
Abstract
Purpose
Unlike other laparoscopic techniques, the peritoneum is not incised in laparoscopic totally extraperitoneal inguinal hernia repair (TEP), and the preperitoneal space is developed as the surgical field by blunt dissection and CO2 insufflation. While many studies have investigated the effect of neuromuscular blockade (NMB) on the surgical conditions and postoperative pain of laparoscopic intraperitoneal surgery, few studies have investigated those of TEP. In the present study, we investigated the effect of NMB on the surgical conditions and postoperative pain of TEP.
Methods
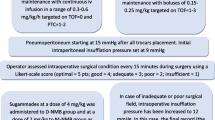
Forty-two adult patients scheduled for unilateral TEP under general anesthesia with remifentanil and desflurane were randomly assigned to paralyzed or non-paralyzed groups. In the paralyzed group, rocuronium doses were administered to maintain post-tetanic count at ≤ 5 during surgery. Non-paralyzed subjects were not given any rocuronium. Postoperatively, surgeon-evaluated surgical conditions, assessed using a 100-mm visual analogue scale ranging from 0 mm (not acceptable) to 100 mm (excellent), were compared between the two groups. For evaluation of postoperative pain, the time from the end of anesthesia to the initial requirement of postoperative analgesia was compared by the log-rank test.
Results
Median [interquartile range] score of surgical condition in the paralyzed and non-paralyzed groups were 84 [75–90] and 84 [78–87], respectively (P = 0.46). Significant differences in postoperative analgesic requirements between the two groups were not confirmed (P = 0.74).
Conclusion
NMB did not improve the surgical conditions nor reduce postoperative pain. NMB is not routinely needed for TEP just because it is a laparoscopic procedure.
Clinical trial registration
The trial was registered in the UMIN clinical trials registry (UMIN000029683, October 24, 2017; Principal investigator: Masafumi Fujimoto, https://upload.umin.ac.jp/cgi-open-bin/ctr/ctr_view.cgi?recptno=R000033920) prior to patient enrolment.



Similar content being viewed by others
Data availability
Available from the corresponding author on reasonable request.
References
Lauscher JC, Yafaei K, Buhr HJ, Ritz JP (2008) Laparoscopic and open inguinal hernia repair with alloplastic material: do the subjective and objective parameters differ in the long-term course? Surg Laparosc Endosc Percutan Tech 18:457–463. https://doi.org/10.1097/SLE.0b013e31817f4d70
Kuhry E, van Veen RN, Langeveld HR, Steyerberg EW, Jeekel J, Bonjer HJ (2007) Open or endoscopic total extraperitoneal inguinal hernia repair? A systematic review. Surg Endosc 21:161–166. https://doi.org/10.1007/s00464-006-0167-4
Andersson B, Hallén M, Leveau P, Bergenfelz A, Westerdahl J (2003) Laparoscopic extraperitoneal inguinal hernia repair versus open mesh repair: a prospective randomized controlled trial. Surgery 133:464–472. https://doi.org/10.1067/msy.2003.98
Park A, Birch DW, Lovrics P (1998) Laparoscopic and open incisional hernia repair: a comparison study. Surgery 124:816–822. https://doi.org/10.1067/msy.1998.92102
Kim MH, Lee KY, Lee KY, Min BS, Yoo YC (2016) Maintaining optimal surgical conditions with low insufflation pressures is possible with deep neuromuscular blockade during laparoscopic colorectal surgery: a prospective, randomized, double-blind, parallel-group clinical trial. Medicine 95:e2920. https://doi.org/10.1097/MD.0000000000002920
Koo BW, Oh AY, Seo KS, Han JW, Han HS, Yoon YS (2016) Randomized clinical trial of moderate versus deep neuromuscular block for low-pressure pneumoperitoneum during laparoscopic cholecystectomy. World J Surg 40:2898–2903. https://doi.org/10.1007/s00268-016-3633-8
Staehr-Rye AK, Rasmussen LS, Rosenberg J, Juul P, Lindekaer AL, Riber C, Gätke MR (2014) Surgical space conditions during low-pressure laparoscopic cholecystectomy with deep versus moderate neuromuscular blockade: a randomized clinical study. Anesth Analg 119:1084–1092. https://doi.org/10.1213/ANE.0000000000000316
Blobner M, Frick CG, Stäuble RB, Feussner H, Schaller SJ, Unterbuchner C, Lingg C, Geisler M, Fink H (2015) Neuromuscular blockade improves surgical conditions (NISCO). Surg Endosc 29:627–636. https://doi.org/10.1007/s00464-014-3711-7
Swann DG, Spens H, Edwards SA, Chestnut RJ (1993) Anaesthesia for gynaecological laparoscopy—a comparison between the laryngeal mask airway and tracheal intubation. Anaesthesia 48:431–434. https://doi.org/10.1111/j.1365-2044.1993.tb07021.x
Honing GHM, Martini CH, Olofsen E, Bevers RFM, Huurman VAL, Alwayn IPJ, van Velzen M, Niesters M, Aarts LPHJ, Dahan A, Boon M (2021) Deep neuromuscular block does not improve surgical conditions in patients receiving sevoflurane anaesthesia for laparoscopic renal surgery. Br J Anaesth 126:377–385. https://doi.org/10.1016/j.bja.2020.09.024
Bruintjes MH, van Helden EV, Braat AE, Dahan A, Scheffer GJ, van Laarhoven CJ, Warlé MC (2017) Deep neuromuscular block to optimize surgical space conditions during laparoscopic surgery: a systematic review and meta-analysis. Br J Anaesth 118:834–842. https://doi.org/10.1093/bja/aex116
Fuchs-Buder T, Claudius C, Skovgaard LT, Eriksson LI, Mirakhur RK, Viby-Mogensen J; 8th International Neuromuscular Meeting (2007) Good clinical research practice in pharmacodynamic studies of neuromuscular blocking agents II: the Stockholm revision. Acta Anaesthesiol Scand 51:789–808. https://doi.org/10.1111/j.1399-6576.2007.01352.x
Eger EI 2nd (2001) Age, minimum alveolar anesthetic concentration, and minimum alveolar anesthetic concentration-awake. Anesth Analg 93:947–953. https://doi.org/10.1097/00000539-200110000-00029
Caldwell JE, Laster MJ, Magorian T, Heier T, Yasuda N, Lynam DP, Eger EI 2nd, Weiskopf RB (1991) The neuromuscular effects of desflurane, alone and combined with pancuronium or succinylcholine in humans. Anesthesiology 74:412–418. https://doi.org/10.1097/00000542-199103000-00004
King M, Sujirattanawimol N, Danielson DR, Hall BA, Schroeder DR, Warner DO (2000) Requirements for muscle relaxants during radical retropubic prostatectomy. Anesthesiology 93:1392–1397. https://doi.org/10.1097/00000542-200012000-00008
Williams MT, Rice I, Ewen SP, Elliott SM (2003) A comparison of the effect of two anaesthetic techniques on surgical conditions during gynaecological laparoscopy. Anaesthesia 58:574–578. https://doi.org/10.1046/j.1365-2044.2003.03150.x
Martini CH, Boon M, Bevers RF, Aarts LP, Dahan A (2014) Evaluation of surgical conditions during laparoscopic surgery in patients with moderate vs deep neuromuscular block. Br J Anaesth 112:498–505. https://doi.org/10.1093/bja/aet377
Neudecker J, Sauerland S, Neugebauer E, Bergamaschi R, Bonjer HJ, Cuschieri A, Fuchs KH, Jacobi Ch, Jansen FW, Koivusalo AM, Lacy A, McMahon MJ, Millat B, Schwenk W (2002) The European Association for Endoscopic Surgery clinical practice guideline on the pneumoperitoneum for laparoscopic surgery. Surg Endosc 16:1121–1143. https://doi.org/10.1007/s00464-001-9166-7
Schwarte LA, Scheeren TW, Lorenz C, De Bruyne F, Fournell A (2004) Moderate increase in intraabdominal pressure attenuates gastric mucosal oxygen saturation in patients undergoing laparoscopy. Anesthesiology 100:1081–1087. https://doi.org/10.1097/00000542-200405000-00009
Sarli L, Costi R, Sansebastiano G, Trivelli M, Roncoroni L (2000) Prospective randomized trial of low-pressure pneumoperitoneum for reduction of shoulder-tip pain following laparoscopy. Br J Surg 87:1161–1165. https://doi.org/10.1046/j.1365-2168.2000.01507.x
Hua J, Gong J, Yao L, Zhou B, Song Z (2014) Low-pressure versus standard-pressure pneumoperitoneum for laparoscopic cholecystectomy: a systematic review and meta-analysis. Am J Surg 208:143–150. https://doi.org/10.1016/j.amjsurg.2013.09.027
Acknowledgements
We thank Hiroshi Kaneda, M.D., Shigeki Okamura, M.D., Kazuki Hori, M.D., Toshiyuki Okuma, M.D. and Hidetaka Sugihara, M.D., the surgeons of Nishinihon Hospital for their help in performing the study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Masafumi Fujimoto, Fumiyo Kubota and Hiroshi Kaneda. The first draft of the manuscript was written by Masafumi Fujimoto and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Masafumi Fujimoto, Fumiyo Kubota and Hiroshi Kaneda declare that they have no conflict of interest.
Ethics approval
This prospective randomized clinical trial was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The trial was approved by the ethics committee of Nishinihon Hospital, Kumamoto, Japan (protocol H29-4; October 31, 2017; Chairperson: Toshiyuki Arima).
Consent to participate
Prior written informed consent was obtained from all subjects participating in the trial.
Consent to publish
Patients signed informed consent regarding publishing their data.
Ethical standards
This clinical trial complies with the current laws of Japan.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Fujimoto, M., Kubota, F. & Kaneda, H. Effects of neuromuscular blockade on the surgical conditions of laparoscopic totally extraperitoneal inguinal hernia repair: a randomized clinical trial. Hernia 26, 1179–1186 (2022). https://doi.org/10.1007/s10029-022-02570-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-022-02570-5