
Abstract
Introduction
Dose escalation of infliximab in both primary and secondary nonresponders is widely reported; however, the usefulness of dose escalation has been disputed. The objective of this analysis is to evaluate trends in clinical efficacy following multiple infliximab dose escalations in patients with rheumatoid arthritis (RA).
Methods
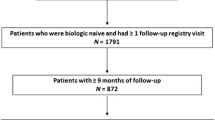
Patients enrolled in a US RA registry were included if they initiated infliximab at 3 mg/kg every 8 weeks, received ≥ 1 infliximab dose escalation within 12 months of initiation, and had ≥ 1 visit following dose escalation. Trends in mean Clinical Disease Activity Index (CDAI) and Health Assessment Questionnaire (HAQ) scores from visits following dose escalations were evaluated.
Results
In patients who received 2 or 3 dose escalations, the initial (1 or 2) dose escalations resulted in reduced mean CDAI scores, but subsequent escalations did not further reduce disease activity. In patients who received ≥ 4 dose escalations, mean CDAI scores did not further reduce disease activity over time. Mean HAQ scores were stable over time in patients who received 2 or 3 dose escalations. In patients who received ≥ 4 dose escalations, mean HAQ scores decreased following 1 dose escalation but progressively increased following subsequent dose escalations.
Conclusion
Initial dose escalations (from 3 mg/kg to the equivalent of approximately 5 to 7 mg/kg) may be useful in controlling disease activity; however, there may be diminishing clinical benefit of further escalations, which can also increase the potential risk for infection and increase incremental drug costs.
Key Points
• Initial infliximab dose escalations (1 to 2) may be useful in lowering disease activity in patients with rheumatoid arthritis.
• There does not appear to be a clinical benefit in infliximab dose escalations above the equivalent of 5 to 7 mg/kg.




Similar content being viewed by others

References
Singh JA, Saag KG, Bridges SL Jr, Akl EA, Bannuru RR, Sullivan MC, Vaysbrot E, McNaughton C, Osani M, Shmerling RH, Curtis JR, Furst DE, Parks D, Kavanaugh A, O'Dell J, King C, Leong A, Matteson EL, Schousboe JT, Drevlow B, Ginsberg S, Grober J, St.Clair EW, Tindall E, Miller AS, McAlindon T (2016) 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol 68:1–26
Smolen JS, Landewé R, Bijlsma J, Burmester G, Chatzidionysiou K, Dougados M, Nam J, Ramiro S, Voshaar M, van Vollenhoven R, Aletaha D, Aringer M, Boers M, Buckley CD, Buttgereit F, Bykerk V, Cardiel M, Combe B, Cutolo M, van Eijk-Hustings Y, Emery P, Finckh A, Gabay C, Gomez-Reino J, Gossec L, Gottenberg JE, Hazes JMW, Huizinga T, Jani M, Karateev D, Kouloumas M, Kvien T, Li Z, Mariette X, McInnes I, Mysler E, Nash P, Pavelka K, Poór G, Richez C, van Riel P, Rubbert-Roth A, Saag K, da Silva J, Stamm T, Takeuchi T, Westhovens R, de Wit M, van der Heijde D (2017) EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis 76:960–977
Cannon GW, DuVall SL, Haroldsen CL et al (2014) Persistence and dose escalation of tumor necrosis factor inhibitors in US veterans with rheumatoid arthritis. J Rheumatol 41:1935–1943
Infliximab package insert (2013) Janssen Biotech, Inc., Horsham. In: PA
Plasencia C, Jurado T, Villalba A et al (2015) Effect of infliximab dose increase in rheumatoid arthritis at different trough concentrations: a cohort study in clinical practice conditions. Front Med (Lausanne) 2:71
Furst DE, Keystone EC, Braun J et al (2011) Updated consensus statement on biological agents for the treatment of rheumatic diseases, 2010. Ann Rheum Dis 70(Suppl 1):i12–i36
Stern R, Wolfe F (2004) Infliximab dose and clinical status: results of 2 studies in 1642 patients with rheumatoid arthritis. J Rheumatol 31:1538–1545
Ellis L, Le C, McDermott JD, Daniel SR (2017) Real-world, multi-site, observational study of infusion time and treatment satisfaction in rheumatoid arthritis patients treated with intravenous golimumab or infliximab [poster PM548]. Poster presented at: 22nd Annual International Meeting of the International Society for Pharmacoeconomics and Outcomes Research; May 20–24, 2017; Boston, MA
Moots RJ, Mays R, Stephens J, Tarallo M (2015) Burden of dose escalation with tumour necrosis factor inhibitors in rheumatoid arthritis: a systematic review of frequency and costs. Clin Exp Rheumatol 33:737–745
Fisher MD, Watson C, Fox KM, Chen YW, Gandra SR (2013) Dosing patterns of three tumor necrosis factor blockers among patients with rheumatoid arthritis in a large United States managed care population. Curr Med Res Opin 29:561–568
Schabert VF, Bruce B, Ferrufino CF, Globe DR, Harrison DJ, Lingala B, Fries JF (2012) Disability outcomes and dose escalation with etanercept, adalimumab, and infliximab in rheumatoid arthritis patients: a US-based retrospective comparative effectiveness study. Curr Med Res Opin 28:569–580
Pavelka K, Jarosová K, Suchý D et al (2009) Increasing the infliximab dose in rheumatoid arthritis patients: a randomised, double blind study failed to confirm its efficacy. Ann Rheum Dis 68:1285–1289
Rahman MU, Strusberg I, Geusens P, Berman A, Yocum D, Baker D, Wagner C, Han J, Westhovens R (2007) Double-blinded infliximab dose escalation in patients with rheumatoid arthritis. Ann Rheum Dis 66:1233–1238
Eng G, Stoltenberg MB, Szkudlarek M, Bouchelouche PN, Christensen R, Bliddal H, Marie Bartels E (2013) Efficacy of treatment intensification with adalimumab, etanercept and infliximab in rheumatoid arthritis: a systematic review of cohort studies with focus on dose. Semin Arthritis Rheum 43:144–151
Joyce AT, Gandra SR, Fox KM, Smith TW, Pill MW (2014) National and regional dose escalation and cost of tumor necrosis factor blocker therapy in biologic-naïve rheumatoid arthritis patients in US health plans. J Med Econ 17:1–10
Aletaha D, Smolen J (2005) The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): a review of their usefulness and validity in rheumatoid arthritis. Clin Exp Rheumatol 23(Suppl 39):S100–S108
Anderson J, Caplan L, Yazdany J, Robbins ML, Neogi T, Michaud K, Saag KG, O'dell JR, Kazi S (2012) Rheumatoid arthritis disease activity measures: American College of Rheumatology recommendations for use in clinical practice. Arthritis Care Res 64:640–647
Fries JF, Spitz P, Kraines G, Holman H (1980) Measurement of patient outcome in arthritis. Arthritis Rheum 23:137–145
Cleveland WS (1993) Bivariate data. In: Cleveland WS (ed) Visualizing data. Hobart Press, New Jersey, pp 90–101
Newson R (2000) sg151: B–splines and splines parameterized by their values at reference points on the x–axis. Stata Tech Bull 57:20–27, Reprinted in Stata Tech Bull Reprints 10:221–230
Takeuchi T, Miyasaka N, Tatsuki Y, Yano T, Yoshinari T, Abe T, Koike T (2011) Baseline tumour necrosis factor alpha levels predict the necessity for dose escalation of infliximab therapy in patients with rheumatoid arthritis. Ann Rheum Dis 70:1208–1215
Dervieux T, Weinblatt ME, Kivitz A, Kremer JM (2013) Methotrexate polyglutamation in relation to infliximab pharmacokinetics in rheumatoid arthritis. Ann Rheum Dis 72:908–910
Acknowledgments
Writing support was provided by Holly Capasso-Harris, PhD, of Synchrogenix, a Certara Company, Wilmington, DE. This study was sponsored by Corrona, LLC, and the analysis and medical writing support were funded by Janssen Scientific Affairs, LLC, Spring House, PA. Corrona, LLC, Waltham, MA, has been supported through contracted subscriptions in the last 2 years by AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Crescendo, Eli Lilly and Company, Genentech, Gilead, GlaxoSmithKline, Horizon Pharma USA, Janssen, Momenta Pharmaceuticals, Novartis, Pfizer Inc., Roche, Sun-Merck, UCB, and Valeant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed consent
All study participants provided written informed consent. Institutional Review Board (IRB) approvals for this study were obtained from a central IRB (New England IRB, Needham, Massachusetts, USA; IRB registration number 120160610) for private practice sites and local IRBs of participating academic sites.
Conflict of interest
Dr. Cohen has served as an investigator and consultant for Amgen, AbbVie, Janssen, Genentech, Pfizer, Merck, Bristol-Myers Squibb, and Roche (less than $10,000 each). Dr. Kremer is employed by and has equity interest in Corrona, LLC, and has served as a consultant for AbbVie, Amgen, Bristol-Myers Squibb, Gilead, GSK, Eli Lilly and Company, Genentech, Medimmune, Sanofi, and Pfizer Inc. (less than $10,000 each) and an investigator for AbbVie, Genentech, Eli Lilly and Company, Novartis, and Pfizer Inc. (less than $10,000 each). Ms. Dandreo is employed by Corrona, LLC. Dr. Reed is employed by and has stock ownership in Corrona, LLC. Mr. Magner is employed by Corrona, LLC. Dr. Shan is employed by Corrona, LLC. Dr. Kafka is employed by and has stock ownership in Johnson and Johnson. Dr. DeHoratius was employed by (at the time the work was conducted) and has stock ownership in Johnson and Johnson. Dr. Ellis is employed by and has stock ownership in Johnson and Johnson. Dr. Parenti was employed by (at the time the work was conducted) and has stock ownership in Johnson and Johnson.
The authors have full control of all primary data. Corrona dataset is based on a large US multicenter study adhering to a number of institutional review boards, with complex logistics. Patients did not provide consent to raw data sharing during the data collection for this purpose, and the Corrona data sharing policies do not permit raw data sharing for this purpose. An aggregated limited dataset from the current analyses is available to qualified investigators with an approved protocol. Data requests may be sent to Corrona, represented by Dr. Leslie Harrold, email lharrold@corrona.org.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Cohen, S.B., Kremer, J.M., Dandreo, K.J. et al. Outcomes of infliximab dose escalation in patients with rheumatoid arthritis. Clin Rheumatol 38, 2501–2508 (2019). https://doi.org/10.1007/s10067-019-04543-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-019-04543-z