characteristics of classic PRES. Given the overall good prognosis of the disease, it is important to promptly diagnose antibiotic-associated PRES and discontinue the causative drug.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Posterior reversible encephalopathy syndrome (PRES) is an acute neurological syndrome associated with subcortical vasogenic oedema, particularly in the posterior parieto-occipital regions. Typical clinical manifestations include non-specific symptoms such as headache and dizziness, but also more severe features such as altered consciousness, visual impairment and seizures [1, 2]. The pathophysiology of PRES is not fully understood yet but appears to be related to dysregulation of cerebral blood flow, cytokine release, disruption of the blood–brain barrier. This may result in endothelial damage and fluid leakage [2]. The posterior regions of the brain appear to be particularly susceptible to hyperperfusion and vasogenic oedema because of the relatively reduced sympathetic innervation in the posterior fossa, and consequently lower autoregulatory potential [1]. Indeed, in the majority of cases (approximately 75–80%) patients diagnosed with PRES showed moderate to severe increase of blood pressure (BP) values [3]. Other conditions that predispose to PRES include eclampsia/pre-eclampsia and renal failure, but also autoimmune or genetic disorders [1, 4,5,6,7]. In addition, the development of PRES may be secondary to the administration of drugs. A recent study based on the World Health Organization (WHO) global pharmacovigilance database identified 152 drugs significantly associated with PRES, most of which were antineoplastic, immunomodulatory, and antimicrobial agents [2]. These agents might cause injury or inhibition of endothelial cell proliferation [2] (Fig. 1).

Clinical features and pathophysiological mechanisms of PRES associated with antibiotic and other drug administration. Disruption of the blood–brain barrier (BBB) with endothelial dysfunction (red box) leads to fluid leakage and vasogenic oedema with or without haemorrhage (blue box) in the central nervous system (CNS) interstitium. Drug intake (e.g., antineoplastic, immunomodulatory, and antimicrobial agents) might cause injury or inhibition of endothelial cell proliferation. Arterial hypertension is also a contributor in PRES pathophysiology. Involved risk factors are represented in red squares. Main clinical manifestations associated with PRES are summarized in the light blue box on the left part of the figure
To date, most data on antibiotic-associated PRES are limited to case reports and small case series. However, given the widespread use of antibiotics in daily clinical practice, it is important to better understand this rare but severe complication of antibiotics. This should also be emphasized in the scenario where non-specific symptoms related to PRES in antibiotic-treated patients may be overlooked and mistakenly attributed to underlying infections as well as other comorbidities that complicate hospitalisation. Furthermore, given the overall good prognosis of PRES with appropriate treatment, it is important to promptly identify potential predisposing factors and discontinue the agent in drug-associated PRES.
Considering all these issues, we aimed to describe a novel case of PRES after metronidazole administration and to perform a systematic review of the clinico-radiological characteristics and prognosis of available cases of PRES associated with antibiotic therapy.
Case description
A 55-year-old woman with no history of immunological, renal or cardiovascular disease was admitted to our neurosurgery department for planned surgical removal of a right vestibular schwannoma causing long-standing right-sided hypoacusis. After the complete removal of the mass, a right-sided peripheral facial nerve palsy (Grade 4, according to the House-Brackmann score) [8] was noted as a postoperative complication. This was treated with eye protection and physiotherapy.
The patient received no antithrombotic or anticoagulant medication before and after surgery.
Two days after successful surgery, the patient complained of abdominal pain and diarrhea. Microbiological testing revealed positive stool samples for Clostridium difficile, for which metronidazole (400 mg × 3/day) was administered. One day after starting metronidazole, the patient developed a diffuse mild headache (numerical rating scale 4/10), dizziness and nausea, followed by altered mental status with somnolence. Neurological examination revealed left-sided homonymous hemianopia without further focal deficits. BP was modestly elevated at clinical onset (158/60 mmHg). Computed tomography (CT) revealed a right occipital intracerebral haemorrhage with peripheral oedema, right subdural and subarachnoid bleeding (Fig. 2A) as well as contralateral grey-white matter junction oedema. Laboratory parameters indicated a mild inflammatory reaction (Supplementary Table 1). Renal function was unremarkable [glomerular filtration rate, GFR > 90 ml/min (normal range > 60), creatinine 62 micromol/L (normal range 44–809) and electrolytes [Na+ 144 mmol/l (normal range 136–145), K+ 4.0 mmol/l (normal range 3.4–4.5), Ca++ 2.19 mmol/l (normal range 2.15–2.50), Cl− 107 (normal range 98–107)]. The patient was therefore admitted to the neurological intensive care unit (ICU) and the arterial hypertension was treated with continuous administration of urapidil and nimodipine. Over the next days, BP values remained normal without the need for intravenous antihypertensive medication. Headache was treated with metamizole and fentanyl transdermal patch. Magnetic resonance imaging (MRI), performed one day after symptom onset, showed subcortical T2, fluid-attenuated inversion recovery (FLAIR) and apparent diffusion coefficient (ADC) hyperintensities in occipital areas (Fig. 2B-C) without diffusion restriction signals reflecting vasogenic oedema (Supplementary Fig. 1). MRI including T2* gradient-echo sequences did not reveal findings associated with cerebral amyloid angiopathy [9]. Based on clinical and radiological findings, the diagnosis of PRES was made [1]. Given the previous association between PRES and metronidazole administration reported in the literature [10,11,12], metronidazole was discontinued 3 days after first administration and replaced by vancomycin (125 mg × 4/die). Neurofilament light chain protein (NfL) was measured in serum using the ELLA technology as previously described [13]. Serum NfL was massively elevated two days after symptom onset (166 pg/ml, normal values < 35 pg/ml according to our in-house reference values). Within 2 days of discontinuing metronidazole, the patient showed rapid clinical improvement with reduction of headache and improvement of mental status. At follow-up (4 days after symptom onset) serum NfL concentration were further increased (433 pg/ml).

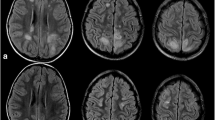
Imaging findings in our case of PRES after metronidazole administration. Native brain CT imaging showed A) right-sided occipital intracerebral haemorrhage with peripheral oedema (thin arrow), subdural bleeding (large arrow); left-sided grey-white matter junction oedema (*). MRI performed 2 days after clinical onset revealed bilateral occipital B) FLAIR (thin arrow and *) and C) ADC hyperintensities (thin arrow and *) indicating vasogenic edema. The relative right occipital hypointensity on the ADC map is related to the haemorrhage. D) Follow-up MRI after 2 months from clinical onset showed in the ADC map almost complete resolution of the vasogenic oedema and subtotal resorption of parenchymal haemorrhage (thin arrow and *). Abbrevations. ADC: apparent diffusion coefficient; CT: computed tomography; FLAIR: fluid-attenuated inversion recovery; MRI: magnetic resonance imaging; PRES: posterior reversible encephalopathy syndrome
After progressive improvement, the patient was discharged 13 days after the onset of PRES without hemianopia or other neurological sequelae, except for the unchanged right facial palsy. Follow-up MRI at approximately 2 months showed almost complete radiological recovery with resolution of the vasogenic oedema and subtotal resorption of parenchymal haemorrhage (Fig. 2D).
Methods
We conducted a systematic study-level meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and a protocol agreed upon by all authors. Four authors (LB, SAR, LD, MF) searched for articles in publicly available literature databases (PubMed, Scopus) from inception to 10th January 2024. The search strategy was based on the combination of antibiotic names listed in the World Health Organization (WHO) Aware, Watch and Reserve (AWaRe) Classification 2021 [14] and "pres" or "posterior reversible encephalopathy syndrome" as either keywords or Medical Subject Heading (MeSH) terms (full search string is provided in the Supplementary materials). Reference lists and citing articles were also reviewed to increase the identification rate of relevant studies. Titles and abstracts were screened independently. Potentially relevant articles were acquired in full text and assessed for eligibility by the same four authors working in pairs. The final selection was shared among all the four authors. Disagreements were resolved by consensus.
Non-original records, studies with no full text available and articles in languages other than English were excluded. In addition, we included only studies that reported: 1) diagnosis of PRES [1, 2]; 2) recent administration of antibiotics and medical indication thereof; 3) information on symptoms and vital parameters at clinical onset; 4) at least one neuroimaging marker supporting the diagnosis of PRES [1, 2].
From the included studies, we extrapolated the following data, if available: 1) general information and clinical history of the patient, including all prescribed drugs and corresponding medical indications; 2) symptoms at clinical onset and after drug withdrawal; 3) vital and laboratory parameters; 4) therapeutic management of PRES; 5) neuroimaging findings at clinical onset and follow-up. The strength of the association between antibiotic prescription and PRES symptoms was assessed through the Naranjo Adverse Drug Reaction Probability Scale (NADRPS) [15].
Results
By using the reported search string (Supplementary materials, Appendix), we identified a total of 232 articles published in literature. After duplicate removal, 187 articles were screened. Title and abstract screening led to the selection of 24 articles for full read, which brought us to a final number of 11 articles fulfilling the inclusion criteria and reporting one case each (Supplementary Table 1) [10,11,12, 16,17,18,19,20,21,22,23]. Full data on literature case reports (n = 11) and on our case are summarized in Table 1 and detailed in Supplementary Table 1.
Demographic and clinical characteristics of reported cases
We performed the final analysis on 12 subjects, including our case. Patients had a mean age of 50.2 years (± standard deviation: 22.3 years; range: 16–87) and were predominantly female (10 of 12, 83.3%). Patients had multiple comorbidities, especially cardiovascular, renal and metabolic diseases (Table 1). The list of all prescribed antibiotics, their indications and other clinical information regarding the cases are reported in detail in Supplementary Table 1 and are summarized in Table 1. No pathogen-specific patterns were found, but gastrointestinal infections were most common (4 of 12, 33.3%). Of note, three articles [10, 11, 18] described the possible association of 2 antibiotics each with PRES. Metronidazole and fluoroquinolones were the most commonly reported antibiotics, each being administered in 4 cases (33.3%) (Table 1). The association between antibiotic administration and PRES, as assessed by the NADRPS score, was considered possible in 11 cases including our case report (NADRPS score 1–4, 91.7%) and probable in 1 case (NADRPS score 5, 8.3%). The types of infection and, when reported, the underlying pathogens were heterogeneous between studies and did not show any specific pattern (Table 1 and Supplementary Table 2).
Clinical, laboratory and radiological findings at clinical onset
PRES manifestations started within one week of antibiotic administration in most cases (7 of 12 reports, 66.7%) and, most commonly, included altered mental status (11 of 12 reports, 91.7%), seizures (7 of 12 studies, 58.3%) and headache (6 of 12 reports, 50.0%), often in combination (Table 1). At presentation, patients often had elevated BP (> 140/90 mmHg) (6 of 12 reports, 50.0%), but PRES also occurred in the setting of normal (90–140/60–90 mmHg) (5 of 12 reports, 41.7%) or decreased BP (< 90/60 mmHg) (1 of 12 reports, 8.3%). Laboratory changes related to the ongoing inflammatory process were found in 7 of 12 reports (58.3%), while electrolyte disturbances and renal dysfunction were described in 4 (33.3%) and 5 of 12 reports (41.7%), respectively. In addition, pathological electroencephalogram (EEG) findings were reported in 4 out of 12 subjects (33.3%). In all cases, MRI performed during the acute phase showed posterior hyperintensities in occipital areas (11 of 12 reports, 91.7%) or the pons (1 of 12, 8.3%), compatible with PRES. Our case was the only one to show lobar haemorrhage occurring together with bilateral vasogenic oedema. ICU admission and mechanical ventilation were required in 4 of 12 (33.3%) and 2 of 12 (16.7%) cases, respectively. Antiepileptic therapy was administered in 5 of 12 patients (41.7%) (Table 1).
Follow-up data
The vast majority of subjects showed significant clinical improvement within a few days after antibiotic cessation, with no neurological sequelae at follow-up (9 out of 10 cases reported, 90.0%, in 2 articles no follow-up data were reported). Furthermore, follow-up imaging showed complete radiological recovery in almost all cases (9 out of 10 reported cases, 90.0%, in 2 articles no follow-up data were reported) (Table 1).
Discussion
In this study, we described a case of PRES associated with recent antibiotic therapy and reviewed similar reports in the literature. Our main findings suggest that PRES associated with antibiotic therapy: 1) can occur at any age and may affect both sexes, with a higher frequency in female patients; 2) is often, but not necessarily, associated with arterial hypertension; 3) occurs within a few days of drug administration, presents with altered mental status and/or seizures, and shows pathological MRI findings in the parieto-occipital areas, as well as heterogeneous EEG changes; 4) may require admission to ICU and mechanical ventilation in about one third of cases, but in the vast majority of patients show complete or almost complete clinical and radiological recovery after prompt discontinuation of the drug; 5) may not be antibiotic or pathogen specific, although metronidazole and fluoroquinolones were the most commonly reported antibiotics.
Overall, our findings are in line with previous literature on the pathophysiological and clinical features of PRES; indeed, previous studies reported also on the female predominance in drug-associated PRES cases [2]. Further, the elevation of arterial BP is thought to be the driving pathological mechanism in most cases of PRES, leading to cerebral hyper-perfusion [1]. In our study, the frequencies of patients with hyper-, normo- and hypotension well reflects those of previous reports (i.e., approximately 30–50% of PRES cases without elevated BP values) [3]. In addition, altered mental status (92%), headache (50%) and seizures (58%) were common findings in the patient group analyzed, largely reflecting the prevalences reported in other PRES cohorts [1, 5, 24,25,26]. To date, there are no data to support specific antiepileptic treatment regimens for PRES compared with those used in other conditions. Furthermore, although seizures in PRES may be associated with a worse clinical outcome [26] in most cases they do not recur [27]. Prospective studies are therefore urgently needed to assess the impact of antiepileptic therapy on outcomes in PRES.
Brain MRI is currently the gold standard for the diagnosis of PRES [1]. Although parieto-occipital hyperintensities are the classic neuroradiological features of PRES [1], concomitant intraparenchymal or subarachnoid haemorrhages, like in our case report, have been described in literature in patients with PRES not associated with antibiotics [24, 28,29,30,31]. Our reported case is therefore peculiar because it is the first to be described. As previously hypothesised, reperfusion injury due to vasoconstriction or pial rupture secondary to hypertension appears to be the leading pathogenic mechanism in PRES-associated intracranial haemorrhage [24].
NfL is a marker of neuroaxonal damage in primary and non-primary neurological diseases [32]. To date, only one study has investigated and demonstrated an increase in serum NfL in patients with PRES [33]. Our case report supports these observations, but we cannot exclude the significant confounding effects of cerebral haemorrhage and neurosurgical treatment on NfL concentrations as described previously [13, 34].
Regarding the prognosis, most cases of PRES associated with antibiotic therapy or other drugs showed a complete or almost complete clinical recovery [35], however also permanent disability and death have been reported in few cases [36].
Of note, metronidazole and fluoroquinolones turned out to be the antibiotics more frequently associated with PRES in our systematic review. Some authors have hypothesized that metronidazole treatment may lead to autonomic dysfunction and, thus, to PRES. Indeed, a case of metronidazole-induced sympathetic autonomic dysfunction has been described [37]. Interestingly, metronidazole therapy has previously been related also to another neurological syndrome, namely metronidazole-induced encephalopathy (MIE). Indeed, MIE can present with encephalopathic symptoms as well as seizures mimicking PRES [38]. However, unlike PRES, MIE often occurs weeks/months after drug ingestion, presenting primarily with motor symptoms (e.g., dysarthria, postural instability, and oculomotor dysfunction) due to the involvement of cerebellar and brainstem structures [38]. In addition, in MIE, MRI shows characteristic reversible symmetrical T2/FLAIR hyperintense lesions of the dentate nuclei in the vast majority of patients [38]. Taking in to account these findings, we suggest that a misdiagnosis might possibly explain the low number of PRES cases associated with metronidazole prescription in studies of pharmacovigilance databases [38].
With regard to fluoroquinolones, these drugs are known to cause central and peripheral neurotoxicity with variousmanifestations such as headache and seizures [39], but the underlying mechanisms of fluoroquinolone-associated PRES remain unclear [12]. Nevertheless, given the frequent use of these antibiotics and the relatively modest absolute risk of adverse neurological effects following fluoroquinolone administration [39], it is important to consider PRES early in the differential diagnosis of acute neurological symptoms emerging on this therapy. Furthermore, in clinical practice it can sometimes be difficult to understand whether the antiinfective therapy or a specific infectious disease itself is the trigger of PRES. For example, in a literature case of PRES in a human immunodeficiency virus (HIV)-infected patient on antiretroviral therapy, both the pathogen and the drug were discussed to play a pathogenic role [40].
The main limitation of our review is its retrospective nature; therefore, our findings should be confirmed by pharmacovigilance investigations, or by prospective or translational studies to identify the pathophysiological mechanisms underlying antibiotic-associated PRES. Moreover, further studies on PRES associated with other classes of drugs, especially antiviral and antineoplastic agents, are needed.
In conclusion, the occurrence of acute or subacute neurological symptoms after antibiotic treatment should raise the clinical suspicion towards PRES. MIE should be considered in the differential diagnosis in case of metronidazole prescription [41]. Brain MRI allows rapid and accurate identification of vasogenic oedema consistent with PRES, which could otherwise be missed on CT alone. Indeed, in our case description, the peculiar presence of concomitant intracerebral haemorrhage could have been misleading without advanced imaging. Early recognition and appropriate management of PRES is necessary to eliminate any predisposing causes. This would lead to a shorter recovery time, reduced need for intensive care and overall better clinical outcomes.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Fugate JE, Rabinstein AA (2015) Posterior reversible encephalopathy syndrome: clinical and radiological manifestations, pathophysiology, and outstanding questions. Lancet Neurol 14:914–925. https://doi.org/10.1016/S1474-4422(15)00111-8
Balcerac A, Bihan K, Psimaras D, Lebrun-Vignes B, Salem JE, Weiss N (2023) Drugs associated with posterior reversible encephalopathy syndrome, a worldwide signal detection study. J Neurol 270:975–985. https://doi.org/10.1007/s00415-022-11450-y
Rabinstein AA, Mandrekar J, Merrell R, Kozak OS, Durosaro O, Fugate JE (2012) Blood pressure fluctuations in posterior reversible encephalopathy syndrome. J Stroke Cerebrovasc Dis 21:254–258. https://doi.org/10.1016/j.jstrokecerebrovasdis.2011.03.011
Mueller-Mang C, Mang T, Pirker A, Klein K, Prchla C, Prayer D (2009) Posterior reversible encephalopathy syndrome: do predisposing risk factors make a difference in MRI appearance? Neuroradiology 51:373–383. https://doi.org/10.1007/s00234-009-0504-0
Fugate JE, Claassen DO, Cloft HJ, Kallmes DF, Kozak OS, Rabinstein AA (2010) Posterior reversible encephalopathy syndrome: associated clinical and radiologic findings. Mayo Clin Proc 85:427–432. https://doi.org/10.4065/mcp.2009.0590
Shaharir SS, Remli R, Marwan AA, Said MS, Kong NC (2013) Posterior reversible encephalopathy syndrome in systemic lupus erythematosus: pooled analysis of the literature reviews and report of six new cases. Lupus 22:492–496. https://doi.org/10.1177/0961203313478303
Cani I, Righini M, Cenni P, Foschi M (2022) Teaching NeuroImage: Partially Reversible Widespread Leukoencephalopathy Associated With Atypical Hemolytic Uremic Syndrome. Neurology 99:1128–1129. https://doi.org/10.1212/WNL.0000000000201378
House JW, Brackmann DE (1985) Facial nerve grading system. Otolaryngol Head Neck Surg 93(2):146–147. https://doi.org/10.1177/019459988509300202
Charidimou A, Boulouis G, Frosch MP, Baron JC, Pasi M, Albucher JF, Banerjee G, Barbato C, Bonneville F, Brandner S, Calviere L, Caparros F, Casolla B, Cordonnier C, Delisle MB, Deramecourt V, Dichgans M, Gokcal E, Herms J, Hernandez-Guillamon M, Jäger HR, Jaunmuktane Z, Linn J, Martinez-Ramirez S, Martínez-Sáez E, Mawrin C, Montaner J, Moulin S, Olivot JM, Piazza F, Puy L, Raposo N, Rodrigues MA, Roeber S, Romero JR, Samarasekera N, Schneider JA, Schreiber S, Schreiber F, Schwall C, Smith C, Szalardy L, Varlet P, Viguier A, Wardlaw JM, Warren A, Wollenweber FA, Zedde M, van Buchem MA, Gurol ME, Viswanathan A, Al-Shahi Salman R, Smith EE, Werring DJ, Greenberg SM (2022) The Boston criteria version 2.0 for cerebral amyloid angiopathy: a multicentre, retrospective. MRI-neuropathology diagnostic accuracy study. Lancet Neurol. 21(8):714–725
Kikuchi S, Orii F, Maemoto A, Ashida T (2016) Reversible Posterior Leukoencephalopathy Syndrome Associated with Treatment for Acute Exacerbation of Ulcerative Colitis. Intern Med 55:473–477. https://doi.org/10.2169/internalmedicine.55.5250
Gilbert BW, Gabriel A, Velazquez L (2020) A Case of Antibiotic-Induced Posterior Reversible Encephalopathy Syndrome. Hosp Pharm 55:338–341. https://doi.org/10.1177/0018578719844706
Hosaka T, Terada M, Okubo K, Iwabuchi S, Kajii E (2023) Management of a rare case of metronidazole-induced encephalopathy presenting as posterior reversible encephalopathy syndrome: a case report. Neurol Sci 44:1101–1103. https://doi.org/10.1007/s10072-022-06480-3
Abu-Rumeileh S, Barba L, Bache M, Halbgebauer S, Oeckl P, Steinacker P, Güttler A, Keßler J, Illert J, Strauss C, Vordermark D, Otto M (2023) Plasma β-synuclein, GFAP, and neurofilaments in patients with malignant gliomas undergoing surgical and adjuvant therapy. Ann Clin Transl Neurol 10:1924–1930. https://doi.org/10.1002/acn3.51878
World Health Organization (WHO) Aware, Watch and Reserve (AWaRe) Classification 2021 (2021) https://www.who.int/publications/i/item/2021-aware-classification
Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, Janecek E, Domecq C, Greenblatt DJ (1981) A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther 30:239–245. https://doi.org/10.1038/clpt.1981.154
Tomar LR, Pandita N, Arya S, Agrawal C (2022) Linezolid-Associated Posterior Reversible Leuco-encephalopathy Syndrome in a Patient with Disseminated Tuberculosis. Trop Doct 52:196–198. https://doi.org/10.1177/00494755211053194
Ali WH. Ciprofloxacin-associated posterior reversible encephalopathy (2013) BMJ Case Rep:bcr2013008636. https://doi.org/10.1136/bcr-2013-008636.
Bitar De Zayas-Enriquez A, Soper C (2019) Daptomycin-Induced Posterior Reversible Encephalopathy Syndrome (PRES). Case Rep Neurol Med 2019:8756932. https://doi.org/10.1155/2019/8756932
Cordeanu EM, Gaertner S, Faller A, Mirea C, Lessinger JM, Kemmel V, Stephan D (2017) Rifampicin reverses nicardipine effect inducing uncontrolled essential hypertension. Fundam Clin Pharmacol 31:587–589. https://doi.org/10.1111/fcp.12292
Kim L, Kolar L, Abu A, Wu LJ (2021) Posterior Reversible Encephalopathy Syndrome in a Case of Vancomycin-Induced Acute Kidney Injury. J Clin Neurol 17:140–141. https://doi.org/10.3988/jcn.2021.17.1.140
Nagel S, Köhrmann M, Huttner HB, Storch-Hagenlocher B, Schwab S (2007) Linezolid-induced posterior reversible leukoencephalopathy syndrome. Arch Neurol 64:746–748. https://doi.org/10.1001/archneur.64.5.746
Nasu K, Fujisawa M, Kato H, Nangaku M (2017) Three cases of posterior reversible encephalopathy syndrome with chronic kidney disease triggered by infection. Nephrology (Carlton) 22:322–325. https://doi.org/10.1111/nep.12930
Reyes HA, Witsch J, Sueldo C, Hong J (2017) Posterior reversible encephalopathy in an adult patient with poststreptococcal glomerulonephritis. BMJ Case Rep :bcr2017220043. https://doi.org/10.1136/bcr-2017-220043.
Triplett JD, Kutlubaev MA, Kermode AG, Hardy T (2022) Posterior reversible encephalopathy syndrome (PRES): diagnosis and management. Pract Neurol 22:183–189. https://doi.org/10.1136/practneurol-2021-003194
Liman TG, Bohner G, Heuschmann PU, Endres M, Siebert E (2012) The clinical and radiological spectrum of posterior reversible encephalopathy syndrome: the retrospective Berlin PRES study. J Neurol 259:155–164. https://doi.org/10.1007/s00415-011-6152-4
Bastide L, Legros B, Rampal N, Gilmore EJ, Hirsch LJ, Gaspard N (2018) Clinical Correlates of Periodic Discharges and Nonconvulsive Seizures in Posterior Reversible Encephalopathy Syndrome (PRES). Neurocrit Care 29:481–490. https://doi.org/10.1007/s12028-018-0548-2
Kastrup O, Gerwig M, Frings M, Diener HC (2012) Posterior reversible encephalopathy syndrome (PRES): electroencephalographic findings and seizure patterns. J Neurol 259:1383–1389. https://doi.org/10.1007/s00415-011-6362-9
Cordelli DM, Masetti R, Ricci E, Toni F, Zama D, Maffei M, Gentili A, Parmeggiani A, Pession A, Franzoni E (2014) Life-threatening complications of posterior reversible encephalopathy syndrome in children. Eur J Paediatr Neurol 18:632–640. https://doi.org/10.1016/j.ejpn.2014.04.014
Pilato F, Calandrelli R, Distefano M, Panfili M, Della Marca G, Colosimo C (2019) Acute radiological pattern and outcome in posterior reversible encephalopathy syndrome patients. Clin Neurol Neurosurg 185:105459. https://doi.org/10.1016/j.clineuro.2019.105459
Vallone MG, Vázquez C, Pigretti S, Oses LL, Angriman F, Zurru MC (2020) Clinical Presentation and Risk Factors for Poor Outcomes Among Adult Patients With Posterior Reversible Encephalopathy Syndrome: A Retrospective Cohort Study. Neurologist 25:162–167. https://doi.org/10.1097/NRL.0000000000000294
Appiani F, Claverie CS, Klein FR (2023) Posterior Reversible Leukoencephalopathy With Hemorrhagic Features: A Case Series. Cureus 15(11):e49587. https://doi.org/10.7759/cureus.49587
Abu-Rumeileh S, Abdelhak A, Foschi M, D’Anna L, Russo M, Steinacker P, Kuhle J, Tumani H, Blennow K, Otto M (2023) The multifaceted role of neurofilament light chain protein in non-primary neurological diseases. Brain 146(2):421–437. https://doi.org/10.1093/brain/awac328
Fang X, Liang Y, Zhang W, Wang Q, Chen J, Chen J, Lin Y, Chen Y, Yu L, Wang H, Chen D (2021) Serum Neurofilament Light: a Potential Diagnostic and Prognostic Biomarker in Obstetric Posterior Reversible Encephalopathy Syndrome. Mol Neurobiol 58:6460–6470. https://doi.org/10.1007/s12035-021-02562-z
Zheng P, Wang X, Chen J, Wang X, Shi SX, Shi K (2023) Plasma Neurofilament Light Chain Predicts Mortality and Long-Term Neurological Outcomes in Patients with Intracerebral Hemorrhage. Aging Dis 14(2):560–571
Tlemsani C, Mir O, Boudou-Rouquette P, Huillard O, Maley K, Ropert S, Coriat R, Goldwasser F (2011) Posterior reversible encephalopathy syndrome induced by anti-VEGF agents. Target Oncol 6:253–258. https://doi.org/10.1007/s11523-011-0201-x
Legriel S, Schraub O, Azoulay E, Hantson P, Magalhaes E, Coquet I, Bretonniere C, Gilhodes O, Anguel N, Megarbane B, Benayoun L, Schnell D, Plantefeve G, Charpentier J, Argaud L, Mourvillier B, Galbois A, Chalumeau-Lemoine L, Rivoal M, Durand F, Geffroy A, Simon M, Stoclin A, Pallot JL, Arbelot C, Nyunga M, Lesieur O, Troché G, Bruneel F, Cordoliani YS, Bedos JP, Pico F, Critically III Posterior Reversible Encephalopathy Syndrome Study Group (CYPRESS) (2012) Determinants of recovery from severe posterior reversible encephalopathy syndrome. PLoS One 7:e44534. https://doi.org/10.1371/journal.pone.0044534
Hobson-Webb LD, Roach ES, Donofrio PD (2006) Metronidazole: newly recognized cause of autonomic neuropathy. J Child Neurol 21(5):429–431. https://doi.org/10.1177/08830738060210051201
Sørensen CG, Karlsson WK, Amin FM, Lindelof M (2020) Metronidazole-induced encephalopathy: a systematic review. J Neurol 267:1–13. https://doi.org/10.1007/s00415-018-9147-6
Ellis DE, Hubbard RA, Willis AW, Zuppa AF, Zaoutis TE, Hennessy S (2021) Comparative neurological safety of fluoroquinolones versus therapeutic alternatives. Pharmacoepidemiol Drug Saf 30(6):797–805. https://doi.org/10.1002/pds.5219
Birner B, Hirzel C, Wagner F, Waldegg G (2018) Posterior reversible encephalopathy syndrome in an HIV-infected patient on antiretroviral treatment: what is the risk factor? BMJ Case Rep 2018:bcr2017221998. https://doi.org/10.1136/bcr-2017-221998
Bhattacharyya S, Darby RR, Raibagkar P, Gonzalez Castro LN, Berkowitz AL (2016) Antibiotic-associated encephalopathy. Neurology 86:963–971. https://doi.org/10.1212/WNL.0000000000002455
Acknowledgements
We are indebted to the staff of the Neurology Laboratory of Halle University Hospital. LB received research support from the Medical Faculty of Martin-Luther-University Halle-Wittenberg (Junior Clinician Scientist Programm No. JCS24/02). SAR received research support from the Medical Faculty of Martin-Luther-University Halle-Wittenberg (Clinician ScientistProgramm No. CS22/06).
Funding
Open Access funding enabled and organized by Projekt DEAL. No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
Lorenzo Barba, Carmelo Carrubba, Alexander Mensch and Samir Abu-Rumeileh contributed to the study conception and design. All authors performed the literature search and/or data analysis. The first draft of the manuscript was written by Lorenzo Barba, Carmelo Carrubba, Alexander Mensch and Samir Abu-Rumeileh and all authors commented on previous versions of the manuscript. All authors critically revised the final manuscript.
Corresponding author
Ethics declarations
Research involving human participants and/or animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This is a case report including one patient and a literature review. No ethical approval is required.
Disclosure of potential conflicts of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Informed consent
The patient included in this study provided informed consent for the publication of anonymized data in accordance with the declaration of Helsinki.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Alexander Mensch and Samir Abu-Rumeileh shared last co-authorship.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Barba, L., Carrubba, C., Spindler, K. et al. Posterior reversible encephalopathy syndrome associated with antibiotic therapy: a case report and systematic review. Neurol Sci (2024). https://doi.org/10.1007/s10072-024-07545-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10072-024-07545-1