
Abstract
This experiment examined the feasibility of 360° video as a tool for public health messaging by investigating the effect that viewing the 360° documentary The Waiting Room VR had on female viewers’ sense of identification, attitudes to breast cancer screening and mortality salience. A key part of the documentary places participants in a viewpoint ambiguously aligned to that of the film’s director and subject, Victoria Mapplebeck (VM), in a scene that recreates her radiotherapy treatment for breast cancer. Eighty female participants watched the documentary either sitting upright with the chair back set at a 90° angle or reclining with the chair back set at a 140° angle (consistent with VMs posture) under conditions of either high or low cognitive load. The effect of posture type was measured explicitly using questionnaires on presence, identification and breast self-examination (BSE) intention as well as implicitly using a lexical decision task to measure death-thought awareness (DTA). Reclined posture led to a higher sense of spatial presence but no increase in identification with VM. Significantly increased identification with VM led to greater intention to conduct BSE. There were no effects of posture, cognitive load or identification on DTA. The implications of these results for using 360° video as a behaviour change tool, the effects of the COVID-19 pandemic on the terror management manipulation and the relevance of spatial viewpoint in 360° video are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Recent advances in virtual reality technology (VR; see supplementary materials for a full table of acronyms) have produced considerable interest in the development of non-fiction VR content (Bevan et al. 2019). One key part of VR’s appeal lies in its ability to enable the user to see the world through the perspective of another. It has been argued that this ability to shift perspective has the potential to increase empathy, change attitudes and influence behaviour (Bertrand et al. 2018; Farmer and Maister 2017; Ventura et al. 2020). One area in which this effect could be particularly valuable is in the transmission of public health-related messages. In the current study, participants viewed a 360° video documentary recounting the director Victoria Mapplebeck’s (VM) treatment for breast cancer using a head-mounted display. We manipulated the postural match between VM and the participant to increase or decrease identification with her. We then examined the effect of this manipulation and of identification with VM on participants’ intention to conduct breast self-examination (BSE) and on their levels of death-thought awareness (DTA).
1.1 Virtual reality, embodiment and empathy
One of the key reasons that VR may increase empathy more than other forms of media is that it allows the user to experience a strong sense of embodying another person (Bailey et al. 2016; Kilteni et al. 2012). Kilteni et al. (2012) suggest embodiment consists of three subcomponents: the sense of self-location, the sense of agency, and the sense of body ownership. Generally, the sense of self-location has been most closely linked to having the first-person visual perspective of the body (Blanke and Metzinger 2009), sense of agency to the synchronicity of sensorimotor signals (Farrer and Frith 2002), and body ownership to the synchrony of multisensory signals (Tsakiris 2010). However, several studies have found that giving participants a first-person perspective over a virtual body was sufficient to create a feeling of embodiment even without multisensory or visuomotor synchronisation (Carey et al. 2019; Galvan Debarba et al. 2017; Slater et al. 2010). The extent to which a first-person perspective is necessary for embodiment is much debated with some studies, suggesting that a first-person perspective is essential for the experience of embodiment (Petkova et al. 2011), while others have suggested that synchronous multisensory stimulation can induce a sense of embodiment even with a third-person perspective (Galvan Debarba et al. 2017), albeit not as strongly.
One aspect of bodily alignment that has been less explored is the role of postural match between real and virtual body in creating a sense of embodiment. Research using the rubber hand illusion has demonstrated that the sense of ownership over specific body parts is highly sensitive to their congruency with the participants actual body (Costantini and Haggard 2007; Tsakiris and Haggard 2005). To date, there has been comparatively little research into the effects of postural match in the full-body illusion. De la Peña et al. (2010) demonstrated that embodying a virtual avatar, which was viewed in a stress position, led participants to report negative affective responses even though the participants were not in the same position. In a follow-up study, Bergström et al. (2016) found that body ownership reports were lower when an avatar was viewed in a stress position compared to a comfortable position even though neither of these positions matched that of the participant’s real body. The authors also noted that ownership scores in both conditions were lower than in previous studies in which the posture of the participant and avatar matched although they could not directly compare matching and non-matching postures. In the current study, we aimed to manipulate postural alignment in order to change the level of identification with VM.
Documentary work has demonstrated that having a virtual body and feeling ownership over it helped the participant to engage with the content (de la Peña et al. 2010). As well as creating a feeling of “being there” known as presence, immersive virtual environments may also result in increased feelings of embodiment. Some argue that there are differences between perspective taking that can lead to empathy requiring use of cognitive resources and motivation as opposed to virtual embodied experiences (Van Loon et al. 2018). Several researchers have sought to investigate how factors like presence, embodiment and empathy modulate the process of engagement. Shin (2018) found evidence for a two-stage process in which initial levels of presence lead to an increase in both empathy and embodiment, and these factors then influence the participant’s feeling of engagement. Barbot and Kaufman (2020), on the other hand, have suggested a direct pathway between the experience of embodiment and changes in empathy when viewing immersive VR.
1.2 Virtual reality, identification and health outcomes
In the past two decades, VR has increasingly been deployed as a healthcare tool across a range of areas. In terms of training, VR has been used to train skills in practitioners including surgeons (Jin et al. 2021; Logishetty et al. 2019) and nurses (Chen et al. 2020), as a tool for simulating decision making during doctor–patient interactions (Fertleman et al. 2018) and as a means of increasing empathy and communication among practitioners (Buchman and Henderson 2019). VR has also been used in the treatment of patients in areas including physical (Elor and Kurniawan 2020; Howard 2017; Voinescu et al. 2021) and cognitive (Maggio et al. 2019) rehabilitation, pain relief (Matamala-Gomez et al. 2019) and in the treatment of mental health (Emmelkamp and Meyerbröker 2021). However, to date, there has been little interest in VR use as a medium for communicating public health messages.
The idea that creating a sense of presence and identification with the protagonist of a narrative might change behaviours has been of interest to researchers in public health messaging. Researchers across several disciplines have highlighted the power of narrative to immerse audiences within the situations they depict and argued that this process of transportation makes narratives a powerful persuasive tool (Dal Cin et al. 2004; Green and Brock 2000; Van Laer et al. 2014). This persuasive power of narrative transportation has been applied to a range of public health contexts including encouraging intentions towards: sun safe-behaviour (Jensen et al. 2017; Lillie et al. 2021); human papillomavirus vaccination for cervical cancer prevention (Frank et al. 2015; Krakow et al. 2017); attending mammograms (McQueen et al. 2011; McQueen and Kreuter 2010); and attending colonoscopies (Jensen et al. 2014).
A meta-analysis of 25 studies that investigated the persuasive effective of narratives in healthcare found a small but significant effect of narrative techniques (Shen et al. 2015). Of particular interest to the current study were the findings that narratives presented via audio–visual channels were more effective than those presented via text alone, a finding the authors attributed to the stronger emotional effect of these channels compared to text. It was also found that longer texts with more detailed information were more effective than shorter texts. Both these findings suggest that narratives delivered in a more immersive and engaging manner have a strong persuasive effect. In this context, the immersive nature of VR to drive engagement with issues around healthcare can be viewed as an extension of the narrative persuasion approach to a new technological platform.
1.3 Breast cancer and self-examination
The target of identification in the current study is VM a woman undergoing treatment for breast cancer. Breast cancer is the most common form of cancer in the UK, accounting for 15% of all new cancer cases (Cancer Research UK 2021). However, it also has a high survival rate with 75% of women being diagnosed with breast cancers surviving their disease for more than 10 years post-diagnosis. This is due to its high survival rate when detected early, a fact that highlights the potential benefits of breast cancer awareness and regular BSE. The importance of regular BSE is promoted through frequent prominent public health campaigns such as Breast cancer awareness month (Jacobsen and Jacobsen 2011) and the promotion of breast cancer awareness on social media (Vraga et al. 2018).
The effectiveness of BSE has been contested (Allen et al. 2010; Austoker 2003) with some research (Køsters and Gøtzsche 2008; Miller and Baines 2011), suggesting that BSE does not lead to greater survival rates. However, a recent meta-analysis suggested that increased uptake of BSE does lead to greater attendance for breast cancer screening (Anastasi and Lusher 2019). Therefore, willingness to conduct BSE may stand as a useful proxy for overall awareness of the risks of developing breast cancer.
1.4 Death-thought awareness and terror management theory
In addition to the direct effect of identifying with VM on BSE intention, we were also interested in understanding the cognitive mechanisms underlying this relationship. One possible mechanism that may be relevant is DTA. The significance of DTA in cognitive processing has been most thoroughly addressed by proponents of terror management theory (Pyszczynski et al. 2015; Rosenblatt et al. 1989) who have argued that awareness of our own mortality plays a significant role in a wide range of cognitive, affective and social processes. In brief, terror management theory argues that, as humans, we reduce the sense of threat generated by mortality awareness via anxiety buffering processes including: self-esteem; close attachments and cultural worldviews.
Given the crucial role that awareness of mortality plays in terror management theory proponents of the theory have developed multiple tasks aimed at measuring the extent to which a participant is focused on death-related thoughts. In their review of the literature, Hayes et al. (2010) identify several methodologies used to tap into DTA. One such measure is the use of a lexical decision task containing death- and non-death-related words. Participants have been found to respond faster to death-related words after reminders of mortality (Fritsche et al. 2008) and threats to their worldview (Schimel et al. 2007).
Several previous studies have sought to investigate how the insights of terror management theory might be applied to healthcare provision and public health messaging (e.g. Bozo et al. 2009; Goldenberg et al. 2008; Stevens 2009). Of particular interest to our study given the documentary’s focus on cancer treatment is research by Arndt et al. (2007). In a series of studies, the authors found that priming participants with cancer-related words led to increased DTA but only under conditions of high cognitive load or subliminal priming. They explained these results by drawing on previous research, suggesting that conscious awareness of mortality results in the effortful suppression of death-related thoughts, which was not possible when cognitive load was high or when the priming of cancer-related words occurred below conscious awareness (Arndt et al. 1997).
In addition to showing the effect of cancer primes on DTA, Arndt et al. (2007) also showed a link between DTA and intention to conduct BSE. In one experiment, participants who learned about cancer under low cognitive load (and so were better able to suppress DTA) were more likely to respond positively to questions around conducting a BSE compared to those who learned about cancer under high cognitive load who were unable to suppress thoughts linking cancer to death. In a separate experiment, the authors found a link between personal relevance and DTA with participants who viewed themselves as more at risk of cancer showing less DTA. The authors interpreted this as evidence that those participants were the most motivated to suppress DTA. This finding suggests that those who identify most with a cancer patient will be more likely to show decreased DTA.
1.5 Current study
The current study examined whether changing identification with a breast cancer patient through the manipulation of posture would lead to changes in both DTA and intention to conduct a BSE. To do this, we used The Waiting Room VR (Mapplebeck 2019: TWR) a 17-min-long 360° documentary film that describes filmmaker VM’s journey through her breast cancer diagnosis and subsequent treatment. In VM’s words: “TWR challenges the cultural myths that surround this disease, putting under the microscope the language of illness. TWR begins with a personal journey but as cancer affects one in two of us over the course of a lifetime, it also tells a very universal story” (Mapplebeck 2022).
TWR is constructed around a central 10-min ‘long take’ scene that reconstructs a session of radiotherapy. Throughout this scene, the camera (and thus the viewpoint of the audience in VR) is positioned within the radiotherapy machine slightly above the patient’s head, resulting in a perspective that is close to, but deliberately not wholly, first-person subjective. This ambiguous perspective was carefully designed by VM who wished her audience to feel “right by me” without feeling as if they were her, as a truly first-person subjective perspective might suggest, they were expected to be “in a position of having a chronic illness or a cancer diagnosis, with all of the fears and baggage that comes with that” (V. Mapplebeck, personal communication).
This ambiguity of viewpoint meant that the extent of alignment between VM and the viewer’s perspective in this central scene could be manipulated by altering the bodily posture of the viewer (see Fig. 1). When viewed in an upright position the viewer sees themselves as sitting next to VM while she is reclined; however, if the viewer is also reclined, then they see the scene from an angle much more consistent with VMs view creating a closer match to a first-person perspective. Therefore, we had our participants watch the film in either an upright or reclined position and measured the effects of that manipulation on participant’s sense of presence, identification with VM, BSE intention and DTA. In line with the findings of Arndt et al. (2007) regarding the importance of supressing DTA in promoting BSE intention, we also employed a manipulation of cognitive load in which high load was expected to prevent the suppression of death-related thoughts.

Example of participant view during radiotherapy sequence of The Waiting Room VR. This viewpoint was present for both conditions
1.6 Hypotheses
Based on the reviewed literature, we developed the following hypotheses:
-
H1.
Viewing TWR in the reclined position compared to the upright position will lead to a greater sense of presence within the scene.
-
H2.
Viewing TWR in the reclined position compared to the upright position will lead to greater explicit identification between the viewer and VM.
-
H3.
Greater identification with VM will lead to stronger intention to conduct BSE.
-
H4.
Viewing TWR in the reclined position under low cognitive load will lead to higher intention to conduct BSE compared to other conditions.
-
H5.
Greater identification with VM will lead to decreased DTA.
-
H6.
Viewing TWR in the reclined position under high cognitive load will lead to increased DTA compared to other conditions.
2 Method
2.1 Design
The experiment was a between-participants design with two independent variables viewing posture (upright vs. reclined) and cognitive load (high vs. low). The dependent variables were level of presence; level of identification with VM; intention to conduct BSE and DTA.
2.2 Participants
Eighty cisgender women between the ages of 18 and 40 (M = 21.65, SD = 5.07) gave their written informed consent to participate and were paid for their participation. See Supplementary Materials for details of how the COVID-19 pandemic affected participant recruitment. See Table 1 for the distribution of participants across conditions. Participants were pre-screened for personal history of breast cancer, epilepsy, brain injury and propensity to motion sickness before taking part in the study and had normal or corrected to normal vision. No participant had a previous diagnosis of breast cancer. Thirty participants (37.5%) had relatives and/or friends with a history of breast cancer. No participants had previously viewed TWR. Ethical approval for the study was given by the University of Bath’s Department of Psychology Research Ethics Committee. A sensitivity analysis suggested that our final sample of 80 participants had 80% power to detect an effect size of Cohen’s d 0.63 (a medium-to-large effect size) at an alpha of 0.05 for comparisons in our 2 × 2 design and 80% power to detect an effect size of Cohen’s d 0.2 (a small effect size) at an alpha of 0.05 for our regression analyses.
2.3 Apparatus and materials
2.3.1 360° video viewing setup
The study was conducted in laboratory spaces at the Department of Psychology, University of Bath and the Centre for Innovation, University of Bristol. Both locations were approximately the same size and used an identical hardware setup. Participants viewed TWR using an Oculus Go headset with a field of view of 100° nominal, a resolution of 1220 × 1440 pixels per eye and a refresh rate of 72 Hz. Audio was delivered via external over-ear headphones. The documentary was displayed using a custom-built 360° video player application that was created by the researchers using the Unity software development package (Unity Technologies 2019). Playback of 360° video content was facilitated using the in-built video player component provided by Unity and was rendered using the Skybox Panoramic Shader method detailed in Margerie (2018). This setup allowed participants to control their viewpoint in the 360° video by moving their heads in the pitch and yaw axes.
In the upright posture condition, participants viewed the film seated in a standard (non-rotating) desk chair with the back set at a 90° angle (see Fig. 2A). In the reclined posture condition, participants viewed the film lying in a medical examination chair that was similar in colour, size and configuration to the one Victoria was placed in within the scene, with their legs extended at 90° and the chair back reclined to 140° (see Fig. 2B). In both conditions, the viewport of the headset was adjusted with an offset of 15° of yaw applied to the headset gyroscope. This offset served to align VM’s legs within the scene as closely as possible with those of the participant. In addition, for each participant a calibration was performed using the headset’s built in re-centring function so that the initial title credits would be directly in front of the participant regardless of their actual physical posture. (In the reclined position, the participants' head was tilted back slightly, resting against the headrest.) This meant that the initial view was the same in each condition although anatomical constraints meant that looking directly down to see VMs head was much more effortful in the reclined position creating a greater sense of viewing the scene from VMs perspective.

Participant posture in the upright (A) and reclined (B) conditions
2.3.2 Questionnaire measures
We collected demographic information on participants’ age and gender. At the end of the experiment, participants indicated whether they had relatives or close friends with a history of breast cancer and whether they were a parent (since VM's relationship with her son is a key theme of the documentary). Only one participant was a parent, so this measure was not employed.
The presence was measured using the i-group presence questionnaire (Schubert et al. 2001) which contains subscales measuring spatial presence, involvement and experienced realism. Identification with VM was measured using two questionnaires. The Inclusion of Other in the Self scale (IOS; Aron et al. 1992) which asks participants to indicate their connectedness to the other person using the proximity of two circles and the State Empathy Questionnaire (SEQ; Shen 2010) which includes three dimensions within state empathy: affective, cognitive, and associative empathy.
Intention to conduct BSE was measured using a six-item questionnaire taken from Arndt et al. (2007). The items were rated on a nine-point Likert scale ranging from one (not at all true/not at all likely) to nine (very true/extremely likely).
To control for existing levels of trait empathy, participant’s completed the Toronto Empathy Questionnaire (Spreng et al. 2009), which represents trait empathy as a unidimensional emotional process.
Finally, to test the effectiveness of our load manipulation mental workload was measured using the NASA Task Load Index (Hart and Staveland 1988). This index used a 20-point scale to evaluate mental workload demand on the participant during the experiment with questions measuring mental demand, physical demand, temporal demand, performance, frustration and effort.
2.3.3 Lexical decision task
DTA was measured using a mortality version of the lexical decision task based on that used by Arndt et al. (2007). Participants were asked to categorise letter strings into words and nonwords by pressing letters on the keyboard (E for nonwords, I for words) as fast as possible. In each trial, a blank screen appeared for 500 ms followed by a ready screen showing “****” in the middle of the screen for a further 500 ms, after this the letter string was displayed for 1000 ms and then the ready screen was shown again until a response was entered. Participants could respond at any point after the letter string appeared. There were 4 categories of letter string: negative words, death-related words, neutral words and nonwords. Each of the word categories contained ten words, and there were 30 nonwords leading to a total of 60 trials. Participants completed a practice round containing three neutral word and three non-word trials.
2.4 Procedure
The full procedure is illustrated in Fig. 3. See Supplementary Materials for details of COVID-related protocols. At the start of the study, participants were randomly assigned to one of the four combinations of posture and cognitive load conditions before being briefed about the study and giving their informed consent. Participants next saw a 10-digit number for 30 s and had to memorise it as part of the cognitive load manipulation. They then completed the demographics questionnaire and the Toronto Empathy Questionnaire.

Experimental Procedure. The two-load probes, where participants were asked to repeat the memorised number were completed only for participants in the specified cognitive load condition (High or Low). TWR = The Waiting Room VR, LDT = lexical decision task, BSE = breast self-examination
Participants were then placed in the viewing posture (upright or reclined) of their assigned condition and fitted with the HMD and headphones before watching TWR. During viewing, the lights in the room were turned off, the curtains were drawn, and the experimenter left the room. At the end of the film, participants were invited to take a moment to readjust before the lights were turned back on. They then completed a distractor task of a wordsearch for five minutes. The distractor task was performed as the effects of mortality primes on DTA tend to be stronger when there is a delay between the mortality prime (in this case TWR) and the subsequent test. Once the five minutes had passed, participants completed the lexical decision task and the intention to conduct a BSE questionnaire. Following this, they were told that they did not need to remember it any longer. Finally, participants completed the remaining measures in the following order: NASA task load index, the IOS, the SEQ, the i-group presence questionnaire, and the questions regarding whether they had relatives or close friends with experience of breast cancer.
To manipulate cognitive load, we varied the point at which participants were probed to recall the 10-digit number, enter it to the computer and cease trying to recall the number. For participants in the low cognitive load condition, this recall probe occurred immediately before they viewed TWR. For participants in the high cognitive load condition, this recall probe occurred after they had seen TWR and completed the lexical decision task and BSE questionnaire (see Fig. 1).
Upon completion of the study tasks, participants were thoroughly debriefed and given a detailed sheet explaining the purpose of the experiment. The total duration of the study was between 45 min and one hour. No participants reported any experience of VR sickness during the task.
3 Results
3.1 Randomisation and manipulation checks
To check whether there were any differences between our four groups in terms of age or trait empathy, we ran a series of 2 × 2 ANOVAs comparing age and trait empathy across posture and cognitive load conditions. The ANOVA on participant age revealed no significant difference between posture. F(1,76) = 0.06, p = 0.802, ηp2 = 0.02, or cognitive load, F(1,76) = 1.18, p = 0.281, ηp2 < 0.01, conditions for age, and no significant interaction between them, F(1,76) = 0.45, p = 0.504, ηp2 < 0.01. The ANOVA on trait empathy revealed no significant difference between posture. F(1,76) = 0.18, p = 0.671, ηp2 < 0.01, or cognitive load, F(1,76) = 0.72, p = 0.400, ηp2 < 0.01, conditions for trait empathy, nor any significant interaction between them, F(1,76) = 0.18, p = 0.676, ηp2 < 0.01. To check whether there were differences between our groups on past experience of breast cancer among relatives and close friends, we ran a logistic regression as the data was binomial. We found no significant difference between posture, Χ2(1,N = 80) = 1.15, p = 0.284, OR = 0.77, or cognitive load, Χ2(1,N = 80) = 0.14, p = 0.710, OR = 0.91, conditions for past experience of breast cancer, and no interaction between them, Χ2(1,N = 80) = 1.35, p = 0.245, OR = 0.76. Thus, our groups did not differ significantly on any of these factors.
In addition, we also tested the success of our cognitive load manipulation by comparing scores on the NASA task load index measure of mental workload between our four conditions. A 2 × 2 ANOVA revealed no significant effect of posture. F(1,76) = 0.27, p = 0.608, ηp2 < 0.01, or cognitive load, F(1,76) = 0.12, p = 0.726, ηp2 < 0.01 on mental workload, and no significant interaction between them, F(1,76) = 0.25, p = 0.620, ηp2 < 0.01, suggesting that participants did not view the high-load conditions as involving more mental workload than the low-load conditions. See Table 2 for means and SDs of each variable by group.
3.2 H1. Relationship between viewing posture and presence
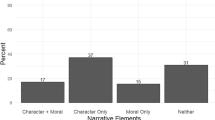
To investigate how our posture manipulation changed participants’ sense of presence within the virtual setting, we tested the effect of posture on the total of the i-group Presence Questionnaire as well as on each of the subscales (see Fig. 4, Table 3). For the total presence score, a Shapiro–Wilk test showed a significant departure from normality (W(80) = 0.97, p = 0.029). A nonparametric Wilcoxon–Mann–Whitney test revealed no significant difference between total presence scores in the upright and reclined posture conditions, U(Nupright = 40,Nreclined = 40) = 728, Z = -0.69, p = 0.488, r = 0.08.

Score on each iGroup Presence Questionnaire subscale in the upright and reclined position
For the spatial presence subscale, a Shapiro–Wilk test showed no significant departure from normality (W(80) = 0.99, p = 0.590). A Welch two-sample t-test revealed significantly lower scores in the upright compared to reclined condition, t(76.61) = − 2.25, p = 0.027, d = − 0.51. For the involvement subscale, a Shapiro–Wilk test showed a significant departure from normality (W(80) = 0.93, p < 0.001). A nonparametric Wilcoxon–Mann–Whitney test revealed no significant difference between total presence scores in the upright and reclined) posture conditions, U(Nupright = 40,Nreclined = 40) = 810, Z = 0.10, p = 0.923, r = 0.01. For the experienced realism subscale, a Shapiro–Wilk test showed no significant departure from normality (W(80) = 0.98, p = 0.451). A Welch two-sample t-test revealed no significant difference between scores in the upright and reclined conditions, t(75.45) = 0.14, p = 0.891, d = 0.03.
3.3 H2. Relationship between viewing posture and identification with VM
To investigate whether our posture manipulation affected identification with VM, we tested the effect of posture on the IOS scale as well as on the total of the SEQ and each of its subscales (see Table 4). For the IOS, a Shapiro–Wilk test showed a significant departure from normality (W(80) = 0.92, p < 0.001). A nonparametric Wilcoxon–Mann–Whitney test revealed no significant difference between total presence scores in the upright and reclined posture conditions, U(Nupright = 40,Nreclined = 40) = 797.5, Z = − 0.02, p = 0.980, r < 0.01.
For the total SEQ score, a Shapiro–Wilk test showed no significant departure from normality (W(80) = 0.98, p = 0.235). A Welch two-sample t-test revealed no significant difference between the upright (M = 31.73, SD = 7.68) and reclined (M = 33.55, SD = 6.62) conditions, t(76.32) = − 1.14, p = 0.259, d = − 0.26. For the affective subscale, a Shapiro–Wilk test showed a significant departure from normality (W(80) = 0.95, p = 0.004). A nonparametric Wilcoxon–Mann–Whitney test revealed no significant difference between total presence scores in the upright and reclined posture conditions, U(Nupright = 40,Nreclined = 40) = 748.5.5, Z = − 0.50, p = 0.618, r = 0.06. For the cognitive subscale, a Shapiro–Wilk test showed a significant departure from normality (W(80) = 0.94, p = 0.001). A nonparametric Wilcoxon–Mann–Whitney test revealed no significant difference between total presence scores in the upright and reclined posture conditions, U(Nupright = 40,Nreclined = 40) = 644.5, Z = − 1.51, p = 0.130, r = 0.17. For the associative subscale, a Shapiro–Wilk test showed no significant departure from normality (W(80) = 0.98, p = 0.090). A Welch two-sample t-test revealed no significant difference between the upright and reclined conditions, t(77.40) = − 0.89, p = 0.374, d = − 0.20.
3.4 H3. Relationship between identification with VM and intention to conduct breast self-examination
To investigate how far identification with VM predicted intention to conduct BSE, we fitted two linear models to predict BSE intention. The first with IOS as a predictor and the second with the three SEQ subscales as predictors. The IOS model explained a statistically significant proportion of variance, Adj. R2 = 0.07, F(1, 78) = 6.82, p = 0.011 (see Fig. 5). Within this model, the effect of IOS was statistically significant and positive, std. β = 0.28, t(78) = 2.61, p = 0.011. The SEQ model explained a statistically non-significant proportion of variance, adj. R2 < − 0.01, F(3, 76) = 0.81, p = 0.493, and none of the individual subscales were significant predictors.

Relationship between breast self-examination (BSE) intention and inclusion of the other in the self (IOS) rating
We further investigated the relationship between identification with VM and BSE intention by running two exploratory mediation analyses using the lavaan package’s bootstrapping method (Rosseel 2012) to determine whether this effect was mediated by other factors. The first of these tested the hypothesis that past experience of friends or family with breast cancer mediated the effect of identification on BSE intention. Results indicated that identification did not significantly predict past experience, B = 0.04, SE = 0.03, 95% CI [− 0.02,0.11], β = 0.14, p = 0.215, but that past experience was a significant predictor of BSE intention, B = 0.95, SE = 0.36, 95% CI [0.23,1.65], β = 0.26, p = 0.006. These results did not support a mediating effect of past experience. In addition, identification remained as a significant predictor of BSE intention after controlling for the mediator, past experience, B = 0.031, SE = 0.12, 95% CI [0.06,0.55], β = 0.28, p = 0.012, consistent with no mediation. Approximately 15% of the variance in BSE intention was accounted for by the predictors (R2 = 0.15). The indirect effect was tested using a percentile bootstrap estimation approach with 10,000 samples (Shrout and Bolger 2002). These results indicated the indirect coefficient was non-significant, B = 0.04, SE = 0.04, 95% CI [− 0.02,0.12], β = 0.04, p = 0.253, indicating that the effect of affiliation with VM on BSE intention was not significantly mediated by past experience of breast cancer.
We then tested whether the effect of IOS on BSE intention was mediated by total iGroup Presence score. Results indicated that identification did not significantly predict presence, B = 0.1.36, SE = 1.01, 95% CI [− 0.64,3.33], β = 0.17, p = 0.169, and that presence was not a significant predictor of BSE intention, B = − < 0.01, SE = 0.01, 95% CI [− 0.03,0.02], β = − 0.02, p = 0.850. These results did not support a mediating effect of presence. In addition, identification remained as a significant predictor of BSE intention after controlling for the mediator, presence, B = 0.32, SE = 0.13, 95% CI [0.06,0.56], β = 0.28, p = 0.012, consistent with no mediation. Approximately 8% of the variance in BSE intention was accounted for by the predictors (R2 = 0.08). The indirect effect was tested using a percentile bootstrap estimation approach with 10,000 samples. These results indicated the indirect coefficient was not significant, B = − < 0.01, SE = 0.02, 95% CI [− 0.04,0.05], β = − < 0.01, p = 0.848, indicating that the effect of affiliation with VM on BSE intention was not significantly mediated by presence.
3.5 H4. Relationship between posture, cognitive load and intention to conduct breast self-examination
To test whether posture and cognitive load modulated the intention to conduct BSE, we ran 2 × 2 ANOVA with BSE as the DV and posture and load as the IVs. Table 5 shows the mean and standard deviation (SD) for BSE scores in each condition. The ANOVA revealed no significant effect of posture. F(1,76) = 0.07, p = 0.794, ηp2 < 0.01, or cognitive load, F(1,76) = 0.14, p = 0.713, ηp2 < 0.01, and no significant interaction between them, F(1,76) = 0.05, p = 0.823, ηp2 < 0.01.
3.6 H5. Relationship between identification with VM and death thought awareness
To investigate how far identification with VM predicted DTA, we followed Arndt et al.’s (2007) approach and controlled for general RT by regressing out the neutral word RTs from death word RTs. We then fitted two linear models to the residualised death word RTs. The first with IOS as a predictor and the second with the three SEQ subscales as predictors. The IOS model was non-significant, adj. R2 = 0.02, F(1, 76) = 2.50, p = 0.118, and identification was not a significant predicator. Similarly, the SEQ model explained a statistically nonsignificant proportion of variance, adj. R2 = 0.03, F(3, 74) = 1.78, p = 0.159, and none of the individual subscales were significant predictors.
3.7 H6. Relationship between posture, cognitive load and death-thought awareness
To test whether posture and cognitive load modulated the DTA, we ran 2 × 2 × 2 ANOVA with residualised RTs after the RTs for neutral words had been regressed out as the DV and posture, cognitive load and word type as the IVs. Table 6 shows EMM and SE for the residualised RTs in each condition. The ANOVA revealed no significant effect of posture, F(1,74) = 0.39, p = 0.563, ηp2 = < 0.01, cognitive load, F(1,74) = 0.56., p = 0.456, ηp2 < 0.01, or word type, F(1,74) < 0.01, p = 0.967, ηp2 < 0.01. None of the interactions were significant (all F < 1).
4 Discussion
The current study aimed to examine how changes in postural matching between viewer and VM, the documentary subject acted to change levels of identification with VM. In addition, we investigated how identification with VM affected participant’s behavioural intentions to conducted BSE and their cognitive awareness of death-related topics. While we did not find a strong link between postural matching and identification with VM, we did find a link between having a matching posture to VM and increased spatial presence. More interestingly, we found that overall identification with VM led to an increased intention to conduct a BSE examination and showed, via mediation analysis, that this effect was independent of either the relationship between identification with VM and experience of breast cancer in one's own family and friends and the relationship between identification with VM and overall levels of presence. Below we discuss the implications of these results before moving on to highlight some of the study’s limitations and suggest future directions for research on VR in healthcare.
4.1 Identifying with a cancer patient predicts increased breast self-examination intention
The finding that the level of identification with VM predicted behavioural intentions to conduct BSE is consistent with previous studies, which have found that narrative identification with a patient can help to encourage positive health-related behaviour. For example, Frank et al. (2015) showed that identification with a character in a video who contracted HPV predicted talking to a doctor about taking an HPV vaccination 6 months after watching the video. In addition, Igartua et al. (2020) investigated the role of similarity to protagonist and narrative voice on encouraging smoking cessation via a narrative intervention and found that the effects of both on smoking cessation were mediated by increased identification with the protagonist.
We further examined the relationship between identification with VM and intention to conduct BSE by running two mediation analyses to see whether the effect was driven by either pre-existing experience of friends or relatives having breast cancer or by the amount of presence that participants experienced while watching the VR documentary. The first analysis found that while both past experience of breast cancer and identification with VM were significant positive predictors of intention to conduct a BSE these effects were independent of each other. This indicates that our finding was not driven simply by the fact that those participants with greater prior experience of breast cancer were more likely to intend to conduct self-examination and more likely to identify closely with VM. Our second mediation model found that overall rating of presence, as measured by the iGroup presence scale, was not a significant predictor of BSE intentions and did not mediate the relationship between identification with VM and intention to conduct BSE. This null result suggests a need to be cautious when attributing the effects of identification on BSE to the distinctly immersive nature of VR, something that is also highlighted by previous studies which have demonstrated similar effects using less immersive media forms such as traditional flat screen film (McQueen et al. 2011; Occa and Suggs 2016) or text (McQueen et al. 2019).
These analyses help to situate the current results within a wider theoretical framework. A number of researchers have suggested that narratives can help to persuade by subverting resistance to the suggested idea (Knowles and Linn 2004). One early piece of evidence in favour of this was the finding that individuals who reported high levels of transportation or absorption into the narrative of a story showed increased agreement with story-consistent statements and reduced critical appraisal of the story’s content (Green and Brock 2000). Slater and Rouner (2002) further developed this theory in their extended elaboration likelihood model (E-ELM), which added identification with specific characters as an additional narrative feature alongside overall transportation, and claimed that both transportation and identification worked via supressing counterarguing, one key form of resistance to persuasion. More recently, Moyer-Gusé (2008) has put forward the entertainment overcoming resistance model (EORM) which expanded on the previous theories by increasing the amount narrative features that might help to overcome resistance to include perceived similarity, parasocial interaction (i.e. the feeling of having a two-way social relationship with the “performer”) and enjoyment. EORM also widens the scope of resistance mechanisms beyond counterarguing to include mechanisms such as reluctance and selective avoidance.
Empirical support for these models can be seen in a recent meta-analysis (Ratcliff and Sun 2020), which surveyed nine experimental studies and 25 correlational studies to examine the evidence for the relationship between narrative and overcoming resistance. The study determined that narrative studies generated less resistance to persuasion than non-narrative studies and that the levels of resistance were negatively correlated with reported amounts of narrative engagement. More fine-grained analyses suggested that both transportation and identification were effective means of overcoming resistance.
When applying these theoretical considerations to the current study, we can roughly map transportation as being reflected in participants’ score on the iGroup presence questionnaire and identification as being reflected in scores on the IOS measure. On this basis, we can say that our study finds evidence for increased narrative persuasion operating via identification but no evidence for it operating via transportation. To go one step further, Cohen (2001) breaks down the concept of identification with a character into empathic (sharing the character’s feelings), cognitive (sharing the character’s perspective), motivational (internalising the character’s goals) and absorptive (loss of self other distinction) aspects. While our IOS measure does not distinguish between these, it is worth noting that neither affective nor cognitive measures of empathy towards VM affected BSE intention, suggesting that the motivational and absorptive aspects may have been more important in changing behaviour.
It is also worth noting that we did not directly measure other features picked out by the EORM including perceived similarity, defined as the degree to which the viewer believes they share traits, values or experiences with another character, or parasocial interaction, However, it might be argued that both of these would be increased by having had past experience of a family member with breast cancer which was shown to be an independent predictor of BSE intention but not to mediate the effect of identification on BSE intention.
4.2 No effect of posture, cognitive load or identification on death-thought awareness
In addition to the effects of viewing TWR on public health intentions, we also sought to examine whether it led to changes in participant’s level of DTA. Based on previous findings (Arndt et al. 2007), we were particularly interested in whether viewing under conditions of increased cognitive load, which would prevent the suppression of death-related thoughts, would lead to increased DTA and whether this would be modulated by the posture participants were in when viewing the documentary and by the extent to which participants identified with VM. Our analyses showed no significant effect of either cognitive load or posture on DTA and no significant interaction between them. Nor did we find any significant relationship between identification with VM and levels of DTA. One possible explanation for the lack of any effect of cognitive load on DTA is that our manipulation of load while modelled on that of Adrndt et al. was ineffective. Evidence for this possibility comes from the fact that the NASA task load index failed to find a significant difference between our two load conditions. It is possible that a more effective load manipulation would have done better in preventing suppression of death thoughts.
However, it is also worth noting the wider context in which our study was conducted. We commenced data collection for this study on 6 March 2020 the day on which the UK reported its first confirmed death from COVID-19. Data collection was then interrupted by the first UK-wide lockdown and was concluded in November 2020 as the UK entered its second lockdown with the total number of COVID deaths reaching over 50,000. Given this backdrop, it is possible that levels of DTA as well as measures to supress them were already at ceiling meaning that our content and the manipulations of posture and cognitive load were not strong enough to have a significant effect on DTA. Indeed, Fairlamb (2021) demonstrates a strong link between the daily number of COVID cases and deaths and DTA within a UK population, while other researchers have highlighted the relevance of terror management theory in the COVID pandemic (Courtney et al. 2020; Pyszczynski et al. 2021).
4.3 Changing participant posture affected spatial presence but not identification with VM
One of the key purposes of this study was to investigate whether increasing the postural congruency between the participant and VM by having the participant view TWR in a reclined position would lead to increase feelings of presence and identification with VM. Here we found evidence of some effect of posture on presence but only within the spatial presence subscale of the i-group questionnaire (Schubert et al. 2001); by contrast, we found no effect of posture on either the involvement or realism subscales. This divergent effect of postural congruency on the different presence subscales can be understood by considering the construct that each subscale seeks to measure. Schubert and colleagues defined the spatial presence subscale as capturing a spatial-conceptual facet of presence which relates directly to the possibility of embodied action within the virtual environment and relates most closely to the sense of bodily overlap targeted by our postural manipulation. By contrast, the involvement scale maps onto an attentional facet relating to the suppression of sensory information from the real world, which is incompatible with stimuli from the virtual environment, while the realism subscale relates to how realistic the virtual world seemed to participants. Neither of these concepts is directly related to the degree of overlap between one’s own body and the body presented to the participant within the virtual world.
It is more surprising, however, that the alignment of the participants posture and that of VM did not seem to lead to any increase in identification with VM as measured with the IOS. Here we note three possible reasons for this dissociation. The first is that our postural manipulation had a relatively minimal effect on the visual scene that participants perceived. By design, we adjusted the viewpoint of participants so that in both posture conditions the viewer saw the scene at roughly the angle originally intended by VM. This did not completely remove the effect of posture on viewpoint; for example, it was physically easier for participants to move their head to look directly down in the upright compared to reclining position. It did, however, reduce the visual effects of the postural change, which may well have reduced the distinctiveness of the two conditions for participants. This is particularly relevant when considering previous evidence for a greater weighting of visual as opposed to proprioceptive information (Burns et al. 2006; Carey et al. 2019).
A second, though related explanation for the lack of an effect of posture on identification relates to our use of 360° video in this study. While 360° video is both easier to create and presents a more and visually faithful experience than computer-generated environments (Crawford-Holland 2018), it lacks the sensorimotor congruency that comes with embodying an avatar in computer-generated VR (Bailey et al. 2016) and nor did we seek to induce embodiment via synchronous visuotactile stimulation (Lenggenhager et al. 2007). Rather we relied on postural matching alone to drive identification with VM which may have failed to produce a sufficiently increased sense of embodiment in the reclining condition to affect identification ratings or behaviour intentions. It is worth noting that other studies that employed either visuomotor (Neyret et al. 2020) or multisensory (Ventura et al. 2022) methods have found significant effects of embodiment on attitude. On the other hand, attitude changes have also been found in studies that have only manipulated the first-person perspective (Hasler et al. 2021), while a recent meta-analysis found that sense of embodiment was not a moderating factor in the power of VR to change attitudes (Nikolaou et al. 2022), suggesting that non-embodied immersive experiences such as 360° video still be affective in modulating viewers intentions. The third reason why posture failed to modulate levels of identification relates more to the affective and perspective taking aspects of identification than to the bodily aspect. In addition to the visual representation of the radiotherapy session in which participants experienced VM’s perspective, the documentary also includes approximately 7 min of non-POV scenes showing images relating to VMs clinical scans and containing multiple audio clips relating both VMs thought as well as recorded messages from both VMs family and medical professionals. This additional visual and audio content provided an alternative channel through which identification with VM could be established at a more cognitive-affective level and may have overwhelmed any effects of our, relatively subtle, postural manipulation on identification.
4.4 Limitations
Finally, we would like to note some limitations to our study. First, we would note that the current results cannot speak directly to the causal direction between the identification with VM and the change in BSE intentions. It is possible that greater awareness of the risks of breast cancer could both lead to increased identification with VM and a more positive inclination towards BSE. This possibility was raised by the fact that having a friend or relative who had experienced breast cancer was directly correlated with higher BSE intentions. The fact that our mediation analysis showed no mediating effect on past experience of breast cancer on the relationship between identification and BSE intention makes this possibility less likely. Nonetheless, further research in this area should examine how factors such as the perceived threat of cancer to the individual (Arndt et al. 2007) might act as mediators in the path between identification and healthcare intentions.
A second limitation of the current study relates to our choice of stimuli, the 360° video The Waiting Room VR. As mentioned in the methods section, this video’s key scene involved an ambiguous perspective in which the viewer’s POV was next to, but not directly aligned with, that of VM. Although being in the reclined position increased the similarity between the posture of the participant and VM neither condition led to a full alignment with the virtual body. In addition, as mentioned above, the additional non-embodied scenes in the piece may also have led to increased identification with VM regardless of postural alignment. Future research could use a “purer” experimental setting, which would make the contrast between the posture of a virtual avatar and participant more obvious. This purer setting would also remove any additional factors encouraging identification allowing for the testing of how postural matching alone affected identification and its effects on health messaging.
A third limitation of the study is that since all conditions involved the use of a head-mounted display with head movement control of the camera position, it is not possible to state that the use of VR-based 360 video is necessarily more effective for public health messaging than showing the same video using a more traditional 2D screen. It may be that identification with VM would at similar levels and lead to similar effects on BSE intentions even in a less immersive format.
The final important limitation of the current study is that the mechanism by which identification leads to change in behavioural intentions was not specifically identified. Further research in this area could examine whether identification in VR targets the possible routes to persuasion suggested by theories like the EORM (Moyer-Gusé 2008) including reducing counterarguing and selective avoidance, increasing perceived vulnerability and changing outcome expectancies.
5 Conclusion
In conclusion, the current study investigated how manipulating postural alignment with a cancer patient within a 360 degree VR documentary affected identification, healthcare intentions and DTA. While our manipulation of posture did not modulate the level of identification, we did find a significant relationship between identification with the patient and healthcare intentions, suggesting that 360° video has the potential to be a useful tool in promoting positive health behaviours in the public.
References
Allen TL, Van Groningen BJ, Barksdale DJ, McCarthy R (2010) The breast self-examination controversy: what providers and patients should know. J Nurse Pract 6(6):444–451. https://doi.org/10.1016/j.nurpra.2009.11.005
Anastasi N, Lusher J (2019) The impact of breast cancer awareness interventions on breast screening uptake among women in the United Kingdom: a systematic review. J Health Psychol 24(1):113–124. https://doi.org/10.1177/1359105317697812
Arndt J, Greenberg J, Pyszczynski T, Solomon S, Simon L (1997) Suppression, accessibility of death-related thoughts, and cultural worldview defense: exploring the psychodynamics of terror management. J Pers Soc Psychol 73(1):5–18. https://doi.org/10.1037/0022-3514.73.1.5
Arndt J, Cook A, Goldenberg JL, Cox CR (2007) Cancer and the threat of death: the cognitive dynamics of death-thought suppression and its impact on behavioral health intentions. J Pers Soc Psychol 92(1):12–29. https://doi.org/10.1037/0022-3514.92.1.12
Aron A, Aron EN, Smollan D (1992) Inclusion of other in the self scale and the structure of interpersonal closeness. J Pers Soc Psychol 63(4):596–612
Austoker J (2003) Breast self examination. BMJ 326(7379):1–2. https://doi.org/10.1136/bmj.326.7379.1
Bailey JO, Bailenson JN, Casasanto D (2016) When does virtual embodiment change our minds? Presence 25(3):222–233. https://doi.org/10.1162/PRES
Barbot B, Kaufman JC (2020) What makes immersive virtual reality the ultimate empathy machine? Discerning the underlying mechanisms of change. Comput Hum Behav 111(May):106431. https://doi.org/10.1016/j.chb.2020.106431
Bergström I, Kilteni K, Slater M (2016) First-person perspective virtual body posture influences stress: a virtual reality body ownership study. PLoS ONE 11(2):e0148060. https://doi.org/10.1371/journal.pone.0148060
Bertrand P, Guegan J, Robieux L, McCall CA, Zenasni F (2018) Learning empathy through virtual reality: multiple strategies for training empathy-related abilities using body ownership illusions in embodied virtual reality. Front Robot AI 5(26):1–18. https://doi.org/10.3389/frobt.2018.00026
Bevan C, Green DP, Farmer H, Rose M, Cater K, Stanton Fraser D, Brown H (2019) Behind the curtain of the “ultimate empathy machine”: On the composition of virtual reality nonfiction experiences. In: Brewster S, Fitzpatrick G, Cox A, Kostakos V (eds) Proceedings of the 2019 CHI conference on human factors in computing systems. ACM Press, pp 1–12. https://doi.org/10.1145/3290605.3300736
Blanke O, Metzinger TK (2009) Full-body illusions and minimal phenomenal selfhood. Trends Cogn Sci 13(1):7–13. https://doi.org/10.1016/j.tics.2008.10.003
Bozo Ö, Tunca A, Simsek Y (2009) The effect of death anxiety and age on health-promoting behaviors: a terror-management theory perspective. J Psychol 143(4):377–389. https://doi.org/10.3200/JRLP.143.4.377-389
Buchman S, Henderson D (2019) Interprofessional empathy and communication competency development in healthcare professions’ curriculum through immersive virtual reality experiences. J Interprof Educ Pract 15(December 2018):127–130. https://doi.org/10.1016/j.xjep.2019.03.010
Burns E, Razzaque S, Panter AT, Whitton MC, McCallus MR, Brooks FP (2006) The hand is more easily fooled than the eye: users are more sensitive to visual interpenetration than to visual-proprioceptive discrepancy. Presence Teleoper Virtual Environ 15(1):1–15. https://doi.org/10.1162/pres.2006.15.1.1
Cancer Research UK (2021) Breast cancer statistics. https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer
Carey M, Crucianelli L, Preston C, Fotopoulou A (2019) The effect of visual capture towards subjective embodiment within the full body illusion. Sci Rep 9(1):1–12. https://doi.org/10.1038/s41598-019-39168-4
Chen FQ, Leng YF, Ge JF, Wang DW, Li C, Chen B, Sun ZL (2020) Effectiveness of virtual reality in nursing education: Meta-analysis. J Med Internet Res 22(9):1–13. https://doi.org/10.2196/18290
Cohen J (2001) Defining identification: a theoretical look at the identification of audiences with media characters. Mass Commun Soc 4(3):245–264. https://doi.org/10.1207/S15327825MCS0403_01
Costantini M, Haggard P (2007) The rubber hand illusion: sensitivity and reference frame for body ownership. Conscious Cogn 16(2):229–240. https://doi.org/10.1016/j.concog.2007.01.001
Courtney EP, Goldenberg JL, Boyd P (2020) The contagion of mortality: a terror management health model for pandemics. Br J Soc Psychol 59(3):607–617. https://doi.org/10.1111/bjso.12392
Crawford-Holland S (2018) Humanitarian VR documentary and its cinematic myths. Synoptique 7(1):19–31
Dal Cin S, Zanna MP, Fong GT (2004) Narrative persuasion and overcoming resistance. In: Knowles ES, Linn JA (eds) Resistance and Persuasion. Lawrence Erlbaum Associates, Mahwah, pp 175–191
de la Peña N, Weil P, Llobera J, Giannopoulos E, Pomés A, Spanlang B, Friedman D, Sanchez-Vives MV, Slater M (2010) Immersive journalism: immersive virtual reality for the first-person experience of news. Presence 19(4):291–301. https://doi.org/10.1162/PRES_a_00005
de Margerie T (2018) How to integrate 360 video with unity. https://blogs.unity3d.com/2017/07/27/how-to-integrate-360-video-with-unity/?_ga=2.159851645.1308616920.1543498780-421605029.1517835635#
Elor A, Kurniawan S (2020) The ultimate display for physical rehabilitation: a bridging review on immersive virtual reality. Front Virtual Real 1(November 2020):1–17. https://doi.org/10.3389/frvir.2020.585993
Emmelkamp PMG, Meyerbröker K (2021) Virtual reality therapy in mental health. Annu Rev Clin Psychol 17:495–519. https://doi.org/10.1146/annurev-clinpsy-081219-115923
Fairlamb S (2021) The relationship between COVID-19-induced death thoughts and depression during a national lockdown. J Health Psychol. https://doi.org/10.1177/13591053211067102
Farmer H, Maister L (2017) Putting ourselves in another’s skin: using the plasticity of self-perception to enhance empathy and decrease prejudice. Soc Justice Res 30(4):323–354. https://doi.org/10.1007/s11211-017-0294-1
Farrer C, Frith CD (2002) Experiencing oneself vs another person as being the cause of an action: the neural correlates of the experience of agency. Neuroimage 15(3):596–603. https://doi.org/10.1006/nimg.2001.1009
Fertleman C, Aubugeau-Williams P, Sher C, Lim AN, Lumley S, Delacroix S, Pan X (2018) A discussion of virtual reality as a new tool for training healthcare professionals. Front Public Health 6(FEB):1–5. https://doi.org/10.3389/fpubh.2018.00044
Frank LB, Murphy ST, Chatterjee JS, Moran MB, Baezconde-Garbanati L (2015) Telling stories, saving lives: creating narrative health messages. Health Commun 30(2):154–163. https://doi.org/10.1080/10410236.2014.974126
Fritsche I, Jonas E, Fankhänel T (2008) The role of control motivation in mortality salience effects on ingroup support and defense. J Pers Soc Psychol 95(3):524–541. https://doi.org/10.1037/a0012666
Galvan Debarba H, Bovet S, Salomon R, Blanke O, Herbelin B, Boulic R (2017) Characterizing first and third person viewpoints and their alternation for embodied interaction in virtual reality. PLoS ONE 12(12):1–19. https://doi.org/10.1371/journal.pone.0190109
Goldenberg JL, Arndt J, Hart J, Routledge C (2008) Uncovering an existential barrier to breast self-exam behavior. J Exp Soc Psychol 44(2):260–274. https://doi.org/10.1016/j.jesp.2007.05.002
Green MC, Brock TC (2000) The role of transportation in the persuasiveness of public narratives. J Pers Soc Psychol 79(5):701–721. https://doi.org/10.1037/0022-3514.79.5.701
Hart SG, Staveland LE (1988) Development of NASA-TLX (Task Load Index): results of empirical and theoretical research. Adv Psychol 52(C):139–183. https://doi.org/10.1016/S0166-4115(08)62386-9
Hasler BS, Landau HD, Hasson Y, Schori-Eyal N, Giron J, Levy J, Halperin E, Friedman D (2021) Virtual reality-based conflict resolution: the impact of immersive 360° video on changing view points and moral judgment in the context of violent intergroup conflict. New Media Soc 23(8):2255–2278. https://doi.org/10.1177/1461444821993133
Hayes J, Schimel J, Arndt J, Faucher EH (2010) A theoretical and empirical review of the death-thought accessibility concept in terror management research. Psychol Bull 136(5):699–739. https://doi.org/10.1037/a0020524
Howard MC (2017) A meta-analysis and systematic literature review of virtual reality rehabilitation programs. Comput Hum Behav 70:317–327. https://doi.org/10.1016/j.chb.2017.01.013
Igartua J-J, Rodríguez-Contreras L, Marcos-Ramos M, González-de-Garay B, Frutos FJ (2020) Smoking prevention with narrative messages. An experimental study on the joint effect of audience- character similarity and narrative voice. Adicciones 33(3):245. https://doi.org/10.20882/adicciones.1339
Jacobsen GD, Jacobsen KH (2011) Health awareness campaigns and diagnosis rates: evidence from National Breast Cancer Awareness Month. J Health Econ 30(1):55–61. https://doi.org/10.1016/j.jhealeco.2010.11.005
Jensen JD, King AJ, Carcioppolo N, Krakow M, Samadder NJ, Morgan S (2014) Comparing tailored and narrative worksite interventions at increasing colonoscopy adherence in adults 50–75: a randomized controlled trial. Soc Sci Med 104:31–40. https://doi.org/10.1016/j.socscimed.2013.12.003
Jensen JD, Yale RN, Krakow M, John KK, King AJ (2017) Theorizing foreshadowed death narratives: examining the impact of character death on narrative processing and skin self-exam intentions. J Health Commun 22(1):84–93. https://doi.org/10.1080/10810730.2016.1252816
Jin C, Dai L, Wang T (2021) The application of virtual reality in the training of laparoscopic surgery: a systematic review and meta-analysis. Int J Surg 87(299):105859. https://doi.org/10.1016/j.ijsu.2020.11.022
Kilteni K, Groten R, Slater M (2012) The sense of embodiment in virtual reality. Presence Teleoper Virtual Environ 21(4):373–387. https://doi.org/10.1162/PRES_a_00124
Knowles ES, Linn JA (2004) The importance of resistance to persuasion. In: Knowles ES, Linn JA (eds) Resistance and Persuasion. Lawrence Erlbaum Associates, Mahwah, pp 3–10
Køsters JP, Gøtzsche PC (2008) Regular self-examination or clinical examination for early detection of breast cancer. Int J Epidemiol 37(6):1217–1218. https://doi.org/10.1093/ije/dyn218
Krakow M, Yale RN, Torres DP, Christy K, Jensen JD (2017) Death narratives and cervical cancer: impact of character death on narrative processing and HPV vaccination. Health Psychol 36(12):1173–1180. https://doi.org/10.1037/hea0000498.supp
Lenggenhager B, Tadi T, Metzinger TK, Blanke O (2007) Video ergo sum: manipulating bodily self-consciousness. Science 317(5841):1096–1099. https://doi.org/10.1126/science.1143439
Lillie HM, Pokharel M, John KK, Christy KR, Upshaw S, Giorgi EA, Jensen JD (2021) Does it matter if a story character lives or dies? A message experiment comparing survivor and death narratives. Psychol Health. https://doi.org/10.1080/08870446.2021.1873337
Logishetty K, Rudran B, Cobb JP (2019) Virtual reality training improves trainee performance in total hip arthroplasty: a randomized controlled trial. Bone Jt J 101-B(12):1585–1592. https://doi.org/10.1302/0301-620X.101B12.BJJ-2019-0643.R1
Maggio MG, Latella D, Maresca G, Sciarrone F, Manuli A, Naro A, De Luca R, Calabrò RS (2019) Virtual reality and cognitive rehabilitation in people with stroke: an overview. J Neurosci Nurs 51(2):101–105. https://doi.org/10.1097/JNN.0000000000000423
Mapplebeck V (2019) The waiting room VR. East City Films, Shoreditch
Mapplebeck V (2022) The waiting room VR. https://victoriamapplebeck.com/immersive/the-waiting-room-vr/
Matamala-Gomez M, Donegan T, Bottiroli S, Sandrini G, Sanchez-Vives MV, Tassorelli C (2019) Immersive virtual reality and virtual embodiment for pain relief. Front Hum Neurosci 13(August):1–12. https://doi.org/10.3389/fnhum.2019.00279
McQueen A, Kreuter MW (2010) Women’s cognitive and affective reactions to breast cancer survivor stories: a structural equation analysis. Patient Educ Couns 81S:S15–S21. https://doi.org/10.1016/j.pec.2010.08.015
McQueen A, Kreuter MW, Kalesan B, Alcaraz KI (2011) Understanding narrative effects: the impact of breast cancer survivor stories on message processing, attitudes, and beliefs among African American women. Health Psychol 30(6):674–682. https://doi.org/10.1037/a0025395
McQueen A, Caburnay C, Kreuter MW, Sefko J (2019) Improving adherence to colorectal cancer screening: a randomized intervention to compare screener vs. survivor narratives. J Health Commun 24(2):141–155. https://doi.org/10.1080/10810730.2019.1587109
Miller AB, Baines CJ (2011) The role of clinical breast examination and breast self-examination. Prev Med 53(3):118–120. https://doi.org/10.1016/j.ypmed.2011.05.001
Moyer-Gusé E (2008) Toward a theory of entertainment persuasion: explaining the persuasive effects of entertainment-education messages. Commun Theory 18(3):407–425. https://doi.org/10.1111/j.1468-2885.2008.00328.x
Neyret S, Navarro X, Beacco A, Oliva R, Bourdin P, Valenzuela J, Barberia I, Slater M (2020) An embodied perspective as a victim of sexual harassment in virtual reality reduces action conformity in a later milgram obedience scenario. Sci Rep 10(1):1–18. https://doi.org/10.1038/s41598-020-62932-w
Nikolaou A, Schwabe A, Boomgaarden H (2022) Changing social attitudes with virtual reality: a systematic review and meta-analysis. Ann Int Commun Assoc 46(1):30–61. https://doi.org/10.1080/23808985.2022.2064324
Occa A, Suggs LS (2016) Communicating breast cancer screening with young women: an experimental test of didactic and narrative messages using video and infographics. J Health Commun 21(1):1–11. https://doi.org/10.1080/10810730.2015.1018611
Petkova VI, Khoshnevis M, Ehrsson HH (2011) The perspective matters! Multisensory integration in ego-centric reference frames determines full-body ownership. Front Psychol 2:35. https://doi.org/10.3389/fpsyg.2011.00035
Pyszczynski T, Solomon S, Greenberg J (2015) Thirty years of terror management theory: from genesis to revelation. In: Advances in experimental social psychology, 1st edn, vol 52. Elsevier Inc. https://doi.org/10.1016/bs.aesp.2015.03.001
Pyszczynski T, Lockett M, Greenberg J, Solomon S (2021) Terror management theory and the COVID-19 pandemic. J Humanist Psychol 61(2):173–189. https://doi.org/10.1177/0022167820959488
Ratcliff CL, Sun Y (2020) Overcoming resistance through narratives: findings from a meta-analytic review. Hum Commun Res 46(4):412–443. https://doi.org/10.1093/hcr/hqz017
Rosenblatt A, Greenberg J, Solomon S, Pyszczynski T, Lyon D (1989) Evidence for terror management theory: I. The effects of mortality salience on reactions to those who violate or uphold cultural values. J Pers Soc Psychol 57(4):681–690. https://doi.org/10.1037/0022-3514.57.4.681
Rosseel Y (2012) lavaan: an R package for structural equation modeling. J Stat Softw 48(2):1–93. https://doi.org/10.18637/jss.v048.i02
Schimel J, Hayes J, Williams T, Jahrig J (2007) Is death really the worm at the core? Converging evidence that worldview threat increases death-thought accessibility. J Pers Soc Psychol 92(5):789–803. https://doi.org/10.1037/0022-3514.92.5.789
Schubert TW, Friedmann F, Regenbrecht H (2001) The experience of presence: factor analytic insights. Presence Teleoper Virtual Environ 10(3):266–281. https://doi.org/10.1162/105474601300343603
Shen L (2010) On a scale of state empathy during message processing. West J Commun 74(5):504–524. https://doi.org/10.1080/10570314.2010.512278
Shen F, Sheer VC, Li R (2015) Impact of narratives on persuasion in health communication: a meta-analysis. J Advert 44(2):105–113. https://doi.org/10.1080/00913367.2015.1018467
Shin D (2018) Empathy and embodied experience in virtual environment: to what extent can virtual reality stimulate empathy and embodied experience? Comput Hum Behav 78:64–73. https://doi.org/10.1016/j.chb.2017.09.012
Shrout PE, Bolger N (2002) Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods 7(4):422–445. https://doi.org/10.1037/1082-989X.7.4.422
Slater MD, Rouner D (2002) Entertainment-education and elaboration likelihood: understanding the processing of narrative persuasion. Commun Theory 12(2):173–191. https://doi.org/10.1111/j.1468-2885.2002.tb00265.x
Slater M, Spanlang B, Sanchez-Vives MV, Blanke O (2010) First person experience of body transfer in virtual reality. PLoS ONE 5(5):e10564. https://doi.org/10.1371/journal.pone.0010564
Spreng RN, McKinnon MC, Mar RA, Levine B (2009) The Toronto empathy questionnaire: scale development and initial validation of a factor-analytic solution to multiple empathy measures. J Pers Assess 91(1):62–71. https://doi.org/10.1080/00223890802484381
Stevens E (2009) Extending knowledge of terror management theory to improve palliative nursing care. Int J Palliat Nurs 15(8):368–370. https://doi.org/10.12968/ijpn.2009.15.8.43793
Tsakiris M (2010) My body in the brain: a neurocognitive model of body-ownership. Neuropsychologia 48(3):703–712. https://doi.org/10.1016/j.neuropsychologia.2009.09.034
Tsakiris M, Haggard P (2005) The rubber hand illusion revisited: visuotactile integration and self-attribution. J Exp Psychol Hum Percept Perform 31(1):80–91. https://doi.org/10.1037/0096-1523.31.1.80
Unity Technologies (2019) Unity software development package (2019.4.29f1)
Van Laer T, De Ruyter K, Visconti LM, Wetzels M (2014) The extended transportation-imagery model: a meta-analysis of the antecedents and consequences of consumers’ narrative transportation. J Consum Res 40(5):797–817. https://doi.org/10.1086/673383
Van Loon A, Bailenson JN, Zaki J, Bostick J, Willer R (2018) Virtual reality perspective-taking increases cognitive empathy for specific others. PLoS ONE. https://doi.org/10.1371/journal.pone.0202442
Ventura S, Badenes-Ribera L, Herrero R, Cebolla A, Galiana L, Banõs R (2020) Virtual reality as a medium to elicit empathy: a meta-analysis. Cyberpsychol Behav Soc Netw 23(10):667–676. https://doi.org/10.1089/cyber.2019.0681
Ventura S, Miragall M, Cardenas G, Baños RM (2022) Predictors of the sense of embodiment of a female victim of sexual harassment in a male sample through 360-degree video-based virtual reality. Front Hum Neurosci 16(May):1–10. https://doi.org/10.3389/fnhum.2022.845508
Voinescu A, Sui J, Stanton Fraser D (2021) Virtual reality in neurorehabilitation: an umbrella review of meta-analyses. J Clin Med. https://doi.org/10.3390/jcm10071478
Vraga EK, Stefanidis A, Lamprianidis G, Croitoru A, Crooks AT, Delamater PL, Pfoser D, Radzikowski JR, Jacobsen KH (2018) Cancer and social media: a comparison of traffic about breast cancer, prostate cancer, and other reproductive cancers on Twitter and Instagram. J Health Commun 23(2):181–189. https://doi.org/10.1080/10810730.2017.1421730
Acknowledgements
This work was supported by the EPSRC Virtual Realities—Immersive Documentary Encounters project (EP/P025595/1). We would also like to thank: Dr Victoria Mapplebeck and the production team of “The Waiting Room VR” for proivding us with access to the documentary; Professor Mandy Rose and Dr David Green for their comments during the study design; and Dr Anca Salagean for her assitance in figure production.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
Cite this article
Farmer, H., Skoulikari, E., Bevan, C. et al. Using narrative 360° video as a tool to promote breast self-examination. Virtual Reality 28, 34 (2024). https://doi.org/10.1007/s10055-023-00918-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10055-023-00918-5