
Abstract
Previous studies showed similar spatial orientation ability (SO) between real world (RW) and virtual reality (VR). As the SO deteriorates with age, it is crucial to investigate whether the degradation is similar in VR, as it may affect the use of VR tools for older people, such as in physical therapy. Therefore, we extended our previous study, in which similar SO between RW and VR was measured for younger participants (18–35 years) with a higher age group (> 55 years) to examine the VR's influence on their SO. Two main tests were conducted. In the first test, the participants were blindfolded, asked to rotate (0°, 45°, 180°, 225°) on a fixed starting position, and walk straight to different objects they had memorized before. This test was conducted twice. An ANOVA only revealed a significant interaction between the factors Age (young/old) and Condition (VR/RW) for the 45°-rotation in the second run. Here, both age groups performed similarly in RW, while in VR, greater deviations in the older participants appeared. Nevertheless, the overall Age*Condition-interaction in the first test was not significant. In the second test, subjects were required to walk blindfolded to two objects starting from different positions. The starting position and objects changed three times in each condition but were equal between RW and VR. No interactions between the factors Age and Condition were found (p > 0.05). Both tests showed a similar influence of VR on the SO of both age groups, supporting the usage of VR, regardless of age.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Extended realities (XR) are used in many different fields, like architecture and construction (Alizadehsalehi et al. 2020), education (Alnagrat et al. 2022), and medicine (Morimoto et al. 2022). The term includes virtual reality (VR), augmented reality (AR) and mixed reality (MR). AR refers to a real environment in which virtual objects are included. In VR, a completely new environment is presented where the real world (RW) is completely shut out (Alizadehsalehi and Yitmen 2023). MR refers to everything that is in between VR and AR. Especially VR is becoming more common in society and has resulted in numerous research studies to evaluate the effectiveness of VR for various tasks. The applications with their advantages are already used for older people (> 55 years, in the following called Seniors). For example, VR training can lead to higher motivation and is adaptable to the capabilities of Seniors (Vries et al. 2018). In a systematic review, Tuena et al. (2020) summarized possible application fields of VR for Seniors, for example, the rehabilitation of sensorimotor, physical and psychological deficits. They concluded that VR usage for Seniors is beneficial. Still, full-immersive devices like head-mounted displays (HMDs) should be considered more often since, mostly, non-immersive devices (e.g. desktop VR) are used (Tuena et al. 2020). However, the literature concerning the usage of HMDs for Seniors is contradictory. While Plechatá et al. (2019) noticed a perceptional overload of Seniors in HMD-VR, Huygelier et al. (2019) observed great acceptance of this technology. Furthermore, Petri et al. (2020) stated that cybersickness, characterized by physical discomfort in VR, appears to be more common and severe in Seniors. In particular, after more than 10 min in VR, Seniors (> 60 years) are more affected by cybersickness than younger people (18–35 years, in the following called Juniors) (Petri et al. 2020).
Based on the results of past research, the question of whether humans perform similarly in VR and RW still needs to be determined for tasks requiring spatial judgments. Similar performance in both environments is a prerequisite for utilizing the benefits of VR. Otherwise, a transfer of the VR behavior into RW, which is considered to be the main goal of VR training (Gray 2017), may be limited. Previous research has already compared different aspects between VR and RW for Juniors (Bhagavathula et al. 2018; Pastel et al. 2020a, c). For example, in distance estimation, similar results in both environments were found using the HTC Vive Pro Eye (Pastel et al. 2020c), the HTC Vive Pro (Solini et al. 2021) and the HTC Vive (Kelly et al. 2017). In contrast, Bhagavathula et al. (2018) observed discrepancies in the speed estimation of moving objects while using the HTC Vive, as the speed of cars was estimated higher in VR than in RW.
In almost every sport, the spatial orientation ability (SO) is a performance-determining factor (Stoyanova et al. 2016). For this reason, SO seems to be an essential aspect that needs to be similar in both environments to enable a transfer of VR behavior into RW. In a review, Wolbers and Hegarty (2010) describe the SO as a multisensory ability involving perceptional and basic memory-related processes. The perceived information must be processed in relation to space and time. The study by Castillo Escamilla et al. (2020), in which participants with a better working memory made fewer mistakes in an orientation test, supports the assumption of a relationship between the (visual) memory and the SO. Furthermore, Wolbers and Hegarty (2010) mention two reference systems that can be used for SO: the allocentric and egocentric system. In the allocentric system, positions are memorized relative to external objects, while in the egocentric system, the position is memorized relative to one's position (Byrne and Crawford 2010; Klatzky 1998; Wolbers and Wiener 2014). According to Battaglia-Mayer et al. (2003), positions are often memorized in both systems.
The SO has already been compared between VR and RW for Juniors (Kimura et al. 2017; Pastel et al. 2021; Rodrigues et al. 2010). The literature divides the SO into small-scale and large-scale orientations. Small-scale orientation describes the orientation in a room where everything is visible from one point, and large-scale orientation refers to the orientation in a larger environment that extends beyond the visible area (Regian et al. 1992). In this paper, we use the term small-scale orientation when the perception of the own body in space and the position relative to specific objects is crucial, and large-scale orientation when navigation or wayfinding tasks are performed. In large-scale orientation, Rodrigues et al. (2010) found better performance in the RW than in VR by counting the errors participants made when reproducing a route they had memorized before. Furthermore, Waller et al. (1998) showed a good way to train the SO in VR in a maze. In small-scale orientation, Kimura et al. (2017) observed similar SO between VR and RW but found differences in how the results were achieved. The authors showed that in VR, the participants' SO relied more on the position of objects than on the geometry of the room, as the geometry is more difficult to encode in VR than in RW. Pastel et al. (2021) examined the SO to static objects in VR and RW. The participants had to memorize the position of objects in a room and later orientate themselves to these objects while being blindfolded. The authors report no differences between the two environments.
Previous research has shown that the SO of Seniors is generally reduced compared to the SO of Juniors (Newman and Kaszniak 2000). Due to lower technological affinity, this difference may be even larger in VR. Therefore, to use VR for Seniors, it is crucial to know whether the difference in SO between Juniors and Seniors in VR is comparable to the difference in RW. Research has been conducted comparing SO in RW and VR for Juniors and Seniors. In a large-scale setting, Cushman et al. (2008) examined the navigation skills in a hospital using a desktop to present the virtual scene. Overall, the Seniors performed worse than the Juniors, and the orientation in RW was better than in VR. However, no interaction between age and environment occurred, suggesting a similar influence of VR in the SO of Juniors and Seniors. Taillade et al. (2015) and Wiener et al. (2020) reached a similar conclusion for a wayfinding test in a city, while Head and Isom (2010) and Moffat and Resnick (2002) concluded this for virtual mazes. All of these studies only used desktop VRs (Cushman et al. 2008; Head and Isom 2010; Moffat and Resnick 2002; Wiener et al. 2020) or semi-immersive VRs (Taillade et al. 2015), where immersion is reduced compared to an HMD (Mujber et al. 2004). There is a lack of studies examining the SO in small-scale settings with Juniors and Seniors in RW and VR. Kalová et al. (2005) observed similar SO in RW and VR for Seniors but did not compare their results with a Junior group. In contrast, Merhav and Wolbers (2019) examined the SO of Juniors and Seniors in VR using an HMD but did not include an RW task for comparison. The Seniors' SO in VR was worse than the Juniors' when relying on the allocentric reference system and similar when only the egocentric or both systems were available.
Overall, there is a lack of studies examining the small-scale SO in VR and RW for Juniors and Seniors. As the SO is essential in sports, it should be similar between VR and RW for all age groups to enable the transfer of VR behavior into RW. Therefore, our primary goal is to clarify whether VR affects the SO of Seniors in the same way as Juniors, which would support the usage of VR in sports and physical therapy regardless of the participant's age. For this purpose, we extended our previous study (Pastel et al. 2021) with a senior group and compared the data with these of the existing junior group. The study consisted of two main tasks. In the first task, the participants memorized the position of objects from a fixed starting position and were blindfolded after 15 s. Then they had to rotate toward the memorized object and walk toward it while still being blindfolded. For the second task, the participants memorized the position of four objects while walking around in the testing area for 2 min. Afterward, they returned to the starting position, were blindfolded, and were led to a new position (called perspective) in the testing area. The experimenter named two of the four memorized objects to which the participants had to walk blindfolded in the given order, starting from the new perspective. We expect that the difference in the SO between Juniors and Seniors remains the same in RW and VR since various studies have already shown similarities in SO in VR and RW for both age groups separately. Furthermore, similarities between the conditions were observed in SO tests concerning wayfinding and navigational tasks, which consider a different part of SO than in small-scale settings. In our study, similar SO differences between the two age groups in VR and RW would be indicated by non-significant interactions between the age groups and testing environments. As it is state-of-the-art and suggested by Tuena et al. (2020), an HMD is used to present the VR. Furthermore, we conducted memory tests to examine the influence of working memory on SO for the two age groups, like in our previous study (Pastel et al. 2021). In addition, to check whether one group is more affected by cybersickness, we used the already established Simulator Sickness Questionnaire (SSQ, Kennedy et al. 1993).
2 Methods
2.1 Participants
40 healthy participants with normal or corrected vision participated in this study. The participants were divided into a group of Juniors (12 females and 8 males, age: 23.1 ± 3.3 years, already analyzed in Pastel et al. (2021)) and Seniors (13 females and 7 males, age: 67.5 ± 6.5 years). The statistical power, considering the used statistical method (ANOVA: Repeated measures, within-between interaction), expected effect (η2p = 0.06) and α-error probability (0.05), was acceptable (1 − β = 0.87 (error probability)), G*Power, version 3.1.9.7). The exclusion criteria consisted of cognitive impairments, balance problems and physical limitations (e.g. injuries, need for a walker). Furthermore, the participants in the Junior group had to be between 18 and 35 years, and those in the Senior group had to be older than 55 years. All participants were informed about the general procedure of the experiment and signed a letter of agreement. The approval of the Ethics Committee of the Otto-von-Guericke University at the Medical Faculty and University Hospital Magdeburg was obtained under the number 132/16. 10 Juniors and 4 Seniors stated to have prior experience with VR, mainly due to participation in other VR studies. No participant spent more than a total of 2 h in a VR or owned a device. Only 1 Junior and 2 Seniors stated that they had slight problems orienting themselves in unfamiliar surroundings. The distribution of sex (χ2(1) = 0.120, p = 0.729) and stated orientation problems (χ2(1) = 0.364, p = 1.000) was equal between the two groups, while the distribution of the VR experience (χ2(1) = 4.208, p = 0.040) differed.
2.2 Design
The participants completed the same orientation tasks in both conditions, VR and RW, in which they were instructed to walk to different static objects. The condition which was tested first was randomized and counterbalanced throughout the participants. First, the rotation ability was tested in four tasks. Rotations with different degrees (0°, 45°, 180°, 225°) were conducted blindfolded. These tasks were called Rotation Tasks (RTs) and only enabled the egocentric reference system for orientation. Here, the aim was to examine the ability to rotate in an unfamiliar environment. Afterward, three Pathway Tasks (PTs) were conducted, for which the participants had to walk blindfolded to two different previously memorized objects. Here, the egocentric and allocentric reference system could be used for orientation and free movement under more complex conditions was examined. The individual pathways from the starting position to the objects were equal in both conditions. Only the order of the pathways changed to reduce a possible learning effect. The four RTs from the beginning were repeated after the PTs to investigate the occurrence of a learning effect. The order of the RTs did not change.
Memory tests were conducted before the tests in VR and RW started. One test was to memorize and reproduce ten words from a list, and the second was an orientation test from the BIS-4 (Berliner-intelligence-structure test), in the following called OT-BIS-4. After the whole experiment, the participants were again asked to reproduce the ten words memorized in the beginning. The design is shown in Fig. 1.

Overview of the study design. Half of the participants started in VR (top), whereas the other half started in RW (bottom)
2.3 Experimental apparatuses and setup
A detailed description of the used apparatuses and their setup is provided by Pastel et al. (2021). The VR was presented using an HMD, the HTC Vive Pro Eye (HTC, Taiwan; resolution 2880 × 1600 pixels, horizontal field of view 110 degrees). A Vicon setup (Vicon, United Kingdom) with 13 infrared cameras was used to capture the motion of the participants. They were equipped with 6 reflective markers, one on the sternum, one on each center of the scapula, one on the shoulder, one on the elbow and one on the hand. The participants could decide which arm the markers should be placed on.
The VR was a replica of the RW and was built using Blender (version 2.8). It was imported into Unity3D (version 2019.1) and, with SteamVR (version 2.5), transferred to the HMD. The motion data were captured and processed with Vicon Nexus (version 2.4). The processed data were imported into a MATLAB script (version R2019a) to determine the point at which the participant expected to have reached the target object. From this point, the deviation between the participant's hand marker and the target object was computed. For data analysis, SPSS Statistics (version 26) was used (α = 0.05).
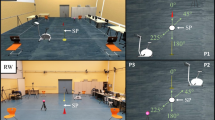
The testing area (7.5 m × 5.5 m) was defined using four chairs and ropes between them. Four sport-specific objects were placed inside this area: an ergometer, a bar, a pylon and a ball. These objects were in fixed positions. In the different environments, the position of the ergometer and the ball, as well as the bar and the pylon, were switched to reduce a learning effect. The starting position, where all RTs and PTs began, was the center of the four objects. Three different perspectives were chosen, P1, P2, and P3, whose function is described later. The setup can be seen in Fig. 2.

Experimental setup in VR (top) and RW (bottom) in side view (left) and bird's eye view (right), modified from Pastel et al. (2021). In the middle of the objects is the starting position (SP), and in three corners of the room are different perspectives (P1, P2, P3). The function of the perspectives is described in 2.4
2.4 Procedure
After arriving, the participants were informed about the study's aim, signed a letter of agreement and completed a self-designed questionnaire about their SO and previous VR experience. Afterward, two memory tests followed. First, the participants had one minute to memorize 10 random words from a given list. Then the list was taken away, and the OT-BIS-4 was performed, in which marked buildings on a map had to be memorized for 90 s and then marked on an empty map. When the OT-BIS-4 was finished, the participants had to reproduce the 10 words they had memorized before. The numbers of correctly marked buildings and correctly reproduced words were recorded. Afterward, the participants were ready to start with the RTs and PTs. Pastel et al. (2021) provide a detailed description of the tasks. For the participants starting in VR, a 3 min acclimatization phase was completed first. Here, the participant could walk around in the room freely before the RTs started. For these, the participants remained on the starting position and were asked to memorize the position of one of the four objects for 15 s. They were only allowed to turn around on the starting position while memorizing. After 15 s, they were told to turn toward the object on the 0°-position (see Fig. 2) and were blindfolded. Then, the participants were asked to rotate until they thought they would face the target object, walk straight to this object, and hold their hand over the expected position. After completing a task, they were returned to the starting position, and the blindfold was removed. Afterward, a new 15 s memorizing phase began. There were four RTs requiring rotations with the angles of 0° (no rotation), 45°, 180° and 225°, and walking distances between 2.1 and 3.1 m. The order of the RTs was always the same, starting with the 0°-rotation followed by the 45°-, 180°- and 225°-rotation. This was done to increase the difficulty level with each task. When the RTs were completed, the PTs followed. Here, the participants had a 2 min observation phase, during which they were free to move around in the testing area while memorizing the objects' positions. Then, they returned to the starting position, and the vision was covered while the participants faced the object standing at the 0°-position. Afterward, they were taken to a new unknown perspective in the room (P1, P2 or P3) and asked to orientate to two of the previously memorized objects memorized before in a specific order. After the participants finished where they expected the second object, they were returned to the starting position and the blindfold was removed. A new trial with a 2 min observation phase began. Three PTs were performed from different perspectives and with different target objects. When the PTs were completed, the RTs were repeated. The order of the perspectives in the two conditions and the target objects can be seen in Table 1.
When a task (RT and PT) was finished, the participants were asked to estimate the difficulty of this task by stating a number between 1 ("very easy") and 10 ("very difficult"). In the RTs and PTs, the 2D distance (height did not matter) between the participant's hand and the object and the task's completion time were recorded. For the PTs, there were two deviations: to the first and the second object. To obtain one value for each PT, additionally, the mean of both deviations was calculated.
After the RTs and PTs in the first condition, there was a break of approximately 5 min. The test in the remaining condition followed. When the tasks in VR were finished, the participants completed the SSQ to evaluate their cybersickness. When the tests were conducted in both conditions, the participants had to recall the 10 words they had learned at the beginning. The experiment lasted 75–90 min, of which the participants spent 11 min in VR.
2.5 Data analysis
For the RTs, the deviation between hand and object, the time for completion and the estimation of difficulty was analyzed using mixed ANOVAs with repeated measures with the within-factors Condition (RW and VR), Rotation (0°, 45°, 180° and 225°) and Run (1st run and 2nd run) and the between-subject factor Age (Juniors and Seniors). For the deviation and the time for completion, 4 participants deviated strongly from the average (determined by using Boxplots), 2 in the Junior and 2 in the Senior group. Also, in the estimation of difficulty of the RTs, one participant in the Junior group had incomplete data. Therefore, we excluded the data of these participants from the analysis. The PTs were analyzed with mixed ANOVAs with repeated measures as well, with the within-subject factors Condition (VR and RW) and Perspective (trial from P1, P2 and P3) and the between-subject factor Age (Juniors and Seniors). Here, a separate test for the deviation to the first object, the second object, the mean of these two deviations, the time for completion and the estimation of difficulty was calculated. For the deviation to the first object and the time for completion, one participant of the Juniors deviated strongly from the average and was removed from the data. In the estimation of difficulty data, the results of one participant in the Juniors are missing. For the results of the ANOVAs, only the main effects of the factors Age and Condition and the interactions involving these two factors are interpreted.
As the starting condition was alternated and counterbalanced, a possible influence of the order of the two tasks was checked. There was no significant difference between the values of the condition that was tested first compared to the second condition for all tasks and variables and both age groups (p > 0.05).
For the mixed ANOVAs, the requirements were checked. In terms of violated sphericity, the Greenhouse–Geisser-correction was used. No normal distribution was accepted due to previous research stating that ANOVAs are robust against this violation (Blanca et al. 2017). Further outliers are marked in the results. For interactions, η2p (η2p = 0.01, small effect, η2p = 0.06 moderate effect, η2p = 0.14 large effect), and for main effects, Cohen's d (d = 0.2, small effect, d = 0.5 moderate effect, d = 0.8 large effect) are used as effect size (Cohen 1988).
The three memory tests (10 words test before the orientation test, OT-BIS-4, 10 words test after the orientation test) were analyzed with t-tests for independent samples to examine the difference between the Junior and Senior group. In case of violated variance homogeneity, Welch-tests are calculated instead. Again, Cohen's d is used as effect size. Furthermore, correlation coefficients (Pearson's r; r = 0.1 weak correlation, r = 0.3 moderate correlation, r = 0.5 strong correlation) (Cohen 1988) between the three memory tests' results and the PTs' deviations were calculated separately for each age group.
The scores of the SSQ are calculated as described in Kennedy et al. (1993). The means of each age group are compared with the classification of Stanney et al. (1997). Furthermore, the scores are compared between Juniors and Seniors using a t-test and Cohen's d as effect size.
3 Results
Figure 3 shows an overview of the RTs' and PTs' Condition x Age-interactions for the deviations, the time for completion and the estimation of difficulty. The different rotation degrees and perspectives are merged. None of these diagrams show a significant interaction between the factors Condition and Age.

Overview of the interaction of the factors Condition x Age for the different tasks. In the first row are the results of the Rotation Tasks, and in the second, those of the Pathway Tasks. The 'Deviation' means the deviation between the participant's hand and the target object, the 'Time for Completion' the time the participants needed to orientate to the objects and the 'Estimation of Difficulty' the estimated difficulty the participants verbally stated after each task as points (1 point equals "very easy", 10 points "very difficult"). As indicated by the approximately parallel lines, none of these interactions were significant (p > 0.05)
3.1 Deviation
3.1.1 Rotation task
The means and standard deviations and the significant results for the deviation in the RTs are shown in Table 2. The results are considered separately for the 1st and 2nd run, as there is a significant difference between the hand-object deviation for the two runs of the Seniors, who performed better in the 2nd run (p = 0.009). For the Juniors, no significant difference between the runs occurred (p > 0.05). The deviations of the 1st run revealed no significant interactions or differences concerning the factors Condition and Age (p > 0.05). For the 2nd run, there is a significant interaction between the factors Condition x Rotation x Age. Further analysis with a two-way mixed ANOVA with the factors Condition x Age for each rotation degree showed interactions of these factors for the 45°rotation. Here, none of the groups significantly differed in their deviations between RW and VR. Furthermore, both age groups reached similar deviations in RW, but Seniors performed worse in VR than Juniors. Significant main effects occurred in the 0°-rotation (factor Age), where Juniors reached smaller deviations than the Seniors and in the 225°-rotation (factor Condition), where the results in VR were better than in RW. For the 180°-rotation no significant differences or interactions occurred (p > 0.05).
3.1.2 Pathway tasks
The means and standard deviations and the significant results for the deviation in the PTs are shown in Table 3. The participants always orientated to the correct objects and made no memory mistakes. For the deviation to the first object in the PTs, there were significantly smaller values in VR (168.1 ± 47.6 cm) than in RW (197.9 ± 61.8 cm). Furthermore, the Seniors reached smaller deviations (169.1 ± 39.2) than the Juniors (197.6 ± 34.1 cm). Regarding the deviation to the second object, no significant main effect or interaction with the factors Age and Condition occurred (p > 0.05). For the mean of both deviations, the Seniors reached smaller deviations (179.7 ± 39.5 cm) than the Juniors (212.5 ± 37.9 cm).
3.1.3 Time for completion
Table 4 shows the means and standard deviations of the participants' completion time for the RTs and PTs. As there is only one significant result in the PTs, only this is shown in the table.
3.1.4 Rotation task
For the time for completion in the RTs, there is no significant difference between the two runs for both age groups. Therefore, the results are merged. There is no significant main effect or interaction concerning the factors Condition and Age (p > 0.05, see Table 4).
3.1.5 Pathway tasks
The ANOVA for the completion time in the PTs only revealed a significant main effect of the factor Age. Overall, the Juniors completed the tasks faster (32.3 ± 8.0 s) than the Seniors (39.5 ± 11.6 s) (see Table 4).
3.2 Estimation of difficulty
The estimation of difficulty in the RTs significantly differed between the two runs for the Juniors (p = 0.001), who rated the tasks as more difficult in the 1st run. No significant differences occurred for the Seniors (p > 0.05). Nevertheless, the results are separated into 1st and 2nd run. In the 1st run, there are significant main effects for the factor Condition, as the tasks were estimated as easier in RW (2.4 ± 1.2) than in VR (2.8 ± 1.5), and the factor Age, as the Juniors (3.0 ± 1.3) estimated the tasks as more difficult than the Seniors (2.2 ± 1.1). No significant interactions or main effects occurred for the 2nd run (p > 0.05).
For the PTs' estimation of difficulty, there is neither a significant main effect nor a significant interaction between the factors Condition and Age (p > 0.05).
3.2.1 Memory tests
The t-tests showed significantly better performance of the Juniors for all memory tests. In the 10 words test before the orientation tests, the Juniors remembered 9.0 ± 1.1 words and the Seniors 6.0 ± 2.2 words (t(27.595) = 5.477, p < 0.001, d = 1.777, large effect, Welch-test is used). The Juniors marked 14.7 ± 3.5 correct buildings in the OT-BIS-4 and the Seniors 10.0 ± 3.6 (t(38) = 4.187, p < 0.001, d = 1.358, large effect). In the 10 words test after the orientation tests, the Juniors remembered 8.7 ± 2.3 words and the Seniors 5.2 ± 2.5 words (t(28.183) = 5.588, p < 0.001, d = 1.813, large effect, Welch-test is used).
For the Juniors and Seniors, no correlations between the memory tests and the deviations from the PTs that significantly differ from zero could be found (p > 0.05).
3.2.2 Simulator sickness
The SSQ scores ranged from "minimal symptoms" to "problem simulator" according to the classification of Stanney et al. (1997). Nevertheless, no participant complained about any problems concerning cybersickness.
The comparisons of the subscores and the Total Score between the two age groups revealed no significant differences (p > 0.05).
4 Discussion
In the present study, we examined the SO of Juniors and Seniors in VR and RW. The participants were asked to walk blindfolded to different static objects they had memorized before. For all tasks, the deviation between the participant's hand and the target object and the needed completion time were measured as SO indicators. Two tasks with different demands were conducted. In the RTs, the estimation of the own body rotation and the distance estimation to the objects were crucial. In the PTs, the memory of the objects' positions and their orientation to each other were decisive. We examined whether VR influences Juniors and Seniors equally, which would be noticeable by non-significant interactions between the factors Condition and Age. Furthermore, the included memory tasks were used to analyze a possible connection between the memory and the results of the PTs. In addition, the SSQ was used to compare the cybersickness between the two age groups.
For the RTs, the results for the deviations were considered separately for each run since the Seniors performed significantly better in the second run. That can be explained by the low number of Seniors having previous VR experience mentioned above. We assume that they needed more time to acclimate to VR or to explore the room, which was the case in the 2nd run due to the observation phases in PTs before. This is in line with the study by Solini et al. (2021), in which a predecessor model of our HMD was used, and the distance estimation was better after participants interacted with the virtual environment. However, in our study, only the Seniors benefited from interacting with the environments. An explanation could be that the tasks were already too simple for the Juniors in the first run. Surprisingly, no significant interactions or main effects occurred regarding the deviations in the first run. The main effect of the factor Age almost reached the significance level for the 1st run (p = 0.059), showing a tendency for the Juniors to achieve better results than the Seniors. In the 2nd run, the Juniors performed significantly better than the Seniors in the 0°- rotation. No significant effect of the Condition occurred. Here, mainly the distance estimation during blind walking (distance to object 2.5 m) was needed, as no rotation was required. Therefore, our results are consistent with previous work (Kelly et al. 2017; Pastel et al. 2020c; Solini et al. 2021), which used the same or previous models of our HMD, where the distance estimation did not differ between VR and RW. However, only Juniors were tested in these studies. For Seniors, the distance estimation in VR is not examined but seems more difficult according to the 0°-rotation's results in the 2nd run, even after interacting with the VR. Overall in the RTs, there is only a significant interaction between the factors Condition and Age for the deviations in the 45°-rotation of the 2nd run. More detailed analyses showed difficulties for Seniors for this rotation in VR as they performed worse than the Juniors. The significant interaction could again be explained by a problematic egocentric distance estimation of the Seniors. In the two following rotations (180° and 225°), smaller distances between the starting position and the objects existed and no significant interactions with the factors Age and Condition occurred. There was only a significant main effect for the factor Condition in the 225°-rotation showing smaller deviations in VR than in RW. Besides this, the results in RW and VR were similar, so we assume that the ability to estimate rotations does not differ between RW and VR for Juniors and Seniors. A more detailed analysis of the rotated angle of the participants would be insightful, as, in our task, the distance estimation had a large influence on a task that was intended to measure the rotation. When the rotation degrees are merged, no significant interaction of the factors Condition and Age occurred for the deviations and completion time, indicating a similar influence of VR on the SO of Juniors and Seniors.
There are significant main effects of the factors Condition and Age in the PTs for the deviation to the first object. Surprisingly, the deviations were smaller in VR than in RW and the Seniors showed smaller deviations than the Juniors. Considering the high standard deviations, it seems that the difficulty of orientating toward different objects with closed eyes results in a high scattering of the measured values, leading to surprising results. Nevertheless, they indicate that VR does not influence the SO for both age groups. For the deviation to the second object and the mean of both deviations, the results are similar for VR and RW. That is in line with a route recall test by Pastel et al. (2020c), where the result was quite similar between VR and RW except in the middle part of the route. Here, it is almost the same, as there is no difference between the deviations to the second object (the end of the route in this study) but the deviations to the first object (the middle part in this study). Nevertheless, in Pastel et al. (2020c), the results in RW were better in the middle part than in VR and vice versa compared to our study. Just as with the deviations to the first object, the mean of both deviations was smaller for the Seniors than for the Juniors. Regarding the PTs' completion time, there is only a significant main effect for the factor Age, as the Juniors performed faster than the Seniors. That is not surprising, as, for example, the gait velocity decreases with rising age and the Seniors probably already needed more time to walk to the objects (Patterson et al. 2012). In total, no significant interaction between the factors Age and Condition occurred, neither for the deviations nor the completion time, indicating a similar influence of VR on the SO of Juniors and Seniors.
Overall, in our tests, there were hardly any interactions between the factors Condition and Age for the deviations between hand and target objects or the tasks' completion times, leading to the assumption that VR influences the small-scale SO of Juniors and Seniors similarly. This is in line with previous large-scale work (Cushman et al. 2008; Taillade et al. 2015), but in contrast to our findings, their results were better for the Juniors than the Seniors and better for RW than VR. The different results may have occurred because desktop VR was used in these studies instead of HMDs. Further studies show better SO of Juniors in VR compared to Seniors in a large-scale setting (Head and Isom 2010; McAvan et al. 2021; Moffat and Resnick 2002; Wiener et al. 2020). Merhav and Wolbers (2019) differentiated between the two reference systems for their small-scale orientation test. When only the allocentric system was used, they found a superior performance of the Juniors but no differences when the egocentric system or a combination of both was used. In our study in the RTs, only the egocentric system and in PTs, both reference systems could be used. Therefore, Merhav and Wolbers' (2019) results are consistent with ours, as Juniors and Seniors reached similar results in the RTs with minor exceptions. According to McIntyre et al. (1998), egocentric information, stored in short-term memory, decays in the dark. In our study, the short-term memory was better for the Juniors, as they were able to reproduce more of the memorized words before the SO tasks. The superior memory of the Juniors can explain their slightly better results in the RTs, as their egocentric information could have decayed more slowly than that of the Seniors. Furthermore, the improved results of the Seniors in the 2nd run compared to the 1st run could have occurred because they had more allocentric information due to the observation phases in the PTs. Therefore, although the egocentric information may have decayed, it was possible to rely on allocentric information. The same applies to the PTs. In large-scale studies, Moffat and Resnick (2002) observed a better SO of Juniors when the allocentric vision was used, while Rodgers et al. (2012) showed that Seniors were more likely to choose the egocentric system for SO. That is in contrast to our work, where the Seniors partly even reached better results than the Juniors, presumably by using the allocentric system for SO. McAvan et al. (2021) found similar SO impairments of Juniors and Seniors due to allocentric cues in VR in a large-scale study, which is also observed in our study regarding the 2nd object's deviation in the PTs. They hypothesized that the different results occurred due to the use of HMDs instead of desktop VRs, which were used in many studies mentioned above. Furthermore, our results align with a small-scale study by Kalová et al. (2005), who tested the SO of Seniors in a desktop VR and found similar results between both conditions.
Concerning the estimation of difficulty, the participants rated the RTs in VR as more difficult in the 1st run. There were no significant interactions or main effects in the 2nd run of the RTs or the PTs. We assume that VR was initially rated as more difficult because most participants had no prior contact with VR. The fact that the PTs were estimated as equally difficult may result from exploring the virtual environment in the observation phases. That would also explain the similarity in the 2nd run of the RTs, which were right after the PTs. The results of the estimation of difficulty align with Pastel et al. (2020c) and Pastel et al. (2020b) but only for the 1st run of the RTs, where tasks in VR were also rated as more difficult.
The Juniors reached better results in the memory tasks. That is not surprising, as memory declines with age (Luo and Craik 2008). However, there were no significant correlations between the results of the PTs and the memory tests. Several studies showed a connection between these two factors (Castillo Escamilla et al. 2020; Mitolo et al. 2015), contrasting our work. So, either the memory test examined a different aspect of memory, or the RTs and PTs did not require a high performance since too few objects had to be remembered to challenge the memory. In our study, there were four objects. Except for 3 Seniors, each participant was able to recall at least 4 words from the 10 words, which tested their short-term memory.
Regarding cybersickness, the SSQ showed high scores, although no participants verbally stated any major problems. According to the categorization of Stanney et al. (1997), the symptoms ranged from "minimal symptoms" to "problem simulator". The authors stated that SSQ scores for VR simulators might be higher due to a different symptomatic situation and the fact that it was initially designed for the military. Saredakis et al. (2020) support this assumption and suggest that the general population is expected to have higher values. Therefore, the high SSQ scores should not influence the interpretation of our results. Nevertheless, the comparison between the two age groups revealed no significant differences in the SSQ scores. Petri et al. (2020) also observed similar cybersickness between Juniors and Seniors. They reported hardly any differences in cybersickness for Juniors and Seniors in the first 10 min in VR. In our study, the participants spent a total of 11 min in VR, but this was divided into several smaller experiences.
4.1 Limitations
The study contains some limitations that have to be noticed. First of all, the test did not consider conditions that can be found in sports. That might not be essential for seniors in physical therapy, but in sports, there are more complex situations, including moving objects and time pressure. Therefore, the transfer of the results into a sport setting is limited. Second, only sporty and motivated participants were examined, which could have influenced the results. Third, more participants would improve the statistical power of the study and could enable the examination of a possible impact of gender, previous VR experience and self-estimation of the SO. Fourth, in the RTs, the distance estimation greatly influenced the result. The rotated angle may have been more insightful as we wanted to measure the rotation ability. Furthermore, the order of the RTs and PTs was fixed, which could have led to order effects. The objects in the RTs and PTs were only switched between the conditions but were equal for all participants. Randomization of these objects would have been insightful to reduce possible order effects. Moreover, in our study, the participants' body was not visualized in VR, which might improve the feeling of presence.
4.2 Practical implications
Under consideration of the limitations, the study supports the usage of VR for older people. As the SO is a crucial factor in sports and everyday life, training scenarios can be built to conserve or improve Seniors' abilities and skills. Moreover, it provides the basis for further examinations concerning the usage of modern HMD-VR for Seniors.
5 Conclusion and future research
The two conducted orientation tests showed that the difference in the SO performance between the younger and older age group is similar in RW and VR regarding the deviation to the objects and the task's completion time. The similar difference indicates that VR influenced the SO of younger participants like it influenced older participants. In general, the SO was very similar in VR and RW for both age groups. Therefore, we conclude that the usage of modern HMD-VR is possible concerning the SO, regardless of age. Especially, tasks that require motion toward and interaction with static objects are feasible and can be used in VR applications for Seniors. Nevertheless, older people seem to need more acclimatization time in VR compared to younger adults.
The current tests examined the SO in VR and RW with static objects and without time pressure. To ensure the same conditions between VR and RW in sports, more realistic tests of the SO, for example with moving objects, should be conducted. The orientation with open eyes would also be an interesting aspect of future work. Furthermore, it should be examined whether Seniors can train their SO in VR with a transfer into RW. Moreover, other abilities, like balance ability, can be examined for older people to further support the usage of VR for Seniors.
Data availability
Yes.
Code availability
Yes.
References
Alizadehsalehi S, Yitmen I (2023) Digital twin-based progress monitoring management model through reality capture to extended reality technologies (DRX). SASBE 12:200–236. https://doi.org/10.1108/SASBE-01-2021-0016
Alizadehsalehi S, Hadavi A, Huang JC (2020) From BIM to extended reality in AEC industry. Autom Constr 116:103254. https://doi.org/10.1016/j.autcon.2020.103254
Alnagrat A, Che Ismail R, Syed Idrus SZ, Abdulhafith Alfaqi RM (2022) A review of extended reality (XR) technologies in the future of human education: current trend and future opportunity. HumEnTech 1:81–96. https://doi.org/10.11113/humentech.v1n2.27
Battaglia-Mayer A, Caminiti R, Lacquaniti F, Zago M (2003) Multiple levels of representation of reaching in the parieto-frontal network. Cereb Cortex 13:1009–1022. https://doi.org/10.1093/cercor/13.10.1009
Bhagavathula R, Williams B, Owens J, Gibbons R (2018) The reality of virtual reality: a comparison of pedestrian behavior in real and virtual environments. Proceed Human Fact Ergon Soci Annual Meet 62:2056–2060. https://doi.org/10.1177/1541931218621464
Blanca MJ, Alarcón R, Arnau J, Bono R, Bendayan R (2017) Non-normal data: is ANOVA still a valid option? Psicothema 29:552–557. https://doi.org/10.7334/psicothema2016.383
Byrne PA, Crawford JD (2010) Cue reliability and a landmark stability heuristic determine relative weighting between egocentric and allocentric visual information in memory-guided reach. J Neurophysiol 103:3054–3069. https://doi.org/10.1152/jn.01008.2009
Castillo Escamilla J, Fernández Castro JJ, Baliyan S, Ortells-Pareja JJ, Ortells Rodríguez JJ, Cimadevilla JM (2020) Allocentric spatial memory performance in a virtual reality-based task is conditioned by visuospatial working memory capacity. Brain Sci. https://doi.org/10.3390/brainsci10080552
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Erlbaum, Hillsdale, NJ
Cushman LA, Stein K, Duffy CJ (2008) Detecting navigational deficits in cognitive aging and Alzheimer disease using virtual reality. Neurology 71:888–895. https://doi.org/10.1212/01.wnl.0000326262.67613.fe
de Vries AW, Faber G, Jonkers I, van Dieen JH, Verschueren SMP (2018) Virtual reality balance training for elderly: similar skiing games elicit different challenges in balance training. Gait Posture 59:111–116. https://doi.org/10.1016/j.gaitpost.2017.10.006
Gray R (2017) Transfer of training from virtual to real baseball batting. Front Psychol. https://doi.org/10.3389/fpsyg.2017.02183
Head D, Isom M (2010) Age effects on wayfinding and route learning skills. Behav Brain Res 209:49–58. https://doi.org/10.1016/j.bbr.2010.01.012
Huygelier H, Schraepen B, van Ee R, Vanden Abeele V, Gillebert CR (2019) Acceptance of immersive head-mounted virtual reality in older adults. Sci Rep 9:4519. https://doi.org/10.1038/s41598-019-41200-6
Kalová E, Vlcek K, Jarolímová E, Bures J (2005) Allothetic orientation and sequential ordering of places is impaired in early stages of Alzheimer’s disease: corresponding results in real space tests and computer tests. Behav Brain Res 159:175–186. https://doi.org/10.1016/j.bbr.2004.10.016
Kelly JW, Cherep LA, Siegel ZD (2017) Perceived space in the HTC Vive. ACM Trans Appl Percept 15:1–16. https://doi.org/10.1145/3106155
Kennedy RS, Lane NE, Berbaum KS, Lilienthal MG (1993) Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int J Aviat Psychol 3:203–220. https://doi.org/10.1207/s15327108ijap0303_3
Kimura K, Reichert JF, Olson A, Pouya OR, Wang X, Moussavi Z, Kelly DM (2017) Orientation in virtual reality does not fully measure up to the real-world. Sci Rep. https://doi.org/10.1038/s41598-017-18289-8
Klatzky RL (1998) Allocentric and egocentric spatial representations: definitions, distinctions, and interconnections. In: Goos G, Hartmanis J, van Leeuwen J, Freksa C, Habel C, Wender KF (eds) Spatial cognition, vol 1404. Springer. Berlin, Heidelberg, pp 1–17
Luo L, Craik FIM (2008) Aging and memory: a cognitive approach. Can J Psychiatry 53:346–353. https://doi.org/10.1177/070674370805300603
McAvan AS, Du YK, Oyao A, Doner S, Grilli MD, Ekstrom A (2021) Older adults show reduced spatial precision but preserved strategy-use during spatial navigation involving body-based cues. Front Aging Neurosci. https://doi.org/10.3389/fnagi.2021.640188
McIntyre J, Stratta F, Lacquaniti F (1998) Short-term memory for reaching to visual targets: psychophysical evidence for body-centered reference frames. J Neurosci 18:8423–8435. https://doi.org/10.1523/JNEUROSCI.18-20-08423.1998
Merhav M, Wolbers T (2019) Aging and spatial cues influence the updating of navigational memories. Sci Rep. https://doi.org/10.1038/s41598-019-47971-2
Mitolo M, Gardini S, Caffarra P, Ronconi L, Venneri A, Pazzaglia F (2015) Relationship between spatial ability, visuospatial working memory and self-assessed spatial orientation ability: a study in older adults. Cogn Process 16:165–176. https://doi.org/10.1007/s10339-015-0647-3
Moffat SD, Resnick SM (2002) Effects of age on virtual environment place navigation and allocentric cognitive mapping. Behav Neurosci 116:851–859. https://doi.org/10.1037/0735-7044.116.5.851
Morimoto T, Kobayashi T, Hirata H, Otani K, Sugimoto M, Tsukamoto M, Yoshihara T, Ueno M, Mawatari M (2022) XR (Extended reality: virtual reality, augmented reality, mixed reality) technology in spine medicine: status quo and quo vadis. J Clin Med. https://doi.org/10.3390/jcm11020470
Mujber TS, Szecsi T, Hashmi M (2004) Virtual reality applications in manufacturing process simulation. J Mater Process Technol 155–156:1834–1838. https://doi.org/10.1016/j.jmatprotec.2004.04.401
Newman MC, Kaszniak AW (2000) Spatial memory and aging: performance on a human analog of the morris water maze. Aging Neuropsychol Cogn 7:86–93. https://doi.org/10.1076/1382-5585(200006)7:2;1-U;FT086
Pastel S, Chen C-H, Martin L, Naujoks M, Petri K, Witte K (2020a) Comparison of gaze accuracy and precision in real-world and virtual reality. Virt Real. https://doi.org/10.1007/s10055-020-00449-3
Pastel S, Chen C-H, Petri K, Witte K (2020) Effects of body visualization on performance in head-mounted display virtual reality. PLoS One. https://doi.org/10.1371/journal.pone.0239226
Pastel S, Chen CH, Bürger D, Naujoks M, Martin LF, Petri K, Witte K (2020) Spatial orientation in virtual environment compared to real-world. J Mot Behav. https://doi.org/10.1080/00222895.2020.1843390
Pastel S, Bürger D, Chen CH, Petri K, Witte K (2021) Comparison of spatial orientation skill between real and virtual environment. Virt Real. https://doi.org/10.1007/s10055-021-00539-w
Patterson KK, Nadkarni NK, Black SE, McIlroy WE (2012) Gait symmetry and velocity differ in their relationship to age. Gait Posture 35:590–594. https://doi.org/10.1016/j.gaitpost.2011.11.030
Petri K, Feuerstein K, Folster S, Bariszlovich F, Witte K (2020) Effects of age, gender, familiarity with the content, and exposure time on cybersickness in immersive head-mounted display based virtual reality. Am J Biomed Sci 12:107–121. https://doi.org/10.5099/aj200200107
Plechatá A, Sahula V, Fayette D, Fajnerová I (2019) Age-related differences with immersive and non-immersive virtual reality in memory assessment. Front Psychol. https://doi.org/10.3389/fpsyg.2019.01330
Regian JW, Shebilske WL, Monk JM (1992) Virtual reality: an instructional medium for visual-spatial tasks. J Commun 42:136–149. https://doi.org/10.1111/j.1460-2466.1992.tb00815.x
Rodgers MK, Sindone JA, Moffat SD (2012) Effects of age on navigation strategy. Neurobiol Aging 33:202.e15–22. https://doi.org/10.1016/j.neurobiolaging.2010.07.021
Rodrigues J, Sauzéon H, Wallet G, N’Kaoua B (2010) Transfer of spatial-knowledge from virtual to real environment: Effect of active/passive learning depending on a test-retest procedure and the type of retrieval tests. J Cyber Ther Rehabil 3:275–283
Saredakis D, Szpak A, Birckhead B, Keage HAD, Rizzo A, Loetscher T (2020) Factors associated with virtual reality sickness in head-mounted displays: a systematic review and meta-analysis. Front Hum Neurosci. https://doi.org/10.3389/fnhum.2020.00096
Solini HM, Bhargava A, Pagano CC (2021) The effects of testing environment, experimental design, and ankle loading on calibration to perturbed optic flow during locomotion. Atten Percept Psychophys 83:497–511. https://doi.org/10.3758/s13414-020-02200-1
Stanney KM, Kennedy RS, Drexler JM (1997) Cybersickness is not simulator sickness. Proceed Human Fact Ergon Soci Annual Meet 41:1138–1142. https://doi.org/10.1177/107118139704100292
Stoyanova S, Ivantchev N, Petrova K (2016) Spatial orientation in sportsmen. Eur Scient J 12(24):88
Taillade M, N’Kaoua B, Sauzéon H (2015) Age-related differences and cognitive correlates of self-reported and direct navigation performance: the effect of real and virtual test conditions manipulation. Front Psychol. https://doi.org/10.3389/fpsyg.2015.02034
Tuena C, Pedroli E, Trimarchi PD, Gallucci A, Chiappini M, Goulene K, Gaggioli A, Riva G, Lattanzio F, Giunco F, Stramba-Badiale M (2020) Usability issues of clinical and research applications of virtual reality in older people: a systematic review. Front Hum Neurosci. https://doi.org/10.3389/fnhum.2020.00093
Waller D, Hunt E, Knapp D (1998) The transfer of spatial knowledge in virtual environment training. Presence 7:129–143. https://doi.org/10.1162/105474698565631
Wiener JM, Carroll D, Moeller S, Bibi I, Ivanova D, Allen P, Wolbers T (2020) A novel virtual-reality-based route-learning test suite: assessing the effects of cognitive aging on navigation. Behav Res Methods 52:630–640. https://doi.org/10.3758/s13428-019-01264-8
Wolbers T, Hegarty M (2010) What determines our navigational abilities? Trends Cogn Sci 14:138–146. https://doi.org/10.1016/j.tics.2010.01.001
Wolbers T, Wiener JM (2014) Challenges for identifying the neural mechanisms that support spatial navigation: the impact of spatial scale. Front Hum Neurosci. https://doi.org/10.3389/fnhum.2014.00571
Funding
Open Access funding enabled and organized by Projekt DEAL. Open Access funding is enabled and organized by Project DEAL. The study was financed by the German Research Foundation (DFG) under Grant No. WI 1456/22-1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
The approval of the Ethics Committee of the Otto-von-Guericke University at the Medical Faculty and University Hospital Magdeburg was obtained under the number 132/16.
Consent of participate
Available.
Consent for publication
All authors agreed to the publication process.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bürger, D., Pastel, S., Chen, CH. et al. Suitability test of virtual reality applications for older people considering the spatial orientation ability. Virtual Reality 27, 1751–1764 (2023). https://doi.org/10.1007/s10055-023-00775-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10055-023-00775-2