
Abstract
Synovial osteochondromatosis is an extremely rare benign condition in children and adolescents that have joint pain as a presenting manifestation. It is usually monoarticular with the knee as the most common affected joint. In this article, we describe the case of a female adolescent suffering from debilitating chronic right knee pain initially mimicking juvenile idiopathic arthritis, who was subsequently diagnosed with primary synovial osteochondromatosis. We present a review of synovial osteochondromatosis focusing on the clinical manifestations, radiographic features, histopathologic findings, and treatment, with a summarized review of pediatric patients with initial musculoskeletal presentations who were ultimately diagnosed as synovial osteochondromatosis. Although synovial osteochondromatosis is rare in children and adolescents, this condition should be included in the differential diagnosis of joint pain and may mimic juvenile idiopathic arthritis. Appropriate diagnostic radiography, including both plain radiography and magnetic resonance imaging, is necessary to accurately diagnose this condition. We also emphasize the importance of a multidisciplinary team approach to managing patients with synovial osteochondromatosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Primary synovial osteochondromatosis is a rare benign condition that is characterized by cartilaginous metaplasia in the synovium, bursa, and tendon sheath, followed by secondary calcification, ossification, and detachment that results in the presence of loose bodies [1]. The etiology of this condition remains unknown. This condition is most commonly found in adult males during the third to fifth decades of life, and it is very rare in children and adolescents [2]. It commonly manifests as monoarticular joint pain, although involvement of more than one joint has been reported [3]. Any joints can be involved; however, among the large joints, the knees, hips, and elbows are more commonly affected, and the shoulders, wrists, and ankles are less commonly affected [4]. Here, we describe the case of a female adolescent suffering from debilitating chronic right knee pain who was subsequently diagnosed with primary synovial osteochondromatosis.
Case report description
A 12-year-old female presented with chronic right knee pain for 2 months. From the history, she was previously diagnosed with and treated for juvenile idiopathic arthritis (JIA). She was given non-steroidal anti-inflammatory drugs, methotrexate, and sulfasalazine for 1 month; however, her knee pain worsened. She was then referred to the Faculty of Medicine Siriraj Hospital, Mahidol University — Thailand’s largest national tertiary referral center — for further investigations and treatment. The patient’s right knee pain was aggravated by movement and weight-bearing, and she was in a wheelchair. She denied morning stiffness, but subjectively reported occasional swelling at her right knee. She denied preceding trauma or prior intraarticular corticosteroid injection. From review of systems, there was history of chronic abdominal pain without other symptoms.
On physical examination, she had difficulty bearing weight on her right knee due to pain. The right knee was mildly swollen with tenderness over the entire anterior aspect, and along the lateral joint line of the right knee. No warmth or erythema was detected. Due to the findings of the mildly swollen right knee and tenderness, it was possible that she had arthritis at the right knee. Her other joints and entheses were unaffected. She had no rash and no conjunctival injection. Abdominal examination was unremarkable.
The results of her laboratory investigations were as follows: complete blood count (CBC): white blood cell count 5910/µL, hemoglobin 12.7 g/dL, and platelet 400,000/µL; erythrocyte sedimentation rate (ESR) 17 mm/h (0–20 mm/h); C-reactive protein (CRP) concentration 0.74 mg/L (< 5.0 mg/L); negative rheumatoid factor (RF); negative antinuclear antibodies (ANA); and negative human leucocyte antigen (HLA)-B27. Esophagogastroduodenoscopy (EGD) and colonoscopy were performed due to history of chronic abdominal pain from review of systems and both results were negative.
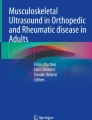
Preoperative plain radiography of both knees is shown in Fig. 1, and preoperative magnetic resonance imaging (MRI) of the right knee is shown in Fig. 2. Plain radiographs of both knees in anteroposterior (AP) view (Fig. 1A), and lateral radiograph of the right knee (Fig. 1B) showed multiple intraarticular ossifications within the lateral tibiofemoral compartment and suprapatellar regions. MRI of the right knee in coronal T1-weighted (T1W), coronal post-Gadolinium (Gd) T1-weighted fat suppression (T1WFS), sagittal proton density-weighted (PDW), and sagittal T2-weighted (T2W) images demonstrated multiple intraarticular bodies with low signal intensity on T1W, low signal intensity on T2W, and intermediate signal intensity on PDW without enhancement (Fig. 2A, B, C, D). However, increased synovial thickening and enhancement was observed. Axial PDW fat suppression (PDWFS), 3-dimensional spoiled gradient (3D-SPGR), and post-Gd T1WFS images showed these intraarticular bodies to have cartilaginous signal intensity with partly blooming artifact on the surface suggestive of calcified rims (Fig. 2E, F, G). Coronal T2-weighted fat suppression (T2WFS) images of both knees showed no intraarticular body within left knee (Fig. 2H). These findings were compatible with a diagnosis of synovial osteochondromatosis.

Preoperative plain radiograph of both knees in anteroposterior view (A), and lateral radiograph of the right knee (B). Multiple intraarticular ossifications can be observed in the lateral tibiofemoral compartment and the suprapatellar region (arrows)

MRI of the right knee in coronal T1W (A), coronal post-Gd T1WFS (B), sagittal PDW (C), and sagittal T2W (D) images demonstrated multiple intraarticular bodies with low signal intensity on T1W, low signal intensity on T2W, and intermediate signal intensity on PDW without enhancement (white arrows). However, increased synovial thickening and enhancement was observed (arrow heads). Axial PDWFS (E), 3D-SPGR (F), and post-Gd T1WFS (G) images showed these intraarticular bodies to have cartilaginous signal intensity with partly blooming artifact on the surface suggestive of calcified rims (curve arrow). Coronal T2WFS of both knees (H) showed no intraarticular bodies within left knee. (Abbreviations: MRI, magnetic resonance imaging; T1W, T1-weighted; post-Gd: post-gadolinium; T1WFS, T1-weighted fat suppression; PDW, proton density-weighted; T2W, T2-weighted; PDWFS, proton density-weighted fat suppression; 3D-SPGR, 3-dimensional spoiled gradient; T2WFS, T2-weighted fat suppression)
An orthopedic consultation was then requested. Arthroscopic removal of loose bodies and partial synovectomy with synovial biopsy was performed using anterolateral and anteromedial portals. The operative findings are demonstrated in Fig. 3. Multiple chondral bodies were found within the lateral compartment, and most were located beneath the lateral meniscus. Identified bodies were removed with arthroscopic grasping forceps and a motorized shaver. Mild synovitis was observed, but the articular cartilage was intact. Histopathology demonstrated osteocartilagenous nodules, covered by synovial tissue. Clusters of chondrocytes were arranged in lobules. The chondrocytes revealed mild nuclear atypia. Intense calcification and ossification were observed. No pannus, no lymphoid follicles, no acute inflammation, no tumor or granulomatous inflammation had been seen in the tissue. These findings were compatible with synovial osteochondromatosis (Fig. 4A and B).

Surgical findings of the right knee. A Multiple loose bodies at the posterolateral compartment of the knee. B Multiple loose bodies (arrow) beneath the lateral meniscus. C Chondral bodies attached to the synovium posterior to the anterior cruciate ligament. D Loose bodies removed from the knee. (Abbreviations: LFC, lateral femoral condyle; LTP, lateral tibial plateau; ACL, anterior cruciate ligament)

A Histopathology 20 × magnification showed osteocartilagenous tissue and synovial tissue. No pannus formation, no acute inflammation, no lymphoid follicles, and no tumor or granuloma were seen. B In histopathology 100 × magnification, the chondrocytes showed mild nuclear atypia, arranged in clusters and lobules. Intense calcification & ossification were noted
The duration from the patient’s first visit to our center until surgery was 5 months. The lag time in definite diagnosis and treatment was due to the 2019 COVID-19 pandemic, which adversely affected scheduling for both MRI and elective surgery. As such, during the period before MRI and definite diagnosis, the patient continued to receive treatment for presumed JIA with NSAIDS, methotrexate, and sulfasalazine. However, all of these medications were discontinued one week prior to surgery, and they were not restarted after surgery. Postoperative radiograph of both knees in AP view (Fig. 5A) and lateral radiograph of the right knee (Fig. 5B) showed markedly decreased calcification along the lateral compartment of the right knee. The patient’s knee pain rapidly subsided after surgery. At the 10-week follow-up, she was able to walk with no difficulty and she had complete resolution of pain. At the 6-month follow-up, her previous improvements were sustained with additional complete resolution of any morning stiffness, and she had resumed all normal activities of daily living as well as physical activities such as exercise and dancing.

Postoperative plain radiograph of both knees in anteroposterior view (A), and lateral radiograph of the right knee (B). A marked decrease in calcification along the lateral compartment of the right knee can be observed
Discussion and review of the literature
Synovial osteochondromatosis was first described by Laennec in 1813 [5], and the disease can be classified as primary or secondary form. Secondary synovial osteochondromatosis is associated with previous joint diseases or abnormalities, such as trauma, osteoarthritis, osteonecrosis, neuropathic joint, and rheumatoid arthritis, that can develop intraarticular chondral bodies [6]. The etiology of primary synovial osteochondromatosis remains unknown. This disease usually manifests as monoarticular joint pain, joint swelling, and/or palpable mass, and it mainly affects large joints, such as the knees, hips, and elbows, but it can also occasionally develop in the ankles, shoulders, temporomandibular joints, and small joints [7]. Acromio-clavicular joint involvement is very rare but was reported in the pediatric age group [8]. Mechanical pain was reported in 93% of adult patients, with 70% having gradual onset of pain, and 23.3% having acute sudden onset of pain. Eighty-four percent of patients experienced intermittent joint pain, and 16% reported continuous joint pain. Approximately 30% of patients reported increased pain upon physical activity or exercise [9]. In pediatric patients, the most commonly affected joint was the knee [2, 10,11,12,13,14,15,16] followed by the hip [6, 17,18,19,20,21]. Destructive patterns of arthritis and involvement of more than one joint are uncommon findings but have been reported by Emad [3]. The patient was a 14-year-old who presented with chronic pain and swelling of both knees and right ankle, which occurred simultaneously, leading to severe destructive arthropathy due to synovial osteochondromatosis [3]. Moreover, Kistler [11] and Giancane [2] both reported that the common clinical presentation of joint pain could mimic JIA at the onset of disease.
The patient profiled in our report had gradual mechanical pain in her right knee for 2 months that was exaggerated by weight-bearing and other physical activities. Small effusion could be secondary to concomitant synovitis. Concerning the differential diagnoses in our patient, she had chronic monoarticular joint pain at the right knee that could be the presentation of oligoarticular JIA, which usually manifests as chronic monoarthritis or oligoarthritis of the lower extremities, or enthesitis-related arthritis, which can manifest as chronic arthritis in the lower extremities, including the knee joint. Although our patient had physical examination findings of mild swollen right knee and tenderness which can be suggestive of arthritis, she had knee pain that was exacerbated by physical activities, but did not have morning stiffness, which is usually found in inflammatory arthritis, especially JIA. She also had initial normal laboratory results, including CBC, ESR, CRP, and negative HLA-B27 and ANA. She also experienced no clinical improvement despite treatment with NSAIDs and disease-modifying anti-rheumatic drugs. Most importantly, JIA is a diagnosis of exclusion; therefore, the underlying cause of joint paint must be investigated before arriving at a final diagnosis. Another differential diagnosis in this case was inflammatory bowel disease (IBD) with arthropathy because she had a history of chronic abdominal pain in addition to her knee pain, which could be an extragastrointestinal manifestation of IBD. However, we excluded IBD after normal results of EGD and colonoscopy. Her history of activity-related pain, difficulty in weight-bearing, and finding of mild swelling with tenderness of the anterior aspect and lateral joint line of the right knee were important clues that influenced us to suspect structural abnormalities within the knee joint that could result in mechanical MSK pain. Subsequent plain radiography and MRI that were performed were very helpful for making an accurate diagnosis. From the imaging of our patient, synovial osteochondromatosis was suspected.
The results of our literature review for studies in pediatric patients with initial musculoskeletal (MSK) presentations who were ultimately diagnosed as synovial osteochondromatosis are shown in Table 1 [2, 3, 7, 8, 11,12,13,14,15, 17,18,19,20,21,22,23,24,25,26]. From our review, the plain radiographs were performed in all cases to help in diagnosis. Additional techniques commonly used to provide further details were MRI, followed by computed tomography and ultrasonography. The typical radiographic features of synovial osteochondromatosis include multiple intraarticular loose bodies with a “rings-and-arcs” pattern of cartilage mineralization [27]. In a previous study, radio-opaque bodies were observed in 79% of cases [28]. Differences in imaging findings distinguish synovial osteochondromatosis from other joint diseases. In long-standing JIA, chronic irreversible joint damage, subchondral bone erosion, and narrow joint space due to cartilage destruction can be observed on plain radiography. However, loose bodies are only rarely seen. In patients with a tumor, soft tissue mass that contains calcifications with adjacent bone erosion can be seen [29]. MRI is essentially important for diagnosing synovial osteochondromatosis [2] because it can demonstrate the characteristics of chondroid tissue and evaluate extraarticular structures, such as the tendon sheath and bursa, that can be occasionally found in lesions associated with synovial osteochondromatosis [23].
Secondary synovial osteochondromatosis can be distinguished from primary disease by history of underlying joint abnormality, along with correlations from radiographic and pathologic findings of fewer chondral bodies of variable size and shape, with concentric rings of growth [27, 30]. In primary synovial osteochondromatosis, the pattern of calcification is patchy and diffuse with absence of fragments of articular cartilage, subchondral bone, and fibrin, whereas in secondary disease, there may be presence of these findings and zonal “ring-like” calcification patterns [6]. Our patient’s MRI result showed multiple uniform-sized round and oval lesions within the lateral compartment of the right knee, a small amount of joint effusion with no underlying joint disease, and no history of trauma prior to the onset of illness. Taken together, the findings and features in our patient suggest a diagnosis of primary synovial osteochondromatosis. Three distinct phases of synovial osteochondromatosis have been described. The early phase is characterized by active synovitis without loose bodies, followed by nodular synovitis with loose bodies, and the late phase has loose bodies with resolution of synovitis [31]. Our patient was likely in the second phase with the arthroscopic findings of mild synovitis and multiple loose bodies, and histopathologic results that correlate with the clinical findings.
To date, there are no reports of JIA associated with synovial osteochondromatosis. However, there was one case of a 35-month-old boy diagnosed with oligoarticular JIA that mimicked synovial osteochondromatosis [32]. That patient presented with pain and limping for 3 weeks that was aggravated by running with MSK examination findings of antalgic gait, right knee effusion, limited range of motion, and mobile mass at the superior aspect of the right patella. His MRI revealed joint effusion and tumifactive synovial hypertrophy with hyperplasia mimicking synovial osteochondromatosis; however, arthroscopic findings revealed hypertrophy and inflammation of the synovium without the presence of loose bodies. Histopathology also confirmed hypertrophic and hyperplastic synovium with reactive change without findings of synovial osteochondromatosis. He also had positive ANA and bilateral cataracts with synechiae, which were complications of uveitis [32]. In this boy, the clinical manifestations and correlated radiographic and pathologic findings were compatible with oligoarticular JIA without synovial osteochondromatosis.
The curative treatment for synovial osteochondromatosis involves the removal of loose bodies and synovectomy either by arthroscopy or open arthrotomy [9]. Medical treatment has no definitive role in synovial osteochondromatosis. The recurrence rate was reported to vary from 3 to 23% [33]. Our patient underwent arthroscopic removal of loose bodies and synovectomy with no recurrence of symptoms at the most recent follow-up (6 months).
This case yielded several important key points for physicians who may encounter a patient with synovial osteochondromatosis that have initial presentations which could mimic JIA. First, information from history and physical examination are very helpful for differentiating between inflammatory MSK pain and mechanical MSK pain. A finding of mechanical MSK pain increases the suspicion of synovial osteochondromatosis. Second, plain radiography is essential for evaluating structural abnormalities in patients with joint pain and abnormal MSK examination, and, if indicated, further imaging by MRI will help to diagnose synovial osteochondromatosis. Third, a multidisciplinary approach to patient management will improve diagnosis, treatment, and outcomes for children and adolescents with synovial osteochondromatosis.
Conclusions
Synovial osteochondromatosis is a rare distinctive benign condition that can cause debilitating joint pain mimicking JIA in children and adolescents. Appropriate diagnostic radiography, including both plain radiography and MRI, is necessary to accurately diagnose this condition. We also emphasize the importance of a multidisciplinary team approach to managing patients with synovial osteochondromatosis.
Data availability
All data relevant to the clinical case are included in the article.
Change history
13 June 2022
The Table 1 entries has been aligned correctly.
References
McKenzie G, Raby N, Ritchie D (2008) A pictorial review of primary synovial osteochondromatosis. Eur Radiol 18:2662–2669. https://doi.org/10.1007/s00330-008-1024-8
Giancane G, Tanturri de Horatio L, Buonuomo PS, Barbuti D, Lais G, Cortis E (2013) Swollen knee due to primary synovial chondromatosis in pediatrics: a rare and possibly misdiagnosed condition. Rheumatol Int 33:2183–2185. https://doi.org/10.1007/s00296-012-2382-8
Emad Y, Gheita T, Ragab Y, Zeinhom F (2007) Pauciarticular severe destructive arthropathy in a child secondary to synovial osteochondromatosis. Clin Rheumatol 26:604–606. https://doi.org/10.1007/s10067-005-0183-0
Davis RI, Hamilton A, Biggart JD (1998) Primary synovial chondromatosis: a clinicopathologic review and assessment of malignant potential. Hum Pathol 29:683–688. https://doi.org/10.1016/s0046-8177(98)90276-3
Halstead AE (1895) IV. Floating bodies in joints. Ann Surg 22:327–342. https://doi.org/10.1097/00000658-189507000-00030
Villacin AB, Brigham LN, Bullough PG (1979) Primary and secondary synovial chondrometaplasia: histopathologic and clinicoradiologic differences. Hum Pathol 10:439–451. https://doi.org/10.1016/s0046-8177(79)80050-7
Narasimhan R, Kennedy S, Tewari S, Dhingra D, Zardawi I (2011) Synovial chondromatosis of the elbow in a child. Indian J Orthop 45:181–184. https://doi.org/10.4103/0019-5413.77141
Lohmann CH, Koster G, Klinger HM, Kunze E (2005) Giant synovial osteochondromatosis of the acromio-clavicular joint in a child. A case report and review of the literature. J Pediatr Orthop B 14:126–128. https://doi.org/10.1097/01202412-200503000-00013
Boyer T, Dorfmann H (2008) Arthroscopy in primary synovial chondromatosis of the hip: description and outcome of treatment. J Bone Joint Surg Br 90:314–318. https://doi.org/10.1302/0301-620X.90B3.19664
Carey RP (1983) Synovial chondromatosis of the knee in childhood. A report of two cases. J Bone Joint Surg Br 65:444–447. https://doi.org/10.1302/0301-620X.65B4.6874717
Kistler W (1991) Synovial chondromatosis of the knee joint: a rarity during childhood. Eur J Pediatr Surg 1:237–239. https://doi.org/10.1055/s-2008-1042496
Kukreja S (2013) A case report of synovial chondromatosis of the knee joint arising from the marginal synovium. J Orthop Case Rep 3:7–10
Srinivas KRD, Ramana Y, Kumar PK (2015) Synovial chondromatosis in a young child: a rare presentation. J NTR Univ Health Sci 4:36–38
Pirimoglu B, Koru A, Yalcin A, Polat G, Sade R (2021) An unusual cause of limping in a 2-year-old girl: synovial chondromatosis of the knee. Am J Phys Med Rehabil 100:e37. https://doi.org/10.1097/PHM.0000000000001494
Chou PH, Huang TF, Lin SC, Chen YK, Chen TH (2007) Synovial chondromatosis presented as knocking sensation of the knee in a 14-year-old girl. Arch Orthop Trauma Surg 127:293–297. https://doi.org/10.1007/s00402-006-0144-3
Cho HJ, Suh JD (2018) An unusual presentation of synovial chondromatosis of the knee in a 10-year-old girl. Acta Orthop Traumatol Turc 52:162–165. https://doi.org/10.1016/j.aott.2017.04.008
Pelker RR, Drennan JC, Ozonoff MB (1983) Juvenile synovial chondromatosis of the hip. A case report. J Bone Joint Surg Am 65:552–554
Raza A, Kailash K, Malviya A (2014) (2014) Rare cause of hip pain in a young girl. BMJ Case Rep. https://doi.org/10.1136/bcr-2014-203802
Shapira-Zaltsberg G, Highmore K (2017) Synovial osteochondromatosis in a 14-year-old boy with a history of Legg-Calve-Perthes disease. Radiol Case Rep 12:405–408. https://doi.org/10.1016/j.radcr.2017.01.021
Philip MC, Usman S (2017) Synovial chondromatosis: a rare differential diagnosis of hip pain in a child. J Orthop Case Rep 7:37–39. https://doi.org/10.13107/jocr.2250-0685.740
Wen J, Liu H, Xiao S, Li X, Fang K, Tang Z et al (2018) Synovial chondromatosis of the hip joint in childhood: a case report and literature review. Medicine (Baltimore) 97:e13199. https://doi.org/10.1097/MD.0000000000013199
Forsythe B, Lou J, States L, Guttenberg M, Dormans JP. (2004) Painless ankle mass in a 12-year-old boy. Clin Orthop Relat Res:263–269. https://doi.org/10.1097/01.blo.0000127815.91541.12
Walker EA, Murphey MD, Fetsch JF (2011) Imaging characteristics of tenosynovial and bursal chondromatosis. Skeletal Radiol 40:317–325. https://doi.org/10.1007/s00256-010-1012-3
Kim HK, Zbojniewicz AM, Merrow AC, Cheon JE, Kim IO, Emery KH. (2011) MR findings of synovial disease in children and young adults: part 1. Pediatr Radiol 41:495–511; quiz 545–496. https://doi.org/10.1007/s00247-011-1971-0
Sathe P, Agnihotri M, Vinchu C (2020) Synovial chondromatosis of ankle in a child: a rare presentation. J Postgrad Med 66:112–113. https://doi.org/10.4103/jpgm.JPGM_628_19
Botaya EGALP, Menchón M, Muñoza AS, Moscardó-Navarro A, Rey M (2020) Synovial chondromatosis of the knee. A rare cause of knee pain in pediatric age. Arch Argent Pediatr 118:e34–e38
Murphey MD, Vidal JA, Fanburg-Smith JC, Gajewski DA (2007) Imaging of synovial chondromatosis with radiologic-pathologic correlation. Radiographics 27:1465–1488. https://doi.org/10.1148/rg.275075116
Maurice H, Crone M, Watt I (1988) Synovial chondromatosis. J Bone Joint Surg Br 70:807–811. https://doi.org/10.1302/0301-620X.70B5.3192585
Turan A, Celtikci P, Tufan A, Ozturk MA (2017) Basic radiological assessment of synovial diseases: a pictorial essay. Eur J Rheumatol 4:166–174. https://doi.org/10.5152/eurjrheum.2015.0032
Utashima D, Matsumura N, Suzuki T, Iwamoto T, Ogawa K (2020) Clinical results of surgical resection and histopathological evaluation of synovial chondromatosis in the shoulder: a retrospective study and literature review. Clin Orthop Surg 12:68–75. https://doi.org/10.4055/cios.2020.12.1.68
Milgram JW (1977) Synovial osteochondromatosis: a histopathological study of thirty cases. J Bone Joint Surg Am 59:792–801
Rousslang LK, Rooks E, Hixson C, West P (2020) Tumefactive synovial thickening mimicking synovial chondromatosis in the setting of oligoarticular juvenile idiopathic arthritis in a toddler. Radiol Case Rep 15:218–221. https://doi.org/10.1016/j.radcr.2019.11.016
Sedeek SM, Choudry Q, Garg S (2015) Synovial chondromatosis of the ankle joint: clinical, radiological, and intraoperative findings. Case Rep Orthop 2015:359024. https://doi.org/10.1155/2015/359024
Acknowledgements
The authors gratefully acknowledge the patient profiled in this study and her parents for granting us permission to report details and images relating to her case. The authors also gratefully acknowledge Mr. Kevin Jones, medical research manuscript editor, Siriraj Medical Research Center (SiMR) Faculty of Medicine Siriraj Hospital, Mahidol University, for the professional English language editing of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
Not applicable; ethical approval not required.
Patient consent for publication
Verbal assent was obtained from the patient, and written informed consent was obtained from the patient’s parents granting permission that details and images relating to the patient’s case can be submitted for journal publication.
Disclosures
None.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yothakol, N., Charuvanij, S., Siriwanarangsun, P. et al. Synovial osteochondromatosis mimicking juvenile idiopathic arthritis in an adolescent: a case-based review. Clin Rheumatol 41, 2571–2580 (2022). https://doi.org/10.1007/s10067-022-06224-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-022-06224-w