
Abstract
Purpose
The present study aimed to assess whether there was an increase in physical aggression in women treated in Belo Horizonte, Minas Gerais, through the mandatory quarantine.
Methods
Data from a cross-sectional study were collected and analyzed, from March 1 to December 31, 2020. Additionally, data from the same period the previous year were collected for comparison.
Results
Of the etiologies reviewed for 2020, physical aggression had the highest percentage increase (+ 4.9%) and was the only etiology that showed a significant difference (p = 0.045). The mean age of the included patients was 34.05 years in 2019 and 33.97 in 2020, and most of the women had facial fractures, with nasal fractures being the most frequent, followed by jaw fractures. There was a significant increase (p = 0.34) in the conservative treatment of fractures from 2019 (48.6%) to 2020 (71.7%) and a minor (p = 0.088) increase in aggression toward intimate partners (2019, 40.9%; 2020, 63.9%).
Conclusion
Physical aggression against women increased during the period of mandatory social isolation that resulted from the COVID-19 pandemic. Health professionals, including emergency services professionals, must be trained to identify victims and refer them to specialized care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In December 2019, an increase in cases of respiratory diseases was reported in Wuhan, Hubei Province, China. Studies surrounding this novel disease revealed that the causative virus was severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 [1]. The disease caused by this pathogen was named coronavirus disease 2019 (COVID-19) by the World Health Organization (WHO) and was determined to be a global pandemic in March 2020 [1, 2]. Certain preventive measures, including the mandatory use of masks, social distancing, and isolation, were introduced in many countries during the pandemic to decrease the transmission rate of the virus [3, 4].
Relevant literature reported worrisome social and community consequences, such as anxiety, depression, suicide, substance abuse, and domestic violence, as the result of preventive social isolation [3, 5, 6]. For women who were already in abusive relationships, and those with a history of domestic violence, the home became a dangerous place during extended quarantines, as they were forced to stay with their partners all the time, increasing the risk of aggression [4, 6, 7].
Violence against women is a significant public health challenge, which generates emotional, psychological, and physical consequences, and affects women of all ages, socioeconomic classes, cultures, and religions [7, 9,10,11,12]. According to data published by WHO [13], 30% of all women who have been in a relationship reported having experienced physical and/or sexual violence by their intimate partner at some point in their lifetime [8, 10, 13].
The head and face are the most exposed and unprotected regions of the body and are often the focus of the aggressor [14, 15]. The face represents the identity of the individual, and injuries to this region can result in facial disfigurement, affect identity and self-image, and interfere with the individual’s social life [16]. Episodes of violence are often repetitive, and maxillofacial injuries may represent an initial sign of violence that tends to increase in severity [10].
The aim of the present study was to determine whether there was an increase in physical aggression toward women who were treated by an oral and maxillofacial surgery (OMFS) emergency service after the onset of mandatory quarantines compared to the same period the year prior.
Methods
Study design
The present retrospective, cross-sectional, and exploratory study was performed based on the analysis of medical records of patients admitted to the Oral and Maxillofacial Surgery department of the João XXIII Hospital/Hospital Foundation of Minas Gerais (FHEMIG), a level I trauma center in Belo Horizonte, in the state of Minas Gerais in southeast Brazil. This institution serves as a reference center for the state of Minas Gerais, which encompasses a population of more than 31,411,923 habitants. During the COVID-19 pandemic, the present hospital did not become a referral for patients with respiratory symptoms. The hospital remained a reference for trauma patients.
Eligibility criteria
All female patients with who presented to the João XXIII Hospital with signs of physical aggression, as well as complete medical records, were included in the present study. The exclusion criteria were as follows: male patients, women who did not receive clinical or surgical care from the OMFS team, and those who presented with missing data. Data were collected from electronic medical records for visits from March 1, 2020, to December 31, 2020, as well as the same period from the previous year (2019), with which to perform comparisons.
Data collection
The etiology of each injury was subdivided into seven primary categories: physical aggression, falls, traffic accidents, sports, work accidents, and others, which included face-to-face collision with a fixed object and fractures during third molar extraction. Sociodemographic data, circumstances of aggression, and characteristics of oral and maxillofacial trauma were all investigated. The hospitalization time was counted in days, from the day of admission to the day of discharge. Concomitant injuries included orthopedic fractures, chest or abdominal injuries, and neurological injuries. The treatment was subdivided into the following categories: open reduction, closed reduction, non-surgical treatment, and transfer before definitive treatment. Women were also asked about the mechanism of aggression, which included punches and kicks, paddles and stones, firearms, bladed weapons, and others (bricks, throwing objects at the face, and assault). The aggressor was identified by the women during the hospital stay and was defined as intimate partners (partner or ex-partner), son, or others (unknown). The notification data were collected based on the documentation of the professionals who evaluated the women.
Statistical analysis
All data were tabulated and analyzed using IBM SPSS 26 (IBM, Armonk, NY, USA). Absolute numbers and percentages were used for the descriptive statistics, and the Shapiro–Wilk test was used to check the normality of the distribution of the numeric variables. The distribution of the variables (“etiology”; “patient fracture”; “fracture type”; “concomitant injuries”; “treatment”; “who attacked”; and “notification”) was found to be normal. The chi-square test was used for categorical variables, while Fisher’s exact test was utilized for any cell with five or fewer observations. A confidence interval of 95% was considered statistically significant at p < 0.05.
Ethical aspects
The present study was approved by the Research Ethics Committee at FHEMIG (protocol no. 104/2018), and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cross-sectional studies was followed.
Results
From March 1, 2019, to December 31, 2019, and March 1, 2020, to December 31, 2020, 725 women with facial trauma were admitted to our hospital: 370 in 2019 and 355 in 2020. Gross and relative comparisons were performed between the 2019 and 2020 groups, and of the etiologies evaluated, physical aggression was found to be the only etiology that had a significant difference (p = 0.045), as it increased (+ 4.9%) from 2019 to 2020. The other etiology that increased was sports accidents (+ 0.8%), although the difference was not significant (p = 0.430). The other etiologies evaluated decreased slightly from 2019 to 2020, as follows: traffic accidents (− 1.9%), falls (− 5.1%), work accidents (− 0.5%), and others (− 2.2%), as seen in Table 1.
The physical aggression etiology group included 130 women, 56 treated in 2019, and 74 in 2020 (Table 1). The mean age of the women was 34.05 years in 2019 and 33.97 in 2020, and marital status was reported by 102 women. Single was the most common status, at 78.3% and 75.0% in 2019 and 2020 respectively, followed by married, at 13.0% and 14.3%, respectively. Race/ethnicity was reported by 127 patients; in 2019 and 2020, brown ethnicity was most frequently reported (62.5 and 71.8%, respectively), followed by white (28.6 and 21.1%, respectively) and black (8.9 and 7.0%, respectively), as seen in Table 2.
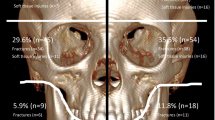
In 2019, 35 women (62.5%) presented with facial fractures, compared with 46 (62.2%) in 2020, showing no significant difference between the groups (p = 0.969). There were a total of 101 fractures, and some women had > 1 facial fracture. Nasal fractures (17; 37.8%) were the most common fractures in 2019, followed by the mandible (14; 31.1%), frontal bone (9; 20.0%), zygomatic arch (3; 6.7%), and maxilla and orbit (1 each; 2.2%). Nasal fractures (26; 46.4%) were also more common in 2020, followed by the mandible (7; 12.5%), orbit (7; 12.5%), frontal bone (4; 7.1%), maxilla (6; 10.7%), zygomatic arch (4; 7.1%), and dento-alveolar (2; 3.6%). When comparing the groups, only mandibular fractures were significantly different (p = 0.017) from 2019 to 2020. In 2019, 13 patients had concomitant injuries (23.2%), compared to 29 patients (39.25%) in 2020, although there was no significant difference (p = 0.054) between the groups. The average hospital stay was 1.64 days in 2019 and 4.15 days in 2020, although the difference between the years was not significant (p = 0.885). The Mann–Whitney U test was used to compare the hospital stay and concomitant injuries and showed a significant difference (p = 0.001).
When evaluating the day of the week on which the trauma occurred, the weekend days were most common, with Sundays (25.0%), Fridays (16.1%), and Saturdays (13.0%) being more frequent in 2019, while Sundays (31.5%), Saturdays (16.4%), and Tuesdays (15.1%) were the most frequent in 2020. The time from trauma to initial care was 0.32 days in 2019, compared to 0.46 days in 2020, with no significant difference between the years (p = 0.526). A mechanism of aggression was reported in 94 patients, most frequently through punches and kicks in 2019 and 2020 (85.7 and 57.7%, respectively), followed by paddles and stones (7.1 and 15.4%, respectively).
A total of 81 patients received treatment for their injuries. In 2019, non-surgical treatment was most frequently utilized (48.6%), followed by open (40.0%), and closed surgery (8.6%), with only 1 patient having been transferred to another hospital prior to undergoing definitive treatment. In 2020, non-surgical treatment was even more frequently selected (71.7%), followed by closed (15.1%) and open surgery (10.9%). Again, one patient was transferred to another hospital prior to undergoing definitive treatment. The statistical analyses comparing year and treatment showed a decrease in open surgery in 2020 compared to 2019, which was a significant difference (p = 0.002). In contrast, non-surgical treatment significantly increased from 2019 to 2020 (p = 0.034).
Data regarding who assaulted them was only reported by 58 women. In 2019, others were most frequently reported (54.4%), followed by intimate partners (40.9%). In 2020, the number of women who reported abuse by an intimate partner increased (63.9%), although not significantly (p = 0.088). Fisher’s exact test was performed between the variables who assaulted and time from trauma to initial care, although the difference was not found to be significant (p < 0.138). The number of notifications increased from 2019 to 2020 (58.1%), although the difference was not significant (p = 0.179).
Discussion
Social isolation was made mandatory in many countries during the COVID-19 pandemic, as a way to reduce the transmission of the virus [4]. Although data are still scarce, relevant literature reports that, during this period, there was an increase in violence against women [5, 6, 8]. Kilius et al. [17] suggested that, in women, in particular, there was a significant increase in aggressive dream content from March to July 2020. No studies, however, have directly addressed the aspect of facial trauma in female victims of physical aggression during quarantines resulting from the COVID-19 pandemic.
Intimate partner violence is one of the most common causes of maxillofacial trauma in women [11]. The results of the present study showed an increase in physical aggression during the period of mandatory social isolation, with 56 women reporting physical aggression in 2019 compared to 75 in 2020, an increase of + 32.1%. Compared with the other groups, physical aggression was the etiology with the highest percentage of increase (+ 4.9%) from 2019 to 2020 and the only one with a significant difference.
The average age of the women included in the present study was 34.05 in 2019 and 33.97 in 2020, with women in their 3rd decade of life being the most numerous. Most of the women were single (78.3% in 2019 and 75.0% in 2020), followed by married (13 and 14.3%, respectively), and the race/ethnicity selection of brown was the most common in both of the included periods (Table 2). The epidemiological findings of the present study corroborate relevant literature; however, these data may vary depending on the location of the study [12, 18]. The relevant literature reported a higher incidence of physical aggression on weekends, which coincides with the days when the abuser is more likely to become intoxicated with alcohol and/or drugs, and the days when victims have few options to flee [10, 12]. The results of the present study revealed that aggression occurred on the weekend, being more common on Sunday, followed by Saturday in both periods.
Studies have shown an overall higher alcohol consumption in men, as well as an association between alcohol consumption and intimate partner violence, and one American study showed that abusers’ use of alcohol was associated with an 8 times greater occurrence of violence against women [12, 19]. Considering the high occurrence of physical aggression during weekends, it is important that services aimed at protecting women and assisting victims are available every day [12]. Due to fear, financial dependence, or the victim’s affective relationship with the abuser, shame, or the abuser forbidding the victim to seek medical attention, women may often prolong the time between the trauma and the initial care [10]. In contrast, the findings of the present study revealed that there was no relationship between who attacked the patient and the time from trauma to initial care (p < 0.138).
Data collected at a referral hospital for victims of violence in Malaysia revealed that 50.4% of the patients evaluated had maxillofacial injuries [20]. In a retrospective study performed in Oregon, 81% of the patients had lesions on the face [21]. Of the women included in the present study, facial fractures were most common in both years (62.5% in 2019 and 62.2% in 2020), although there was no significant difference (p = 0.969).
In total, 101 facial fractures were documented during the study period, with some women having more than one facial fractures. Nasal fractures were the most common injuries documented (37.8% in 2019 and 46.4% in 2020), corroborating findings in the relevant literature which may be attributed to the central position and the protuberance of the nose, which make it more vulnerable to impact than other facial structures, the relatively thin bones, and the low force required to fracture the bones [10, 21, 22]. Despite the increase in the number of nasal fractures between the time periods, however, there was no significant difference (p = 0.566). Mandible fractures were the second most common fracture, at 31.1% in 2019 and 12.5% in 2020, as the results of the present study indicated a significant decrease between the study periods (p = 0.017). Other locations were also affected, such as the frontal bones, orbits, zygomatic complex, maxilla, and dentition.
Oftentimes, women may have concomitant injuries, such as orthopedic fractures in conjunction with thoracic, abdominal, and neurological injuries. There was an increase in concomitant injuries from 2019 to 2020, from 23.2 to 39.2%, respectively, although the difference was not significant (p = 0.054). Women with concomitant bodily injuries had a greater chance of prolonged hospitalization and increased hospital costs, and the results of the present study indicated that this relationship was statistically different (p < 0.001). It is worth mentioning the multidisciplinary team is critical at the initial presentation to ensure the correct diagnosis and adequate and efficient treatment.
The costs of healthcare, prolonged hospital stays, and work absenteeism that victims experience are high for the public health system [23]. According to the United Nations, worldwide violence against women costs 1.5 trillion United States dollars per year for those involved in serving women [23]. In the present study, the length of the average hospital stays increased in 2020, although the difference was not statistically significant (p = 0.885).
Boyes and Fan observed that the most common injury mechanism was punches, followed by aggression with common household objects, such as a lamp or knife [9]. A study by Barbosa et al. indicated that the primary mechanism of injury was brute force or body strength, which includes punches, kicks, slaps, headbutts, and knee strikes [18]. The findings in relevant literature corroborate those of the present study, in which the most common mechanisms of aggression were punches and kicks, followed by paddles and stones.
The conservative (non-surgical) treatment of facial fractures increased significantly (p = 0.34) from 48.6% in 2019 to 71.7% in 2020. In contrast, open surgery decreased significantly (p = 0.002), from 40.0% in 2019 and 10.9% in 2020. During the lockdown period, it was highly recommended to postpone elective surgeries and perform only emergency interventions, due to the scarcity of resources and to avoid exposure to the virus [24].
The government of Minas Gerais Brazilian state published a decree in July 2020, which suspended elective care and classified the following as emergency care: uncontrolled bleeding, serious infections, and trauma involving the facial bones with the potential to compromise the airway [25]. A potential bias of this present study is that the hospital could potentially have experienced an artificial increase the number of facial trauma referrals secondary to manning shortages, and reduced services offered, at referral hospitals in the community due to the COVID-19 pandemic. However, upon review, the authors found a similar number of female patients’ victims of aggression in the period before COVID-19 pandemic status compared to the lockdown period. In 2019, there were 370 patients while in 2020, 355 patients were encountered, suggesting a very similar sample.
Interpersonal violence encompasses both domestic and community violence. The first includes cases involving family members and people in romantic or intimate relationships, while the second occurs between unrelated people who may or may not be known to each other [18]. In a study conducted in London, most aggressors were found to be current or former partners of the victim (83%), followed by family members (17%) [9].
A study conducted in Brazil showed that the aggressors were identified as men by 97.6% of female victims, and another Brazilian study demonstrated that 80% of women suffered from physical aggression by current or ex partners [10, 12]. The results of the present study showed an increase in intimate partner aggression from 2019 (9; 40.9%) to 2020 (23; 63.9%); however, the difference was not significant (p = 0.088).
Some legislative measures have been carried out, such as the Brazilian Law n. 10 778/2003, which requires all cases of domestic violence against women to be reported [26]. Reporting by health professionals is mandatory for all family, sexual, and violent incidents, and these reports are filed into a large government database called the Notifiable Diseases Information System (SINAN) [18]. The number of SINAN notifications is still very low, as evidenced in the present study, in which 130 women were treated for physical aggression, but only 40 women named their aggression. Female victims of intimate partner violence often seek health services to treat injuries, with health professionals being their first point of contact [12]. Relevant literature has pointed out that female victims of violence identify health professionals as reliable confidantes, to whom they can reveal their experience with domestic violence [12]. As such, health professionals must be trained to recognize the indicators of violence against women [8].
The present study did have some limitations, owing to its retrospective nature, as all of the information analyzed was based on medical records. In an effort to minimize variability in the data collection, only one author reviewed the data. Additionally, the etiology was based on the patients’ reports at the initial visit; therefore, it is possible that some women may have omitted the true cause of their trauma.
In conclusion, physical aggression against women increased during the period of mandatory social isolation that resulted from the COVID-19 pandemic. Health professionals, including emergency services professionals, must be trained to identify victims and refer them to specialized care. Additionally, further studies are needed to assess the consequences of this impact.
Data availability
Not applicable.
References
He F, Deng Y, Li W (2020) Coronavirus disease 2019: What we know? J Med Virol 92:719–725. https://doi.org/10.1002/jmv.25766
Peng X, Xu X, Li Y, Cheng L, Zhou X, Ren B (2020) Transmission routes of 2019-nCoV and controls in dental practice. Int J Oral Sci 12:9. https://doi.org/10.1038/s41368-020-0075-9
Alharbi FF, Alkheraiji MA, Aljumah AA, Al-Eissa M, Qasim SS, Alaqeel MK (2021) Domestic violence against married women during the COVID-19 quarantine in Saudi Arabia. Cureus 25:15231. https://doi.org/10.7759/cureus.15231
Coulthard P, Hutchison I, Bell JA, Coulthard ID, Kennedy H (2020) COVID-19, domestic violence and abuse, and urgent dental and oral and maxillofacial surgery care. Br Dent J 228:923–926. https://doi.org/10.1038/s41415-020-1709-1
Bradbury-Jones C, Isham L (2020) The pandemic paradox: the consequences of COVID-19 on domestic violence. J Clin Nurs 29:2047–2049. https://doi.org/10.1111/jocn.15296
Klimovich-Mickael A, Kubick N, Milanesi E, Dobre M, Łazarczyk M, Wijas B et al (2021) Trends of anger and physical aggression in Russian women during COVID-19 lockdown. Front Glob Womens Health 2:698151. https://doi.org/10.3389/fgwh.2021.698151
Mazza M, Marano G, Lai C, Janiri L, Sani G (2020) Danger in danger: interpersonal violence during COVID-19 quarantine. Psychiatry Res 289:113046. https://doi.org/10.1016/j.psychres.2020.113046
Roesch E, Amin A, Gupta J, García-Moreno C (2020) Violence against women during covid-19 pandemic restrictions. BMJ 369:1712. https://doi.org/10.1136/bmj.m1712
Boyes H, Fan K (2020) Maxillofacial injuries associated with domestic violence: experience at a major trauma centre. Br J Oral Maxillofac Surg 58:185–189. https://doi.org/10.1016/j.bjoms.2019.11.009
Mayrink G, Araújo S, Kindely L, Marano R, de Filho ABM, de Assis TV et al (2021) Factors associated with violence against women and facial trauma of a representative sample of the Brazilian population: results of a retrospective study. Craniomaxillofacial Trauma Reconstr 14:119–25
O’Doherty L (2015) Screening women for intimate partner violence in healthcare settings. Cochrane Database Syst Rer 7:CD007007. https://doi.org/10.1002/14651858.CD007007.pub3
Garcia LP, da Silva GDM (2018) Violência por parceiro íntimo: perfil dos atendimentos em serviços de urgência e emergência nas capitais dos estados brasileiros, 2014. Cad Saúde Pública 34:e00062317. https://doi.org/10.1590/0102-311X00062317
World Health Organization. Violence against women. World Health Organization, 29 November 2017. [Homepage on the Internet] [Accessed April 4, 2022]. https://www.who.int/news-room/fact-sheets/detail/violence-against-women
de Dourado SM, Noronha CV (2015) Marcas visíveis e invisíveis: danos ao rosto feminino em episódios de violência conjugal. Ciênc saúde coletiva 20:2911–20
de Macedo BÍ, Santos LM, Ferreira AVP, de Almeida Lima TLM, da Nóbrega LM, d’Avila S (2018) Multiple correspondence analysis as a strategy to explore the association between categories of qualitative variables related to oral–maxillofacial trauma and violent crimes at the community level. Int J Oral Maxillofac Surg 47:339–344. https://doi.org/10.1016/j.ijom.2017.08.001
da Nóbrega LM, Bernardino Í de M, Barbosa KGN, e Silva JAL, Massoni AC de LT, d’Avila S (2017) Pattern of oral-maxillofacial trauma from violence against women and its associated factors. Dent Traumatol 33:181–8. https://doi.org/10.1111/edt.12327
Kilius E, Abbas NH, McKinnon L, Samson DR (2021) Pandemic nightmares: COVID-19 lockdown associated with increased aggression in Female University Students’ Dreams. Front Psychol 12:644636. https://doi.org/10.3389/fpsyg.2021.644636
Barbosa KGN, Walker BB, Schuurman N, Cavalcanti SDLB, Ferreira e Ferreira E, Ferreira RC (2019) Epidemiological and spatial characteristics of interpersonal physical violence in a Brazilian city: a comparative study of violent injury hotspots in familial versus non-familial settings, 2012-2014. PLoS One 14:e0208304. https://doi.org/10.1371/journal.pone.0208304
Sharps PW, Campbell J, Campbell D, Gary F, Webster D (2001) The role of alcohol use in intimate partner femicide. Am J Addict 10:122–35. http://doi.wiley.com/10.1080/105504901750227787
Saddki N, Suhaimi AA, Daud R (2010) Maxillofacial injuries associated with intimate partner violence in women. BMC Public Health 10:268. https://doi.org/10.1186/1471-2458-10-268
Le BT, Dierks EJ, Ueeck BA, Homer LD, Potter BF (2001) Maxillofacial injuries associated with domestic violence. J Oral Maxillofac Surg 59:1277–1283. https://doi.org/10.1053/joms.2001.27490
Sindi A, Abaalkhail Y, Malas M, Alghamdi A, Joharji M (2020) Patients With Nasal Fracture J Craniofac Surg 31:275–277. https://doi.org/10.1097/SCS.0000000000006269
UN W (2017) UN warns of costs of violence against women worldwide. [Homepage on the Internet] [Accessed April 4, 2022]: https://www.unwomen.org/en/news/stories/2016/9/speech-by-lakshmi-puri-on-economic-costs-of-violence-against-women
Zimmermann M, Nkenke E (2020) Approaches to the management of patients in oral and maxillofacial surgery during COVID-19 pandemic. J Craniomaxillofac Surg 48:521–526. https://doi.org/10.1016/j.jcms.2020.03.011
Government of the State of Minas Gerais. Technical Note no 68/ses/coes minas covid-19/2020. guidelines for dental care in the scenario of facing COVID-19 [Homepage on the Internet] [Accessed April 4, 2022]. https://coronavirus.saude.mg.gov.br/images/profissionais-e-gestores/23-07_Nota-Tecnica-COES-MINAS-COVID-19-N68.pdf
Brazil. Law n. 10 778. 2003 [Homepage on the Internet] [Accessed April 24, 2022]: http://www.planalto.gov.br/ccivil_03/leis/2003/l10.778.htm
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of the study. S. C. S. A. performed data acquisition. All authors analyzed or interpreted the data, contributed drafting of article and/or critical revision, and final approval of manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The present study was approved by the Research Ethics Committee at FHEMIG (protocol no. 104/2018).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Araujo, S.C.S., de Souza, A.A.B., Coelho, L.V. et al. Did physical aggression in women increase during the novel coronavirus 2019 (COVID-19) pandemic? A perspective of facial trauma. Oral Maxillofac Surg 28, 149–155 (2024). https://doi.org/10.1007/s10006-022-01118-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10006-022-01118-2