
Abstract
The subjective presence experience in virtual reality (VR) is associated with distinct brain activation patterns. Particularly, the dorsolateral prefrontal cortex (DLPFC) seems to play a central role. We investigated the effects of electric brain stimulation (transcranial direct current, tDCS) on the presence experience as well as on brain activity and connectivity. Thirty-eight participants received either anodal (N = 18) or cathodal (N = 20) stimulation of the DLPFC before interacting in an immersive VR as well as sham stimulation. During VR interaction, EEG and heart rate were recorded. After VR interaction, participants rated their subjective presence experience using standardized questionnaires. Cathodal stimulation led to stronger brain connectivity than sham stimulation. Increased brain connectivity was associated with numerically lower levels of subjective presence. Anodal stimulation did not lead to changes in brain connectivity, and no differences in subjective presence ratings were found between the anodal and sham stimulation. These results indicate that cathodal tDCS over the DLPFC leads to a more synchronized brain state, which might hamper the activity in networks, which are generally associated with the evolvement of the subjective presence experience. Our results underline the importance of the DLPFC for the presence experience in VR.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Virtual reality (VR) technology is becoming increasingly important not only for the entertainment industry but also in the context of training, therapy, and education. In this context, immersion and presence in VR play a crucial role. Technological advancements such as head-mounted displays (HMD), motion tracking systems, or advanced graphical designs and interactivity can influence the level of immersion of a VR system. In contrast, presence is defined as a psychological and subjective feeling of being in a VR, resulting from experiences induced by immersive VR technology (Diemer et al. 2015; Grassini and Laumann 2020; Slater 1999; Slater et al. 2009; Slater and Wilbur 1997; Steuer 1995; Witmer and Singer 1998). A higher degree of immersion generally leads to an increased presence experience (Diemer et al. 2015; Slater and Wilbur 1997). It is assumed that a heightened sense of presence in VR enhances the user’s capacity for interaction with the virtual simulation, fosters natural behavior in VR, and increases the chance of transfer effects to real-world behavior (Cummings and Bailenson 2016; Grassini and Laumann 2020; Kober et al. 2012; Riva and Mantovani 2012; Slater et al. 1996; Slater and Wilbur 1997). Therefore, studying and increasing the level of presence in VR is especially important when using VR in clinical settings, e.g., to treat phobias, or in educational settings, e.g., to train firefighters or surgeons (Diemer et al. 2015; Riva and Mantovani 2012; Slater and Wilbur 1997). As mentioned before, increasing the immersiveness of a VR by using advanced technology is one attempt to manipulate the subjective level of presence in VR. Another approach is to modulate the presence experience by using brain stimulation techniques (Beeli et al. 2008), which is the main aim of the present study. We investigate the effects of electrical brain stimulation on the presence experience in an interactive VR compared to sham stimulation and examine possible neural correlates.
There are different attempts to measure the subjective presence experience (Sanchez-Vives and Slater 2005). Self-report questionnaires are the most frequently used method to assess presence. Various presence questionnaires are available such as the Slater–Usoh–Steed Questionnaire (SUS; Usoh et al. 2000) or the Presence Questionnaire (PQ; Witmer and Singer 1998). There is evidence that the results of the different presence questionnaires are highly correlated (Kober and Neuper 2013). After interacting in VR, participants have to rate their subjective feeling of being in the VR on a rating scale.
An alternative and probably more objective way to measure presence experience is to record neural or physiological data (Grassini and Laumann 2020; Kober and Neuper 2012; Sanchez-Vives and Slater 2005). Changes in physiological signals such as heart rate or galvanic skin response might be indicators of presence experience indices (Grassini and Laumann 2020; Meehan et al. 2001) (see also Supplementary Material A). Different neuroscientific studies using the electroencephalogram (EEG) or functional magnet resonance tomography (fMRT) found an increased parietal activation and a decreased activation of the dorsolateral prefrontal cortex (DLPFC) during higher levels of presence (Baumgartner et al. 2006, 2008; Clemente et al. 2014; Jäncke et al. 2009; Kober et al. 2012). It is assumed that an egocentric or body-centered representation of space provided by the parietal lobe might be essential for the feeling of being in VR (Baumgartner et al. 2006, 2008; Kober et al. 2012). The DLPFC generally exerts executive control (top-down control processes) over other brain areas (Dosenbach et al. 2007; Shallice and Cooper 2011). In the context of presence experience, it is assumed that the DLPFC might exercise inhibitory control over activity of parietal brain regions and consequently modulates the associated experience of presence (fronto-parietal network hypothesis) (Jäncke et al. 2009). This is supported by empirical findings showing that children for whom prefrontal regions are not yet fully developed show an increased presence experience in VR compared to adults (Baumgartner et al. 2008). The higher presence experience in children compared to adults goes along with a decreased activation in these prefrontal brain areas in kids (Baumgartner et al. 2006). Summing up, the DLPFC is believed to play an important role in the development of the experience of presence in VR. It is identified as a key node of the brain network, which is associated with presence experience and modulates the activity of this network (Jäncke et al. 2009).
To directly investigate the functional role of the DLPFC in modulating presence in VR, Beeli et al. (2008) used transcranial direct current stimulation (tDCS) to activate or inhibit activity in this brain area and investigated the effects on presence experience, the vegetative nervous system and impulsiveness in a passive, non-interactive VR. TDCS is a noninvasive electrical brain stimulation technique, which either increases the excitability of neurons of specific brain areas (anodal stimulation) or decreases it (cathodal stimulation). There is evidence that tDCS over the DLPFC can have positive effects on cognition (Dedoncker et al. 2016) and mood (Herrera-Melendez et al. 2019). Beeli et al. (2008) applied anodal (to activate) and cathodal (to deactivate) tDCS to the right DLPFC to modulate the experience of presence while watching a virtual roller coaster ride on a 2D conventional computer screen. They assessed the subjective feeling of presence using questionnaires as well as physiological measures (electrodermal activity). They only found effects of cathodal tDCS on electrodermal activity. Cathodal tDCS led to an increased skin conductance level, which the authors interpreted as substantial change in responses of the vegetative nervous system. No effects on subjective presence questionnaire data were reported. Beeli et al. (2008) did not directly assess the effects of tDCS on brain activity or connectivity. Hence, we do not know whether tDCS applied over the DLPFC affected networks in the brain responsible for the development of presence experience in VR and consequently the feeling of being in VR.
In the present study, we want to expand the findings by Beeli et al. (2008) by using an interactive, 3D immersive VR. We investigate the effects of activating or deactivating the DLPFC by means of anodal/cathodal tDCS on the level of presence in an interactive VR and compare it to sham stimulation. In line with Beeli et al. (2008), we assess the subjective presence experience using questionnaires as well as more objective physiological indicators of presence, i.e., heart rate. Additionally, we focus on possible changes in brain connectivity/activity due to the tDCS intervention using electroencephalography (EEG) to investigate whether activating/deactivating the DLPFC by means of tDCS leads to activation changes in the fronto-parietal network associated with presence experience (Jäncke et al. 2009; Kober et al. 2012). We expect that tDCS, compared to sham stimulation, should lead to different levels of brain connectivity/activity in a fronto-parietal network associated with presence experience, consequently leading to different levels of presence experience in VR (Beeli et al. 2008; Jäncke et al. 2009; Kober et al. 2012).
2 Material and methods
2.1 Participants
Forty-three right-handed, healthy adults were pseudo-randomly assigned to an anodal and a cathodal stimulation group. Before entering the VR, all participants received both real tDCS stimulation and sham stimulation. Five participants were excluded due to excessive EEG artifacts. Hence, N = 18 participants were in the anodal tDCS group (mean age = 26.00 years, SD = 4.79, 9 men) and N = 20 were in the cathodal tDCS group (mean age = 24.90 years, SD = 3.77, 10 men). Participants and experimenter were not aware of the grouping design (anodal vs. cathodal) and the time point of the genuine stimulation (real vs. sham) using a double-blind design. All volunteers gave written informed consent. The study was approved by the local ethics committee of the University of Graz, Austria (GZ. 39/70/63 ex 2018/19) and is in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans [WMA (World Medical Association) 2009].
2.2 Procedure
Participants underwent the same procedure in both groups, except for the type of stimulation in the real tDCS condition (anodal/cathodal). After receiving written instructions explaining the procedure, demographic data were assessed as well as a baseline measurement of cybersickness using the Simulator Sickness Questionnaire (SSQ; Kennedy et al. 1993). This questionnaire assesses symptoms that can occur during or after interactions with VR systems, encompassing nausea, disorientation, and oculomotor symptoms. Moreover, two other questionnaires were completed for exploratory purpose with no further relevance for the present study.
Before the experimental conditions started, a test run was performed to familiarize participants with the VR system. Therefore, system handling and locomotion controls could be tested within a test environment for a maximum of 3 minutes. Afterward, participants consecutively underwent the real and the sham tDCS conditions, which only differed in the authenticity of the stimulation. The order of these conditions was balanced over all participants, so that each condition was preceded by the other condition equally often. In each condition, tDCS was applied before the VR interaction began. Before and after each tDCS application, resting EEGs were recorded. During VR interactions, participants could freely explore the virtual environment. To assess brain connectivity/activity inside the VR, EEG measurements were conducted at the beginning and at the end of each VR interaction. VR interactions lasted for 8 minutes each (including EEG measurements). After each VR interaction, subjective presence was measured using presence questionnaires, followed by a post-VR measurement of cybersickness using the SSQ. Furthermore, the subjective experience of the tDCS stimulation (e.g., the perceived electrical current flow) was assessed after every VR interaction using visual analogue rating scales ranging from 0 to 100. At the end of the procedure, subjectively experienced comfort during the EEG measurement was assessed using a self-made four-item questionnaire. There were no differences in the experienced comfort between groups or conditions. Therefore, the experienced comfort will not be analyzed in further detail. The whole experiment lasted approximately 2 hours.
2.3 Virtual reality
For the presentation of VR, a head-mounted display (HMD; HTC Vive Pro) with a resolution of 2880 × 1600 pixels (1440 × 1600 pixels per eye) and a refresh rate of 90 Hz was used. This is an immersive VR system that is widely used in the gaming industry. It enables the stereoscopic presentation of a virtual environment in 360 degrees from the egocentric perspective using modern tracking technology to accurately determine the position of the HMD and the controllers.
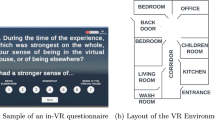
An adapted version of the virtual environment Sun Temple (Sandro 2019) was presented for the VR interaction, which is based on the game engine Unity (Unity Technologies, San Francisco, CA) and available in the Unity Asset Store (https://assetstore.unity.com). The environment consisted of a village with different buildings, streets, squares, gardens, and various types of vegetation. Also, a variety of small objects like stacks of stones, wooden benches, or fire pits within metal stands were scattered all over the environment. The whole environment was surrounded by a wide valley and confined by mountains on the horizon. We preferred this immersive, HMD-presented virtual environment over a non-interactive presentation on a screen (Beeli et al. 2008), so that the results of the study hold for the current state of the art in VR technology. Furthermore, Sun Temple is a static environment that does not contain virtual avatars, dynamic changes, or other elements, which might elicit emotional reactions when encountering them. This ensured comparability between VR interactions, because it is known that there is a strong link between emotion and presence (e.g., Riva et al. 2007).
Participants were instructed to explore the environment freely. This free exploration without a specific task was chosen because the emerging of natural and task-independent presence experience was intended. For exploration, a teleportation locomotion technique was implemented using the SteamVR Plugin (Valve Corporation, Bellevue, WA). Teleportation points and areas were placed inside the environment, to which participants could navigate using the HTC Vive Controller with their right hand. The controller as well as a virtual hand holding the controller were visualized inside the VR. Teleportation was preferred over continuous locomotion, because it is known that continuous locomotion is associated with higher levels of cybersickness (e.g., Clifton and Palmisano 2020). Participants interacted with the VR system in standing position. Because the VR system tracked the position of the HMD, locomotion was also possible by real movement in the limited interaction space of the laboratory (~ 4.5 m2).
2.4 Brain stimulation
For the tDCS, a conventional one-channel stimulator was used, the DC-STIMULATOR PLUS (neuroConn GmbH, Ilmenau, Germany). Saline-soaked electrodes (5 × 7 cm) were placed on the scalp overlying prefrontal sites. The anode was placed at the right temple (right DLPFC, EEG electrode position F4), and the cathode was placed at the right mastoid in the anodal tDCS group. The cathode was placed at the right temple (F4), and the anode was placed at the right mastoid in the cathodal tDCS group. This ipsilateral stimulation was in line with the stimulation protocol of Beeli et al. (2008). In the sham tDCS condition, the DC current was initially increased in a ramp-like fashion over a second until reaching 1 mA (current density of 0.06 μA/cm2) and turned off afterward (Gandiga et al. 2006). This protocol ensures that participants detect initial sensations on the scalp which also occur at the beginning of real tDCS (e.g., tingling).
In the real tDCS condition, direct current was applied with an intensity of 1 mA for 7 minutes. Prior studies show that a stimulation intensity of 1 mA and a duration of 7 minutes lead to aftereffects which last for a minimum of 10 minutes and a maximum of 20 minutes (Antal et al. 2004; Nitsche et al. 2003; Nitsche and Paulus 2000, 2001; Rogalewski et al. 2004). Thus, the effects of tDCS could be expected to be still present during the following VR interaction. At the same time, real and sham condition were separated by enough time (more than 20 min) to avoid carry-over effects.
Both real and sham stimulation were started by entering predefined codes encrypted by a third person. Thus, the experimenter also could not distinguish real from sham stimulation. Also, participants were not told that they receive a sham stimulation until the end of the experiment.
During stimulations, a toneless video showing wild animals (4K Urban Life 2017) was presented on a screen to achieve similar stimulation conditions between participants and stimulation conditions. Furthermore, watching an animal video was expected to draw participants’ attention in a constant manner over the time of stimulation and therefore should distract them from potential tDCS sensations on the skin.
2.5 Assessment of subjective presence experience
Subjective presence was measured using three different presence questionnaires, which were filled in after each VR interaction in randomized order: the Igroup Presence Questionnaire (IPQ; Schubert et al. 2001), the Spatial Presence Experience Scale (SPES; Hartmann et al. 2016), and the Slater–Usoh–Steed Questionnaire (SUS; Usoh et al. 2000).
The IPQ contains 14 items, assessing spatial presence, involvement, and experienced realism. Additionally, one item refers to general presence. The items are evaluated on a seven-point Likert scale (e.g., ranging from “fully disagree” to “fully agree”). One example of an IPQ spatial presence item is: “I felt present in the virtual space.” The IPQ subscale spatial presence has an internal consistency of 0.79, the subscale involvement 0.76, and the subscale experienced realism 0.69 (Schubert et al. 2001).
The SPES contains eight items, assessing self-location and perceived possible actions. The items are assessed on a five-point Likert scale ranging from “I do not agree at all” to “I fully agree.” One example of a SPES self-location item is: “It was as though my true location had shifted into the environment in the presentation.” This questionnaire is a short version of the MEC Spatial Presence Questionnaire (MEC-SPQ; Vorderer et al. 2004). The internal consistency of the subscale self-location is 0.86 and 0.88 for the subscale perceived possible actions (Hartmann et al. 2016).
The SUS contains 15 items, of which 5 items are related to presence assessing the sense of being in the VR, the extent to which the VR becomes the dominant reality, and the extent to which the VR is remembered as a place. The items are assessed on a seven-point scale ranging for instance from “Never” to “The whole time.” One example of a SUS item is: “When you think back about your experience, do you think of the virtual environment more as images that you saw, or more as somewhere that you visited?”. For this example, the scale ranged from “Images that I saw” to “Somewhere that I visited.” The SUS is highly correlated with other presence questionnaires, with correlation coefficients ranging from 0.60 to 0.67 (Kober and Neuper 2013; Usoh et al. 2000).
In line with Beeli et al. (2008), we focus on spatial presence, which primary refers to the feeling of being physically located in the virtual environment (International Society for Presence Research 2000). Hence, we analyzed the spatial presence subscale of the IPQ and the self-location subscale of the SPES. Since the SUS does not differentiate between different subscales, we included all five presence-related items of the SUS in the analysis.
For better comparability between the different presence questionnaires, we transferred the mean scores of all presence scales to percentage scores using the following formula: percentage score = [(original mean score − 1)/(number of possible answers − 1)] × 100. This led to percentage scores for subjective presence with a maximum score of 100%. Note that higher scores indicate higher presence experience.
2.6 EEG data recording and analysis
EEG data were recorded by Ag/AgCl electrodes over Fz, Cz, and Pz against a linked mastoid reference using a 10-channel EEG amplifier with a sampling rate of 256 Hz (NeXus-10 MKII, Mind Media BV). The ground was placed on the left mastoid, and one EOG channel was recorded over the left eye. During VR interaction, the EEG electrodes were placed under the VR headset, and the EEG amplifier was attached to the participants’ clothes (pants) and connected to the recording computer via Bluetooth. During VR interaction, participants were in an upright position and could move freely through the VR. To prevent that the EEG is too contaminated by movement artifacts, a 30-s fixation period was performed at the beginning and at the end of the VR interaction. During these 30-s fixation periods, participants were asked to focus on a point in the VR (to reduce eye movement artifacts) and to stand still and relaxed for a duration of 30 s. These fixation periods were used for EEG data analysis.
EEG data preprocessing and analysis were performed with the BrainVision Analyzer software (version 2.01, Brain Products GmbH, Munich, Germany). Ocular artifacts such as eye blinks were manually rejected by visual inspection based on the information about EOG activity provided by the EOG channel. After ocular artifact correction, automated rejection of other EEG artifacts (e.g., muscles) was performed (criteria for rejection: > 50.00 μV voltage step per sampling point, absolute voltage value > ± 200.00 μV, lowest allowed activity in 100 ms intervals: 0.5 µV). All epochs with artifacts were excluded from the EEG analysis.
We analyzed EEG coherence and power in the lower (8–10 Hz) and upper alpha (10–12 Hz) frequency range in accordance with prior studies investigating EEG correlates of presence experience (Baumgartner et al. 2006; Kober et al. 2012). We split up the alpha frequency range (8–12 Hz) in a lower and upper range since there is strong evidence for different functional meanings of lower and upper alpha (Klimesch 1999). Analysis of the resting measurements with open and closed eyes revealed that the individual alpha frequency was around 10 Hz for both groups (anodal tDCS group: 10.38 Hz; cathodal tDCS group: 10.02 Hz). Changes in the alpha frequency range are generally valid indicators of cortical activation/deactivation (i.e., power in the alpha frequency range is negatively related to activity) (Klimesch 1999; Laufs et al. 2003; Pfurtscheller and Lopes da Silva 1999).
To analyze EEG coherence in the lower and upper frequency range, each 30-s fixation period was cut in artifact-free 1-s epochs. FFT transformation was performed per epoch (Hanning window, 10%). Then, the magnitude-squared coherence was calculated for all channel pairs (Fz–Cz, Fz–Pz, Cz–Pz). Average coherence values were extracted per 30-s fixation period. Coherence values can range from 0 to 1, where 0 indicates no functional coupling (connectivity) or similarity between signals assessed at two different electrode positions. A high coherence is generally associated with synchronous electrical activity over two recording sites, while a lower coherence is a sign of desynchronized activity at two electrode positions (Nunez et al. 1997; Varela et al. 2001).
EEG power in the lower and upper alpha frequency range was extracted by means of complex demodulation implemented in the BrainVision Analyzer software (Brain Products GmbH 2009; Draganova and Popivanov 1999). Power values of artefact-free 1-s epochs were averaged per 30-s fixation period.
2.7 Statistical analysis
In the present study, we focus on the within-subject comparison between real vs. sham tDCS rather than on the between-subject comparison between anodal and cathodal tDCS groups to increase statistical power and because of the problem of inter-subject variability of tDCS effects (Horvath et al. 2014). Therefore, statistical analyses were performed separately for each group.
To analyze differences in presence experience between the sham and the real tDCS condition, paired-samples t tests were performed for questionnaire subscales assessing the sense of being in VR.
Repeated measures ANOVAs with the within-subject factors condition (real vs. sham tDCS), time (start and end of VR interaction), and electrode pair (Fz–Cz, Fz–Pz, Cz–Pz) were performed for the dependent variables coherence in the lower and upper alpha frequency range separately for the anodal and cathodal tDCS group.
For the statistical analysis of alpha power, heart rate, and the subjective experience of the tDCS stimulation, please see Supplementary Material B, C, and D.
The level for a type I error was set to 5%, and posttests for significant ANOVA effects were Bonferroni-corrected. Bonferroni–Holm correction was used when performing multiple t tests. Greenhouse–Geisser-corrected degrees of freedom are reported when the assumption of sphericity was violated.
3 Results
3.1 Presence experience
When looking at the data from a descriptive viewpoint, the cathodal group showed a numerically higher presence experience in VR after sham tDCS compared to real tDCS according to the results of the SUS (Table 1). However, this difference did not reach statistical significance. The cathodal group also showed a numerically higher presence rating after sham tDCS compared to real tDCS as assessed with the IPQ subscale spatial presence, but this difference did not reach statistical significance (Table 1). In contrast, the anodal group showed no differences in presence experience between the sham and real tDCS condition in none of the used questionnaires (Table 1).
3.2 EEG results: EEG coherence analysis
In the cathodal tDCS group, coherence in the lower alpha range was significantly increased after real than after sham stimulation (F(1,19) = 7.04, p = 0.016, ɳp2 = 0.27) (Fig. 1A). The ANOVA model revealed a significant main effect of electrode pair, too (F(1.42,26.88) = 8.95, p = 0.003, ɳp2 = 0.32). Lower alpha coherence was stronger for electrode pair Fz–Cz (M = 0.26, SE = 0.03) than for Fz–Pz (M = 0.14, SE = 0.02) and stronger for Cz–Pz (M = 0.26, SE = 0.03) compared to Fz–Pz (M = 0.14, SE = 0.02).

Results of EEG coherence analysis. A Coherence values (M and SE) for the real and sham tDCS condition, presented separately for the cathodal and anodal tDCS group. The significant main effect tDCS condition as revealed by the ANOVA model is marked with an asterisk. B Coherence values (M and SE) for each pair of electrodes in the upper and lower alpha frequency range, presented separately for the cathodal and anodal tDCS group, the real and the sham tDCS condition, and the start (T1) and end (T2) of the VR interaction
The ANOVA for the anodal tDCS group only revealed a significant main effect of electrode pair (F(1.41,23.99) = 11.72, p = 0.001, ɳp2 = 0.41). Lower alpha coherence was stronger for electrode pair Fz–Cz (M = 0.21, SE = 0.02) than for Fz–Pz (M = 0.12, SE = 0.02) and stronger for Cz–Pz (M = 0.26, SE = 0.04) compared to Fz–Pz (M = 0.12, SE = 0.02).
For coherence in the upper alpha range, the ANOVA for the cathodal tDCS group revealed a significant main effect of electrode pair (F(1.49,28.29) = 12.30, p < 0.001, ɳp2 = 0.39). Upper alpha coherence was stronger for electrode pair Fz–Cz (M = 0.25, SE = 0.03) than for Fz–Pz (M = 0.12, SE = 0.01) and stronger for Cz–Pz (M = 0.24, SE = 0.03) compared to Fz–Pz (M = 0.12, SE = 0.01).
The anodal tDCS group also showed a significant main effect of electrode pair (F(1.35,22.97) = 13.85, p < 0.001, ɳp2 = 0.45). Upper alpha coherence was strongest for electrode pair Cz–Pz (M = 0.26, SE = 0.04), second strongest for Fz–Cz (M = 0.16, SE = 0.02), and lowest for Fz–Pz (M = 0.11, SE = 0.01).
Coherence did not change over time (start and end of VR interaction). Figure 1B illustrates the coherence values for upper and lower alpha separately for each group, condition, and time point.
Results of the analysis of EEG power, heart rate, and subjective experience of the tDCS stimulation can be found in the Supplementary Material B, C, and D, respectively.
4 Discussion
In the present study, we investigated the effects of tDCS over the DLPFC on presence experience in an interactive and immersive VR. In the cathodal group, the cathode was placed over the right DLPFC during tDCS stimulation before VR interaction, which should lead to a deactivation of this brain region. In the anodal group, the anode was placed over the right DLPFC during tDCS before VR interaction, which should lead to an activation of this brain region. Modulating activity of the DLPFC using external brain stimulation should affect presence experience in VR. Presence was evaluated on the subjective, physiological, and neural level by analyzing subjective presence ratings as well as changes in heart rate and brain connectivity/activity in brain networks associated with presence experience. In the cathodal group, we found lower but nonsignificant subjective presence ratings and higher coherence between frontal, central and parietal brain regions in lower alpha frequency after real tDCS compared to sham. In the anodal group, no such differences in subjective presence ratings or coherence were found.
Cathodal stimulation, which should lead to a deactivation of the right DLPFC, was associated with an increased fronto-centro-parietal connectivity after real cathodal stimulation compared to sham stimulation. Prior tDCS studies also found changes in coherence measures after cathodal stimulation compared to sham tDCS (Notturno et al. 2014; Polanía et al. 2011; Shafi et al. 2012). Our results are in line with earlier findings, suggesting that the effect of tDCS cannot be reduced to focal brain regions, but rather to the manipulation of activity/connectivity in complex functional networks (Keeser et al. 2011; Lang et al. 2005). Hence, a numerically lower subjective presence experience was associated with higher brain connectivity in the cathodal tDCS group. This is in line with a previous study by Kober and Neuper (2012), who also found a negative relationship between the subjective presence experience and functional brain connectivity between frontal and parietal brain regions. Kober and Neuper (2012) investigated the subjective presence experience and EEG correlates while participants interacted either in a highly immersive Single-Wall-VR system or in a less immersive Desktop-VR system. Participants in the Desktop-VR group, who reported a lower subjective presence experience than participants of the Single-Wall-VR group, showed a significant higher alpha coherence than the Single-Wall-VR group. The authors concluded that their result might indicate that the functional connectivity between frontal and parietal brain regions is crucial for the presence experience and that it corroborates the assumptions of the fronto-parietal network hypothesis (Baumgartner et al. 2008; Jäncke et al. 2009; Kober et al. 2012). Generally, an increase in fronto-parietal long-range coherence in the alpha frequency mirrors activation of a fronto-parietal network (Sauseng et al. 2005). However, according to Beeli et al. (2008) deactivation of the DLPFC by means of cathodal stimulation should lead to a stronger sense of presence, since the DLPFC should inhibit activity in the presence network (e.g., activity in parietal brain areas), which should be responsible for the evolvement of the sense of being there (Baumgartner et al. 2008; Jäncke et al. 2009; Kober et al. 2012). Reducing these inhibitory effects of the DLPFC using cathodal tDCS should consequently lead to an increased presence experience (Beeli et al. 2008). Beeli et al. (2008) could not directly confirm this assumption in their study since they did not find any significant effects of cathodal tDCS on subjective measures of presence. Instead, cathodal tDCS over the DLPFC led to an increased skin conductance level. Additionally, Beeli et al. (2008) did not directly assess the effects of tDCS on brain activity or connectivity. In the present study, we found that cathodal tDCS significantly increased brain connectivity measures, which goes along with a reduced but statistically nonsignificant sense of being in VR. An increased coherence between different electrode positions is a sign for synchronous electrical activity of these brain areas. Consequently, this indicates a stronger functional relationship between these different brain areas (Varela et al. 2001). That in turn might indeed confirm the assumption that frontal executive functions exercised by the DLPFC might modulate activity in other brain areas (e.g., parietal regions) responsible for the evolvement of the presence experience (2009). A stronger frontal executive control over other brain areas might be indicated by increased brain connectivity measures (Sauseng et al. 2005). Hence, we could not support the assumption that cathodal stimulation deactivates or reduces such inhibitory processes by frontal brain areas leading to increased presence experience (Beeli et al. 2008). Instead, our results show that cathodal tDCS increases synchronous activity between frontal areas and centro-parietal areas in the brain indicating increased inhibitory processes which might lead to reduced presence experience.
We only observed significant effects of cathodal tDCS on coherence in the lower but not in the upper alpha frequency range. Lower and upper alpha generally have different functional meanings. Lower alpha is related to general attentional processes, while upper alpha is related to memory processes (Klimesch 1999). Hence, it makes sense that we found effects on lower alpha in relation to the subjective presence experience, which is associated with attention allocation from the real world to the virtual world, and not on upper alpha. The effects of the cathodal tDCS seemed to be stable since coherence did not change over time (from start to the end of the VR interaction, duration of 8 min). Different tDCS studies show that with the present stimulation parameters (1 mA for 7 minutes), tDCS effects last up to 10–20 min (Antal et al. 2004; Nitsche and Paulus 2000, 2001; Rogalewski et al. 2004).
In contrast to the study by Beeli et al. (2008), we used an interactive VR scenario, which could be explored freely. Additionally, participants saw the VR using an HMD. Hence, the level of immersion was higher in our study compared to the study by Beeli et al. (2008), in which participants passively watched a virtual roller coaster ride on a 2D conventional computer screen. A higher degree of immersion generally leads to an increased presence experience (Diemer et al. 2015; Slater and Wilbur 1997). Hence, the general presence experience in VR might have been higher in our study compared to the study by Beeli et al. (2008), limiting the direct comparability between studies. Differences in presence experience might also affect brain activity measures. For instance, higher levels of presence are associated with an increased parietal brain activation (Baumgartner et al. 2006, 2008; Clemente et al. 2014; Jäncke et al. 2009; Kober et al. 2012). Hence, a general increased presence experience in the present study might have led to an overall increased parietal brain activation. Consequently, real tDCS could not increase parietal brain activation any more, which might explain why we did not find significant effects on EEG power over parietal areas (see Supplementary Material B). Future studies might address the question of VR immersiveness and related specific effects of brain stimulation on presence experience and underlying neural correlates.
The cathodal group showed a numerically lower presence experience as assessed with the SUS in the real compared to the sham tDCS condition. In contrast to the cathodal group, the anodal group showed the same average values in the real and sham condition (Table 1). We used different presence questionnaires to assess the subjective feeling of presence. Prior studies showed that different presence questionnaires are highly intercorrelated (Kober and Neuper 2013). The used subjective presence measures (IPQ spatial presence, SPES self-location, SUS) all assessed spatial presence in VR, more concrete the subjective feeling of being located in the VR, which should be rated on Likert scales (either five or seven-point Likert scales, respectively). Here, we found the numerically largest difference in presence ratings between real and sham tDCS using the SUS, which was not significant any more after correction for multiple comparisons. As can be seen in Table 1, participants showed higher values in the sham compared to the real cathodal tDCS condition for the other two questionnaires, too, although these differences did not reach significance either. The reason why differences in presence ratings between real cathodal and sham tDCS were strongest for the SUS compared to the IPQ or SPES might be related to the anchor points of the rating scales. Probably, the SUS might be more sensitive since the anchor points of the Likert scales are always adapted to the question. For instance, the anchor points of the question “When you think back about your experience, do you think of the virtual environment more as images that you saw, or more as somewhere that you visited?” are “Images that I saw” to “Somewhere that I visited,” while the other two questionnaires use the same anchor points for each item (e.g., “fully disagree” to “fully agree”).
However, differences in presence ratings between real and sham tDCS were not statistically significant. Although using self-report questionnaires to ask for the subjective level of presence seems to be the most obvious method to assess presence, the questionnaires are associated with some disadvantages. Prior information can affect the presence rating (Freeman et al. 1999); they are retrospective and might be susceptible to response bias (Grassini and Laumann 2020). Presence questionnaires probably were not sensitive enough to reveal significant effects. In the study by Beeli et al. (2008), no differences in subjective presence ratings were found when comparing tDCS conditions. In this study, the authors also used a different presence questionnaire, namely an adapted version of the spatial presence questionnaire MEC-SPQ (Beeli et al. 2008). It is mentioned that they have focused on spatial presence as in the present study. We also used the SPES, which is a short version of the MEC Spatial Presence Questionnaire (MEC-SPQ; Vorderer et al. 2004). However, the exact adaptation of the questionnaire used in the study by Beeli et al. (2008) is not reproduceable. Therefore, differences concerning the tDCS effects on spatial presence ratings between the present study and the study by Beeli et al. (2008) might be caused by differences in the assessment of the subjective presence experience.
5 Limitations
One limitation of the present study is that we did not assess changes in electrical brain activity directly over the right DLPFC, where the anode/cathode was placed (EEG electrode position F4). Instead, we assessed the EEG over Fz, Cz, and Pz. The reason for that was that it was not possible to place an EEG electrode at position F4 under the VR headset without producing too much discomfort for the participants. Preliminary measurements showed that using Fz, Cz, and Pz was the most comfortable EEG montage when measuring EEG during VR interaction. Hence, we do not know whether the right DLPFC was really deactivated or activated by means of cathodal or anodal tDCS, respectively.
The analysis of the subjective experience of the tDCS stimulation (see Supplementary Material D) showed that perceived electrical current flow during the tDCS was higher in the real than in the sham tDCS condition in both groups. This indicates that participants’ blinding might not have been entirely successful, even though a standard sham protocol, which led to similar sensations as real tDCS (e.g., initial tingling), was used (Ambrus et al. 2012). However, this was the case in the cathodal and anodal group. Therefore, different effects of anodal/cathodal stimulation on brain activity/connectivity or presence measures cannot be explained by the subjective experienced intensity of current flow.
A further limitation of the present study is that we cannot directly compare anodal and cathodal tDCS groups since this is a between-subject factor. Due to the high inter-subject variability of tDCS effects, it only makes sense to perform within-subjects comparisons (Horvath et al. 2014). Therefore, we focused on the within-subject comparison between real and sham stimulation, separately for the anodal and cathodal group. Hence, we cannot draw any conclusion by directly comparing anodal and cathodal tDCS. Since the whole experiment already lasted approximately 2 hours, it would have taken too long for the participants to perform both anodal and cathodal tDCS, as well as the corresponding sham conditions. Future studies might probably overcome this timing problem by reducing the number of questionnaires or reducing the time spent in the VR, etc. A direct comparison between anodal and cathodal tDCS in future studies would reveal more about their specific effects on presence and underlying neural correlates.
6 Conclusion and outlook
Here, we show that cathodal tDCS over the right DLPFC leads to a more synchronized brain state, which might hamper the activity in networks, which are generally associated with the evolvement of the subjective presence experience. On the other hand, anodal tDCS over the right DLPFC did not affect brain connectivity measures. These results underline the importance of this brain area for the presence experience in VR. Knowing more about the emergence of the feeling of presence in the brain might reveal inter- but also intra-individual differences in presence experience and might also help to increase presence in future VR applications. For instance, individuals with a generally high connectivity in neural networks relevant for the emergence of presence might not experience such a strong sense of presence than individuals with lower connectivity levels. Or, when using VR in therapy, e.g., to train spatial orientation skills in patients with brain lesions (Kober et al. 2013), the location of the brain lesion might affect the patients’ presence experience and probably also the training outcome. Our results also demonstrate that the presence experience might be modulated by external brain stimulation. This would be of high relevance for the practical application of VR, e.g., in the clinical context. Effects of VR therapy or training might be increased by an increased presence experience, which might be evoked by altering the brain synchronization state using prefrontal tDCS in the future.
Availability of data and materials
Data that support the findings of this study are available on request from the corresponding author (S.E.K.) after contacting the Ethics Committee of the University of Graz (ethikkommission@uni-graz.at) for researchers who meet the criteria for access to confidential data. These ethical restrictions prohibit the authors from making the dataset publicly available.
References
4K Urban Life. (2017, May 27). 4K Ultra HD Video of Wild Animals - 1 HR 4K Wildlife Scenery with Floating Music [Video]. https://www.youtube.com/watch?v=TKmGU77INaM&t=470s
Ambrus GG, Al-Moyed H, Chaieb L, Sarp L, Antal A, Paulus W (2012) The fade-in—short stimulation—fade out approach to sham tDCS—reliable at 1 mA for naïve and experienced subjects, but not investigators. Brain Stimul 5:499–504. https://doi.org/10.1016/j.brs.2011.12.001
Antal A, Nitsche MA, Kruse W, Kincses TZ, Hoffmann K-P, Paulus W (2004) Direct current stimulation over V5 enhances visuomotor coordination by improving motion perception in humans. J Cogn Neurosci 16:521–527. https://doi.org/10.1162/089892904323057263
Baumgartner T, Valko L, Esslen M, Jäncke L (2006) Neural correlate of spatial presence in an arousing and noninteractive virtual reality: an EEG and psychophysiology study. Cyberpsychol Behav 9:30–45
Baumgartner T, Speck D, Wettstein D, Masnari O, Beeli G, Jäncke L (2008) Feeling present in arousing virtual reality worlds: prefrontal brain regions differentially orchestrate presence experience in adults and children. Front Hum Neurosci 2:1–2
Beeli G, Casutt G, Baumgartner T, Jancke L (2008) Modulating presence and impulsiveness by external stimulation of the brain. Behav Brain Funct 4:1–7
Brain Products GmbH (2009) BrainVision analyzer 2.0.1 user manual, 3rd edn. Brain Products GmbH, Munich
Clemente M, Rey B, Rodriguez-Pujadas A, Barros-Loscertales A, Banos RM, Botella C, Alcaniz M, Avila C (2014) An fMRI study to analyze neural correlates of presence during virtual reality experiences. Interact Comput 26:269–284. https://doi.org/10.1093/iwc/iwt037
Clifton J, Palmisano S (2020) Effects of steering locomotion and teleporting on cybersickness and presence in HMD-based virtual reality. Virtual Real 24:453–468. https://doi.org/10.1007/s10055-019-00407-8
Cummings JJ, Bailenson JN (2016) How immersive is enough? A meta-analysis of the effect of immersive technology on user presence. Media Psychol 19:272–309. https://doi.org/10.1080/15213269.2015.1015740
Dedoncker J, Brunoni AR, Baeken C, Vanderhasselt M-A (2016) A systematic review and meta-analysis of the effects of transcranial direct current stimulation (tDCS) over the dorsolateral prefrontal cortex in healthy and neuropsychiatric samples: influence of stimulation parameters. Brain Stimul 9:501–517. https://doi.org/10.1016/j.brs.2016.04.006
Diemer J, Alpers GW, Peperkorn HM, Shiban Y, Mühlberger A (2015) The impact of perception and presence on emotional reactions: a review of research in virtual reality. Front Psychol 6:26. https://doi.org/10.3389/fpsyg.2015.00026
Dosenbach NUF, Fair DA, Miezin FM, Cohen AL, Wenger KK, Dosenbach RAT, Fox MD, Snyder AZ, Vincent JL, Raichle ME, Schlaggar BL, Petersen SE (2007) Distinct brain networks for adaptive and stable task control in humans. Proc Natl Acad Sci USA 104:11073–11078. https://doi.org/10.1073/pnas.0704320104
Draganova R, Popivanov D (1999) Assessment of EEG frequency dynamics using complex demodulation. Physiol Res 48:157–165
Freeman J, Avons SE, Pearson DE, IJsselsteijn WA, (1999) Effects of sensory information and prior experience on direct subjective ratings of presence. Presence: Teleoper Virtual Environ 8:1–13
Gandiga PC, Hummel FC, Cohen LG (2006) Transcranial DC stimulation (tDCS): a tool for double-blind sham-controlled clinical studies in brain stimulation. Clin Neurophysiol 117:845–850. https://doi.org/10.1016/j.clinph.2005.12.003
Grassini S, Laumann K (2020) Questionnaire measures and physiological correlates of presence: a systematic review. Front Psychol 11:349. https://doi.org/10.3389/fpsyg.2020.00349
Hartmann T, Wirth W, Schramm H, Klimmt C, Vorderer P, Gysbers A, Böcking S, Ravaja N, Laarni J, Saari T, Gouveia F, Maria Sacau A (2016) The spatial presence experience scale (SPES). J Media Psychol 28:1–15. https://doi.org/10.1027/1864-1105/a000137
Herrera-Melendez A-L, Bajbouj M, Aust S (2019) Application of transcranial direct current stimulation in psychiatry. Neuropsychobiology. https://doi.org/10.1159/000501227
Horvath JC, Carter O, Forte JD (2014) Transcranial direct current stimulation: five important issues we aren’t discussing (but probably should be). Front Syst Neurosci 8:2. https://doi.org/10.3389/fnsys.2014.00002
International Society for Presence Research (2000) The concept of presence: explication statement. http://ispr.info/. Accessed 4 August 2001
Jäncke L, Cheetham M, Baumgartner T (2009) Virtual reality and the role of the prefrontal cortex in adults and children. Front Neurosci 3:52–59
Keeser D, Padberg F, Reisinger E, Pogarell O, Kirsch V, Palm U, Karch S, Möller H-J, Nitsche MA, Mulert C (2011) Prefrontal direct current stimulation modulates resting EEG and event-related potentials in healthy subjects: a standardized low resolution tomography (sLORETA) study. Neuroimage 55:644–657. https://doi.org/10.1016/j.neuroimage.2010.12.004
Kennedy RS, Lane NE, Berbaum KS, Lilienthal MG (1993) Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int J Aviat Psychol 3:203–220
Klimesch W (1999) EEG alpha and theta oscillations reflect cognitive and memory performance: a review and analysis. Brain Res Brain Res Rev 29:169–195
Kober SE, Wood G, Hofer D, Kreuzig W, Kiefer M, Neuper C (2013) Virtual reality in neurologic rehabilitation of spatial disorientation. J Neuroeng Rehabil 10:1–13
Kober SE, Neuper C (2012) Using auditory event-related EEG potentials to assess presence in virtual reality. Int J Hum Comput Stud 70:577–587. https://doi.org/10.1016/j.ijhcs.2012.03.004
Kober SE, Neuper C (2013) Personality and presence in virtual reality: does their relationship depend on the used presence measure? Int J Hum-Comput Interaction 29:13–25. https://doi.org/10.1080/10447318.2012.668131
Kober SE, Kurzmann J, Neuper C (2012) Cortical correlate of spatial presence in 2D and 3D interactive virtual reality: an EEG study. Int J Psychophysiol 83:365–374
Lang N, Siebner HR, Ward NS, Lee L, Nitsche MA, Paulus W, Rothwell JC, Lemon RN, Frackowiak RS (2005) How does transcranial DC stimulation of the primary motor cortex alter regional neuronal activity in the human brain? Eur J Neurosci 22:495–504. https://doi.org/10.1111/j.1460-9568.2005.04233.x
Laufs H, Kleinschmidt A, Beyerle A, Eger E, Salek-Haddadi A, Preibisch C, Krakow K (2003) EEG-correlated fMRI of human alpha activity. Neuroimage 19:1463–1476
Meehan M, Insko B, Whitton M, Brooks FP (2001) Physiological measures of presence in virtual environments. ACM Trans Graph 21:645–652
Nitsche MA, Paulus W (2000) Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J Physiol 527(Pt 3):633–639. https://doi.org/10.1111/j.1469-7793.2000.t01-1-00633.x
Nitsche MA, Paulus W (2001) Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 57:1899–1901. https://doi.org/10.1212/wnl.57.10.1899
Nitsche MA, Nitsche MS, Klein CC, Tergau F, Rothwell JC, Paulus W (2003) Level of action of cathodal DC polarisation induced inhibition of the human motor cortex. Clin Neurophysiol 114:600–604. https://doi.org/10.1016/s1388-2457(02)00412-1
Notturno F, Marzetti L, Pizzella V, Uncini A, Zappasodi F (2014) Local and remote effects of transcranial direct current stimulation on the electrical activity of the motor cortical network. Hum Brain Mapp 35:2220–2232. https://doi.org/10.1002/hbm.22322
Nunez PL, Srinivasan R, Westdorp AF, Wijesinghe RS, Tucker DM, Silberstein RB, Cadusch PJ (1997) EEG coherency. I: statistics, reference electrode, volume conduction, Laplacians, cortical imaging, and interpretation at multiple scales. Electroencephalogr Clin Neurophysiol 103:499–515
Pfurtscheller G, Lopes da Silva FH (1999) Event-related EEG/MEG synchronization and desynchronization: basic principles. Clin Neurophysiol 110:1842–1857
Polanía R, Nitsche MA, Paulus W (2011) Modulating functional connectivity patterns and topological functional organization of the human brain with transcranial direct current stimulation. Hum Brain Mapp 32:1236–1249. https://doi.org/10.1002/hbm.21104
Riva G, Mantovani F (2012) Being there: understanding the feeling of presence in a synthetic environment and its potential for clinical change. In: Eichenberg C (ed) Virtual reality in psychological, medical and pedagogical applications. InTech
Riva G, Mantovani F, Capideville CS, Preziosa A, Morganti F, Villani D, Gaggioli A, Botella C, Alcañiz M (2007) Affective interactions using virtual reality: the link between presence and emotions. Cyberpsychol Behav 10:45–56. https://doi.org/10.1089/cpb.2006.9993
Rogalewski A, Breitenstein C, Nitsche MA, Paulus W, Knecht S (2004) Transcranial direct current stimulation disrupts tactile perception. Eur J Neurosci 20:313–316. https://doi.org/10.1111/j.0953-816X.2004.03450.x
Sanchez-Vives MV, Slater M (2005) Opinion: From presence to consciousness through virtual reality. Nat Rev Neurosci 6:332–339
Sandro T (2019) Sun Temple (Version 1.0) [virtual environment]. https://assetstore.unity.com/packages/3d/environments/sun-temple-115417
Sauseng P, Klimesch W, Schabus M, Doppelmayr M (2005) Fronto-parietal EEG coherence in theta and upper alpha reflect central executive functions of working memory. Int J Psychophysiol 57:97–103
Schubert T, Friedmann F, Regenbrecht H (2001) The experience of presence: factor analytic insights. Presence: Teleoper Virtual Environ 10:266–281
Shafi MM, Westover MB, Fox MD, Pascual-Leone A (2012) Exploration and modulation of brain network interactions with noninvasive brain stimulation in combination with neuroimaging. Eur J Neurosci 35:805–825. https://doi.org/10.1111/j.1460-9568.2012.08035.x
Shallice T, Cooper R (2011) The organisation of mind. Oxford University Press, Oxford
Slater M (1999) Measuring presence: a response to the witmer and singer presence questionnaire. Presence: Teleoper Virtual Environ 8:560–565
Slater M, Wilbur S (1997) A framework for immersive virtual environments (FIVE): speculations on the role of presence in virtual environments. Presence: Teleoper Virtual Environ 6:603–616. https://doi.org/10.1162/pres.1997.6.6.603
Slater M, Linakis V, Usoh M, Kooper R (1996) Immersion, Presence, and Performance in Virtual Environments: An Experiment with Tri-Dimensional Chess. ACM Virtual Real Softw Technol (VRST) 163–172
Slater M, Lotto B, Arnold MM, Sanchez-Vives MV (2009) How we experience immersive virtual environments : the concept of presence and its measurement. Anu Psicol 40:193–210
Steuer J (1995) Defining virtual reality: dimensions determining telepresence. In: Biocca F, Levy MR (eds) Communication in the age of virtual reality. L. Erlbaum Associates, Hillsdale, pp 33–56
Usoh M, Catena E, Arman S, Slater M (2000) Using presence questionnaires in reality. Presence: Teleoper Virtual Environ 9:497–503
Varela F, Lachaux J-P, Rodriguez E, Martinerie J (2001) The Brainweb: phase synchronization and large-scale integration. Nat Rev Neurosci 2:229–239
Vorderer P, Wirth W, Gouveia, F. R., Biocca F, Saari T, Jäncke F, Böcking S, Schramm H, Gysbers A, Hartmann T, Klimmt C, Laarni J, Ravaja N, Sacau A, Baumgartner T, Jäncke P (2004) MEC spatial presence questionnaire (MEC-SPQ): short documentation and instructions for application. Report to the European Community, Project Presence: MEC (IST-2001-37661). Online. http://www.ijk.hmt-hannover.de/presence
Witmer BG, Singer MJ (1998) Measuring presence in virtual environments: a presence questionnaire. Presence: Teleoper Virtual Environ 7:225–240
WMA (World Medical Association) (2009) Declaration of Helsinki. Ethical principles for medical research involving human subjects. J Indian Med Assoc 107:403–405
Acknowledgements
The authors are grateful to Elija Dentler for data acquisition.
Funding
Open access funding provided by University of Graz. The authors acknowledge the financial support by the University of Graz.
Author information
Authors and Affiliations
Contributions
All authors were involved in designing the research and conceptualization; S.E.K. and W.K. performed research; S.E.K. and G.W. contributed to resources, software, and/or analytic tools; all authors were involved in data analysis and interpretation; S.E.K. and W.K. wrote the original draft. All authors reviewed, edited, and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kogler, W., Wood, G. & Kober, S.E. Effects of electrical brain stimulation on brain indices and presence experience in immersive, interactive virtual reality. Virtual Reality 26, 1019–1029 (2022). https://doi.org/10.1007/s10055-021-00612-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10055-021-00612-4