
Abstract
Objective
The aim of this systematic review (SR) was to gather all available epidemiological evidence on former participation in any type of sport, at a professional and varsity level, as a potential risk factor for neurodegenerative diseases (NDs) and neurocognitive disorders (NCDs).
Design
Systematic searches were performed on PubMed, the Cochrane databases, and the ISI Web of Knowledge databases. Included studies were assessed using the NOS checklist.
Eligibility criteria for selecting studies
All epidemiological studies reporting data on the possible association between a clinical diagnosis of amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND), dementia or mild cognitive impairment (MCI), Parkinson’s disease (PD), chronic traumatic encephalopathy (CTE) at any stage and with any clinical pattern and the former participation in any types of sport at a varsity and professional level were included.
Results
Data from the 17 included studies showed a higher frequency of NDs and NCDs in former soccer and American football players. Updating the previous SR confirmed a higher frequency of ALS/MND in former soccer players. Data reported a significantly higher risk of dementia/AD in former soccer players, and of MCI in former American football players. Results also showed a significantly higher risk of PD in former soccer and American football players, and a significantly higher risk of CTE in former boxers and American football players.
Summary/conclusions
This SR confirmed a higher risk of NDs and NCDs in former professional/varsity athletes. However, the pathological mechanisms underlying this association remain unclear, and further high-quality studies should be performed to clarify whether the association could be sport specific.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Previous epidemiological studies reported an association between professional sport and neurodegenerative diseases (NDs) and neurocognitive disorders (NCDs). These include a range of conditions primarily affecting brain and central nervous system (CNS) functioning [1, 2]. NDs are multifactorial, still incurable, and debilitating conditions resulting in the progressive degeneration and/or death of nerve cells [1]. The pathophysiological mechanisms underlying these conditions can differ, causing deficits ranging from memory loss and cognitive impairment to movement and gait deficits and impairments in language and breathing abilities [3]. Amyotrophic lateral sclerosis (ALS) represents the most common motor neuron disease (MND) and described as a rare progressive neuromuscular disease, typically causes the degeneration of both the upper and lower motor neurons but may also include cognitive and behavioral symptoms [4,5,6]. Parkinson’s disease (PD) is primarily characterized by a specific set of motor symptoms, including tremor, rigidity, and bradykinesia, and by an impairment of balance and postural reflexes. It can also cause several non-motor symptoms, such as gastrointestinal and urogenital disorders, and psychiatric symptoms, including depression [7]. NCDs is a broad term for defining several different chronic and progressive conditions affecting the ability to think, remember and make decisions. Symptoms may vary according to the type and severity of disease, and include memory loss, attention and communication deficits, and impairments in the ability to reason and solve problems [8, 9]. According to the DSM-5 dementia and mild NCD (MCI) are the main categories of NCDs. As for dementia, some subtypes are included among NDs, as they are caused by neurodegenerative mechanisms, while some types of dementia and other NCDs can be due to other causes, including secondary causes as intoxication or trauma [2]. The most common cause of ND dementia is Alzheimer's disease (AD), which is characterized by memory loss and specific deficits in language, sensory, motor and/or executive functions [8, 10]. Among the risk factors for dementia, the most known are genetic factors and aging. However, gender, educational level, and some health conditions are also included among risk factors [11].
Some studies investigated previous participation in some contact sports as a potential risk factor for neurodegenerative diseases (ND) and neurocognitive disorders (NCD) [12,13,14] focusing on pathological changes in former players [15, 16] in particular, soccer [14, 17,18,19,20,21] and American football players [12, 13]. Some small studies and reports have suggested that sports involving repeated traumatic brain injuries (TBI) may cause a long-term risk of NDs [22]. When considering specific NDs or NCDs, a relatively recent systematic review reported a significantly higher frequency of ALS in former professional and varsity soccer, and American football players [23]. The most frequently investigated potential sport-related risk factors for ALS and for all other NDs and NCDs, include multiple trauma and concussion [24, 25] along with oxidative stress [26] and exposure to toxic substances/chemicals (e.g., pesticides) [27, 28] or drugs/dietary supplements [28]. However, as for ALS, a more recent hypothesis also suggested that former athletes might share a phenotype causing simultaneously a higher athletic predisposition, with lower body mass index (BMI) and cardiovascular risk and higher physical fitness, and a higher risk of ALS [28, 29]. Another relatively recent systematic review, specifically focusing on long-term consequences of repeated concussions, reported that former participants in contact, collision, and combat sports seem to be at an increased risk of cognitive impairment and other mental health problems [30]. The review reported a higher frequency of cognitive decline and some NCDs and NDs in former professional athletes, considering NDs/NCDs along with diseases of the nervous system and sense organs, and other mental health conditions, including suicide and cognitive decline, hypothesizing multiple trauma and head injuries as potential causes of such condition. Multiple concussion and trauma and their potential role in the long-term onset of NDs or NCDs have been widely investigated, and are still a matter of debate, particularly in relation to popular sports such as soccer and rugby [31]. However, even though repeated head trauma has been linked to irreversible cognitive deficits [32,33,34] the pathophysiological mechanisms underlying this potential association are still to be clarified.
Traditionally, multiple concussion and head trauma had been known to cause the so-called ‘‘punch-drunk syndrome’’ firstly descripted in 1928 in retired boxers [35] which was associated to a basic lesion due to traumatic multiple hemorrhages, and replaced few years later by the wording ‘‘Dementia pugilistica’’ term coined in 1937 and which took into consideration in its definition the hypothesis of a type of dementia induced by brain trauma [36]. In the following decades, the scientific community focused the attention on the possible association between this type of sport and NDs, suggesting an etiological link between exposure to repeated head trauma and concussion and dementia and/or PD, even hypothesizing synergistic effects between head trauma and apolipoprotein-epsilon four in patients with Alzheimer's disease [37, 38]. In recent times, although the debate is still open, a study investigated the association between the former participation in contact and collision sports such as American football, boxing, soccer, rugby, and hockey, and a higher risk of chronic traumatic encephalopathy (CTE), highlighting a strong dose–response relationship between the duration of American football played and this pathology [39].
Based on all these hypotheses, evidence seems to suggest an association between former participation in professional sports, and mainly in contact and collision sports, with a higher risk of NDs or NCDs. Therefore, the aim of this systematic review (SR) was to gather all available epidemiological evidence on former participation in any type of sport, at a professional and varsity level, as a potential risk factor for NDs or NCDs.
Materials and methods
This SR was performed following the methodology of the Cochrane handbook for SRs [40] and reported based on the PRISMA statement for reporting SRs and meta-analyses [41]. Systematic searches for all available literature up to February 1, 2022, were performed on PubMed, the Cochrane Databases (that gives access to: Cochrane Database of Systematic Reviews, Embase, PubMed, CT.gov, ICTRP and CINAHL), and ISI Web of Knowlegde (that gives access to: Science Citation Index, Social Sciences Citation Index, Arts and Humanities Citation Index, Emerging Sources Citation Index, Conference Proceedings Citation Index–Science, Conference Proceedings Citation Index-Social Sciences and Humanities, Book Citation Index–Science, Book Citation Index–Social Sciences and Humanities, Current Chemical Reactions, and Index Chemicus). The following terms were used: ((neurodegenerative* OR neuro-degenerative* OR “amyotrophic lateral sclerosis” OR ALS OR “motor neuron disease” OR “motor neuron diseases” OR “motor-neuron disease” OR “motor-neuron diseases” OR parkinson* OR parkinsonism* OR Alzheimer* OR dementia* OR encephalopath* OR ((cognitive OR neurocognitive OR neuro-cognitive) AND (impairment* OR degenerati* OR disord*))) AND (((professional* OR competitive* OR competition* OR elite* OR varsity* OR college* OR “high school” OR “high-school”) AND (sport* OR player*)) OR athlete* OR rider* OR fighter* OR boxeur* OR boxer* OR runner* OR skier* OR rower* OR “martial art” OR “martial arts” OR “martial artist” OR “martial artists” OR “combat sport” OR “combat sports” OR “players”)). Further relevant articles were also identified by reviewing the references of considered studies. No limitations were applied for date of publication nor study design; only studies published in English were considered. Retrieved literature was screened by two independent reviewers (GB, PP), and studies were selected based on their pertinence and relevance to the topic of the review. The full texts of selected studies were assessed for inclusion by applying the following predefined eligibility criteria. Potential disagreements were resolved by discussion or, where needed, involvement of a third reviewer (EL). All case–control and cohort studies addressing the possible association between any types of sport practiced as a varsity and/or a professional athlete and the risk of NDs and/or NCDs, were included. Since studies on this topic are performed using any type of available data, including data from structured information sources, ranging from death certificates to biological tissue banks, we included all studies reporting a diagnosis of any of the considered condition based on any type of criteria, including clinical criteria and neurobiological criteria. Therefore, all studies reporting by any means (e.g., death certificates, clinical records) a clinical, neurobiological or neuropathological diagnosis of ALS or motor neuron disease (MND), dementia of any type or mild cognitive impairment (MCI), PD, CTE at any state of disease and with any clinical pattern were also included considering the wider diagnostic category. Case reports, case series, non-systematic or narrative reviews, letters, commentaries, and editorials were excluded. Only epidemiological studies (i.e., cohort and case–control) reporting data on the frequency of any of the considered NDs and/or NCDs were included.
For studies analyzing the association between professional and/or varsity sports and ALS, we updated a previously published systematic review [23] therefore only studies published from January 2016 to February 2022 were included.
Studies meeting the eligibility criteria were qualitatively assessed using the Newcastle–Ottawa Scale (NOS) for quality assessment of non-randomized studies [42]. The NOS scale is structured in 8 items assessing the adequacy of 3 major domains: selection of the study group, comparability of the groups, and ascertainment of the exposure of interest for case–control studies or of the outcome of interest for cohort studies. A maximum of 9 stars can be assigned to each assessed study, and specifically a maximum of 4 stars for the Selection domain, 2 stars for the Comparability domain, and 3 stars for either the Outcome or the Exposure domain. The potential presence of other biases and/or methodological flaws was also considered in assessing the included studies. Data were extracted using structured tables. Specific information was gathered on the type of sport considered by each study, along with how the enrolled population of athletes was defined, and on the diagnostic criteria and procedure used to define the identified cases. Moreover, for cohort studies, specific information was also extracted on the source of the reference population. Gathered information also included study design, year of publication, characteristics of the included population, definition of the exposure(s), diagnostic criteria, length of the follow-up, and results for each analysis.
Results
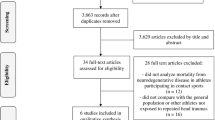
Structured search on bibliographic databases yielded 11,189 articles. Two further studies were identified by reviewing the bibliographic references of included studies [43, 44]. After selection based on the pertinence and relevance to the topic of the review, 11,191 records were excluded, leaving 47 articles meeting the selection criteria. The full texts of the selected articles were assessed for inclusion, and 30 further articles were excluded as 3 were case reports [17, 19, 45], 1 review [46], 1 reported participation in sports as a leisure activity [47] 2 reported data only on an overall measure of physical activity [48, 49] 2 included only athletes who had ≥ 1 head/brain injury [50, 51] 8 did not report any measure of risk of NDs and/or NCDs [20, 52,53,54,55,56,57,58] and 13 were already included in the 2016 review [59,60,61,62,63,64,65,66,67,68,69,70,71].
The flow diagram of the literature is reported in Fig. 1.

Flow diagram of literature
A total of 17 articles were included in the qualitative summary [43, 44, 72,73,74,75,76,77,78,79,80,81,82,83,84,85,86].
Overall, five cohort studies reported data on the frequency of all NDs/NCDs included in this review in former professional or varsity athletes [74, 77, 79, 82, 84]. Considering each single pathology, 10 cohort studies [82, 84] and 1 case–control study [44] reported data on the frequency of dementia/MCI in former athletes, 8 cohort studies [43, 73,74,75, 77, 79, 82, 84], and 1 case–control study [44] reported data on the frequency of PD or Parkinsonism, 1 cohort study [80] reported data on CTE, and 7 new cohort studies [77, 82,83,84,85,86] and 1 new case–control study [81] reported data on the frequency of ALS or MND. The summary of the main characteristics, quality assessment and results from the included studies were reported according to each considered outcome in Tables 1, 2, 3, 4, and 5.
Methodological quality
The overall methodological quality of included studies was moderate. The highest score achieved was 7, while the lowest score was 3. Five cohort studies achieved a score of 7 [43, 74, 75, 84, 86] while 4 studies, 3 cohort [79,80,81] and 1 case–control [44] were assigned 6 stars, 2 cohort studies were assigned 5 stars [73, 77], 5 studies, 4 cohort [72, 76, 78, 83] and 1 case–control [81] were assigned 4 stars, and 1 cohort study [85] was assigned 3 stars.
Selection
Only two cohort studies reached 4 stars, which is the highest possible score, in this domain, while most studies were scored 2 stars. All included cohort studies enrolled professional or varsity athletes from secure records (e.g., sports leagues, yearbooks), thus the enrolled exposed cohort is often adequately defined and representative, and data on exposure are drawn from secure sources. However, the unexposed cohort is often enrolled from different sources from the exposed cohort, and most of the studies did not or could not (e.g., studies using census data) provide information on the absence of the outcome at the beginning of the study.
As for the two case–control studies, cases were enrolled through either registries or death certificates. Therefore, samples were representative, but the definition of cases did not have an independent validation. In both studies, controls were enrolled from the community, as they were either randomly selected from general population or selected among death certificates due to other non-degenerative causes. However, both studies could not and did not ascertain the absence of the outcome at the start of the study.
Comparability
Most studies reached 2 stars (n = 8), which is the highest possible score, in this domain, while 6 studies were assigned 1 star, and 2 studies had no stars [73, 80]. Most studies were either matched or had the analysis adjusted for age [72, 76,77,78, 83] and/or for other variables. In some studies, matched controls were selected from general population, while in some other studies controls were either other athletes [77,78,79] or students from the same schools [75]. In case–control studies, controls were either matched for sex, age, and province of residence [81] or selected based on the availability of enough information for adjusting all analyses [44].
Exposure/outcome
Only 2 cohort studies reached 3 stars in this domain, which is the highest possible score [80, 86] while 6 studies had 2 stars, 6 studies had 1 star, and 1 case–control study and 1 cohort study had no stars [81, 85].
Most of the cohort studies used structured information from death certificates, clinical records, registries, or record-linkage. Of the five remaining studies, 2 studies obtained data on the outcome by clinicians [72, 78] 2 from questionnaires [73, 77] and 2 only from databases or search engines (i.e., PubMed, Google) or books and magazines [83, 85]. Using secure sources such as hospital records and certificates or using an independent validation of the diagnosis to confirm the outcome can minimize the potential for inaccurate information. However, even if death certificates are an extremely valuable source of data, their accuracy in reporting deaths due to NDs/NCDs can be inaccurate. In fact, deaths due to the considered NDs/NCDs were shown to be underreported as primary cause of death [87,88,89,90,91,92,93,94] and studies on mortality are often of poor methodological quality [95].
Moreover, most of the included studies used, for all the considered outcomes, widely heterogeneous diagnostic criteria. Using a heterogeneous set of criteria prevent the direct comparison of data, as different criteria can lead to different prevalence and incidence rates [96,97,98].
Another issue was the length of the follow-up, as at least part of the included sample in most studies using administrative data had a follow-up length insufficient to observe the considered outcome.
As for case–control studies, one [44] had a secure source for ascertaining the exposure, while the other [81] used an unstructured questionnaire and did not use the same method for cases and controls. Moreover, neither reported the response rate for both cases and controls. Moreover, most of the studies did not report the number of participants lost to follow-up.
Qualitative analysis
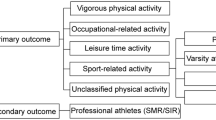
Results from the included studies were reported according to outcome. A summary of the characteristics and results from each study are reported in Tables 1, 2, 3, 4, and 5.
All NDs/NCDs
Only 5 cohort studies reported data on the overall risk of any type of NDs and/or NCDs in former professional/varsity athletes. Specifically, 3 of the 5 cohort studies reported the risk of NDs/NCDs in either former professional American football players [74, 79] or former varsity American football players [77] while the remaining 2 studies reported the risk of NDs/NCDs in former professional soccer players [82, 84]. Both studies on professional American football players enrolled former players from the National Football League (NFL) and used death certificates to calculate their risk of death due to NDs/NCDs as underlying (U) and/or contributing (C) cause of death. The studies reported an overall higher standardized mortality ratio (SMR) due to NDs/NCDs in former NFL players (SMR-U 2.83, 95%CI 1.36–5.21; SMR-U&C 3.26, 95%CI 1.90–5.22) [74] with a specifically higher risk of NDs/NCDs in former NFL players compared to baseball players (HR-U 2.07, 95%CI 1.01–4.23; HR-U&C 2.99, 95%CI 1.64–5.45) [79]. A significantly higher risk of death due to NDs/NCDs was also observed in the 2 studies enrolling former professional soccer players, with HRs ranging from 3.53 to 4.10 (HR-U 4.10, 95%CI 2.88–5.83; HR-U&C 3.53, 95%CI 2.72–4.57; HR 3.66, 95%CI 2.88–4.65) [82, 84]. No risk measure was calculated for former varsity athletes, but the study observed that 3% of the enrolled football athletes reported a diagnosis of NDs/NCDs compared to 4% of the athletes enrolled in the basketball, swimming, or wrestling teams [77].
ALS or MND
The previous review [23] on the risk of ALS and MND in former professional and varsity athletes reported a significantly higher frequency of ALS and MND in professional soccer and American football players, and a slightly increased risk of ALS in varsity athletes. The update of the SR allowed to identify 6 new cohort studies [77, 79, 82,83,84,85] and 1 new case–control study [81]. When considering professional athletes, 5 large cohort studies reported a significantly higher risk of ALS and MND in former soccer and American football players (MND: HR 3.52, p < 0.001; HR 4.33, p < 0.001; ALS: SIR 1.91; ALS: SIR 2.11; ALS: SIR 3.59) [82,83,84,85,86] compared to either general population [79,80,81,82] or matched controls [78]. Two studies specifically reported a significantly higher risk in subjects aged < 45 (SIR: 4.66, 95% CI 2.66–7.57) years and in athletes playing in the top league (SIR 5.69, 95%CI 2.73–10.47) [83] and in athletes having longer careers (OR 1.2, 95% CI 1.1–1.3) [86]. One study also reported a higher risk of death due to ALS compared to general population (SMR 3.94) [86]. Another cohort study used death certificates and did not report a higher risk of death due to ALS in former NFL players compared to baseball players [79]. The last cohort study enrolled varsity athletes from yearbooks and compared the frequency of ALS (i.e., healthcare information system) between football and non-football player, reporting no cases of ALS during its follow-up period [77]. The only, relatively small, case–control study enrolled cases from 2 registries and matched controls from general population and did not observe a significantly higher risk of ALS in athletes (i.e., any type of sport) compared to non-athletes [81].
Dementia and/or MCI
Ten cohort studies [43, 72, 74,75,76,77,78,79, 82, 84] and 1 case–control study [44] reported data on the risk of dementia in former professional and/or varsity athletes. Seven cohort studies [72, 74,75,76, 78, 79, 82, 83] reported information on the frequency of dementias or MCI in former professional athletes. When considering former soccer players, 2 large cohort studies enrolled participants from museum and league club archives and structured healthcare information systems, reporting a higher frequency of dementia (HR 3.59, p < 0.001; HR 3.87, p: < 0.001) and AD (HR 5.07, p: < 0.001) in former soccer players compared to general population [82, 84]. A small study enrolled former soccer players from 4 soccer clubs and did not report an increased risk NCDs as tested with a self-administered questionnaire in former players, irrespective of role and length of career, compared to general population [76]. As for American football, 3 cohort studies reported a slightly higher risk of AD in former NFL players [72, 74, 79]. The first two studies enrolled former NFL player from retired players associations and reported respectively a higher risk of AD compared to general US population (prevalence ratio 1.37) [72], and of death due to AD compared to US male mortality rates (SMR-U 1.80, SMR-U&C 3.86) [74], with the second reporting a significantly higher risk in athletes who played in speed positions (SMR 6.02) [74]. The third cohort study used data from the National Institute of Safety and Health (NIOSH) and reported a slightly, non-significantly, higher risk of death due to dementia/AD (i.e., death certificates) in former NFL players compared to baseball players (HR-U 1.28, HR-U&C 2.26) [79]. When considering varsity athletes, 2 cohort study enrolled former athletes from yearbooks [75, 77]. The first reported no significant differences in the frequency of dementia and MCI in former football players compared to non-football players [77], while the second reported no significant increase in the risk of dementia in former football players compared to participants in non-sport-related clubs [75]. Two further studies, 1 cohort, and 1 case–control study, investigated the association between occupational exposure to professional sports and the risk of death due to NCDs using census data and death certificates [43, 44]. The cohort study reported a significantly higher risk of AD in subjects whose occupation was coded as “writers, artists, entertainers, and athletes” (PMR: 135 (95% CI 111–162) [43], while the case–control study reported no significant increase on risk of AD or pre-senile dementia in subjects whose occupation was coded as “athlete or dancer” [44].
When considering MCI, a small cohort study enrolled participants from alumni associations and reported a slightly, non-significantly, higher risk of MCI (i.e., comprehensive neurocognitive assessment) in former NFL and hokey players compared to former non-contact sport athletes [78]. A small cohort study reported no increased risk of MCI based on a self-administered test in former soccer players from former player associations compared to general population (i.e., data from a large population study on MCI) [76]. However, one study on former NFL players from retired NFL players associations reported a correlation between MCI or memory impairment (MI) (i.e., diagnosed, self-reported, reported by informant) and self-reported recurrent concussion (MCI p = 0.02; self-reported MI p = 0.001; spouse/relative-reported MI p = 0.04) [72].
Parkinson's disease (PD)
Eight cohort studies [43, 73,74,75,76,77, 79, 82, 84] and 1 case–control study [44] reported data on the risk of PD in professional and varsity athletes. As for professional athletes, 2 cohort studies used data from archives of museums or clubs and hospital records, prescriptions, and death certificates, and reported a significantly higher frequency of PD in former soccer players (HR 2.09, p = 0.009; HR 2.15, p = 0.01) [82, 84]. Two further cohort studies used data from information systems (e.g., NIOSH database), and reported a higher risk of death due to PD (i.e., death certificates) in former American football players compared to general population (SMR-U&C 4.31) [74] or to former baseball players (HR-U&C 3.45) [79], with no significant difference between athletes playing in speed vs non-speed position [74]. One cohort study in a relatively limited sample of former Thai boxers enrolled from registers of former boxers (i.e., sports authority, boxers’ clubs, and Thai boxing foundation) reported a prevalence of PD and Parkinsonism, as assessed through a validated scales and questionnaires, comparable to the prevalence observed in several Asian general populations [73]. Two further studies, 1 cohort and 1 case–control, investigated the association between occupational exposure to professional sports and the risk of death due to PD using census data and death certificates [43, 44]. Of these, 1 reported a higher risk of death due to PD in the category of subjects whose occupation was categorized as “Writers, artists, entertainers, and athletes” (PMR: 128) [43], while the other reported no significantly increased risk of PD in subjects whose previous occupation was classified as “athlete” [44]. When considering varsity athletes, 2 studies enrolled former athletes from yearbooks and did not report a higher risk of PD or Parkinsonism in former American football players compared to either members of other non-sport-related clubs [75] or to non-football athletes [77].
Chronic traumatic encephalopathy (CTE)
Only one study reported data on the risk of CTE in former competitive athletes. The study enrolled participants from a brain tissue bank, ascertaining exposure to previous competitive sport participation (e.g., varsity, professional) through obituaries or school yearbooks. In this study, participants were classified as CTE positive (CTE +) in case of pathology fitting with all aspects of the consensus criteria for CTE neuropathology, and as “features of CTE” in case of multiple lesions suggestive of CTE pathology without being consistent with all parts of the criteria verbatim. CTE + and features of CTE were classified together as “combined CTE patology”. CTE + was also evaluated separately as secondary outcome. The study reported a significantly higher risk of CTE in participants who played American football both at during (CTE + OR = 2.87, p = 0.021) and after high school (CTE pathology OR = 13.23, p < 0.001, CTE + OR = 6.84, p = 0.0056), and in former boxers (CTE + OR = 10.29, p = 0.009) [80].
Quantitative analysis
No meta-analyses were carried out due to the clinical, methodological, and statistical heterogeneity of the included studies. The main reasons that prevented the cumulative analysis of data were due to the study designs being different, and their methodological quality not being homogeneous. As for clinical heterogeneity, the definition and source of both the reference population and the cases were widely variable across studies. Moreover, the investigated cohorts of athletes were mostly the same cohorts observed in different time-periods, as in the case of the two large cohort studies on mortality due to NDs among Scottish professional soccer players.
Discussion
Overall, the present systematic review reported a higher frequency of NDs/NCDs in former professional athletes. Specifically, published studies showed an increased frequency of any type of NDs/NCDs in former soccer players [82, 84] and American football players [74] even when compared to other non-contact sport athletes [79]. When considering specific NDs and NCDs, data from the update of the previous SRs confirmed a higher frequency of ALS or MND in former soccer players [82,83,84,85]. Gathered data also reported a significantly higher risk of dementia and AD in former soccer players [82, 84] and a higher risk of MCI in former American football players, mainly associated to a higher risk of concussion [72]. Moreover, data also showed a significantly higher risk of PD in former soccer and American football players [74, 75, 79, 82, 84] and a significantly higher risk of CTE in former boxers and in former American football players [80].
Some studies reported either non-significant results or no increase in risk in some categories of athletes. However, most of these studies were of low or relatively low methodological quality and included very small or relatively small samples defining cases based on self-reports or non-standardized/validated tools. Moreover, some studies only compared different types of sports (i.e., contact vs non-contact, football vs non-football). The only large and high-quality study [44] reporting no difference in the mortality rate for any of the considered NDs and NCDs considered as exposed participants classified as “athlete/dancer” based on the occupational census, which is a wider definition that could lead to potentially underestimating results. Most of the included studies attempted to take into consideration potential confounding factors by either matching non exposed subjects or controls by at least the main characteristics (e.g., gender, age, ethnicity), with some of them also stratifying for potential interacting factors such as length of career and type of sport or position/role played. However, the factors considered for adjustment where heterogeneous across some of the included studies, and most studies only include male professional players due to the availability of data. This further affected the direct comparison of data. Previous reviews suggested that the higher risk of NDs observed in some specific categories of former athletes could be sport specific. However, no studies on sports other than soccer, American football and marginally boxing, were available. Therefore, conclusion can only be based on available studies, as no data are currently available on different sports. Further large studies should be performed on other sports, mainly in other contact sports (e.g., boxing, martial arts) and sports requiring running/speed roles (e.g., rugby, hokey, etc.), should be carried out, as these types of sports resulted to be associated with the highest risk of NDs and NCDs.
As for ALS and MND, our results confirmed the higher risk observed in formed soccer and American football player reported in the previously published SR [23]. Included studies reported an increased risk of ALS in soccer and American football players also confirmed an earlier onset of ALS in soccer players, and a higher frequency of ALS in players with a longer career, in specific positions or roles, and playing in main leagues [82,83,84, 86]. Therefore, based on results from the previous SR and the present update, soccer and American football players seem to be at risk of a specific, more severe, type of ALS or MND, with earlier onset (< 45 years) and shorter survival.
Our data also showed an increased risk of dementia, AD and MCI in former soccer and American football players. This increase in the frequency of these conditions was linked, in some studies, to an increased exposure to brain injuries and concussions, specifically in former American football players. In this last category of athletes, a higher frequency of CTE was also observed. As expected, the risk of CTE resulted the highest in former boxers, who were among the first categories of athletes in whom the formerly called “punch drunk syndrome” and “dementia pugilistica” were investigated [99, 100].
Moreover, a higher risk of PD and Parkinsonism was observed in former soccer and American football players, which was not linked to specific roles or positions. This increased frequency of PD, as for dementia and cognitive decline, was also generally linked to an increased exposure to brain injury and trauma.
On this basis, our results seem to suggest that competitive athletes, and specifically those participating in contact sports, are exposed to a higher risk of trauma, concussion, and subsequent brain injuries, thus leading to a higher risk of developing cognitive outcomes or PD/Parkinsonism later in life. However, professional athletes appear to also be at a higher risk of what seems to be a specific form of ALS/MND. Based on our data and data from our previous SR, in fact, the type of ALS/MND observed in former soccer players seem to have a much earlier, bulbar onset, and a much shorter survival. This increased risk has been linked to several possible genetic and environmental risk factors. Several gene variants are associated with a susceptibility to ALS/MND, and when considering environmental risk factors, the exposure to heavy metals, trace elements, solvents, and other volatile organic compounds (e.g., pesticides and radiation) or toxins (e.g., cyanobacteria), has been linked to a higher risk of developing this condition. As for some life-style factors, the widespread use or abuse of branched-chain amino acids in professional athletes has been hypothesized to be potentially linked to a higher risk of ALS/MND [28]. This led to the specific hypothesis that professional athletes might share a specific phenotype linked to both a better predisposition to high-level sport and a risk of developing ALS/MND. However, all these genetic, environmental, and lifestyle risk factor are shared risk factors for all the considered NDs and NCDs. The exposure to some pesticides, including organophosphorus compounds and carbamates, in fact, has been reported to be associated not only to an increased risk of ALS, but also to a higher risk of AD and PD [101]. Several other compounds, such as solvents and neurotoxic agents, have also been proven to be shared risk factors for ALS and other NDs and NCDs, in particular PD [102]. Moreover, several polymorphisms and gene variants have been reported to be associated to a higher frequency of specific NDs, and some have also been investigated as involved in the epigenetic mechanisms leading to the onset of the disease [103,104,105,106]. The exposure to several lifestyle factors, including smoking, physical activity, and dietary habits along with the use/abuse of some dietary supplements, have also been proven to have a role in the etiological mechanisms of some NDs and NCDs. The evident interlinking and interaction among these factors, and their being shared risk factors for several NDs and NCDs underline the need to start considering neurodegeneration as a process starting with an early, subclinical, phase, which might be common to all NDs. The neurodegenerative process in NDs, in fact, has been proven to start several decades before the onset of symptoms [107]. This long latent period, along with the shared association between several risk factors and some specific NDs suggests that this early process might be common to different NDs and only in a subsequent phase cause specific symptoms according to a subjective susceptibility and specific interactions between risk factors [3, 108]. Thus, based on this hypothesis, research should focus on investigating the interacting role of genetic, environmental, and lifestyle risk factors in this early phase of neurodegeneration to explore the possibility of defining potential preventive strategies [106]. Moreover, former professional athletes should be further investigated, as these risk factors and their interactions, as well as the risk of some specific NDs, appear to be significantly higher in this population. Studies on this population should also aim at clarifying whether the risk might be specific to some type of sports or roles, and whether the clinical characteristics of the NDs are typical of this population.
Our SR has some limitations. The main limitation is the relatively small number of included studies. Studies on this topic are relatively few and are limited to a very small number of sports, mainly soccer and American football. This limits the generalizability of results and the reliability of results. The small number of published studies might be due to the difficulty of investigating a relatively rare exposure as having been a professional athlete, and the subsequent difficulty of enrolling large samples of professional athletes. Moreover, when considering ALS, the difficulty of carrying out large studies might also be due to the rarity of the disease, which would require very large samples. Furthermore, NDs and NCDs are diseases whose typical onset is later in life, thus longitudinal studies require covering very long observation periods. Therefore, prospective studies are almost unfeasible, and retrospective studies might be very difficult to carry out in absence of effective and efficient informative systems and databases. However, the use of data from information systems, such as death certificates and hospital records, largely underestimates the frequency of NDs and NCDs, thus limiting the quality of studies, as does the use, inevitable in these systems, of different diagnostic criteria. A further limitation, due to the above-mentioned difficulties, is that the considered cohorts of athletes should be intended as mostly the same cohorts observed in different time periods. This prevents the comparison and the cumulative analysis of data, allowing only to observe a possible trend in the risk of NDs and NCDs over time within the same cohort. Further high-quality studies including athletes participating in different sports would therefore be extremely useful to assess whether the observed higher risk might be sport-specific or shared with other types of sport, and to further investigate possible characteristic or risk factors suggesting specific pathophysiological mechanisms explaining the observed increase in the risk of NDs and NCDs.
Data availability
The present SR was not registered. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
JPND. Available at: https://www.neurodegenerationresearch.eu/what/ (Last visited: 10/11/2021)
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (5th ed.)
Gitler AD, Dhillon P, Shorter J (2017) Neurodegenerative disease: models, mechanisms, and a new hope. Dis Model Mech 10(5):499–502. https://doi.org/10.1242/dmm.030205
Siddique N, Siddique T. Amyotrophic Lateral Sclerosis Overview. 2001 Mar 23 [updated 2021 Sep 30]. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Gripp KW, Mirzaa GM, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2022
Beeldman E, Raaphorst J, Klein Twennaar M, de Visser M, Schmand BA, de Haan RJ (2016) The cognitive profile of ALS: a systematic review and meta-analysis update. J Neurol Neurosurg Psychiatry 87(6):611–619. https://doi.org/10.1136/jnnp-2015-310734
Pinto WBVR, Debona R, Nunes PP, Assis ACD, Lopes CG, Bortholin T, Dias RB, Naylor FGM, Chieia MAT, Souza PVS, Oliveira ASB (2019) Atypical Motor Neuron Disease variants: Still a diagnostic challenge in Neurology. Rev Neurol (Paris) 175(4):221–232. https://doi.org/10.1016/j.neurol.2018.04.016
Lang AE, Lozano AM (1998) Parkinson's disease. First of two parts. N Engl J Med 339(15):1044–53. https://doi.org/10.1056/NEJM199810083391506
Sacuiu SF (2016) Dementias. Handb Clin Neurol 138:123–151. https://doi.org/10.1016/B978-0-12-802973-2.00008-2
CDC 2019. Available at: https://www.cdc.gov/aging/dementia/index.html (Last visited: 10/11/2021)
Kovacs GG (2017) Concepts and classification of neurodegenerative diseases. Handb Clin Neurol 145:301–307. https://doi.org/10.1016/B978-0-12-802395-2.00021-3
Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, Brayne C, Burns A, Cohen-Mansfield J, Cooper C, Costafreda SG, Dias A, Fox N, Gitlin LN, Howard R, Kales HC, Kivimäki M, Larson EB, Ogunniyi A, Orgeta V, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbæk G, Teri L, Mukadam N (2020) Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 396(10248):413–446. https://doi.org/10.1016/S0140-6736(20)30367-6
Omalu BI, DeKosky ST, Minster RL et al (2005) Chronic traumatic encephalopathy in a National Football League player. Neurosurgery 57:128–134
McKee AC, Stern RA, Nowinski CJ et al (2013) The spectrum of disease in chronic traumatic encephalopathy. Brain 136:43–64
McKee AC, Daneshvar DH, Alvarez VE, Stein TD (2014) The neuropathology of sport. Acta Neuropathol 127:29–51
Hay J, Johnson VE, Smith DH, Stewart W (2016) Chronic traumatic encephalopathy: the neuropathological legacy of traumatic brain injury. Annu Rev Pathol 11:21–45
Stewart W, McNamara PH, Lawlor B et al (2016) Chronic traumatic encephalopathy: a potential late and under recognized consequence of rugby union? QJM 109:11–15
Hales C, Neill S, Gearing M et al (2014) Late-stage CTE pathology in a retired soccer player with dementia. Neurology 83(24):2307–2309
Bieniek KF, Ross OA, Cormier KA et al (2015) Chronic traumatic encephalopathy pathology in a neurodegenerative disorders brain bank. Acta Neuropathol 130:877–889
Grinberg LT, Anghinah R, Nascimento CF et al (2016) Chronic Traumatic Encephalopathy Presenting as Alzheimer’s Disease in a Retired Soccer Player. J Alzheimers Dis 54(1):169–174
Ling H, Morris HR, Neal JW et al (2017) Mixed pathologies including chronic traumatic encephalopathy account for dementia in retired association football (soccer) players. Acta Neuropathol 133(3):337–352
Lee EB, Kinch K, Johnson VE et al (2019) Chronic traumatic encephalopathy is a common co-morbidity, but less frequent primary dementia in former soccer and rugby players. Acta Neuropathol 138:389–399
Pearce N, Gallo V, McElvenny D (2015) Head trauma in sport and neurodegenerative disease: an issue whose time has come? Neurobiol Aging 36:1383–1389
Lacorte E, Ferrigno L, Leoncini E et al (2016) Physical activity, and physical activity related to sports, leisure and occupational activity as risk factors for ALS: A systematic review. Neurosci Biobehav Rev 66:61–79
Piazza O, Sirén AL, Ehrenreich H (2004) Soccer, neurotrauma and amyotrophic lateral sclerosis: is there a connection? Curr Med Res Opin 20(4):505–508
Patricios JS, Kemp S (2014) Chronic traumatic encephalopathy: rugby’s call for clarity, data and leadership in the concussion debate. Br J Sports Med 48(2):76–79
Harwood CA, McDermott CJ, Shaw PJ (2009) Physical activity as an exogenous risk factor in motor neuron disease (MND): a review of the evidence. Amyotroph Lateral Scler 10(4):191–204
Al-Chalabi A, Hardiman O (2013) The epidemiology of ALS: a conspiracy of genes, environment and time. Nat Rev Neurol 9(11):617–628
Beghi E (2013) Are professional soccer players at higher risk for ALS? Amyotroph Lateral Scler Frontotemporal Degener 14(7–8):501–506
Chiò A, Mora G (2012) Physical fitness and amyotrophic lateral sclerosis: dangerous liaisons or common genetic pathways? J Neurol Neurosurg Psychiatry 83(4):389. https://doi.org/10.1136/jnnp-2012-302351
Manley G, Gardner AJ, Schneider KJ et al (2017) A systematic review of potential long-term effects of sport-related concussion. Br J Sports Med 51(12):969–977
Rutherford A, Stewart W, Bruno D (2019) Heading for trouble: is dementia a game changer for football? Br J Sports Med 53(6):321–322
Morris JC, Storandt M, Miller JP et al (2001) Mild cognitive impairment represents early-stage Alzheimer’s disease. Arch Neurol 58:397–405
Petersen RC, Doody R, Kurz A et al (2001) Current concepts in mild cognitive impairment. Arch Neurol 58:1985–1992
Petersen RC, Stevens JC, Ganguli M et al. (2001) Practice parameter: Early detection of dementia–-MCI (an evidencebased review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 56:1133–1142
Martland HS (1928) Punch drunk. JAMA 91(15):1103–1107
Millspaugh JA (1937) Dementia pugilistica. U S Nav Med Bull 35:297–303
Roberts AH. Brain damage in boxers. A study of prevalence of traumatic encephalopathy among ex-professional boxers. London: Pitman Medical & Scientific Publication Company 1969:1–132
Mayeux R, Ottman R, Maestre G et al (1995) Synergistic effects of traumatic head injury and apolipoprotein-epsilon 4 in patients with Alzheimer’s disease. Neurology 45:555–557
Mez J, Daneshvar DH, Abdolmohammadi B et al (2020) Duration of American Football Play and Chronic Traumatic Encephalopathy. Ann Neurol 87(1):116–131
Higgins JPT, Green S (2011) Cochrane Handbook for Systematic Reviews of Interventions Version 5 1.0. The Cochrane Collaboration. Available: www.cochrane-handbook.org (accessed 12.14.2021).
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339(21):b2700
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, et al. (2011) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analysis. Available: www.ohri.ca/programs/clinical epidemiology/ oxford.asp (accessed 12.14.2021)
Schulte PA, Burnett CA, Boeniger MF, Johnson J (1996) Neurodegenerative diseases: occupational occurrence and potential risk factors, 1982 through1991. Am J Public Health 86(9):1281–1288
Park RM, Schulte PA, Bowman JD et al (2005) Potential occupational risks for neurodegenerative diseases. Am J Ind Med 48(1):63–77
Vanacore N, Binazzi A, Bottazzi M, Belli S (2006) Amyotrophic lateral sclerosis in an Italian professional soccer player. Parkinsonism Relat Disord 12(5):327–329
Dhote VV, Raja MKMM, Samundre P, Sharma S, Anwikar S, Upaganlawar AB (2022) Sports-Related Brain Injury and Neurodegeneration in Athletes. Curr Mol Pharmacol 15(1):51–76. https://doi.org/10.2174/1874467214666210910114324
Adani G, Filippini T, Garuti C et al (2020) Environmental Risk Factors for Early-Onset Alzheimer’s Dementia and Frontotemporal Dementia: A Case-Control Study in Northern Italy. Int J Environ Res Public Health 17(21):7941
Feddermann-Demont N, Junge A, Weber KP et al (2017) Prevalence of potential sports-associated risk factors in Swiss amyotrophic lateral sclerosis patients. Brain Behav 7(4):e00630
Cho J, Lee I, Park S et al (2018) Physical activity and all-cause mortality in Korean older adults. Ann Hum Biol 45(4):337–345
Schaffert J, Didehbani N, LoBue C, et al. (2021) Frequency and predictors of traumatic encephalopathy syndrome in a prospective cohort of retired professional athletes. Front Neurol 12:617526. Published 2021 Feb 23. https://doi.org/10.3389/fneur.2021.617526
Schwab N, Wennberg R, Grenier K et al (2021) Association of position played and career duration and chronic traumatic encephalopathy at autopsy in elite football and hockey players. Neurology 96(14):e1835–e1843
Collins MW, Lovell MR, Iverson GL et al. (2002) Cumulative effects of concussion in high school athletes. Neurosurgery 51(5):1175–9;discussion1180–1
Adams JW, Alvarez VE, Mez J et al (2018) Lewy body pathology and chronic traumatic encephalopathy associated with contact sports. J Neuropathol Exp Neurol 77(9):757–768
Vanacore N, Barbariol P, Caffari B et al (2018) Amyotrophic Lateral Sclerosis and soccer: an internet survey of 29 Italian players. Ann Ist Super Sanita 54(4):364–369
Rose SC, Yeates KO, Nguyen JT et al (2021) Exposure to head impacts and cognitive and behavioral outcomes in youth tackle football players across 4 seasons. JAMA Netw Open 4(12):e2140359. https://doi.org/10.1001/jamanetworkopen.2021.40359
Char Bray MJ, Tsai J, Bryant B et al. (2022) Effect of professional fighters' weight class on regional brain volume, cognition, and other neuropsychiatric outcomes. Neurology 98(1 Supplement 1):S10. https://doi.org/10.1212/01.wnl.0000801824.22603.9a
Walia B, Kmush BL, Ehrlich J, Mackowski M, Sanders S (2021) Age at league entry and early all-cause mortality among national football league players. Int J Environ Res Public Health 18(24):13356. https://doi.org/10.3390/ijerph182413356
Tenforde AS, Cortez B, Coughlan-Gifford E et al (2022) Individual and cumulative health afflictions are associated with greater impairment in physical and mental function in former professional American style football players. PM R 14(1):30–39. https://doi.org/10.1002/pmrj.12581
Longstreth WT, McGuire V, Koepsell TD et al (1998) Risk of amyotrophic lateral sclerosis and history of physical activity: a population-based case-control study. Arch Neurol 55:201–206
Scarmeas N, Shih T, Stern Y et al (2002) Premorbid weight, body mass, and varsity athletics in ALS. Neurology 59:773–775
Belli S, Vanacore N (2005) Proportionate mortality of Italian soccer players: is amyotrophic lateral sclerosis an occupational disease? Eur J Epidemiol 20(3):237–242
Chiò A, Benzi G, Dossena M, Mutani R, Mora G (2005) Severely increased risk of amyotrophic lateral sclerosis among Italian professional football players. Brain 128(Pt 3):472–476
Valenti M, Pontieri FE, Conti F, Altobelli E, Manzoni T, Frati L (2005) Amyotrophic lateral sclerosis and sports: a case-control study. Eur J Neurol 12(3):223–225
Abel EL (2007) Football increases the risk for Lou Gehrig’s disease, amyotrophic lateral sclerosis. Percept Mot Skills 104(3):1251–1254
Taioli E (2007) All causes of mortality in male professional soccer players. Eur J Public Health 17(6):600–604
Chiò A, Calvo A, Dossena M et al (2009) LS in Italian professional soccer players: the risk is still present and could be soccer-specific. Amyotroph Lateral Scler 4:205–209
Beghi E, Logroscino G, Chiò A et al (2010) Amyotrophic lateral sclerosis, physical exercise, trauma and sports: results of a population-based pilot case-control study. Amyotroph Lateral Scler 11(3):289–292
Vanacore N, Cocco P, Fadda D, Dosemeci M (2010) Job strain, hypoxia and riskof amyotrophic lateral sclerosis: results from a death certificate study. Amyotroph Lateral Scler 11(5):430–434
Trojsi F, Sagnelli A, Vanacore N et al (2012) Clinical features and lifestyle of patients with amyotrophic lateral sclerosis in Campania: brief overview of an Italian database. Ann Ist Super Sanita 48(3):287–291
Gotkine M1, Friedlander Y, Hochner H (2014) Triathletes are over-represented in a population of patients with ALS. Amyotroph Lateral Scler Frontotemporal Degener 15(7–8):534–536
Fang F, Hållmarker U, James S et al (2016) Amyotrophic lateral sclerosis among cross-country skiers in Sweden. Eur J Epidemiol 31(3):247–253
Guskiewicz KM, Marshall SW, Bailes J et al. (2005) Association between recurrent concussion and late-life cognitive impairment in retired professional football players. Neurosurgery 57(4):719–26;discussion719–26
Lolekha P, Phanthumchinda K, Bhidayasiri R (2010) Prevalence and risk factors of Parkinson’s disease in retired Thai traditional boxers. Mov Disord 25(12):1895–1901
Lehman EJ, Hein MJ, Baron SL, Gersic CM (2012) Neurodegenerative causes of death among retired National Football League players. Neurology 79(19):1970–1974
Savica R, Parisi JE, Wold LE et al (2012) High school football and risk of neurodegeneration: a community-based study. Mayo Clin Proc 87(4):335–340
Vann Jones SA, Breakey RW, Evans PJ (2014) Heading in football, long-term cognitive decline and dementia: evidence from screening retired professional footballers. Br J Sports Med 48(2):159–161
Janssen PH, Mandrekar J, Mielke MM et al (2017) High school football and late-life risk of neurodegenerative syndromes, 1956–1970. Mayo Clin Proc 92(1):66–71
Willer BS, Zivadinov R, Haider MN et al (2018) A preliminary study of early-onset dementia of former professional football and hockey players. J Head Trauma Rehabil 33(5):E1–E8
Nguyen VT, Zafonte RD, Chen JT et al (2019) Mortality Among Professional American-Style Football Players and Professional American Baseball Players. JAMA Netw Open 2(5):e194223
Bieniek KF, Blessing MM, Heckman MG et al (2020) Association between contact sports participation and chronic traumatic encephalopathy: a retrospective cohort study. Brain Pathol 30(1):63–74
Filippini T, Fiore M, Tesauro M et al. (2020) Clinical and Lifestyle Factors and Risk of Amyotrophic Lateral Sclerosis: A Population-Based Case-Control Study. Int J Environ Res Public Health 30;17(3):857
Mackay DF, Russell ER, Stewart K et al (2019) Neurodegenerative Disease Mortality among Former Professional Soccer Players. N Engl J Med 381(19):1801–1808
Pupillo E, Bianchi E, Vanacore N et al (2020) Increased risk and early onset of ALS in professional players from Italian Soccer Teams. Amyotroph Lateral Scler Frontotemporal Degener 21(5–6):403–409
Russell ER, Mackay DF, Stewart K et al (2021) Association of field position and career length with risk of neurodegenerative disease in male former professional soccer players. JAMA Neurol 78(9):1057–1063
Gamez J, Carmona F (2021) Confirmation of early non-bulbar onset of amyotrophic lateral sclerosis in Spanish league soccer players. J Neurol Sci 428:117586
Daneshvar DH, Mez J, Alosco ML et al (2021) Incidence of and mortality from amyotrophic lateral sclerosis in national football league athletes. JAMA Netw Open 4(12):e2138801. https://doi.org/10.1001/jamanetworkopen.2021.38801
Chiò A, Magnani C, Oddenino E et al (1992) Accuracy of death certificate diagnosis of amyotrophic lateral sclerosis. J Epidemiol Community Health 46(5):517–518
Ragonese P, Filippini G, Salemi G et al (2004) Accuracy of death certificates for amyotrophic lateral sclerosis varies significantly from north to south of Italy: implications for mortality studies. Neuroepidemiology 23(1–2):73–77
Yeo L, Lynch C, Hardiman O (2010) Validating population-based registers for ALS: how accurate is death certification? J Neurol 257(8):1235–1239
Stickler DE, Royer JA, Hardin JW (2012) Accuracy and usefulness of ICD-10 death certificate coding for the identification of patients with ALS: results from the South Carolina ALS Surveillance Pilot Project. Amyotroph Lateral Scler 13(1):69–73
Perera G, Stewart R, Higginson IJ, Sleeman KE (2016) Reporting of clinically diagnosed dementia on death certificates: retrospective cohort study. Age Ageing 45(5):668–673
Gao L, Calloway R, Zhao E et al (2018) Accuracy of death certification of dementia in population-based samples of older people: analysis over time. Age Ageing 47(4):589–594
Hobson P, Meara J (2018) Mortality and quality of death certification in a cohort of patients with Parkinson’s disease and matched controls in North Wales, UK at 18 years: a community-based cohort study. BMJ Open 8(2):e018969
Shi H, Counsell C (2021) Accuracy of death certificates for recording parkinsonian syndromes and associated dementia. J Neurol 268(1):140–146
Marin B, Couratier P, Preux PM, Logroscino G (2011) Can mortality data be used to estimate amyotrophic lateral sclerosis incidence? Neuroepidemiology 36(1):29–38
Erkinjuntti T, Ostbye T, Steenhuis R, Hachinski V (1997) The effect of different diagnostic criteria on the prevalence of dementia. N Engl J Med 337(23):1667–1674
Wancata J, Börjesson-Hanson A, Ostling S et al (2007) Diagnostic criteria influence dementia prevalence. Am J Geriatr Psychiatry 15(12):1034–1045
Naik M, Nygaard HA (2008) Diagnosing dementia – ICD-10 not so bad after all: a comparison between dementia criteria according to DSM-IV and ICD-10. Int J Geriatr Psychiatry 23(3):279–282
Fesharaki-Zadeh A (2019) Chronic traumatic encephalopathy: a brief overview. Front Neurol 10:713
Inserra CJ, DeVrieze BW. Chronic traumatic encephalopathy. [Updated 2021 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from:https://www.ncbi.nlm.nih.gov/books/NBK470535/. Accessed 10/11/2021
Baltazar MT, Dinis-Oliveira RJ, de Lourdes BM et al (2014) Pesticides exposure as etiological factors of Parkinson’s disease and other neurodegenerative diseases–a mechanistic approach. Toxicol Lett 230(2):85–103
Pezzoli G, Cereda E (2013) Exposure to pesticides or solvents and risk of Parkinson disease. Neurology 80(22):2035–2041
Bradley WG, Andrew AS, Traynor BJ et al (2018) Gene-Environment-Time Interactions in Neurodegenerative Diseases: Hypotheses and Research Approaches. Ann Neurosci 25:261–267
Fleming SM (2017) Mechanisms of Gene-Environment Interactions in Parkinson’s Disease. Curr Environ Health Rep 4(2):192–199
Berson A, Nativio R, Berger SL, Bonini NM (2018) Epigenetic regulation in neurodegenerative diseases. Trends Neurosci 41(9):587–598
Nativio R, Donahue G, Berson A et al (2018) Dysregulation of the epigenetic landscape of normal aging in Alzheimer’s disease. Nat Neurosci 21(4):497–505
Calne DB, Eisen A, McGeer E, Spencer P (1986) Alzheimer’s disease, Parkinson’s disease, and motoneurone disease: abiotrophic interaction between ageing and environment? Lancet 2(8515):1067–1070
Jellinger KA (2009) Recent advances in our understanding of neurodegeneration. J Neural Transm (Vienna) 116(9):1111–1162
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
- An increased frequency of any type of NDs or NCDs has been identified in former soccer players and American football players.
- An increased risk of dementia and mild cognitive impairment, Alzheimer’s disease, Parkinson’s disease, amyotrophic lateral sclerosis, and chronic traumatic encephalopathy has been identified among former professional and varsity athletes.
- NDs could share common etiopathogenic process, and only in a subsequent phase specific symptoms can occur, according to a subjective susceptibility and specific interactions between risk factors. This can be explained by the long latent period, along with the shared association between several risk factors and specific NDs.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bellomo, G., Piscopo, P., Corbo, M. et al. A systematic review on the risk of neurodegenerative diseases and neurocognitive disorders in professional and varsity athletes. Neurol Sci 43, 6667–6691 (2022). https://doi.org/10.1007/s10072-022-06319-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-022-06319-x