
Abstract
Virtual nature is an innovative approach for promoting mental health. The purpose of this study was to compare the effects on mental health outcomes between two immersion levels of virtual reality natural experiences. The study design was a cluster trial. Healthy adults were allocated to two experimental groups. Identical pre-recorded 360° videos of natural scenes and sounds were played on the two virtual reality devices, one with a higher immersive level via a head-mounted display and the other one with a lower immersive level via a smartphone. The intervention was conducted for 30 min per session, once a week for 12 weeks. Data were collected by self-reported questionnaires at the baseline and post-intervention. In total, 54 participants completed the interventions. A significantly greater effect was revealed on improving happiness, self-rated health, and physical, mental, social, and environmental quality of life, and ameliorating distress, depression, and somatization in participants who experienced the higher immersive level compared to participants who experienced the lower immersive level. Virtual reality natural experiences with high immersion are recommended to promote mental health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Natural environments have multiple health benefits for individuals living in urban areas (Bezold et al. 2018; Dzhambov et al. 2018). Spending time in urban parks, gardens, and green spaces for exposure to nature might increase one’s positive mood, self-esteem, social interactions, community engagement, a sense of belonging, and quality of life (QOL), while also reducing stress, anxiety, depression, and the risk of chronic diseases (Dzhambov et al. 2018).
However, urban residents may still experience several barriers that impede their ability to visit natural environments due to personal (i.e., age, physical limitations, and health conditions), interpersonal (i.e., lack of social support from family, friends, and peers), structural (i.e., time and cost), and environmental constraints (i.e., crowded traffic, safety, weather conditions, and a lack of accessibility) (Du et al. 2021; Rushing et al. 2019). To overcome such constraints, the natural environment can be brought from the outdoors into indoor environments through photographs, videos, live streaming, and virtual reality (VR). A highly controlled immersive virtual environment (IVE) can become a channel and opportunity for urban residents to be exposed to nature (Brivio et al. 2021; Calogiuri et al. 2018; Wang et al. 2019). Virtual nature refers to simulated experiences of being in nature regardless of whether or not one has access to nature. It involves using VR technology to provide audiovisual or multisensory simulations of natural environments (Browning et al. 2023).
Immersion is defined as the objective and quantifiable extent to which the device displays are capable of delivering an inclusive, extensive, surrounding, and vivid illusion of reality to human participants’ senses. Additionally, the presence is defined as a state of self-consciousness and the psychological sense of being in the IVEs (Slater and Wilbur 1997). The level of immersion can be increased to reinforce the user’s sense of presence in IVEs. A previous meta-analysis included evidence from 83 studies containing varied operationalizations of immersion and presence. The meta-analytical result suggested that technological immersion has an overall effect on presence with a medium effect size. In addition, increasing levels of user-tracking, the use of stereoscopic visuals, wider fields of view of visual display, and quality of visual and auditory content might improve the presence (Cummings and Bailenson 2016).
Virtual nature can include pictures, videos, or immersive media that recreate the sights, sounds, and sensations of being in nature (Browning et al. 2023). Individuals’ natural experiences can be divided up according to the degree of immersion. From high to low immersion levels, the highest one is being present in a real natural environment, followed by being a short distance from a natural environment (close to the seaside or on a riverside bridge), being a long distance from the natural environment (viewing it through a window or only hearing nature sounds), experiencing VR-based natural IVEs, and the lowest one is using natural photographs and videos (Dempsey et al. 2018; Palanica et al. 2019).
The immersion level might be key to affecting mental health outcomes when experiencing VR nature (Lundstedt et al. 2018). Users can use VR devices, computer hardware, and software to watch 2D or 3D stereoscopic and 360° visual effects of the virtual world with a nature experience (Calogiuri et al. 2018). Multisensory stimulation may increase the sense of presence in a VR natural experience, including visual stimuli of scenery (i.e., trees, flowers, and green spaces) and audio stimuli of soundscapes (i.e., anthrophony, biophony, and geophony) (Li et al. 2018). Visual and audio stimuli are more common to be included in VR experiences than other stimuli, such as wind, scent, touch, vibration, and temperature (Melo et al. 2022). In addition to 3D videos applied in VR, a monoscopic 360° video refers to a type of VR video that captures a panoramic view of a scene in a 360° format. The video is rendered in a way that appears immersive and realistic when viewed through a head-mounted display (HMD), smartphone, or on a PC monitor. In a monoscopic 360° video, the same footage is presented for both eyes, lacking the depth sensation that stereoscopic videos offer. The monoscopic 360° videos are an easy way to capture and have a low production cost, making them increasingly popular (Knaust et al. 2022).
Popular commercial immersive VR devices include HMDs, stereoscopic projection screens, computer automatic virtual environments (CAVEs), and smartphones with VR adaptors (Calogiuri et al. 2018; Lundstedt et al. 2018). HMDs offer a more highly immersive experience compared to smartphone-based VR due to a wider field of view, high-fidelity audio quality, motion-tracking sensors that accurately track the user’s head movements in real-time, and a design with a comfortable and stable fit. HMDs typically provide more-robust and complete immersion with their superior technology and design specifically for VR by minimizing the sense of being constrained, distracted, or uncomfortable (Bruun-Pedersen et al. 2016; Marín-Morales et al. 2019; Moyle et al. 2018).
1.1 Related work
VR technologies provide different ways to restore attention and promote interactions with natural scenes and sounds to increase the users’ connectedness with nature for mental health benefits (Bornioli et al. 2018; Snell et al. 2018). Immersive VR technologies can create immersive and realistic environments that can induce positive emotions, decrease negative affect, and enhance emotional experiences through the sense of presence in natural content for relaxation purposes. Higher levels of immersion in VR lead to a greater sense of presence and increased subjective arousal. This indicates that VR can provide a highly engaging and emotionally stimulating experience from delivery modes of virtual nature that might enhance positive emotions and overall mental well-being (Pavic et al. 2023; Yeo et al. 2020).
IVEs have widely been applied in the treatment, rehabilitation, training, education, gaming, and outdoor experiences for mental health illness and mental health promotion (Roche et al. 2019). Virtual parks simulate real parks with multisensory stimuli for attention and mental restoration, emotional stability, and stress recovery (Sun et al. 2023). Previous experimental studies suggested that VR natural experiences across different populations could improve multiple mental health outcomes, including physiological and psychological stress indicators, affects (Allen et al. 2018), relaxation, perceived restoration (Bornioli et al. 2018), happiness, moods, awareness (Moyle et al. 2018), emotions (Olafsdottir et al. 2017), anxiety (Wang 2019), distress, nervousness (Veling et al. 2021), and depressive symptoms (Boffi et al. 2022).
Even previous studies have suggested that VR nature had potential positive improvement on participants’ mental health. However, they commonly used a comparatively lower immersion level to create VR natural experiences, including photographs (Gao et al. 2019; Jung et al. 2017), 2D videos (Hedblom et al. 2019), and streaming synchronous videos (Snell et al. 2018). These studies indicated that improving the immersion level to enhance the sense of presence during VR natural experiences simulating the real world might be more effective in promoting mental health outcomes (Gao et al. 2019; Hedblom et al. 2019; Jung et al. 2017). However, these previous studies often conducted a single-time intervention to examine the short-term mental health effect. That exposure times and duration of the total intervention can be extended was suggested.
The evidence for finding the best immersion level of VR natural experiences for better mental health effects is still insufficient. One experimental study was conducted with 26 participants to view 360° videos with nature elements on a higher immersive HMD and a less-immersive computer screen. Participants who experienced an HMD condition revealed an improvement in positive emotions, sense of presence, and physiological responses (Pavic et al. 2023). The other study involved 102 adults presenting monoscopic 360° nature videos through an HMD or a PC monitor. The participants in HMD were more psychologically relaxed, compared to a PC condition. Participants’ physiological stress did not reveal a difference between HMD and PC conditions (Knaust et al. 2022). Another laboratory-based study conducted VR nature by 2D videos on a TV screen, 360° videos via HMD, and interactive computer-generated VR content via HMD. The boredom and negative affects did not reveal a difference among the three conditions (Yeo et al. 2020). However, these study results on mental health effects have not reached a consistent conclusion yet. There was still a research gap in understanding whether the different VR immersive levels with the same natural content might have a different impact on multiple mental health indicators.
There are several technical differences between dedicated HMD headsets and smartphones used for VR experiences. These differences are crucial for understanding the varying capabilities and experiences these devices offer and include processing power, sensors, display quality, optical lenses, and tracking systems. HMD headsets typically have more powerful processors designed for rendering complex environments and maintaining high frame rates, high-quality sensors for precise tracking of head movements and positions, a high-resolution display with rapid refresh rates and lower latency, custom-designed lenses to provide a wider field of view, and advanced tracking systems that allow for full six degrees of freedom (6DoF) tracking. While smartphones are powerful devices with generally smaller screens and less weight, they might not have the same level of processing power, resolution, or refresh rates as dedicated VR systems. Smartphone-based VR relies on sensors within the phone itself for tracking, and 3DoF tracking can be less precise (Molina et al. 2022; Papachristos et al. 2017; Radianti et al. 2020). Overall, VR headsets offer smoother, more-immersive, and more-impressive experiences due to their specialized hardware and optimized VR designs. This was the rationale for developing the HMD-based and smartphone-based VR interventions in this study.
The rationale of the current study indicates real natural environment through the sensory stimuli of natural elements may provide mental health benefits for urban residents’ relaxation (Bezold et al. 2018; Dzhambov et al. 2018). VR technology can be applied to simulate natural experiences by providing sensory stimuli of natural elements, especially audio and vision (Lundstedt et al. 2018). The evidence suggested that the immersive level of VR nature might affect mental health outcomes differently but without a consistent conclusion (Knaust et al. 2022; Pavic et al. 2023; Yeo et al. 2020). The problem might be a single-time intervention for short-term effects. To fill the research gap, the current study aimed to compare two immersive levels of VR devices for long-term mental health effects. The intervention was designed for multiple exposure times with more frequent VR stimuli for a longer duration.
1.2 Purpose
The purposes of this study were to explore the mental health benefits of VR natural experiences and compare the effects between two immersion levels. This VR-based intervention was designed with identical monoscopic 360° videos containing natural scenes and sounds. The VR device with a higher immersive level was an HMD and the lower immersive level used a smartphone. Mental health outcomes included happiness, self-rated health, distress, anxiety, depression, somatization, and various QOL domains.
2 Methods
2.1 Study design
This single-blinded, two-armed cluster trial was conducted between February and June 2021. Participants were recruited from banks in Taipei City. Participants in one office were allocated to the HMD group, and participants in the other office were allocated to the smartphone (SP) group by drawing. Participants in one group were not aware of the existence of the other group. Data were collected twice at the baseline and post-intervention. Participants who agreed to join the study were required to sign an informed consent form before the intervention and data collection.
2.2 Participants
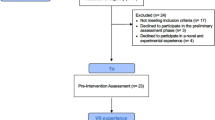
Participants were healthy adults aged 20–50 years with no serious diseases, disabilities, or health problems that might potentially influence the study process and mental health outcomes. Participants with past uncomfortable experiences during the VR were excluded. In total, 30 participants in one office were recruited and allocated to the HMD group and 29 participants in the other office were allocated to the SP group. 50.0% of men (n = 15) and 50.0% of women (n = 15) are in the HMD group, while 34.5% of men (n = 10) and 65.5% of women (n = 19) are in the SP group. The study flow is illustrated in Supplementary Figure S1.
2.3 The intervention: VR natural experiences
The research team recorded videos of natural environments with a 360° camera (Insta360 EVO, Insta360, China). The natural environments we chose were landscapes with lots of natural elements, such as trees, grass, woods, mountains, forests, and rivers (Supplementary Figures S2). The videos were recorded on a sunny day in the afternoon by walking and cycling according to the route and terrain. In total, 12 different natural landscapes were edited into monoscopic 360° videos. However, the simple 360° camera with front and back two lenses was used to make the videos that might have immersion-reducing properties.
The intervention was designed for 30 min per session, once a week for 12 weeks. The 12 monoscopic 360° videos with natural scenes and sounds were played via an HMD or smartphone. Participants can freely choose when they want to proceed with the VR intervention, such as during break time or after work. Participants were asked to get sufficient sleep before the experiment day. To avoid being uncomfortable during VR sessions, they were asked not to do excessive exercise or consume too much food or coffee before the session (Jiang et al. 2014). Participants who felt dizzy or uncomfortable during the session were encouraged to temporarily close their eyes and pause the video.
2.3.1 The HMD group: the higher immersive level
The HMD group was designed for a higher immersive level of VR natural experiences. Participants watched monoscopic 360° videos with sound via an HMD device during the session. Participants were required to sit in a comfortable chair and wear the HMD headset (Oculus Quest 2, Meta, USA) (Fig. 1a, b). In each session, participants were allowed to move their heads with 3DoF (rotational movements in three axes: pitch, yaw, and roll) to freely watch the videos (Knaust et al. 2022). The research team monitored the one-on-one weekly sessions in the HMD group to monitor whether the participants felt uncomfortable for safety.

Head-mounted displays (HMD) group (a front view, b side view); The smartphone (SP) group (c front view, d side view)
2.3.2 The SP group: the lower immersive level
The SP group was designed for lower immersive levels of VR natural experiences. Participants watched monoscopic 360° videos with sound via a smartphone during the session. Participants in the SP group were allowed to use their own smartphones. Participants were required to sit on a chair in a comfortable posture and put their own smartphones in front of them (Fig. 1c, d). In each session, participants were allowed to freely move their smartphones to watch the videos from different angles. All sounds were played by HMD or smartphones without any additional devices. Participants can freely control the volume to be comfortable.
2.4 Data collection
All data were collected by self-administered, structured questionnaires at the baseline and post-intervention. Participants’ backgrounds consisted of age, gender, education level, alcohol use (yes/no), smoking (yes/no), and chronic diseases (yes/no). Mental health outcomes were also assessed.
Happiness was assessed by a single item of “Do you generally feel happy?” on an 11-point scale from very unhappy to very happy (Abdel-Khalek 2006). Self-rated health was assessed by another item, “In general, would you say your health is?” on a five-point scale of poor, fair, good, very good, or excellent (Hays et al. 2015).
QOL was assessed by the World Health Organization Quality of Life Scale-BREF version (World Health Organization 2019). The scale consists of 26 items on a five-point scale. Four subscales were calculated by the average score, including physical, mental, social, and environmental QOL. The scale revealed good test–retest reliability, construct validity, and discriminant validity (Yao et al. 2002). Cronbach’s α in this study was 0.917.
The four-dimensional symptom questionnaire (4DSQ) was used to assess four common mental health problems, including distress, anxiety, depression, and somatization. The 4DSQ consists of 50 items on a five-point scale from no to very often (constantly). The four subscales were calculated by the average score for the severity of mental health problems. A higher score represents worse mental health. The 4DSQ revealed good content validity, criterion-related validity, and construct validity (Terluin et al. 2016). Cronbach’s α in this study was 0.940.
2.5 Statistical analysis
Descriptive analyses were performed on participants’ background information and outcomes by the frequency and percentage of categorical variables and the mean and standard deviation (SD) of continuous variables. Chi-squared tests were performed to compare participants’ backgrounds between the SP and HMD groups. Cramer’s V was calculated for effect sizes of the chi-squared tests. Independent t tests were performed to compare participants’ age and mental health outcomes at the baseline between the two groups. Dependent t tests and mean differences (MD) were calculated for differences in mental health scores between the baseline and post-intervention in each group. Cohen’s d was calculated for effect sizes of t tests. Cohen’s d values of 0.2, 0.5, and 0.8 are considered small, medium, and large (Cohen 1988). A generalized estimating equation (GEE) was used to analyze the between-group effect and group-by-time interaction on outcomes. The GEE was adjusted for participants’ age and baseline scores. SPSS 18.0 software was used for all statistical analyses.
3 Results
Participants’ background and mental health scores at the baseline are given in Table 1. No significant differences in gender, educational levels, alcohol use, smoking, or chronic diseases were revealed between the HMD and SP groups. However, participants’ age (p < 0.001) in the HMD group were significantly lower than those of participants in the SP group with a large effect size (d = 2.98). Regarding baseline scores, participants in the HMD group had a significantly higher score of happiness (p = 0.002, d = 0.83) with large effect size, self-rated health (p = 0.005, d = 0.76), physical (p = 0.034, d = 0.56), mental (p = 0.025, d = 0.60), and environmental QOL (p = 0.003, d = 0.79) with medium effect sizes than those in the SP group. Participants in the HMD group had a significantly lower score of distress (p = 0.013, d = 0.67), depression (p = 0.012, d = 0.70) with a medium effect size, and somatization (p < 0.001, d = 1.26) with a large effect size than those in the SP group. The baseline assessment suggested very different populations between the two groups.
Finally, 30 participants in the HMD group and 24 participants in the SP group completed the interventions and post-intervention data collection. No participant complained of being uncomfortable during the VR sessions, such as nausea, drowsiness, headaches, disorientation, or vomiting.
The result before and after the intervention within each group is given in Table 2. Only participants in the HMD group increased their score of happiness with a small effect size (p = 0.037, d = 0.20) after the intervention, respectively. No other mental health outcomes have changed significantly before and after the intervention within either HMD or SP groups. A correlation matrix of mental health scores before and after the intervention in both groups is demonstrated in Supplementary Table S1. The result indicates a medium to high positive correlation among mental health outcomes in each group before and after the intervention.
A GEE was used to examine the effects of group and group-by-time interactions which were adjusted for participants’ age and baseline scores. The GEE results are given in Table 2. Participants in the HMD group exhibited significantly increased happiness (MD = 0.47, p = 0.037), while participants in the SP group exhibited decreased happiness (MD = − 0.17) with significant group effects (p < 0.001). Participants in the HMD group exhibited increased self-rated health (MD = 0.03), while participants in the SP group exhibited decreases in self-rated health (MD = -0.17) with significant group effects (p = 0.001). Participants in the HMD group exhibited increased physical (MD = 0.04), mental (MD = 0.03), and environmental QOL (MD = 0.13), while participants in the SP group exhibited decreases in these outcomes with significant group-by-time interactions (p = 0.004; p = 0.031; p = 0.044). Participants in the HMD group exhibited increased social QOL (MD = 0.06), while participants in the SP group exhibited a decrease in this outcome with a significant group effect (p = 0.006).
Participants in the HMD group exhibited decreased distress (MD = −0.17) and somatization (MD = −0.77), while participants in the SP group exhibited increases in these outcomes with significant group-by-time interactions (p = 0.040; p = 0.005). Participants in the HMD group (MD = −0.30) exhibited a greater decrease in depression scores than the SP group (MD = −0.08) with a significant group-by-time interaction (p = 0.043).
4 Discussion
This study conducted HMD-based and smartphone-based VR interventions to compare the mental health effects between high and low immersion levels of VR natural experiences. The GEE result suggests different directions in change over time after the intervention between the HMD and SP groups. Participants in the HMD group exhibited increased happiness after the VR natural experiences. Better effects of improving happiness, self-rated health, physical, mental, social, and environmental QOL, distress, depression, and somatization were found in participants who experienced the higher immersive level compared to those who experienced the lower immersive level. However, the different baseline scores suggested very different participants’ characteristics between the experimental and control groups due to a lack of randomization. This may have severely compromised the findings. The interpretability of the changes over time might not solely have been due to the VR interventions.
The current study found that VR natural experiences were found to have positive effects on individuals’ mental health outcomes. Previous studies also suggested a similar result that VR natural experiences improve mental health outcomes (Boffi et al. 2022; Moyle et al. 2018; Veling et al. 2021; Wang et al. 2019). A previous randomized control trial conducted a VR nature study by watching one of six 4-min monoscopic 360° videos of natural environments on VR headsets from Monday to Saturday each week (Browning et al. 2023). Their main result revealed that daily exposure to virtual nature reduced symptoms of anxious arousal and anxious apprehension in college students. This effect was particularly strong for female participants who had previous experience with VR and the outdoors and found beauty in nature. A small effect size between virtual nature and mental health outcomes was revealed, similar to our study. However, a previous study did not find that participants exhibited a significant effect on perceived restoration and mood after sitting in a chair with a VR natural experience compared to only a sitting situation (Browning et al. 2020). One possible reason might have been that that study only conducted a single session for short-term effects on mental health outcomes.
The current study compared the VR natural experiences with two immersive levels. The different directions of the changed score before and after the intervention were found in over half of the mental health outcomes between the HMD and SP groups. A previous review of different VR devices had a similar suggestion that a VR-based nature intervention with a high immersive level, more interaction, and 360° videos could increase positive affect, relations, and sense of presence, while decreasing depression compared to those with a lower immersive level, such as traditional 2D videos and non-interactive VR (Li et al. 2021). Another previous randomized controlled trial suggested similar results in children with cancer. That trial conducted VR natural experiences via an HMD and a tablet as the comparator group. VR with higher immersion exhibited greater improvements in all scores of visual analog scales, including for a positive mood, anxiety, anger, nausea, and pain (Tennant et al. 2020). A previous interventional study found similar results of the level of immersion in VR technology has a significant influence on emotional responses. Participants reported more positive emotions and greater subjective arousal after viewing the videos in the highly immersive setting (HMD) compared to the less-immersive setting (computer screen). The higher levels of immersion provided by the HMD could elicit positive emotions (Pavic et al. 2023).
In contrast, not every mental health indicator revealed a significant improvement in previous studies. One study found that a smartphone-based VR intervention had a significant effect on improving participants’ moods, but that did not change in the HMD-based group (Liu et al. 2020). One possible reason may have been that the population was older adults aged over 60 years, which differed from the current study. Older adults’ preferences and feelings about VR devices should be considered. The other study compared the effects of viewing virtual nature videos through an HMD or a PC monitor, as well as a control condition with no video, on relaxation. The results indicated a significant decrease in stress for both the HMD and PC conditions compared to the control condition, but with no significant difference between the HMD and PC conditions. Participants in the HMD condition reported higher perceived relaxed than the other conditions (Knaust et al. 2022). Another study compared the effect of different displays of a virtual underwater scene on mood changes. The study found that a computer-programmed 3D underwater condition presented with an HMD evoked a stronger positive mood compared to a monoscopic 360° video presented with the same HMD and a traditional video displayed on a TV screen. However, there were no significant differences in mood changes between the 360° video and the TV condition (Yeo et al. 2020). One possible reason may be that these studies only conducted a single-time intervention, so no consistent results have been reached on short-term mental health outcomes.
4.1 Limitations
However, several limitations of the current study are worth mentioning. The first major limitation of the study design was a cluster trial with a small sample size, instead of a randomized controlled trial. Due to the absence of randomization, the baseline levels of the two groups are hardly comparable. Participants’ age and several mental health scores at the baseline exhibited significant differences. Although the GEE was adjusted for these differences, the outcomes should be applied with caution in the future. Second, this study did not recruit a control group with no intervention to compare the effects of VR natural experiences. The improvements in mental health outcomes between the baseline and post-intervention were not guaranteed to exclusively be due to the intervention. There might have been other factors influencing the changes in mental health outcomes. Third, there were a relatively large number of outcome measures which was not considered in the power analysis. It might mislead the effect, such as multiple comparison problems.
The VR intervention was not conducted in a restricted environment. Participants might have had some distractions due to interference from external environments. This would be more of a problem in the SP group as the HMD group is better isolated from outside visual stimuli through the HMDs. The external sounds may influence both groups. The research team did not seriously restrict participants’ behaviors in each session. Thus, the immersion level of natural experiences might have been lower than what this study aimed for. Due to participants in the SP group using diversified smartphones, differences in resolution, sound quality, and personal user experiences among smartphones might have introduced a bias. Also, auditory inclusiveness in a VR experience is the practice of ensuring that individuals with a wide range of auditory abilities can fully participate in and enjoy the virtual environment (Serafin et al. 2023). Auditory inclusiveness was not standardized by using the same headphones in this study. This might have introduced a potential confounding factor.
Finally, because the 360° videos were recorded in motion, cybersickness can be induced. VR sickness, also known as motion cybersickness in VR or simulators, is a condition that occurs when an individual experiences symptoms of nausea, disorientation, dizziness, or discomfort (Chang et al. 2020). The current study did not conduct an assessment of VR sickness during the intervention or adequately document its occurrence. We only observed participants during the intervention sessions and asked whether they felt uncomfortable during the sessions. VR sickness should systematically be recorded with appropriate tools, such as an electroencephalogram, simulator sickness questionnaire, fast-motion sickness scale, or virtual environment performance assessment battery (Chang et al. 2020).
4.2 Implications
Based on this study, we propose several recommendations for practical applications. VR-based natural experiences with mental health benefits are recommended as an effective, safe, and acceptable intervention for individuals living in urban areas, especially those who have little motivation or many barriers to physically going to natural environments (Browning et al. 2023). Health practitioners can apply VR nature for patients with physical disabilities or mental health problems, those in intensive care units or in rehabilitation, or older adults living in long-term care facilities. HMDs typically provide more-robust and complete immersion due to their superior technology and design specifically for VR. HMDs also have a better effect on improving mental health outcomes, and they thus are recommended than smartphone-based VR in mental health care and promotion across populations.
We also make recommendations for future studies. The mental health effects of VR natural experiences can be explored in special populations across multiple healthcare settings. Other mental health outcomes that may be affected by natural environments can be considered, such as physiological and psychological stress, cognitive functions, emotional resilience, life satisfaction, or other mental health diseases. The devices used in the SP group should be the same brand and model of smartphones and headphones to reduce bias within the group. Other different immersion levels of VR devices could be compared to determine which one has the most positive impacts on mental health outcomes, such as stereoscopic VR, 3D videos, computer-generated imagery, CAVEs, and the metaverse. Finally, visional and auditory inclusiveness in VR are essential to make the medium accessible to a broader audience, regardless of their sensor abilities (Dudley et al. 2023). Designing VR experiences with inclusivity in mind ensures that everyone can enjoy and engage in the virtual environment.
5 Conclusions
To our best knowledge, this is the first study to compare the mental health effects of a 12-week monoscopic 360° natural video between two immersion levels by HMD-based and smartphone-based VR interventions. Results of the study indicated different changes in direction over time between the HMD and SP groups. However, it should be emphasized that the very different characteristics of the two groups could have undermined interpretation of the results. VR natural experiences via the HMD with a higher immersive level had greater effects on mental health outcomes than via a smartphone with a lower immersive level, of increasing happiness, self-rated health, and physical, mental, social, and environmental QOL, and reducing distress, depression, and somatization. VR natural experiences with high immersion levels are recommended for promoting mental health.
Data availability statements
The datasets generated during and analyzed during the current study are available from the corresponding author upon reasonable request.
References
Abdel-Khalek AM (2006) Measuring happiness with a single-item scale. Soc Behav Pers 34(2):139–150. https://doi.org/10.2224/SBP.2006.34.2.139
Allen JG, Spengler JD, Yin J, Zhu S, MacNaughton P (2018) Physiological and cognitive performance of exposure to biophilic indoor environment. Build Environ 132:255–262. https://doi.org/10.1016/j.buildenv.2018.01.006
Bezold CP, Banay RF, Coull BA, Hart JE, James P, Kubzansky LD, Missmer SA, Laden F (2018) The association between natural environments and depressive symptoms in adolescents living in the United States. J Adolesc Health 62(4):488–495. https://doi.org/10.1016/j.jadohealth.2017.10.008
Boffi M, Pola LG, Fermani E, Senes G, Inghilleri P, Piga BEA, Stancato G, Fumagalli N (2022) Visual post-occupancy evaluation of a restorative garden using virtual reality photography: restoration, emotions, and behavior in older and younger people. Front Psychol 13:927688. https://doi.org/10.3389/fpsyg.2022.927688
Bornioli A, Parkhurst G, Morgan PL (2018) Psychological wellbeing benefits of simulated exposure to five urban settings: an experimental study from the pedestrian’s perspective. J Transp Health 9:105–116. https://doi.org/10.1016/j.jth.2018.02.003
Brivio E, Serino S, Negro Cousa E, Zini A, Riva G, de Leo G (2021) Virtual reality and 360° panorama technology: a media comparison to study changes in sense of presence, anxiety, and positive emotions. Virtual Reality 25(2):303–311. https://doi.org/10.1007/s10055-020-00453-7
Browning MHEM, Mimnaugh KJ, van Riper CJ, Laurent HK, LaValle SM (2020) Can simulated nature support mental health? Comparing short, single-doses of 360-degree nature videos in virtual reality with the outdoors. Front Psychol 10:2667. https://doi.org/10.3389/fpsyg.2019.02667
Browning MHEM, Shin S, Drong G, McAnirlin O, Gagnon RJ, Ranganathan S, Sindelar K, Hoptman D, Bratman GN, Yuan S, Prabhu VG, Heller W (2023) Daily exposure to virtual nature reduces symptoms of anxiety in college students. Sci Rep 13(1):1239. https://doi.org/10.1038/s41598-023-28070-9
Bruun-Pedersen JR, Serafin S, Kofoed LB (2016) Restorative virtual environment design for augmenting nursing home rehabilitation. J Virtual Worlds Res 9(3):1–25. https://doi.org/10.4101/jvwr.v9i3.7224
Calogiuri G, Litleskare S, Fagerheim KA, Rydgren TL, Brambilla E, Thurston M (2018) Experiencing nature through immersive virtual environments: environmental perceptions, physical engagement, and affective responses during a simulated nature walk. Front Psychol 8:1–14. https://doi.org/10.3389/fpsyg.2017.02321
Chang E, Kim HT, Yoo B (2020) Virtual reality sickness: a review of causes and measurements. Int J Hum Comput Interact 36:1658–1682. https://doi.org/10.1080/10447318.2020.1778351
Cohen J (1988) Statistical power analysis for the behavioural science (2nd ed). In: Statistical power analysis for the behavioral sciences
Cummings JJ, Bailenson JN (2016) How immersive is enough? A meta-analysis of the effect of immersive technology on user presence. Media Psychol 19(2):272–309. https://doi.org/10.1080/15213269.2015.1015740
Dempsey S, Devine MT, Gillespie T, Lyons S, Nolan A (2018) Coastal blue space and depression in older adults. Health Place 54:110–117. https://doi.org/10.1016/j.healthplace.2018.09.002
Du J, Floyd C, Kim ACH, Baker BJ, Sato M, James JD, Funk DC (2021) To be or not to be: negotiating leisure constraints with technology and data analytics amid the COVID-19 pandemic. Leis Stud 40(4):561–574. https://doi.org/10.1080/02614367.2020.1862284
Dudley J, Yin L, Garaj V, Kristensson PO (2023) Inclusive Immersion: a review of efforts to improve accessibility in virtual reality, augmented reality and the metaverse. Virtual Reality. https://doi.org/10.1007/s10055-023-00850-8
Dzhambov AM, Markevych I, Hartig T, Tilov B, Arabadzhiev Z, Stoyanov D, Gatseva P, Dimitrova DD (2018) Multiple pathways link urban green- and bluespace to mental health in young adults. Environ Res 166:223–233. https://doi.org/10.1016/j.envres.2018.06.004
Gao Z, Zhu G, Qiu L (2019) Exploring psychophysiological restoration and individual preference in the different environments based on virtual reality. Int J Environ Res Public Health 16(17):3102. https://doi.org/10.3390/ijerph16173102
Hays RD, Spritzer KL, Thompson WW, Cella D (2015) U.S. general population estimate for “excellent” to “poor” self-rated health item. J Gen Internal Med 30(10):1511. https://doi.org/10.1007/S11606-015-3290-X
Hedblom M, Gunnarsson B, Iravani B, Knez I, Schaefer M, Thorsson P, Lundström JN (2019) Reduction of physiological stress by urban green space in a multisensory virtual experiment. Sci Rep 9(1):1–11. https://doi.org/10.1038/s41598-019-46099-7
Jiang B, Chang CY, Sullivan WC (2014) A dose of nature: tree cover, stress reduction, and gender differences. Landsc Urban Plan 132:26–36. https://doi.org/10.1016/j.landurbplan.2014.08.005
Jung M, Jonides J, Northouse L, Berman MG, Koelling TM, Pressler SJ (2017) Randomized crossover study of the natural restorative environment intervention to improve attention and mood in heart failure. J Cardiovasc Nurs 32(5):464–479. https://doi.org/10.1097/JCN.0000000000000368
Knaust T, Felnhofer A, Kothgassner OD, Höllmer H, Gorzka RJ, Schulz H (2022) Exposure to virtual nature: the impact of different immersion levels on skin conductance level, heart rate, and perceived relaxation. Virtual Reality 26(3):925–938. https://doi.org/10.1007/s10055-021-00595-2
Li H, Zhang X, Wang H, Yang Z, Liu H, Cao Y, Zhang G (2021) Access to nature via virtual reality: a mini-review. Front Psychol 12:725288. Frontiers Media S.A. https://doi.org/10.3389/fpsyg.2021.725288
Li J, Burroughs K, Halim MF, Penbrooke TL, Seekamp E, Smith JW (2018) Assessing soundscape preferences and the impact of specific sounds on outdoor recreation activities using qualitative data analysis and immersive virtual environment technology. J Outdoor Recreat Tour 24:66–73. https://doi.org/10.1016/j.jort.2018.08.001
Liu Q, Wang Y, Yao MZ, Tang Q, Yang Y (2020) The effects of viewing an uplifting 360-degree video on emotional well-being among elderly adults and college students under immersive virtual reality and smartphone conditions. Cyberpsychol Behav Soc Netw 23(3):157–164. https://doi.org/10.1089/cyber.2019.0273
Lundstedt R, Vassiljev P, Albin M, Yeo N, White MP, Wallergård M, Lõhmus M (2018) A prescription for “nature” the potential of using virtual nature in therapeutics. Neuropsychiatr Dis Treat 14:3001–3013. https://doi.org/10.2147/ndt.s179038
Marín-Morales J, Higuera-Trujillo JL, Greco A, Guixeres J, Llinares C, Gentili C, Scilingo EP, Alcañiz M, Valenza G (2019) Real vs. immersive-virtual emotional experience: analysis of psycho-physiological patterns in a free exploration of an art museum. PloS One 14(10):e223881. https://doi.org/10.1371/journal.pone.0223881
Melo M, Goncalves G, Monteiro P, Coelho H, Vasconcelos-Raposo J, Bessa M (2022) Do multisensory stimuli benefit the virtual reality experience? A systematic review. IEEE Trans Visual Comput Graphics 28(2):1428–1442. https://doi.org/10.1109/TVCG.2020.3010088
Molina G, Gimeno J, Portalés C, Casas S (2022) A comparative analysis of two immersive virtual reality systems in the integration and visualization of natural hand interaction. Multimedia Tools Appl 81(6):7733–7758. https://doi.org/10.1007/S11042-021-11760-9/TABLES/16
Moyle W, Jones C, Dwan T, Petrovich T (2018) Effectiveness of a virtual reality forest on people with dementia: a mixed methods pilot study. Gerontologist 58(3):478–487. https://doi.org/10.1093/geront/gnw270
Olafsdottir G, Cloke P, Vögele C (2017) Place, green exercise and stress: an exploration of lived experience and restorative effects. Health Place 46:358–365. https://doi.org/10.1016/j.healthplace.2017.02.006
Palanica A, Lyons A, Cooper M, Lee A, Fossat Y (2019) A comparison of nature and urban environments on creative thinking across different levels of reality. J Environ Psychol 63:44–51. https://doi.org/10.1016/j.jenvp.2019.04.006
Papachristos NM, Vrellis I, Mikropoulos TA (2017) A comparison between oculus rift and a low-cost smartphone VR headset: immersive user experience and learning. In: Proceedings–IEEE 17th International Conference on Advanced Learning Technologies, ICALT 2017, pp 477–481. https://doi.org/10.1109/ICALT.2017.145
Pavic K, Chaby L, Gricourt T, Vergilino-Perez D (2023) Feeling virtually present makes me happier: the influence of immersion, sense of presence, and video contents on positive emotion induction. Cyberpsychol Behav Soc Netw 26(4):1–7. https://doi.org/10.1089/cyber.2022.0245ï
Radianti J, Majchrzak TA, Fromm J, Wohlgenannt I (2020) A systematic review of immersive virtual reality applications for higher education: design elements, lessons learned, and research agenda. Comput Educ 147:103778. https://doi.org/10.1016/J.COMPEDU.2019.103778
Roche K, Liu S, Siegel S (2019) The effects of virtual reality on mental wellness: a literature review. Ment Health Fam Med 14:811–818
Rushing JR, Needham MD, D’Antonio A, Metcalf EC (2019) Barriers to attachment? Relationships among constraints, attachment, and visitation to urban parks. J Outdoor Recreat Tour 27:100228. https://doi.org/10.1016/j.jort.2019.100228
Serafin S, Adjorlu A, Percy-Smith LM (2023) A review of virtual reality for individuals with hearing impairments. Multimodal Technol Interact MDPI 7(4):36. https://doi.org/10.3390/mti7040036
Slater M, Wilbur S (1997) A Framework for Immersive Virtual Environments (FIVE): speculations on the role of presence in virtual environments. Presence: Teleoperators Virtual Environ 6(6):603–616. http://www.cs.ucl.ac.uk/staff/M.Slater
Snell TL, McLean LA, McAsey F, Zhang M, Maggs D (2018) Nature streaming: contrasting the effectiveness of perceived live and recorded videos of nature for restoration. Environ Behav. https://doi.org/10.1177/0013916518787318
Sun Y, Li F, He T, Meng Y, Yin J, Yim IS, Xu L, Wu J (2023) Physiological and affective responses to green space virtual reality among pregnant women. Environ Res 216:114499. https://doi.org/10.1016/j.envres.2022.114499
Tennant M, Youssef GJ, McGillivray J, Clark TJ, McMillan L, McCarthy MC (2020) Exploring the use of immersive virtual reality to enhance psychological well-being in pediatric oncology: a pilot randomized controlled trial. Eur J Oncol Nurs 48:101804. https://doi.org/10.1016/j.ejon.2020.101804
Terluin B, Smits N, Brouwers EPM, de Vet HCW (2016) The Four-Dimensional Symptom Questionnaire (4DSQ) in the general population: Scale structure, reliability, measurement invariance and normative data: a cross-sectional survey. Health Qual Life Outcomes 14(1):1–16. https://doi.org/10.1186/s12955-016-0533-4
Veling W, Lestestuiver B, Jongma M, Hoenders HJR, Driel CV (2021) Virtual reality relaxation for patients with a psychiatric disorder: crossover randomized controlled trial. J Med Internet Res 23(1):e17233. https://doi.org/10.2196/17233
Wang T-C, Tsai C-L, Tang T-W, Wang W-L, Lee K-T (2019) The effect of cycling through a projection-based virtual environment system on generalized anxiety disorder. J Clin Med 8(7):973. https://doi.org/10.3390/jcm8070973
Wang X, Shi Y, Zhang B, Chiang Y (2019) The influence of forest resting environments on stress using virtual reality. Int J Environ Res Public Health 16(18):3263. https://doi.org/10.3390/ijerph16183263
World Health Organization (2019) WHO quality of life-BREF. https://www.who.int/mental_health/publications/whoqol/en/
Yao G, Chung CW, Yu CF, Wang J. Der (2002) Development and verification of validity and reliability of the WHOQOL-BREF Taiwan version. J Formosan Med Assoc 101(5):342–351
Yeo NL, White MP, Alcock I, Garside R, Dean SG, Smalley AJ, Gatersleben B (2020) What is the best way of delivering virtual nature for improving mood? An experimental comparison of high definition TV, 360° video, and computer generated virtual reality. J Environ Psychol 72:101500. https://doi.org/10.1016/j.jenvp.2020.101500
Funding
This work was supported by the Ministry of Science and Technology, Taiwan under grant [MOST 109-2314-B-038-077-MY3].
Author information
Authors and Affiliations
Contributions
Yen involved in data curation; project administration; methodology; software; investigation; formal analysis; and writing. Hsu involved in writing—review. Huang involved in writing—review.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to declare.
Ethical approval
Ethical approval for this study was obtained from the Taiwan Medical University-Joint Institutional Review Board (N202004063).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yen, HY., Hsu, H. & Huang, WH. Virtual reality natural experiences for mental health: comparing the effects between different immersion levels. Virtual Reality 28, 52 (2024). https://doi.org/10.1007/s10055-024-00958-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10055-024-00958-5