
Abstract
Background
Kinesiology tape (KT), a water-resistant and elastic tape which is well known measure for preventing musculoskeletal injuries, has recently gained popularity in neurological rehabilitation. This is a systematic and meta-analysis study, useful both to evaluate the efficacy of kinesiology taping on the functions of upper limbs in patients with stroke and to collect the main outcomes evaluated in the analyzed studies.
Methods
A comprehensive literature search of electronic databases including Medline, Web of science, Embase, Cochrane Central Register of Controlled Trials, Physiotherapy Evidence Database (PEDro), WANFANG, and the China National Knowledge Infrastructure (CNKI). Additional articles were obtained by scanning reference lists of included studies and previous reviews. Keywords were “kinesiology taping,” “kinesio,” “kinesio taping,” “tape” and “stroke,” “hemiplegia,” “hemiplegic paralysis,” “apoplexy,” “hemiparesis,” “upper extremity,” “upper limb.” All the RCTs were included. Quality assessment was performed using Cochrane criteria. Upper extremity function and pain intensity was pooled as the primary outcome, and shoulder subluxation, muscle spasticity, general disability, PROM of abduction, and adverse effects as secondary outcomes.
Results
Twelve articles were included. Pooled data provided evidence that there was significance between kinesiology taping groups and control groups in pain intensity (standardized mean difference − 0.79, 95% CI − 1.39 to − 0.19), shoulder subluxation (standardized mean difference − 0.50, 95%CI − 0.80 to − 0.20), general disability (standardized mean difference 0.35, 95%CI 0.10 to 0.59), upper extremity function (standardized mean difference 0.61, 95%CI 0.18 to 1.04), and the PROM of flexion (standardized mean difference 0.63, 95%CI 0.28 to 0.98).
Conclusion
Current evidence suggested that kinesiology taping could be recommended to improve upper limb function in patients with stroke in pain intensity, shoulder subluxation, general disability, upper extremity function, and the PROM of flexion.
Ethics and dissemination
Ethical approval requirements are not necessary for this review. This systematic review and meta-analysis will be disseminated online and on paper to help guide the clinical practice better.
PROSPERO registration number
CRD42020179762.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Upper limb function after stroke is the main cause of long-term disability, so rehabilitation research is a top priority. Although nerve reorganization occurs soon after stroke, the natural rehabilitation of upper limb function recovery is usually limited. In order to overcome these limitations, new strategies are needed to strengthen nerve regeneration and restore brain structure and function. In addition, upper limb paresis is observed in 87% of stroke survivors [1]. Furthermore, impaired use of the upper limb persists in about 60% of the patients 6 months post-stroke [2]. Impairment of upper limb is a cause of muscle weakness, loss of multi-joint movements coordination, and changes in muscle tone and sensation [3], which is strongly correlated to dependency in activities of daily living (ADL) and participation restrictions [4]. Although previous studies reported that initial degree of severity of paresis, functional and structural changes, and genetic factors may influence recovery of upper limb function, predicting such recovery in stroke patients is difficult [5,6,7].
Clinicians now have more evidence to support the motion exercises, motor imagery, mirror therapy, and non-invasive brain stimulation, such as transcranial magnetic stimulation and transcranial direct current stimulation (tDCS) promote upper limb recovery. In addition, pain is one of the main outcomes that influence the choice of the type of treatment [8].
Kinesiology tape (KT) is an elastic, waterproof, and breathable tape and Kenzo Kase invented this tape in the 1970s. It can be stretched to 120–140% of its original length and can be recoiled after use [9]. KT is a widely used treatment in both clinical and sports fields. KT is similar to the elasticity of human skin, so it allows more movement and feels more comfortable. In recent years, KT has become increasingly popular in rehabilitation for hemiplegic patients. The recent systematic review which found a significant effect on taping for reduction of pain and subluxation in stroke patients was in line with the positive effect of KT and the study focused on various of tapes including therapeutic strapping, inelastic tape, California tri pull taping method and KT [10]. With the development of KT, it is increasingly used in upper limb rehabilitation. Some researchers proposed that KT could offer intensification of sensory input from the paretic upper limb to enhance motor performance and alleviate sensory impairment [11, 12]. Simoneau and Callagan found the positive effect of KT on proprioception [13, 14]. Owing to elastic stimulation of KT, it could allow for facilitation of muscle activation [15].
Research has shown that KT can promote functional use of the upper and lower extremity, in further to improve balance ability [16]. Recent meta-analyses of randomized controlled trials compared KT versus conventional rehabilitation for treating balance impairment after stroke with 22 studies included. The systematic reviews have demonstrated KT was more effective than conventional rehabilitation for balance function. They also pointed out that KT can improve lower limb function, and walking function in stroke patients [17]. A 2015 systematic review reported that there is insufficient evidence for adhesive taping post-stroke in improving outcomes, including pain intensity, range of motion, muscle tone, strength, activity, and participation [18]. As we all know, upper limb ability plays a very important role in the patient’s balance ability. This review focused on evaluate the effect of KT on upper limb function. In general, the efficacy of KT for function of stroke patients remains uncertain [19,20,21,22,23].
This is a systemic and meta-analysis study. The purpose of this review was to evaluate the effect of KT on upper limbs function outcomes in stroke patients. To evaluate the efficacy of KT for upper extremity function, pain intensity, shoulder subluxation, muscle spasticity, general disability, and the passive range of motion (PROM) of flexion and abduction in patients with stroke.
The systematic review was registered on PROSPERO (ID: CRD42020179762). All the PRISMA standards and recommendations for systematic review development were followed [24].
Method
Data sources
We searched Medline (via PubMed), Web of Science, Embase, the Cochrane database of Controlled Trials, PEDro, WANFANG, and CNKI up to July 30, 2021. Additional articles were obtained by scanning reference lists of included studies and previous reviews.
Study selection
Keywords were (1) “kinesiology taping,” “kinesio,” “kinesio taping,” “tape” and (2) “stroke,” “hemiplegia,” “hemiplegic paralysis,” “apoplexy,” “hemiparesis,” “upper extremity,” “upper limb.” Studies were included if they met the following criteria: (1) In adults (18 years and older); (2) if they were RCTs conducted in patients with stroke comparing KT with conventional rehabilitation. (3) There was no restriction on follow-up and study size. (4) Studies needed to report 1 or more of the following outcomes: pain intensity, shoulder subluxation, muscle spasticity, general disability, upper extremity function, and the PROM of flexion and abduction. Studies were excluded if (1) trails using other forms of tape (e.g., inelastic tape). (2) Trails that did not provide abundant information to analyses treatment effects and we got no reply from the authors. (3) Trails that were non-randomized observational trials, cross-over design trails, case reports, clinical observations, and systematic reviews. This study conformed to all PRISMA guidelines and reported the required information accordingly (see Supplementary PRISMA checklist).
Data extraction
Two investigators no involved in any of the selected studies independently screened each title and abstract to exclude duplicates and studies not meeting the inclusion criteria. Additionally, one of the reviewers extracted study and patient characteristics, intervention and comparator details, and outcome data from included studies using pre-specified data extraction tables. The second author check for accuracy, and disagreement was resolved by discussion. Using the criteria suggested in the Cochrane handbook, we assessed the bias of risk. If there were fewer than 10 studies included, publication bias was deemed non-estimable and not rated down [25].
Statistical analysis
Quality assessment was undertaken using Cochrane criteria [26,27,28]. It is a two-part tool with seven specific domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias [29]. Two reviewers conducted the quality assessment independently of each other and then crosschecked their findings. A Chi square test evaluated the statistical significance of heterogeneity. The I2 statistical significance. We defined an I2 > 50% as substantial heterogeneity. A value of 0% means there is no observed heterogeneity and lager percentages indicate more heterogeneity. To address treatment heterogeneity in the included studies, we tried to find an explanation for this heterogeneity by performing sensitivity analysis. Sensitivity analysis was conducted by removing individual studies one by one. Results of meta-analyses may overestimate the true population effect due to publication bias [30]. To reduce its potential impact, publication bias was determined by funnel plots and the Egger’s regression test [31]. Statistical significance was set at P < 0.05. Data were analyzed in Review Manager Version 5.3 software and Stata 15 software.
Results
Baseline characteristics
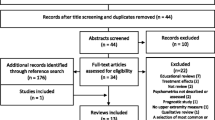
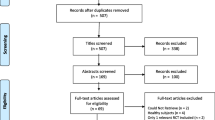
The study selection flow diagram is illustrated in Fig. 1. A total of 12 studies including 535 participants were included in the meta-analysis [21, 23, 32,33,34,35,36,37,38,39,40]. Sample size ranged from 14 to 120 participants. The average age ranged between 50.25 and 68.27 years old. In terms of type of KT, three trials used the NITTO medical adhesive tape, two trials used the Kinesio taping NFDA Production License 1,640,045, one trial used the Kinesio Tex gold tape, one trial used the 3NS kinesiology taping, one trial used the Kindmax Kinesio taping (Shanghai Kangmashi Sports Goods Co. LTD), one trial used the Kinesio taping (Nanjin Siruiqi Medical Supplies Co. LID), and three trials did not report. The intervention frequency varied between five to seven days per week and the follow-up period ranged between 3 to 28 weeks. Characteristic of included studies are summarized in Table 1.

Flow diagram of the literature search and selection process
Methodological quality and risk of bias
Quality assessment was presented in Fig. 2. Ten studies reported whether there was random sequence generation (83.3%, 10/12) [21, 23, 32, 34, 36,37,38,39,40,41]. Seven studies reported whether there was appropriate allocation concealment (58.3%, 7/12) [21, 23, 32, 37, 39,40,41]. Only 41.7% (5/12) studies were double blind and 58.3% (7/12) had inadequate blinding. Although the information for assessing individual study quality was limited, the overall evidence should be considered of fairly high quality since most study had not significant missing data and only randomized trials were included. Additionally, none of the meta-analysis groups had greater than 10 studies and therefore neither Funnel plot or Egger test was completed.

There were twelve randomized controlled studies included in our meta-analysis. The quality of studies was assessed with the Cochrane collaboration’s tool
Outcomes
Upper extremity function
Ten studies totaling 495 participants presented outcome for upper extremity function [21, 23, 32, 33, 35,36,37,38,39,40]. Meta-analysis revealed an association between the application of KT and upper extremity function (SMD 0.61, 95%CI 0.18 to 1.04) with significance heterogeneity across the studies (Fig. 3A, Fig. 4A). Exploratory sensitivity analysis revealed the study of Li et al. to be the likely source of this heterogeneity, with its exclusion from meta-analysis resulting in a revised I2 = 13% [42]. The possible causes may be more than 100 participants, while the sample size of other studies ranged from 14 to 84.

A Forest plot of strategies for efficacy of upper extremity function. B Forest plot of strategies for efficacy of pain intensity. C Forest plot of strategies for efficacy of shoulder subluxation. D Forest plot of strategies for efficacy of muscle spasticity. E Forest plot of strategies for efficacy of general disability. F Forest plot of strategies for efficacy of PROM of flexion. G Forest plot of strategies for efficacy of PROM of abduction

A Funnel plot for efficacy of upper extremity function. B Funnel plot for efficacy of pain intensity. C Funnel plot for efficacy of shoulder subluxation. D Funnel plot for efficacy of muscle spasticity. E Funnel plot for efficacy of general disability. F Funnel plot for efficacy of PROM of flexion. G Funnel plot for efficacy of PROM of abduction
Pain intensity
Pain intensity was reported in seven studies, totaling 364 participants [23, 32,33,34, 36, 38, 41]. Pooled data suggested significant difference in pain intensity with KT (SMD − 0.79, 95%CI − 1.39 to − 0.19, I2 = 85%) (Fig. 3B). The funnel plot (Fig. 4B) was slightly asymmetrical, and the Egger test did not indicate potential publication bias (p = 0.25).
A sensitivity analysis was conducted according to our protocol by excluding one study. Sensitivity analysis suggested that the pooled estimates or heterogeneity were not substantially modified by removing the included studies one by one.
Shoulder subluxation
The pooled estimate based on 5 studies indicated significant effect of KT on alleviating shoulder subluxation (SMD − 0.50, 95%CI − 0.80 to − 0.20, I2 = 3%) without significant heterogeneity across the studies (Fig. 3C) [33, 34, 37, 40, 41]. The publication bias tests were not significant and the funnel plots (Fig. 4C) can be considered slightly asymmetrical and the Egger test did not indicate potential publication bias (p = 0.56).
Muscle spasticity
Three studies (n = 52) reported muscle spasticity [21, 33, 39]. There was no statistically significant reduction in score of modified Ashworth scale (MAS), with KT (MD 0.19, 95%CI − 0.65 to 1.04) compared with conventional rehabilitation alone. There was significant heterogeneity across the studies (Fig. 3D). The results of publication bias showed the funnel plots was symmetrical and there was no significance of Egger’s regression (p = 0.29).
In the case of substantial heterogeneity, we explore possible causes by sensitivity analysis. When we remove the study of Yang et al. [39], the I2 statistics for heterogeneity reduced to 0%. The factor was identified as potential contributors to this observation was a modestly longer follow-up period compared with other studies.
General disability
Data about the effects of KT on general disability were reported in 7 studies [23, 32,33,34,35, 38, 39]. Five trial evaluating general disability showed a favorable effect [32, 34, 35, 38, 39], and the remaining two trials reported no significance effects on general disability [23, 33]. We showed that KT have a positive influence on general disability (SMD 0.35, 95%CI − 0.10 to 0.59). No significant heterogeneity was found in the pooled outcomes, so a fixed-effect model was utilized in our study (Fig. 3E). The publication bias test was not significant with the Egger’s regression test (p = 0.41) and the funnel plot (Fig. 4E) was slightly asymmetrical.
PROM of flexion
For PROM of flexion, the meta-analysis showed an improvement (SMD 0.63, 95%CI 0.28 to 0.98). A fixed-effect model was utilized in our study, since no significant heterogeneity was found in the pooled outcomes (Fig. 3F). The Egger regression test suggested there was no significance (p = 0.62) in agree with the result of funnel plot (Fig. 4F).
PROM of abduction
No statistically significant difference in PROM of abduction was found with KT (SMD 0.32, 95%CI − 0.02 to 0.66) with no significant heterogeneity (Fig. 3G). The funnel plot (Fig. 4G) was slightly asymmetrical, and the Egger test did not indicate potential publication bias (p = 0.94).
Adverse effects
Only 2 studies report whether there was the presence of adverse effects during the application of KT [34, 36]. Of those, only one study reported mild itching [36]. Overall, KT was well tolerated and only common and mild side effects were registered.
Discussion
This is the first review to systematically summarize the benefits of KT on upper extremity function, including pain intensity, shoulder subluxation, general disability, and the PROM of flexion. In this study, we used original data from 12 randomized controlled trials of KT application to explore the effectiveness upper limb function in poststroke patients. Our study shows that the application of KT leads to a significant improvement upper extremity function, pain intensity, shoulder subluxation, general disability, and the PROM of flexion. However, there was no between-group difference in muscle spasticity or the PROM of abduction.
A recent overview that included 12 studies identified reduction in shoulder pain when combined with exercise in shoulder pain symptom patients [43],which is consistent with the present analyses. It has been proposed that the KT increases blood circulation and lymphatic drainage leading to a reduction in swelling and subsequently to relieve pain [44, 45]. The applied KT could also work by lifting the skin, resulting in a reduction of pressure on the subcutaneous nociceptors [46]. To date, the underlying pain-relief mechanism of KT remain confused [47]. Additionally, owing to the inconsistency in intensity, duration, and frequency of the KT application, we should take caution with our findings. For shoulder subluxation, we observed a moderate effect size, and heterogeneity was not obvious, even though different methods of measurement were utilized. Potential mechanisms of KT for shoulder subluxation seems plausible. Dr Kenso Kase suggested that KT can provide therapeutic effects, such as correction of joint misalignment and functional, proprioceptive stimulation [44, 48]. In terms of KT’s thickness and elasticity, it reduces swelling which could improve joint mobility, decrease intra-articular pressure [49]. Some reports have suggested there was significant difference between KT and conventional rehabilitation in muscle spasticity [17], while others suggested that there was no statistically significant improvement in muscle tone [18]. In our study, the pooled data shows that there was no significant in muscle spasticity. However, due to the limited number of included studies, the findings should be taken into consideration when analyzing the results thoroughly. The results of general disability and upper extremity function suggested that KT have positive impact on stroke patients. However, as function outcome, general disability and upper extremity function of stroke patients typically require long-term follow-up and large samples to detect effects on function [50]. Moreover, analyses of the flexion PROM and abduction PROM outcomes included small sample size and were likely not adequately power to detect an effect of KT. Overall, the observation that KT application improve upper extremity function and general disability compared with control groups, but does not reduce the muscle spasticity and the PROM of abduction, suggested that although KT does not improve the muscle tone and PROM, it does confer improve patients’ overall function.
There are four points deserved to think about. First, KT is a safe and effective method, while the mechanism of KT is not clear at present [51], its therapeutic effect may be by sticking KT into different directions and using different tensions [45]. However, the taping method seemed to vary across studies, including difference in target muscle, direction, tension, and concomitant treatment. And it could be found that the application was heterogeneous in terms of type of KT. The elasticity, perspiration, breathability, waterproofness, durability, adhesion, appearance, and other experiences are different in different type of KT. Therefore, our results should be interpreted with caution. Second, conventional rehabilitation or usual treatment may have differed across studies. The improvements in upper extremity function, pain intensity, shoulder subluxation, general disability, and the PROM of flexion demonstrated by studies are a combined effect of KT and conventional rehabilitation or usual treatment. It is unclear what extent contribution the KT made to the improvements because of varies of convention rehabilitation or usual treatment, including the type, intensity, and frequency. Additionally, the control group included a mixture of placebo-controlled and open-label studies, which should be taken into consideration when analyzing the results. Finally, there was a difference between included studies, including the follow-up time and sample size.
The main strength of this study is that we investigate a wide range of function outcomes, which adds exceptional value to this meta-analysis. As the population ages and stroke mortality declines [52], this is an area worthy of future research attention. More high-quality RCTs examining the effect of KT on upper limb function in patients with stroke are urgently needed. Furthermore, investigators should clearly and fully describe the details of the intervention, control, and outcomes. Our study has multiple limitations that need to be disclosed. Only 12 studies were included in this analysis, which limits the reliability of the results, and two trials were performed by the same group of authors. All studies included trials were single center. Additionally, meta-analyses are often limited to short-term effects, due to difficulties interpreting varied follow-up intervals and potential for other treatments during the follow-up phase [49]. However, moderation analyses are very useful in developing preventive strategies and designing appropriate interventions.
Conclusion
In conclusion, the current systematic review and meta-analysis identified that KT could be used for improving upper limb function in stroke patients. However, due to the limited quality of the evidence currently available, the results should be treated with caution.
Abbreviations
- ADL:
-
Activities of daily living
- CI:
-
Confidence intervals
- CNKI:
-
The China National Knowledge Infrastructure
- Co. LTD:
-
Limited company
- KT:
-
Kinesiology taping
- MAS:
-
Modified Ashworth scale
- PRISMA:
-
The preferred reporting items for systematic reviews and meta-analyses
- PROM:
-
Passive range of motion
- PROSPERO:
-
International prospective register of systematic reviews
- PEDro:
-
Physiotherapy evidence database
- RCT:
-
Randomized controlled trial
- SMD:
-
STD mean difference
References
Parker VM, Wade DT, Langton HR (1986) Loss of arm function after stroke: measurement, frequency, and recovery. Int Rehabil Med 8(2):69–73. https://doi.org/10.3109/03790798609166178
Nijland RH, Van Wegen EE, Harmeling BC et al (2010) Presence of finger extension and shoulder abduction within 72 hours after stroke predicts functional recovery: early prediction of functional outcome after stroke: the EPOS cohort study. Stroke 41(4):745–750. https://doi.org/10.1161/STROKEAHA.109.572065
Tedesco Triccas L, Kennedy N, Smith T et al (2019) Predictors of upper limb spasticity after stroke? A systematic review and meta-analysis. Physiotherapy 105(2):163–173. https://doi.org/10.1016/j.physio.2019.01.004
Veerbeek JM, Kwakkel G, van Wegen EE et al (2011) Early prediction of outcome of activities of daily living after stroke: a systematic review. Stroke 42(5):1482–1488. https://doi.org/10.1161/STROKEAHA.110.604090
Cramer SC (2008) Repairing the human brain after stroke: I Mechanisms of spontaneous recovery. Ann Neurol 63(3):272–287. https://doi.org/10.1002/ana.21393
Seitz RJ, Donnan GA (2015) Recovery potential after acute stroke. Front Neurol 6:238. https://doi.org/10.3389/fneur.2015.00238
Lindgren A, Maguire J (2016) Stroke recovery genetics. Stroke 47(9):2427–2434. https://doi.org/10.1161/STROKEAHA.116.010648
Llorens R, Fuentes MA, Borrego A et al (2021) Effectiveness of a combined transcranial direct current stimulation and virtual reality-based intervention on upper limb function in chronic individuals post-stroke with persistent severe hemiparesis: a randomized controlled trial. J Neuroeng Rehabil 18(1):108. https://doi.org/10.1186/s12984-021-00896-2
Travis Halseth JWM, DeBeliso M (2004) The effects of kinesiotm taping on proprioception at the ankle. J Sports Sci Med 2004(3):1–7
Ravichandran H, Janakiraman B, Sundaram S et al (2019) Systematic review on effectiveness of shoulder taping in hemiplegia. J Stroke Cerebrovasc Dis 28(6):1463–1473. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.03.021
Bolognini N, Russo C, Edwards DJ (2016) The sensory side of post-stroke motor rehabilitation. Restor Neurol Neurosci 34(4):571–586. https://doi.org/10.3233/RNN-150606
Reding MJ, Potes E (1988) Rehabilitation outcome following initial unilateral hemispheric stroke. Life table analysis approach. Stroke 19(11):1354–8. https://doi.org/10.1161/01.str.19.11.1354
Simoneau GG, Degner RM, Kramper CA et al (1997) Changes in ankle joint proprioception resulting from strips of athletic tape applied over the skin. J Athl Train 32(2):141–147
Callaghan MJ, Selfe J, Bagley PJ et al (2002) The effects of patellar taping on knee joint proprioception. J Athl Train 37(1):19–24
Yang JM, Lee JH (2018) Is kinesio taping to generate skin convolutions effective for increasing local blood circulation? Med Sci Monit 24:288–293. https://doi.org/10.12659/msm.905708
EwaJaraczewska CL (2006) Kinesio taping in stroke: improving functional use of the upper extremity in hemiplegia. Top Stroke Rehabil 13(3):31–42
Hu Y, Zhong D, Xiao Q et al (2019) Kinesio taping for balance function after stroke: a systematic review and meta-analysis. Evid Based Complement Alternat Med 2019:8470235. https://doi.org/10.1155/2019/8470235
Grampurohit N, Pradhan S, Kartin D (2015) Efficacy of adhesive taping as an adjunt to physical rehabilitation to influence outcomes post-stroke: a systematic review. Top Stroke Rehabil 22(1):72–82. https://doi.org/10.1179/1074935714Z.0000000031
Cho YH, Cho KH, Park SJ (2020) Effects of trunk rehabilitation with kinesio and placebo taping on static and dynamic sitting postural control in individuals with chronic stroke: A randomized controlled trial. Top Stroke Rehabil. 1–10. https://doi.org/10.1080/10749357.2020.1747672
Deng P, Zhao Z, Zhang S, et al. (2020) Effect of kinesio taping on hemiplegic shoulder pain: a systematic review and meta-analysis of randomized controlled trials. Clin Rehabil. 269215520964950. https://doi.org/10.1177/0269215520964950
Huang YC, Chen PC, Tso HH et al (2019) Effects of kinesio taping on hemiplegic hand in patients with upper limb post-stroke spasticity: a randomized controlled pilot study. Eur J Phys Rehabil Med 55(5):551–557. https://doi.org/10.23736/S1973-9087.19.05684-3
Dall’Agnol MS, Cechetti F (2018) Kinesio taping associated with acupuncture in the treatment of the paretic upper limb after stroke. J Acupunct Meridian Stud 11(2):67–73. https://doi.org/10.1016/j.jams.2017.12.003
Hochsprung A, Dominguez-Matito A, Lopez-Hervas A et al (2017) Short- and medium-term effect of kinesio taping or electrical stimulation in hemiplegic shoulder pain prevention: a randomized controlled pilot trial. NeuroRehabilitation 41(4):801–810. https://doi.org/10.3233/NRE-172190
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 151(4):264–9. https://doi.org/10.7326/0003-4819-151-4-200908180-00135 (W64)
Davenport MH, Meah VL, Ruchat SM et al (2018) Impact of prenatal exercise on neonatal and childhood outcomes: a systematic review and metaanalysis. Br J Sports Med. 52:1386–1396
Higgins JP, Altman DG, Gotzsche PC et al (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 343:d5928. https://doi.org/10.1136/bmj.d5928
JelenaSavović LW, Sterne JAC, Turner L et al (2014) Evaluation of the Cochrane collaboration’s tool for assessing the risk of bias in randomized trials:focus groups, online survey, proposed recommendations and their implementation. Systematic Reviews. 3(37):1–12
Akl EA, Sun X, Busse JW et al (2012) Specific instructions for estimating unclearly reported blinding status in randomized trials were reliable and valid. J Clin Epidemiol 65(3):262–267. https://doi.org/10.1016/j.jclinepi.2011.04.015
Andrea D, Furlan VP, Bombardier C et al (2009) Updated method guidelines for systematic reviews in the cochrane back review group. Spine. 34(18):1929–1941
Brannick CJFMT (2012) Supplemental material for publication bias in psychological science: prevalence, methods for identifying and controlling, and implications for the use of meta-analyses. Psychol Methods. 17(1):120–128. https://doi.org/10.1037/a0024445.supp
Egger M, Smith GD, Schneider M et al (1997) Bias in meta›analysis detected by a simple, graphical test. BMJ 316:629–634
Chen B, Ke M, Meng Z et al (2018) Influence of early application of intramuscular tape on shoulder pain in hemiplegic after stroke. Chin J Phys Med Rehabil 40(6):448–450
Huang YC, Pl C, Wang L et al (2016) Effect of kinesiology taping on hemiplegic shoulder pain and functional outcomes in subacute stroke patients:a randomized controlled study. Eur J phys rehabil Med 52(6):774–81
Huang YC, Chang KH, Liou TH et al (2017) Effects of kinesio taping for stroke patients with hemiplegic shoulder pain: a double-blind, randomized, placebo-controlled study. J Rehabil Med 49(3):208–215. https://doi.org/10.2340/16501977-2197
EUNG-BEOM KIM Y-DK (2015) Effects of kinesiology taping on the upper-extremity function and activities of daily living in patients with hemiplegia. J Phys Ther Sci 27(5):1455–1457
Chunxia Li, Chengmao JI, Haicheng Chen et al (2019) Clinical effects of kinesio taping combined with rehabilitation treatment and training on shoulder pain after stroke. Medical Journal of Chinese People’s Health. 31(15):79–81
Shi B, Li K, Yanhu H et al (2018) Therapeutic effectiveness of kinesio taping for relieving shoulder pain in stroke patients with shoulder subluxation. Chinese J Rehabil Med 33(3):310–314
Si B, Tan H (2019) Clinical effect of kinesio taping and joint mobilization in the treatment of hemiplegic shoulder pain. J Clin Pathol Res 39(12):2747–2751. https://doi.org/10.3978/j.issn.2095-6959.2019.12.018
Yang Y, Zhu Y (2016) Effects of kinesio taping on spasticity of upper limbs after stroke. Chin J Rehabil Theory Pract 22(9):1045–1048
Zhao L, Wang J (2017) Effect of kinesio taping on subluxation of shoulder in hemiplegic patients after stroke. Chin J Rehabil Theory Pract 23(10):1200–1202. https://doi.org/10.3969/j.issn.1006-9771.2017.10.016
Yang L, Yang J, He C (2018) The effect of kinesiology taping on the hemiplegic shoulder pain: a randomized controlled trial. J Healthc Eng 2018:8346432. https://doi.org/10.1155/2018/8346432
Sharp K, Hewitt J (2014) Dance as an intervention for people with Parkinson’s disease: a systematic review and meta-analysis. Neurosci Biobehav Rev 47:445–456. https://doi.org/10.1016/j.neubiorev.2014.09.009
Ghozy S, Dung NM, Morra ME et al (2019) Efficacy of kinesio taping in treatment of shoulder pain and disability: a systematic review and meta-analysis of randomised controlled trials. Physiotherapy 107:176–188. https://doi.org/10.1016/j.physio.2019.12.001
Donec V, Kubilius R (2019) The effectiveness of kinesio taping(R) for pain management in knee osteoarthritis: a randomized, double-blind, controlled clinical trial. Ther Adv Musculoskelet Dis 11:1759720X19869135. https://doi.org/10.1177/1759720X19869135
Ramirez-Velez R, Hormazabal-Aguayo I, Izquierdo M et al (2019) Effects of kinesio taping alone versus sham taping in individuals with musculoskeletal conditions after intervention for at least one week: a systematic review and meta-analysis. Physiotherapy 105(4):412–420. https://doi.org/10.1016/j.physio.2019.04.001
Lim EC, Tay MG (2015) Kinesio taping in musculoskeletal pain and disability that lasts for more than 4 weeks: is it time to peel off the tape and throw it out with the sweat? A systematic review with meta-analysis focused on pain and also methods of tape application. Br J Sports Med 49(24):1558–1566. https://doi.org/10.1136/bjsports-2014-094151
ParreiraPdo C, Costa Lda C, Takahashi R et al (2014) Kinesio taping to generate skin convolutions is not better than sham taping for people with chronic non-speci fi c low back pain: a randomised trial. J Physiother 60(2):90–96. https://doi.org/10.1016/j.jphys.2014.05.003
Huang TS, Ou HL, Lin JJ (2019) Effects of trapezius kinesio taping on scapular kinematics and associated muscular activation in subjects with scapular dyskinesis. J Hand Ther. 32(3):345–352. https://doi.org/10.1016/j.jht.2017.10.012
Silva Parreira PdC, Menezes Costa LdC, Takahashi R et al (2013) Do convolutions in kinesio taping matter? Comparison of two kinesio taping approaches in patients with chronic non-specific low back pain: protocol of a randomised trial. Journal of Physiotherapy. 59(1):52. https://doi.org/10.1016/s1836-9553(13)70147-4
Hill NT, Mowszowski L, Naismith SL et al (2017) Computerized cognitive training in older adults with mild cognitive impairment or dementia: a systematic review and meta-analysis. Am J Psychiatry 174(4):329–340. https://doi.org/10.1176/appi.ajp.2016.16030360
Zhang XF, Liu L, Wang BB et al (2019) Evidence for kinesio taping in management of myofascial pain syndrome: a systematic review and meta-analysis. Clin Rehabil 33(5):865–874. https://doi.org/10.1177/0269215519826267
Weber R, Krogias C, Eyding J et al (2019) Age and sex differences in ischemic stroke treatment in a nationwide analysis of 1.11 million hospitalized cases. Stroke 50(12):3494–3502. https://doi.org/10.1161/STROKEAHA.119.026723
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
This brief report has not been submitted to any other journal.
Informed consent
All authors agree to the submission.
Conflict of interest
The authors declare no competing interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
What is Known Kinesiology taping has become increasingly popular in rehabilitation for upper limb function of hemiplegic patients, Yet its effects remain controversial
What is New Altogether 12 studies were included in this meta-analysis, we found that kinesiology taping could be recommended to improve upper limb function in patients with stroke in pain intensity, shoulder subluxation, general disability, upper extremity function, and the PROM of flexion.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wang, Y., Li, X., Sun, C. et al. Effectiveness of kinesiology taping on the functions of upper limbs in patients with stroke: a meta-analysis of randomized trial. Neurol Sci 43, 4145–4156 (2022). https://doi.org/10.1007/s10072-022-06010-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-022-06010-1