
Abstract
Balance problems are widely reported in Pediatric Brain Tumor Survivors (PBTS) due to tumor localization and the side effects of medical treatment. This study investigates the effects of conventional versus video-based games exercise training (exergaming) on balance in PBTS. The present study was a randomized controlled trial. The study included 23 PBTS who were randomized to a Video-Based balance exergaming Group (VBG) or Conventional balance exercise training Group (CG). In both groups, the interventions were targeted to the balance function and balance exercise training was administered twice a week for 8 weeks. VBG exercised using selected Nintendo Wii Fit Plus® balance games while CG received a specially designed balance training using conventional physiotherapy methods. The primary outcome was the balance tests (Timed Up and Go and Nintendo® Wii™ Center of Gravity: COG), and the secondary outcomes were the functional tests (10-m walking, 2-min walking, 5-step climb/descent/times), and disease effect test (PedsQL Brain Tumor Module). The outcomes were assessed before and after the intervention. At baseline, no significant clinical and outcome assessment differences existed between both groups except for COG (p = 0.0495). After training, overall scores for balance, functional, disease effect tests significantly improved in VBG (p < 0.05) while progress observed in CG was not significant (p > 0.05). Video-based balance exergaming was found effective and more so than conventional balance exercise training in PBTS. Greater effectiveness of exergaming is thought to be due to increased motivation and effort of the children who are more attracted to gaming than conventional exercising. Exergaming could be beneficial both in clinical and home settings with physiotherapist supervision and may reduce the costs of treatment while improving their health-related quality of life.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Brain tumors are the most frequent types of solid tumors after leukemia in childhood (Sklar 2002). The disease has many adverse physical, functional, and psycho-social effects (Pollack 1994). The prognosis for brain tumors has improved over the last decades and now exceeds a 5-year survival rate of 83% (Miller et al. 2019). While medical interventions increase survival, they give rise to short and long-term side effects such as pain, reduced physical fitness, fatigue, lower quality of life and balance impairment (Tanriverdi and Cakir 2023). Balance problems specifically occur due to involvement of cerebellum such as in medulloblastoma (Varedi et al. 2021). Besides, muscle weakness, decreased exercise capacity and muscular fatigue may also lead to balance problems (O’Reilly et al. 2013). Balance impairments cause lack of mobility and restriction of daily living activities which significantly reduce the health-related quality of life (HRQoL) (Sato et al. 2014).
While exercise was previously considered a risk factor during the treatment process of the disease, recently it was found that it has beneficial effects and improves HRQoL in children with cancer (Wrisley and Pavlou 2005; Bryanton et al. 2006; Ospina et al. 2021; Riggs et al. 2017). Although exercise programs are recommended for these children, there is no approved exercise guidelines for pediatrics (DeSantis et al. 2014; Runco et al. 2019). There is limited data concerning motor performance and HRQoL, and indeed, no study specific to balance in children with cancer has been reported yet (Hansen et al. 2018; Sparrow et al. 2017). Balance exercise training with conventional means and/or technology supported such as video-based balance exergaming has been applied specially in children with cerebral palsy (Bryanton et al. 2006). Thus, exergaming appears a promising alternative rehabilitation method to improve balance and motor functions which are seriously affected in pediatric brain tumor survivors (PBTS). Although exergaming for pediatric cancers has been popular in recent years, and was found to increase motivation and participation, no definite superiority to conventional exercise programs is established (Braam et al. 2016; Montoro‐Cárdenas et al. 2021).
The purpose of the present study, which is the first such investigation in the literature, is to examine the effects of balance training on PBTS and further, to compare the effectiveness of conventional training methods with video-based exergaming approach.
2 Methods
2.1 Study design and randomization
The present study was a prospective, randomized controlled trial performed at our university hospital rehabilitation unit, in İstanbul, Türkiye. We used the minimisation method to randomize between the VBG group or the CG group, balancing the groups for: sex, age at randomisation. All participants were evaluated at two time points: at the study start, and at the end of study. The evaluations included tests of physical functioning, see below in outcome measures. Other possible treatments (e.g. physiotherapy or occupational therapy) could continue as before, during both the study period, although compliance to this was not registered. Before and after the intervention period parents and children were interviewed about the children’s leisure time activities, especially the amount of regular physical exercise. Eligible participants were randomly assigned to a Video-Based balance exergaming Group (VBG) or Conventional balance exercise training Group (CG) using a sealed envelope method, in which the closed envelopes inclosing participant names were shuffled and selected blindly from an opaque bag by a different person who were not involved in the intervention (Kim and Shin 2014). This study was registered at clinicaltrials.gov (NCTXXXX) and was approved by the ethics committee of our university (Protocol ID: 10840098-604.01.01-E.8320). The study was conducted in accordance with the Helsinki Declaration. A written informed consent was obtained from the parents of each child before enrollment.
2.2 Participants
The study included 23 consecutive participants with balance problems caused by brain tumor, who were present in our university hospital rehabilitation unit. The inclusion criteria were as follows: (1) aged between 6 and 15 years; (2) at a similar clinical stage of the disease (high-risk: according to the pathological evaluation by the pediatric oncologist); (3) receiving alike medical treatment; and (4) receiving participation acceptance. The exclusion criteria were as follows: (1) age < 6 and > 15 years; (2) hospitalization history in past month; (3) active participation in another supervised physiotherapy rehabilitation program; (4) diagnosed comorbidities which may affect balance; and (5) having cognitive or behavioral problems.
2.3 Intervention
All participants received an 8-week face-to-face intervention program (VBG or CG) individually (16 sessions for 45 min per day) in a room for the intervention. The intervention programs exclusively focused on the balance function and were administered by the same physiotherapist who was involved in both the interventions and was exclusively dedicated to this study. The intervention time was the same in both the groups.
2.3.1 Video-based balance exergaming intervention
The intervention program was administered during eight weeks for a total of 16 sessions held two days per week. It has been recommended that the selection of games should be specifically targeted towards well-defined rehabilitation goals which, in our study, is to primarily improve balance (Deutsch et al. 2011). Thus, five different games were selected from the available Nintendo® Wii™ catalog with an objective to maximally improve the ability to weight bearing in all directions and to change the position of the trunk in standing and squatting positions. In this respect, the selected Nintendo® Wii™ balance games were (1) Game-1. “Heading/Soccer”: Standing on Wee-fit™ board, laterally weight shift left/right to hit projected soccer balls with the head. High scores indicate better performance; (2) Game-2. “Ski jump”: Standing on Wee-fit™ board, flex at hips and knees to propel down a ski jump by maintaining a mini squat until the target red zone at the end of the ramp is reached. High scores indicate better performance; (3) Game-3. “Penguin slide”: Standing on Wee-fit™ board, tilt a projected iceberg from side to side with a quick series of medial/lateral weight shifts. High scores indicate better performance; (4) Game-4. “Ski slalom”: Standing on Wee-fit™ board, weight shift in all planes to ski between 19 marked gates. Completion shorter time points to better performance; (5) Game-5. “Balance bubbles”: Standing on Wee-fit™ board, navigate down a river in a bubble containing the virtual body via weight shift in all (anterior/posterior/lateral) planes. High scores indicate better performance. These 5-game showed at Fig. 1.

Nintendo® Wii™ balance games
2.3.2 Conventional balance exercise training intervention
A special program using conventional rehabilitation methods was specifically designed for PBTS to improve balance. It principally included balance exercises involving weight bearing in standing position. Accordingly, the progressive balance exercises performed (with equivalent exercises executed by VBG while exergaming indicated by “G: game numbers”) in our study were (1) Trunk rotation: Rotations made with rotational movements of the trunk. (G:1,3,4,5); (2) Reach of front/ back/ lateral: Reaching exercises performed in different positions. (G:1,4); (3) Weight bearing: Weight is transferred to all directions using the whole body. (G:1,2,3,4,5); (4) Step: Front-back-side-step exercises. (G:2,4); (5) One-leg stand: One-leg stand exercises on the right / left feet, separately. (G:4); (6) Functional exercises: Exercise ball and mini trampoline using exercises. (G:1,2,3,4,5).
2.4 Outcome measures
The baseline characteristics assessed were age, age of diagnosis, sex, height, weight, body mass index, tumor type, chemotherapy cycle number and radiation session number.
2.4.1 Primary outcomes
Balance impairments of PBTS was evaluated using the Nintendo® (Kyoto, Japan) Wii™ Fit Plus Console Balance tests and Timed Up and Go (TUG) Test. In the literature, Nintendo® Wii™ balance scores have been validated (Wikstrom 2012). The Nintendo® Wii™ interactive game videos were shown via a 132 cm television unit. The Nintendo® Wii™ tests selected for assessment were center of gravity (COG) and selected Nintendo® Wii™ balance game scores. Center of Gravity (COG): The child was asked to step and place his/her feet the Nintendo® Wii™ Fit Plus balance board. The weight ratio on the right and left feet was recorded as percentage in the balance board without moving. In healthy children the percent of COG is expected 50%-50% (Right-Left %) and the differences between the sides should be near zero when he/she is stable. The measurement was repeated three times and the average value recorded for analysis. Objective evaluation of balance is very important for demonstrating the effectiveness of the treatment. COG assessment can be considered a reliable indicator of the effects of balance and the Nintendo® Wii™ board system, via a four-point differential weighting technique per each leg, provides an objective measurement of COG imbalance (Deutsch et al. 2011; Wikstrom 2012). Nintendo© Wii™ Balance Game Scores: Participation and the game scores were recorded in each session for every participant who played all five selected Nintendo® Wii™ games in succession and in the same order (Game-1 to Game-5) with no repetitions. Maximal scores for each participant in each game during training were also recorded. Timed Up and Go Test (TUG): This test assesses the balance performance of children during mobility. It is a reliable and valid method for evaluating dynamic balance. It uses the time that a child takes to rise from a chair, walk three meters, turn around, walk back to the chair, and sit down. The time elapsed was recorded in seconds using a stopwatch (Wall et al. 2000).
2.4.2 Secondary outcomes
Functional tests (10-Meter Walking (10 MW) Test, 2-Minute Walking (2 MW) Test, 5-Step Climb & Descent Times Test) and disease effect test (PedsQL Brain Tumor Module) were the secondary outcome measurements.
10-Meter Walking (10 MW) Test is a performance measure used to assess short distance walking speed. Walking time was measured with a stopwatch. The test was repeated twice, and the mean score was recorded in seconds (de Baptista et al. 2020). 2-Minute Walking (2 MW) Test, being a relatively long-distance walking test, it was used to evaluate functional exercise capacity. Children were instructed to walk for two minutes in a 30 m unobstructed and well-lit corridor. The walking distance was measured after a two-minute walking period (Brooks et al. 2001). 5-Step Climb & Descent Times Test assesses functional mobility. All children were asked to climb and descent 5 steps (14 × 28 × 120 cm) as fast as possible supervised by the physiotherapist imposing strict security precautions. The climb, descent and total durations were recorded with a stopwatch. The test was repeated three times and the mean scores were calculated in seconds (Zaino et al. 2004).
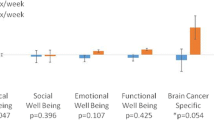
PedsQL Brain Tumor Module (BTM) test was used to measure brain tumor specific health-related quality of life. The test is composed of 23 items comprising 6 dimensions; cognitive problems (6 items), pain and hurt (3 items), movement and balance (3 items), procedural anxiety (3 items), nausea (5 items) and worry (3 items). The test scoring uses a five-level Likert scale from 0 (Never a problem) to 4 (Almost always a problem). Items were reverse scored and linearly transformed to a 0–100 scale as follows: 0 = 100, 1 = 75, 2 = 50, 3 = 25, 4 = 0. Higher scores indicate lower problems (Palmer et al. 2007).
2.5 Statistical analysis
All statistical analysis was conducted using “Statistical Package for Social Sciences (SPSS)” Version 27.0 (SPSS Inc. Chicago. IL. USA). Normality of the distribution of data was checked with the Kolmogorov–Smirnov test. Parametric variables were expressed as mean ± standard deviation (SD) and their in-group and inter-group assessment results were analyzed respectively with Paired Sample and Independent Samples Student’s t-tests. Inter-group comparisons of categorical variables were made using χ2-test. Differences were considered significant when p values < 0.05. Treatment effectiveness was quantified with Cohen’s-d effect-size statistic of post-treatment variations; effect sizes were considered as small (> 0.20), moderate (0.50–0.80) or large (≥ 0.80) effect (Cohen 1992). Possible dependencies between outcome measures were investigated by computing Spearmen’s linear correlation coefficient “r”. Detected correlations were deemed as “strong” if r ≥ 0.70, “moderate” if 0.30 ≤ r < 0.70, and “weak” if r < 0.30. Correlation confidence levels were determined with one-tailed Student's t-test of the r2 value.
2.5.1 Sample size
Nintendo® Wii™ Fit Plus COG score, being a purely static balance assessment, was chosen for power analysis to determine required minimal sizes of our study groups. Based on a pilot study, (N = 5, 3 boys, Age: 10.4 ± 3.5 [min–max = 7–14] years, COG = 18.1 ± 16.6) the minimal sample size was estimated to be N ≥ 7 participants for each group using G*Power software (Mean difference between two independent groups: A-priori sample size—given alpha, power and effect size) to obtain a power of 0.80 (β = 0.20) with α = 0.05 (p < 0.05) with an effect size of 0.85 (Faul et al. 2009; Tanriverdi et al. 2023).
3 Results
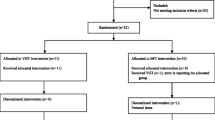
Of the 30 participants included in the present study, 23 completed the 8-week intervention programs and assessments. During the study, 2 and 5 participants from the VBG and CG groups, respectively, did not complete the intervention programs. The sample sizes at the assessment time points are presented in Fig. 2. Eleven participants declined to participate due to not to have time and transfer problems. The statistical analysis of recorded data was performed after the completion final post-training assessment. The intervention program completion rates 87% (13/15) for VBG and 67% (10/15) for CG with no significant difference (χ2-test, p > 0.20) between drop out rates. No adverse effects were reported during the program. There was no difference (p > 0.83) between groups in time spent during sessions; 37.6 ± 4.8 min/session in VBG, and 36.8 ± 2.4 min/session in CG. The demographic/clinical characteristics of the patients completing the training program for both groups are presented in Table 1. No statistically significant differences in these characteristics were detected between groups.

Flow diagram (consort chart) of the study
Baseline and post-treatment assessment statistics for balance, functional, and disease effect tests are tabulated in Table 2 which also summarizes the statistical analysis of the treatment’s effects observed. No sex-related statistically significant differences were found in all assessments. Baseline measurement of all participants (n = 23) for COG imbalance percentage was 13.3 ± 10.4% which is significantly (p < 0.001) different from perfect balance (50–50, i.e., 0%) value. PedsQL BTM baseline assessment of our participants yielded 71 ± 15 points which indicates a significantly (p < 0.001) lower quality of life than their healthy peers (83 ± 13) (Varni et al. 2003). There were no significant differences (p < 0.05) between groups at baseline values of all scores except for COG assessments (p > 0.05).
After training, all assessment scores progressed significantly in VBG while the scores for CG improvements were non-significant (p = 0.075) for COG, (p = 0.064) for TUG and (p = 0.061) for PedsQL BTM. All observed improvements in VBG have been found significantly better than those in CG (all p < 0.05) except marginally so for COG (p = 0.075.) VBG progress can be considered strong (Cohen’s-d ≥ 0.8) for COG, 10 m and 2 min walking tests and medium (Cohen’s-d ≥ 0.5) for the remaining outcome assessments.
The results of Nintendo® Wii™ average game scores and participation statistics of VBG are given in Table 3. Adherence to the training program was 82% in VBG and 87% in CG for patients completing the study. The reasons for missing one or more sessions included patient's refusal, family commitments and school exams. There were significant and immediately noticeable improvements in all games (p < 0.001) after VBG training. The mean scores for each game and overall game performance improvement trend are shown in Fig. 3 which also shows participation data to sessions and to games in each session. Overall game performance progression can be observed in Fig. 3 to consistently increase with the number of sessions played with a visible leveling off the game scores for the last sessions attended.

Video-based exergaming group (VBG) Game attendance, participation and relative performance improvement to baseline scores (X) progression
The game scores of the participants were not directly correlated with functional testing improvements. However, the computed “diligence”, which we defined as the product of average game score improvement ratio with the number of sessions attended for each participant, was found moderately correlated with 10 m walking time (r = − 0.48 p < 0.05), TUG (r = − 0.53 p < 0.05), PedsQL BTM (r = − 0.51 p < 0.05) and 5-step total climb and descent time (r = − 0.56 p < 0.05).
4 Discussion
This study investigated the effects of two different face-to-face physiotherapists who graduated from the equal education level, administered balance training approaches for off-treatment PBTS. Post-training evaluations indicated statistically significant improvements on balance and functional activities for VBG while conventional training was found largely ineffective except for a probable progress trend in COG, TUG and PedsQL BTM assessments. The present work is the first clinical trial investigating the effect of both conventional and video-based balance exercise trainings aiming to improve balance and functional activities of PBTS. Moreover, it is also the first to compare the efficiency of these two radically different approaches.
Video-based exercises were recently tried and gave promising results in the treatment and rehabilitation of children (Tatla et al. 2014; Sabel et al. 2016; Conklin et al. 2019). Exergaming systems support children with facilitative adaptation to the rehabilitation program in many ways. In particular, motivation, which increases compliance, is very desirable in pediatric rehabilitation (Wrisley and Pavlou 2005; Bryanton et al. 2006). Several studies with the Nintendo® Wii™ game console and similar computerized systems to improve balance in children for different diseases have been reported (Cox et al. 2020; Meyns et al. 2017; Gouveia E Silva et al. 2020; Putnam et al. 2014; Clark et al. 2010; Meldrum et al. 2012; Wang and Reid 2011; Tanriverdi et al. 2022; Gokeler et al. 2016). Two such studies, methodologically like ours, Meyns et al. and Gouveia et al. compared two different types (Video-based vs conventional) of exercise interventions on balance problems in children with cerebral palsy and post-polio syndrome; they found significant and similar achievements in both groups (Meyns et al. 2017; Gouveia et al. 2020). Therapists with experiences from Nintendo Wii games on children with brain injuries reported the most common therapeutic achievements were seen in balance and weight shifting (Putnam et al. 2014). This achievement is particularly related to changing and stabilizing the COG values in the lateral and anteroposterior directions, and thus improving postural control (Meyns et al. 2017; Putnam et al. 2014). These observations motivated the selection of balance-oriented exercise games of Nintendo Wii console software inventory in our study. Physiotherapists reported that the program with technological support were easily applicable, adaptable, and habilitative with full of fun to the exercise program. In considering therapy-centered game design besides the needs of patients, the games effects should be considered by the physiotherapists. The necessary and beneficial games for the patients should be addressed after their neurological examination (such as diminished visual or auditory sensation, having epilepsy) and physiotherapy evaluation before the exercise program. Spectrum of games can be changed according to the perspective of their physiotherapist. Some of physiotherapists only concentrate on the defective function of the patients. On the other hand, some of them benefit games which the patients can already have done the function with their abilities (Putnam et al. 2014).
Our baseline COG assessment results confirm that the balance is significantly impaired in PBTS (imbalance ~ 13%, p ≈ 0 for all our participants). Although the improvement in COG in our study was remarkable for VBG and perceptible for CG participants, normal limits (right 50%, left 50%) were not achieved for both groups; some statistically significant imbalance (7.4% for VBG and 4.9% for CG) still remained after training (p ≈ 0). Therefore, we think these children should be directed to long-term physiotherapy balance rehabilitation programs preferably using the exergaming approach that we found more effective. However, the duration and type of pediatric rehabilitation programs lack established guidelines (Wang and Reid 2011). There is no study evaluating the balance function in PBTS with video-based exergaming except Sabel et al. where they found that body coordination score statistically improved by 15% over the intervention period (Sabel et al. 2016).
Significant improvements in all functional tests assessed in this study supported our hypothesis that the balance training is effective on functionality although these were statistically significant only in VBG. We suspect this difference in the effectiveness of treatment is due to much better COG improvement observed in VBG as well as to higher dynamical coordination exercise content of the exergaming method. However, one must note participants in CG had better baseline COG scores with less margin for progress. The range of functional test assessments improvements varied between 16 and 22% after training in VBG which is close to what is reported for body coordination improvement previously reported (Sabel et al. 2016).
Past studies reported PBTS frequently having cognitive problems, inferior physical functioning and being less physically active compared to their healthy peers (Conklin et al. 2019; Cox et al. 2020). All these factors naturally negatively affect their HRQoL which is confirmed by our baseline assessment of PedsQL BTM scores of our participants. After training, these scores progressed and significantly so in VBG indicating the positive impact of balance training on the HRQoL of PBTS. Although we strongly emphasized and evaluated balance training in our study, anecdotal evidence received from the parents of our exergaming participants point to some improvement of their cognitive functions correlated with better school performance.
The examination in Table 3 and Fig. 3 of the game participation and scoring results of our VBG children leads to the following observations: attendance to sessions (85%) was high despite ongoing social and medical constraints. Individual interest to games in each session was lively (96%) with very few games disfavored by the children; four children (all boys) even voluntarily continued exergaming after their post-treatment evaluation. The participation of the physiotherapist to the sessions was welcomed by the children and accelerated their adaptation to the games. We think our choice of games came close to achieve a critical balance between therapeutic efficiency and sustained motivation. All game scores were boosted with repeated gaming in successive sessions although, due to the game scoring differences, not all game scores increased at the same rate. Leveling off the game scores naturally happened (“saturation effect” which is common to all repeated game playing) but was noticeable only during the last sessions (Deutsch et al. 2011). The maximal group average scores for all games were obtained near the end of the treatment period which leads us to conclude our choice of total exergaming prescription dosage was adequate. The efficiency of exergaming depends on individual interest and exercising effort. The moderate correlations we found between our “diligence” scores with functional assessment improvements may justify the efforts we undertook to strengthen motivation and participation.
4.1 Limitations and future work
The present study had several limitations. The primary outcome of our study was to detect COG values at baseline it is demonstrated that COG scores significantly differed surprisingly. However, as the study was a randomized one, we couldn’t suspect this difference. The absence of a control group which consist of healthy children, and the lack of long-term follow-up exercise training results are seen as the main limitations of this study. We could not conduct post-study follow up assessments due to medical and social constraints of the children. Video-based exergaming is considered as having fun by the PBTS but not considered as physiotherapy exercise. Thus, this way of thinking of the PBTS increases the applicability, attendance to the exercises and reduce the participation restrictions. By organizing several video-based exercises on defective functioning of PBTS, more evidence-based data can be gained in future studies. For example, besides the achievement of target effect of the video-based exercises, beneficial outcomes of other functional abilities can be contributed. There is limited data on video-based exercises to standardize these games in terms of functional achievement of PBTS.
5 Conclusions
We confirmed balance was significantly impaired in PBTS. We found video-based balance exergaming, supported by a physiotherapist, was a feasible, enjoyable, and safe form of exercise that improved balance and functionality and is more effective than conventional physiotherapy-based balance training for this purpose. Video-based balance exergaming should therefore be encouraged in PBTS. A long-term program should be scheduled and standardized in PBTS. Nintendo® Wii™ Fit Plus is no longer manufactured but similar exergaming systems exist and may be recommended for such patients for practice at home with periodic physiotherapist supervision to reduce cost of treatment and increase motivation (Bruggers et al. 2018; Zoccolillo et al. 2015). This way of home exercise could be suggested as a model of exercise program in the long run follow up of PBTS. Trans and multidisciplinary teams as a model are suggested to work with each other into clinical care.
Data availability
Data will be made available on reasonable request.
References
Braam KI, van der Torre P, Takken T et al (2016) Physical exercise training interventions for children and young adults during and after treatment for childhood cancer. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD008796.pub3
Brooks D, Parsons J, Hunter JP et al (2001) The 2-minute walk test as a measure of functional improvement in persons with lower limb amputation. Arch Phys Med Rehab 82:1478–1483. https://doi.org/10.1053/apmr.2001.25153
Bruggers CS, Baranowski S, Beseris M et al (2018) A Prototype exercise-empowerment mobile video game for children with cancer, and its usability assessment: developing digital empowerment interventions for pediatric diseases. Front Pediatr 6:69. https://doi.org/10.3389/fped.2018.00069
Bryanton C, Bosse J, Brien M et al (2006) Feasibility, motivation, and selective motor control: virtual reality compared to conventional home exercise in children with cerebral palsy. Cyberpsychol Behav 9:123–128. https://doi.org/10.1089/cpb.2006.9.123
Clark RA, Bryant AL, Pua Y et al (2010) Validity and reliability of the Nintendo Wii balance board for assessment of standing balance. Gait Posture 31:307–310. https://doi.org/10.1016/j.gaitpost.2009.11.012
Cohen J (1992) Statistical power analysis. Curr Dir Psychol Sci 1:98–101. https://doi.org/10.1111/1467-8721.ep10768783
Conklin HM, Ness KK, Ashford JM et al (2019) Cognitive performance, aerobic fitness, motor proficiency, and brain function among children newly diagnosed with craniopharyngioma. J Int Neuropsychol Soc 25:413–425. https://doi.org/10.1017/S1355617718001170
Cox E, Bells S, Timmons BW et al (2020) A controlled clinical crossover trial of exercise training to improve cognition and neural communication in pediatric brain tumor survivors. Clin Neurophysiol 131:1533–1547. https://doi.org/10.1016/j.clinph.2020.03.027
de Baptista CR, Vicente AM, Souza MA et al (2020) Methods of 10-meter walk test and repercussions for reliability obtained in typically developing children. Rehabil Res Pract. https://doi.org/10.1155/2020/4209812
DeSantis CE, Lin CC, Mariotto AB et al (2014) Cancer treatment and survivorship statistics. Cancer 64:252–271. https://doi.org/10.3322/caac.21235
Deutsch JE, Brettler A, Smith C et al (2011) Nintendo Wii sports and Wii fit game analysis, validation, and application to stroke rehabilitation. Top Stroke Rehabil 18(6):701–719. https://doi.org/10.1310/tsr1806-701
Faul F, Erdfelder E, Buchner A, Lang AG (2009) Statistical power analyzes using G*power 3.1: tests for correlation and regression analyses. Behav Res Methods 41:1149–1160. https://doi.org/10.3758/BRM.41.4.1149
Gokeler A, Bisschop M, Myer GD et al (2016) Immersive virtual reality improves movement patterns in patients after ACL reconstruction: implications for enhanced criteria-based return-to-sport rehabilitation. Knee Surg Sports Traumatol Arthrosc 24:2280–2286. https://doi.org/10.1007/s00167-014-3374-x
Gouveia E, Silva EC, Lange B, Bacha JMR, Pompeu JE (2020) Effects of the interactive videogame Nintendo Wii sports on upper limb motor function of individuals with post-polio syndrome: a randomized clinical trial. Games Health J 9:461–471. https://doi.org/10.1089/g4h.2019.0192
Hansen A, Søgaard K, Minet LR, Jarden JO (2018) A 12-week interdisciplinary rehabilitation trial in patients with gliomas—a feasibility study. Disabil Rehabil 40:1379–1385. https://doi.org/10.1080/09638288.2017.1295472
Kim J, Shin W (2014) How to do random allocation (randomization). Clin Orthop Surg 6:103–109. https://doi.org/10.4055/cios.2014.6.1.103
Meldrum D, Glennon A, Herdman S et al (2012) Virtual reality rehabilitation of balance: assessment of the usability of the Nintendo Wii® Fit Plus. Disabil Rehabil Assist Technol 7:205–210. https://doi.org/10.3109/17483107.2011.616922
Meyns P, Pans L, Plasmans K et al (2017) The effect of additional virtual reality training on balance in children with cerebral palsy after lower limb surgery: a feasibility study. Games Health J 6:39–48. https://doi.org/10.1089/g4h.2016.0069
Miller KD, Nogueira L, Mariotto AB et al (2019) Cancer treatment and survivorship statistics. CA Cancer J Clin 69:363–385. https://doi.org/10.3322/caac.21565
Montoro-Cárdenas D, Cortés-Pérez I, Zagalaz-Anula N et al (2021) Nintendo Wii balance board therapy for postural control in children with cerebral palsy: a systematic review and meta-analysis. Dev Med Child Neurol 63:1262–1275. https://doi.org/10.1111/dmcn.14947
O’Reilly RC, Morlet T, Cushing SL (2013) Manual of pediatric balance disorders. Plural Publishing, San Diego
Ospina PA, McComb A, Pritchard-Wiart LE et al (2021) Physical therapy interventions, other than general physical exercise interventions, in children and adolescents before, during and following treatment for cancer. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD012924.pub2
Palmer SN, Meeske KA, Katz ER et al (2007) The PedsQL™ brain tumor module: initial reliability and validity. Pediatr Blood Cancer 49:287–293. https://doi.org/10.1002/pbc.21026
Pollack IF (1994) Brain tumors in children. New Engl J Med 331:1500–1507. https://doi.org/10.1056/NEJM199412013312207
Putnam C, Cheng J, Seymour G (2014) Therapist perspectives: Wii active videogames use in in-patient settings with people who have had a brain injury. Games Health J 3:366–370. https://doi.org/10.1089/g4h.2013.0099
Riggs L, Piscione J, Laughlin S et al (2017) Exercise training for neural recovery in a restricted sample of pediatric brain tumor survivors: a controlled clinical trial with crossover of training versus no training. Neuro Oncol 19:440–450. https://doi.org/10.1093/neuonc/now177
Runco DV, Yoon L, Grooss SA, Wong CK (2019) Nutrition and exercise interventions in pediatric patients with brain tumors: a narrative review. J Natl Cancer Inst Monogr. https://doi.org/10.1093/jncimonographs/lgz025
Sabel M, Sjölund A, Broeren J et al (2016) Active video gaming improves body coordination in survivors of childhood brain tumors. Disabil Rehabil 38:2073–2084. https://doi.org/10.3109/09638288.2015.1116619
Sato I, Higuchi A, Yanagisawa T et al (2014) Impact of late effects on health-related quality of life in survivors of pediatric brain tumors: motility disturbance of limb(s), seizure, ocular/visual impairment, endocrine abnormality, and higher brain dysfunction. Cancer Nurs 37:E1–E14. https://doi.org/10.1097/NCC.0000000000000110
Sklar CA (2002) Childhood brain tumors. J Pediatr Endocr Met 15:669–674. https://doi.org/10.1515/JPEM.2002.15.S2.669
Sparrow J, Zhu L, Gajjar A et al (2017) Constraint-induced movement therapy for children with brain tumors. Pediatr Phys Ther 29:55–61. https://doi.org/10.1097/PEP.0000000000000331
Tanriverdi M, Cakir FB (2023) Cancer-related fatigue and daily living activities in pediatric cancer survivors. J Pediatr Hematol Oncol 45:e567–e572. https://doi.org/10.1097/MPH.0000000000002581
Tanriverdi M, Cakir E, Akkoyunlu ME, Cakir FB (2022) Effect of virtual reality-based exercise intervention on sleep quality in children with acute lymphoblastic leukemia and healthy siblings: a randomized controlled trial. Palliat Support Care 20:455–461. https://doi.org/10.1017/S1478951522000268
Tanriverdi M, Cakir FB, Mutluay FK (2023) Efficacy of a virtual reality-based intervention in children with medulloblastoma: case series. An Pediatr (engl Ed) 98:62–65. https://doi.org/10.1016/j.anpede.2022.04.013
Tatla SK, Radomski A, Cheung J et al (2014) Wii-habilitation as balance therapy for children with acquired brain injury. Dev Neurorehabil 17:1–15. https://doi.org/10.3109/17518423.2012.740508
Varedi M, Lu L, Phillips NS et al (2021) Balance impairment in survivors of pediatric brain cancers: risk factors and associated physical limitations. J Cancer Surviv 15:311–324. https://doi.org/10.1007/s11764-020-00932-5
Varni JW, Burwinkle TM, Seid M, Skarr D (2003) The PedsQL 4.0 as a pediatric population health measure: feasibility, reliability, and validity. Ambul Pediatr 3:329–341. https://doi.org/10.1367/1539-4409(2003)003%3c0329:tpaapp%3e2.0.co;2
Wall JC, Bell C, Campbell S, Davis J (2000) The Timed Get-up-and-Go test revisited: measurement of the component tasks. J Rehabil Res Dev 37:109–113
Wang M, Reid D (2011) Virtual reality in pediatric neurorehabilitation: attention deficit hyperactivity disorder. autism and cerebral palsy. Neuroepidemiology 36:2–18. https://doi.org/10.1159/000320847
Wikstrom EA (2012) Validity and reliability of Nintendo Wii Fit balance scores. J Athl Train 47:306–313. https://doi.org/10.4085/1062-6050-47.3.16
Wrisley DM, Pavlou M (2005) Physical therapy for balance disorders. Neurol Clin 23:855–874. https://doi.org/10.1016/j.ncl.2005.01.005
Zaino CA, Marchese VG, Westcott SL (2004) Timed up and down stairs test: preliminary reliability and validity of a new measure of functional mobility. Pediatr Phys Ther 16:90–98. https://doi.org/10.1097/01.PEP.0000127564.08922.6A
Zoccolillo L, Morelli D, Cincotti F et al (2015) Video-game based therapy performed by children with cerebral palsy: a cross-over randomized controlled trial and a cross-sectional quantitative measure of physical activity. Eur J Phys Rehabil Med 51:669–676
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tanrıverdi, M., Mutluay, F.K. & Çakιr, F.B. Video-based exergaming versus conventional rehabilitation on balance in pediatric brain tumor survivors: a randomized clinical trial. Virtual Reality 28, 94 (2024). https://doi.org/10.1007/s10055-024-00988-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10055-024-00988-z