
Abstract
Purpose
COVID-19 pandemic has affected most components of health systems including rehabilitation. The study aims to compare demographic and clinical data of patients admitted to an intensive rehabilitation unit (IRU) after severe acquired brain injuries (sABIs), before and during the pandemic.
Materials and methods
In this observational retrospective study, all patients admitted to the IRU between 2017 and 2020 were included. Demographics were collected, as well as data from the clinical and functional assessment at admission and discharge from the IRU. Patients were grouped in years starting from March 2017, and the 2020/21 cohort was compared to those admitted between March 2017/18, 2018/19, and 2019/20. Lastly, the pooled cohort March 2017 to March 2020 was compared with the COVID-19 year alone.
Results
This study included 251 patients (F: 96 (38%): median age 68 years [IQR = 19.25], median time post-onset at admission: 42 days, [IQR = 23]). In comparison with the pre-pandemic years, a significant increase of hemorrhagic strokes (p < 0.001) and a decrease of traumatic brain injuries (p = 0.048), a reduction of the number of patients with a prolonged disorder of consciousness admitted to the IRU (p < 0.001) and a lower length of stay (p < 0.001) were observed in 2020/21.
Conclusions
These differences in the case mix of sABI patients admitted to IRU may be considered another side-effect of the pandemic. Facing this health emergency, rehabilitation specialists need to adapt readily to the changing clinical and functional needs of patients’ addressing the IRUs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The COVID-19 pandemic has strongly affected components of healthcare systems, including rehabilitation [1]. Since the World Health Organization WHO declared the pandemic on March 11, 2020, the global situation has been rapidly evolving. The epicenter of the disease, initially located in China, has shifted to Europe, and gradually spread throughout the world. Many countries, such as the USA, the UK, Italy, Spain, France, and, later, Brazil and India, have been severely affected, in terms of deaths, severe cases, health risk, and economic collapse. In Italy, since the beginning of spring 2020, the first wave has mainly affected the north of the country [2] later spreading throughout the central and southern Italy. Within a few weeks, the health system had to modify its usual functioning: hospital medical check-ups were postponed, and only urgent visits were guaranteed, while some medical, surgical, and rehabilitation wards were reconverted [3], allowing the reallocation of health professionals to the care of COVID-19 and post-COVID-19 patients, including those needing intensive care [4]. In addition, primary care physicians, overburdened by the management of COVID-19 patients, reduced access to their surgeries, also in order to limit the risk of infection. In this context, the rehabilitation services had also to adapt to the new situation, and face increased patients’ needs, not only as a consequence of prolonged immobilization and acute pulmonary and neurological complications from COVID-19 [5,6,7] but, also, as a consequence of health and civil mitigation measures [8]. On one hand, rehabilitation hospital facilities became less accessible than usual, inducing rehabilitation health professionals to develop or adopt new means of care, thus giving impulse to the diffusion of telerehabilitation in the fields of physical therapy, occupational therapy, and speech and language therapy [9, 10]. On the other hand, those inpatient rehabilitation facilities that remained active had to adapt to meet the changing needs of patients discharged from acute care hospitals. First, this has required a general understanding of the rehabilitation needs of post-COVID-19 patients, constantly evolving according to the level of knowledge about the post-COVID-19 syndrome [11]. Furthermore, the pandemic has created an enormous pressure on the intensive care units (ICUs) to increase their patients’ turnover and admit more and more severe COVID-19 patients, thus increasing the demand for transferring severely disabled patients from intensive care settings to intensive rehabilitation facilities.
Intensive rehabilitation units (IRUs) for severe acquired brain injuries (sABIs) admit patients with traumatic, post-anoxic, vascular, or other brain injuries that cause coma for at least 24 h and often lead to a permanent disability with sensory, motor, cognitive, and/or behavioral impairment. After sABI, many patients may remain in a state of prolonged disorder of consciousness (DoC) [12] that includes (1) unresponsive waking state (UWS), in which the eyes are open, but there is no evidence of voluntary responses; (2) minimal consciousness state (MCS), an intermediate state in which minimal, inconstant but visible signs of responsiveness are present [13]. Typically, patients with sABI are highly complex, and frequently require life support interventions during the acute phase. To our knowledge, no studies have yet addressed the possible changes on sABI IRUs’ activity and case mix, during the pandemic. This study aims to investigate possible changes in demographics, clinical features, and outcomes of sABI patients admitted to the IRU of the IRCCS-Fondazione Don Gnocchi of Florence before and during the pandemic, by comparing the March 2020 to March 2021 cohort to the March–March cohorts of the previous 3 years.
Materials and methods
A non-concurrent cohort study design was conducted, following STROBE guidelines [14]. In this observational retrospective monocentric study, all patients admitted to the IRU between March 2017 and March 2020 were included. Previous years could not be included since the current admission and discharge assessment has been carried out only since January 2017. Demographic and clinical data were recorded, including age, gender, clinical etiology, and time post-onset (TPO) at admission. A multidimensional clinical and functional assessment was performed by skilled health professionals (neurologists, speech therapists, physiotherapists) both at admission and discharge. Patients’ level of consciousness was classified according to the Italian version of the coma recovery scale-revised (CRS-R) [15], administered repeatedly at least 5 times, within the first week from admission and during the last week before discharge, to reduce the risk of error due to frequent fluctuations in consciousness: the best obtained score was considered for this analysis [16]. The functional status was assessed at admission and discharge by the functional independency measure (FIM) [17], and the disability rating scale (DRS) [18]. Additionally, dysphagia severity was measured by the food oral intake scale (FOIS) [19]. Patients admitted between March 2020 and March 2021 were compared to those admitted between March 2017 and March 2018, and between March 2018 and March 2019 and between March 2019 and March 2020 for all admission and discharge variables, as well as for length of stay (LoS) in the IRU. Written informed consent from the patient or the legal guardian to the anonymous use of their routinely collected data for quality assessment and research purposes was provided at admission to the IRU. The Institutional Ethics Committee approved the study. (Protocol numb: 17505_oss).
Statistical analysis
Descriptive statistics have been calculated for each variable across the assessed recruiting years, testing such variables for normality with the Shapiro–Wilk test. Median and interquartile range were used for the description of numerical variables while occurrences were reported for categorical ones. According to the normality test results, either ANOVA or Kruskal–Wallis test were applied to the numerical variables to evaluate whether the studied variables significantly differed across groups year cohorts. Post hoc analysis, via Dunn-Bonferroni pairwise tests, was carried out for all the pairs of groups, using the Bonferroni correction.
The differences across year cohorts in categorical variables (etiology and gender) were analyzed by chi-square test followed by independent samples z-test with Bonferroni correction for post hoc analysis.
As an additional analysis, DoC and No-Doc patients were analyzed separately by a Kruskal–Wallis test, to check the LoS differences across years for each subset.
Finally, in addition to single year analysis, all the variables were also evaluated comparing the pooled group of pre-pandemic years (2017–2019) and the COVID-19 year, by means of chi-square or Mann–Whitney tests, according to the nature of the variable. In all analyses, a p-value < 0.05 was considered statistically significant.
Results
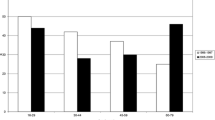
A total of 251 (2017: 63, 2018: 57, 2019: 69 and 2020: 62) patients were included (F: 96, 38%) with median age 68 years [IQR = 19.25], median TPO: 42 days [IQR = 33], traumatic etiology 66 (28%), anoxic etiology 25 (10.2%), ischemic etiology: 48 (19.5), hemorrhagic etiology: 80 (32.5). Comparing demographic and clinical characteristics at admission, the differences in age and functional status between the four cohorts were not significant (Table 1). Conversely, both the CRS-R total score (χ2 (3) = 14.561, p = 0.002) and the number of patients with DoC (UWS and MCS) (χ2 = 15.502, p < 0.001) were significantly different between the groups. Also, post hoc tests revealed a significant difference between the CRS-R total scores in 2020 and each of the previous years’ cohorts, and a significant decrease of patients with DoC in 2020 versus each of the previous considered years (Fig. 1). A confirmation of this was found in the comparison between the 2020/21 vs. the pooled 2017–2019 group (p < 0.01) (Table 2).

Bar plot of significant categorical variables in the multiple years chi-square analysis (upper panels) and box plot of significant numerical variables in the KW groups comparison. Groups with a triangle are significantly different from groups with an asterisk. TPO (time post-onset), LoS (length of stay), CRS-R (coma recovery scale-revised)
The TPO, significant in the KW test χ2 (3) = 12.277, p = 0.006, when entering the post hoc analysis resulted in a significant difference between the 2020–2021 and 2018–2019. A confirm of this was found in the comparison between the 2020/21 vs. the pooled 2017–2019 group (p < 0.01) (Table 2).
A significant difference of sABI aetiologies across the years (χ2 = 26.5, p = 0.009) was also found. The z-tests showed a strongly significant increase of hemorrhagic brain injuries in 2020/21, compared to either 2017 (z = 3.9, p < 0.001), 2018 (z = 3.2, p = 0.002), or 2019 (z = 3.7, p < 0.001) (Table 2, Fig. 1). Etiology was also found to be different between the pooled group and the pandemic-group (χ2 = 25.5, p < 0.001). Specifically, a significant increase of hemorrhagic (pooled 2017–2019: 46 (13.4%) vs. 2020: 34 (57.6%); χ2 = 22.3, p < 0.001) and a decrease of traumatic patients (pooled 2017–2019: 56 (29.9%) vs. 2020: 10 (16.9%); χ2 = 39, p = 0.048) was found.
The patients’ LoS was found to be significantly different across years (χ2(3) = 13.9, p = 0.003). All the pairwise comparisons between 2020/21 and all the previous years resulted significant in the post hoc analysis (2017: p = 0.008; 2018: p = 0.008; 2019: p = 0.026) showing a significant reduction of the LoS in the 2020/2021 cohort, as shown in Fig. 1. A confirmation of this was found in the comparison between the 2020/21 vs. the pooled 2017–2019 group (p < 0.001, Table 2.).
At discharge, consciousness and functional scales were similar in the four considered cohorts (Table 1).
Performing separate analyses on the DoC and No-Doc patients, for the DoC group we did not find any significant differences in the LoS across the years (p = 0.246) while the No-DoC group showed a significant decrease in LoS in 2020/21 (χ2 (3) = 12.9, p = 0.005). For the No-DoC group, we performed post hoc analysis resulting in the year 2020/21 showing a significantly shorter LoS than all previous years (2017: p = 0.003; 2018: p = 0.04; 2019: p = 0.031).
Discussion
COVID-19 pandemic has deeply affected health care at several levels. Intensive rehabilitation settings have faced an increasing demand, to relieve the COVID-19-related overload on ICUs. Due to the speed and severity of the COVID-19 pandemic, not only ICUs, but also IRUs had to adapt rapidly to the pandemic. However, reports on how these changes have taken place are still scarce. In the present study, we investigated the possible changes in case mix, LoS, and outcomes of the cohort of the IRU in-patients in sABI survivors in 2020/21, compared to the data on patients admitted in the same time frame (March–March) of the previous 3 years. Our first finding was that, at admission, the median total CRS-R score was significantly higher, and the number of patients with a DoC significantly lowers during the pandemic in comparison with the previous 3 years. Given that the clinical and instrumental criteria for the selection of patients to be transferred to the IRU [20] were not changed during the pandemic, and that, under current regulations, no withdrawal of life support is practiced in Italian ICUs, this result could be attributed to a higher mortality of the most severe sABI patients during the acute phase, due to an overload of the emergency services, community- and hospital-based [21]. Indeed, this possibility was seriously considered by the American Society of Neurology. The latter, aware of the negative effects of the COVID-19 health emergency on the quality of care provision for several diseases, including stroke, has recently published recommendations for the management of stroke during the acute phase taking into account the global health emergency [22]. In fact, a marked rise of major strokes, requiring primary thrombectomies due to longer onset-to-door and door-to-treatment times has been reported during the pandemic [23]. In addition, a reduction by half of the hospital diagnosed minor strokes and transient ischemic attacks (TIAs), and of transfers from spokes were reported in 2020, compared to 2019 [24]. Thus, although our perspective did not include a direct investigation on ICUs, it is quite possible that the reduction of the number of patients with DoC observed in the present study may be related to their higher mortality in emergency and acute care settings, due to the critical delays in stroke acute care and the possible overloading of territorial emergency services during the pandemic.
Unlike the level of consciousness, we found that the TPO did not significantly change across the four considered years, probably because, once the patient enters the ICU, the reach of the criteria for referral to the rehabilitation ward, depending on the patient’s hemodynamic stability, can hardly be accelerated.
Second, a significant reduction in post-traumatic patients, paralleled by a significant increase of post-hemorrhagic patients, was observed in patients admitted to the IRU. The relative and absolute reduction of post-traumatic patients, shown in the pooled data comparison, can be ascribed to the sharp reduction in population mobility and sport activities due to the numerous lockdowns imposed by the government, that has been reported to lead to a reduction of traumas and traumatic brain injuries [24, 25]. The increase of post-hemorrhagic sABI might be related to the parallel significant reduction of post-traumatic patients; however, this increase, confirmed for each year of the pre-COVID-19 period, regarded specifically only hemorragic stroke patients. The International literature on stroke hospital presentation during COVID-19 pandemic initially reported a decline of stroke, possibly due to less persons seeking hospital care during the pandemic [26, 27]. However, these studies were mainly focused on mild and minor stroke, presenting with stroke-like focal deficit [28]. In fact, more recent publications underline the simultaneous increase in major strokes alongside the reduction in minor strokes and TIAs [29]. The limited number of cases of this single site study and the lack of epidemiological data on our reference population do not allow any inference on the causes of this increase. Nevertheless, the possibility of a negative impact of pandemic on management of medical conditions, such as hypertension, with expected increased incidence of complications, including severe cerebral hemorrhage [30] should also deserve further investigation.
Regarding the rehabilitation process and outcomes, some substantial changes can be highlighted. First of all, a significant reduction in the LoS in the IRU has been observed during the pandemic, as compared to previous years. This overall reduction was not only related to the reduced access of patients with DoC, who generally stay longer in the IRU. Indeed, patients with DoC maintained a stable LoS before and after pandemic, but patients who were not in DoC at admission had a significantly lower LoS during the pandemic than before. The reasons for this are complex. Probably, the most relevant issue was the pressure from families and patients to accelerate the return home, both for fear of exposing the patients to the virus by remaining in a hospital community, and for the major limitations for family/caregivers to access the ward because of the pandemic. Actually, while the interdisciplinary assessment and treatment of our sABI patients did not substantially change during the pandemic, the usual involvement of families in supporting the patients’ recovery, including the caregivers’ training sessions, were only exceptionally allowed during the pandemic. To minimize the emotional impact on patients and caregivers, a video call service was carried out by the team psychologists, when the patient could actually participate to the calls, and team meetings with families were regularly held by video calls, but the limited or no physical access to the patients surely prompted most families to dedicate extra efforts to promote all environmental and social adaptations necessary for home discharge. Moreover, it can be assumed that the reduction of patients in DoC, those with the highest care and rehabilitation burden, possibly allowed the interdisciplinary team to dedicate more time and efforts, during the pandemic, to promote rehabilitation goals other than stimulating consciousness. This included not only strategies to support the families towards earlier home discharge, but also providing any effort to promote earlier decannulation, since this step, along with the recovery of consciousness, is a general criterion, either for home discharge or for transferring the patient to a less specialized rehabilitation setting.
If the absence of difference between outcome scales before and during the pandemic apparently reflects that standards of care have been maintained despite the pandemic-induced upheaval, the hypothesis that anticipating the IRU discharge may have reduced the time dedicated to rehabilitation of neurocognitive and participatory skills deserves to be raised. Indeed, as a limitation of our study, the scales routinely used at discharge from IRU do not capture this information. On the other hand, the possible functional benefits of earlier home discharge need also to be investigated in the long term. Although our observations are limited to one IRU, the question of whether the immediate economic savings due to the shortening of LoS in high specialty IRUs might be associated to possible consequences on the cognitive profile and the degree of family, work, and social participation of sABI patients deserves further investigation. For the patients involved in this analysis, a longitudinal follow-up study is currently being carried out to investigate this issue.
Conclusions
These differences in the case mix of sABI patients admitted to IRU, and the changes in the related rehabilitation processes and outcomes, may be considered another side-effect of the pandemic, with some possible consequences that might be investigated only in the long term.
Abbreviations
- ICUs:
-
Intensive care units
- IRUs:
-
Intensive rehabilitation units
- sABIs:
-
Severe acquired brain injuries
- DoC:
-
Disorders of consciousness
- UWS:
-
Unresponsive waking state
- MCS:
-
Minimal consciousness state
- TPO:
-
Time post-onset
- CRS-R:
-
Coma recovery scale-revised
- FIM:
-
Functional independency measure
- DRS:
-
Disability rating scale
- FOIS:
-
Food oral intake scale
- LoS:
-
Length of stay
- KW:
-
Kruskal-Wallis
- MW:
-
Mann-Whitney
- TIAs:
-
Transient ischemic attacks
References
Leocani, L., Diserens, K., Moccia, M., Caltagirone, C., & Neurorehabilitation scientific panel of the European Academy of Neurology-EAN (2020) Disability through COVID-19 pandemic: neurorehabilitation cannot wait. Eur J Neurol 27(9):e50–e51. https://doi.org/10.1111/ene.14320
Grasselli G, Pesenti A, Cecconi M (2020) Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: early experience and forecast during an emergency response. JAMA 323(16):1545–1546. https://doi.org/10.1001/jama.2020.4031
Grippo A, Assenza G, Scarpino M, Broglia L, Cilea R, Galimberti CA, Lanzo G, Michelucci R, Tassi L, Vergari M, Di Lazzaro V, Mecarelli O, SINC, LICE, and AITN, (2020) Electroencephalography during SARS-CoV-2 outbreak: practical recommendations from the task force of the Italian Society of Neurophysiology (SINC), the Italian League Against Epilepsy (LICE), and the Italian Association of Neurophysiology Technologists (AITN). Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology 41(9):2345–2351. https://doi.org/10.1007/s10072-020-04585-1
Bartolo, M., Intiso, D., Lentino, C., Sandrini, G., Paolucci, S., Zampolini, M., & Board of the Italian Society of Neurological Rehabilitation (SIRN) (2020) Urgent measures for the containment of the coronavirus (Covid-19) epidemic in the neurorehabilitation/rehabilitation departments in the phase of maximum expansion of the epidemic. Front Neurol 11:423. https://doi.org/10.3389/fneur.2020.00423
Scarpino, M., Bonizzoli, M., Lazzeri, C., Lanzo, G., Lolli, F., Ciapetti, M., Hakiki, B., Grippo, A., Peris, A., NeuCOV Study Group†, Ammannati, A., Baldanzi, F., Bastianelli, M., Bighellini, A., Boccardi, C., Carrai, R., Cassardo, A., Cossu, C., Gabbanini, S., Ielapi, C., … Troiano, S (2021) Electrodiagnostic findings in patients with non-COVID-19- and COVID-19-related acute respiratory distress syndrome. Acta Neurol Scand 144(2):161–169. https://doi.org/10.1111/ane.13433
Estraneo A, Ciapetti M, Gaudiosi C, Grippo A (2021) Not only pulmonary rehabilitation for critically ill patients with COVID-19. J Neurol 268(1):27–29. https://doi.org/10.1007/s00415-020-10077-1
Zhao H, Shen D, Zhou H, Liu J, Chen S (2020) Guillain-Barré syndrome associated with SARS-CoV-2 infection: causality or coincidence? The Lancet Neurology 19(5):383–384. https://doi.org/10.1016/S1474-4422(20)30109-5
Lazzerini M, Putoto G (2020) COVID-19 in Italy: momentous decisions and many uncertainties. Lancet Glob Health 8(5):e641–e642. https://doi.org/10.1016/S2214-109X(20)30110-8
Tenforde AS, Borgstrom H, Polich G, Steere H, Davis IS, Cotton K, O’Donnell M, Silver JK (2020) Outpatient physical, occupational, and speech therapy synchronous telemedicine: a survey study of patient satisfaction with virtual visits during the COVID-19 pandemic. Am J Phys Med Rehabil 99(11):977–981. https://doi.org/10.1097/PHM.0000000000001571
Wang CC, Chao JK, Chang YH, Chou CL, Kao CL (2020) Care for patients with musculoskeletal pain during the COVID-19 pandemic: physical therapy and rehabilitation suggestions for pain management. Journal of the Chinese Medical Association : JCMA 83(9):822–824. https://doi.org/10.1097/JCMA.0000000000000376
Carda, S., Invernizzi, M., Bavikatte, G., Bensmaïl, D., Bianchi, F., Deltombe, T., Draulans, N., Esquenazi, A., Francisco, G. E., Gross, R., Jacinto, L. J., Moraleda Pérez, S., O'dell, M. W., Reebye, R., Verduzco-Gutierrez, M., Wissel, J., & Molteni, F. (2020). COVID-19 pandemic. What should physical and rehabilitation medicine specialists do? A clinician’s perspective. European journal of physical and rehabilitation medicine, 56(4), 515–524. https://doi.org/10.23736/S1973-9087.20.06317-0
Hirschberg R, Giacino JT (2011) The vegetative and minimally conscious states: diagnosis, prognosis and treatment. Neurol Clin 29(4):773–786. https://doi.org/10.1016/j.ncl.2011.07.009
Giacino JT, Ashwal S, Childs N, Cranford R, Jennett B, Katz DI, Kelly JP, Rosenberg JH, Whyte J, Zafonte RD, Zasler ND (2002) The minimally conscious state: definition and diagnostic criteria. Neurology 58(3):349–353. https://doi.org/10.1212/wnl.58.3.349
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, Initiative STROBE (2008) The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 61(4):344–349. https://doi.org/10.1016/j.jclinepi.2007.11.008
Estraneo, A., Moretta, P., De Tanti, A., Gatta, G., Giacino, J. T., Trojano, L., & Italian Crs-R Multicentre Validation Group (2015) An Italian multicentre validation study of the coma recovery scale-revised. Eur J Phys Rehabil Med 51(5):627–634
Wannez, S., Heine, L., Thonnard, M., Gosseries, O., Laureys, S., & Coma Science Group collaborators (2017) The repetition of behavioral assessments in diagnosis of disorders of consciousness. Ann Neurol 81(6):883–889. https://doi.org/10.1002/ana.24962
Hall KM, Mann N, High W (1996) Functional measures after traumatic brain injury: ceiling effects of FIM, FIM+FAM. DRS and CIQ Journal of Head Trauma Rehabilitation 11:27–39
Gouvier WD, Blanton PD, LaPorte KK, Nepomuceno C (1987) Reliability and validity of the disability rating scale and the levels of cognitive functioning scale in monitoring recovery from severe head injury. Arch Phys Med Rehabil 68(2):94–97
Battel, I., Calvo, I., & Walshe, M. (2018). Cross-cultural validation of the Italian version of the functional oral intake scale. folia phoniatrica et logopaedica : official organ of the international association of Logopedics and Phoniatrics (IALP), 70(3–4), 117–123. https://doi.org/10.1159/000490792
Regione Toscana: percorso assistenziale per le persone con Gravi Cerebrolesioni Acquisite (GCA) – utilizzo della scheda filtro (marzo 2014)
raccomandazioni di etica clinica per l’ammissione a trattamenti intensivi e per la loro sospensione, in condizioni eccezionali di squilibrio tra necessità e risorse disponibili. società italiana anestesia, analgesia, rianimazione e terapia intensiva - jul , 2020
Leira EC, Russman AN, Biller J, Brown DL, Bushnell CD, Caso V, Chamorro A, Creutzfeldt CJ, Cruz-Flores S, Elkind M, Fayad P, Froehler MT, Goldstein LB, Gonzales NR, Kaskie B, Khatri P, Livesay S, Liebeskind DS, Majersik JJ, Moheet AM, Worrall BB (2020) Preserving stroke care during the COVID-19 pandemic: potential issues and solutions. Neurology 95(3):124–133. https://doi.org/10.1212/WNL.0000000000009713
Baracchini C, Pieroni A, Viaro F, Cianci V, Cattelan AM, Tiberio I, Munari M, Causin F (2020) Acute stroke management pathway during Coronavirus-19 pandemic. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology 41(5):1003–1005. https://doi.org/10.1007/s10072-020-04375-9
Pinggera D, Klein B, Thomé C, Grassner L (2021) The influence of the COVID-19 pandemic on traumatic brain injuries in Tyrol: experiences from a state under lockdown. European journal of trauma and emergency surgery: official publication of the European Trauma Society 47(3):653–658. https://doi.org/10.1007/s00068-020-01445-7
Munari, M., DE Cassai, A., Casartelli Liviero, M., Zanatta, P., Martin, M. A., Soragni, A., Maiorelli, G., Benetton, C., Dall'acqua, G., Chioffi, F., & Navalesi, P. (2021). SARS-CoV-2 pandemic impact on traumatic brain injury epidemiology: an overview of the Veneto region. Minerva anestesiologica, 87(4), 489–490. https://doi.org/10.23736/S0375-9393.20.15148-4
Aguiar de Sousa D, van der Worp HB, Caso V, Cordonnier C, Strbian D, Ntaios G, Schellinger PD, Sandset EC, Organisation ES (2020) Maintaining stroke care in Europe during the COVID-19 pandemic: results from an international survey of stroke professionals and practice recommendations from the European Stroke Organisation. Eur Stroke J 5(3):230–236. https://doi.org/10.1177/2396987320933746
Uchino K, Kolikonda MK, Brown D, Kovi S, Collins D, Khawaja Z, Buletko AB, Russman AN, Hussain MS (2020) Decline in stroke presentations during COVID-19 surge. Stroke 51(8):2544–2547. https://doi.org/10.1161/STROKEAHA.120.030331
Jasne AS, Chojecka P, Maran I, Mageid R, Eldokmak M, Zhang Q, Nystrom K, Vlieks K, Askenase M, Petersen N, Falcone GJ, Wira CR 3rd, Lleva P, Zeevi N, Narula R, Amin H, Navaratnam D, Loomis C, Hwang DY, Schindler J, Sharma R (2020) Stroke code presentations, interventions, and outcomes before and during the COVID-19 pandemic. Stroke 51(9):2664–2673. https://doi.org/10.1161/STR.0000000000000347
Masroor S (2020) Collateral damage of COVID-19 pandemic: delayed medical care. J Card Surg 35(6):1345–1347. https://doi.org/10.1111/jocs.14638
Talevi D, Socci V, Carai M, Carnaghi G, Faleri S, Trebbi E, di Bernardo A, Capelli F, Pacitti F (2020) Mental health outcomes of the CoViD-19 pandemic. Riv Psichiatr 55(3):137–144. https://doi.org/10.1708/3382.33569
Funding
This study was funded by RICERCA CORRENTE 2020 from IRCCS Don Gnocchi.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The Institutional Ethics Committee approved the study: Protocol numb: 17505_oss.
Consent to participate.
Informed consent was obtained from the parents.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hakiki, B., Grippo, A., Scarpino, M. et al. Effects of COVID-19 pandemic on intensive rehabilitation after severe acquired brain injuries. Neurol Sci 43, 791–798 (2022). https://doi.org/10.1007/s10072-021-05709-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-021-05709-x