
Abstract
Purpose
Facial trauma in women is complex with physical, psychosocial, and cultural influences impacting clinical presentations. Although multifactorial, assaults and falls are principally reported as the main causes.
Methods
A retrospective review was conducted from January 2012 to January 2017 at the Women and Children’s Hospital and Royal Adelaide Hospital, Adelaide. All maxillofacial fractures in women that attended or were referred to the unit were included in this study. The primary objective was to analyse epidemiological trends of facial fractures and clinical outcomes in the South Australian female population.
Results
There is a bimodal distribution of facial fractures at 25–35 years and 65 + years. Indigenous females were 19.5 years younger than non-indigenous females (30.5 vs 49.9, P < 0.001). Approximately half the cohort had a fall-related facial fracture, followed by assault (26.2%), and sports (10.3%). There was a higher proportion of non-alcohol-related trauma from assaults than alcohol-related assaults (72.5% vs 27.5%, P < 0.001). Over half (58.0%) of the cohort had a midface fracture. The elderly had increased odds of 1.9 fold for facial fractures in winter, largely from falls, compared to younger women. Associated injuries were present in almost half the elderly women with 2.6 times the risk compared to younger women. Younger women had higher incidences of surgical intervention (52.6% vs 14.3%, P < 0.05).
Conclusions
Young women disproportionately experience larger incidences of non-alcohol-related assaults requiring operative intervention of the mandible, whereas elderly women principally suffer fall-related facial fractures with higher rates of associated injuries.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Facial fractures are largely experienced by young adult males. There is however unique profiling for women who experience facial trauma from childhood to elderly. Often overlooked in many studies, the complexity of facial fractures in women involves a more global assessment of physical and psychosocial wellbeing with potential secondary consequences to functional impairment and disfigurement. Domestic violence is a growing concern amongst developing and developed countries where the perpetrator is often intimately known to the patient adding clout to the mechanism of injury and potential risk factors. International studies have indicated that assaults are disproportionately experienced by indigenous persons from Canada, Australia, and New Zealand compared to their non-indigenous counterparts [1,2,3]. The impact of domestic violence against women and children in Australia has been estimated at $22 billion AUD [4]. In an ageing population, falls are increasingly common presentation and reason for hospitalisation. Elderly females are more prone to falls than men with increased risks of associated injuries and polytrauma.
There is scant data on female maxillofacial fractures internationally, yet alone in Australia, that focuses specifically on the risk profile and clinical outcomes. The Women and Children’s Hospital and Royal Adelaide Hospital is the main tertiary and quaternary referral service for paediatric and adult facial fractures in South Australia, Australia, with care extending to parts of Northern Territory, rural New South Wales and Victoria. Care is delivered through inpatient, ambulatory care and outreach services treating approximately 600 patients yearly [5]. The main objective was to analyse the epidemiology of facial fractures in South Australian females with particular focus on vulnerable groups and differences in clinical outcomes. This study represents the first statewide comprehensive analysis of the South Australian experience focusing on the patterns and trends of facial trauma and clinical outcomes in women.
Methods
A retrospective institutional review was conducted at the Women and Children’s Hospital and Royal Adelaide Hospital, Adelaide, Australia, from January 2012 to January 2017 for all patients who sustained facial fractures. Patients were assessed by a plastic surgical trainee and/or craniofacial surgeon at the time of presentation. According to the national census in 2016, approximately 1.7 million people lived in South Australia with 50.7% females [6]. The data was retrospectively reviewed from medical records, progress notes, imaging, and operative notes. Ethics approval was granted from the Human Research and Ethics Committee [HREC/17/RAH/402]. The primary objective was to analyse epidemiological trends of facial fractures in the female population. The secondary objective was to determine differences in trends and clinical outcomes amongst younger females (18–65 years) and elderly (65 years and above).
The following recorded parameters were analysed for this project as per our standardised registry:
Social demographics: age, age groups, indigenous status, and alcohol intoxication.. Age groups included < 18 years, 18–25, 26–35, 36–45, 46–55, 56–65, and 65 + (elderly).
Socioeconomic parameters and timing of injury: season, timing of injury, postcode, socioeconomic index for areas (SEIFA), and Australian statistical geography standard (ASGS) scale. The Socioeconomic Indexes for Areas (SEIFA) is a measure of disadvantage created by the Australian Bureau of Statistics (ABS) who defines relative socioeconomic advantage and disadvantage in terms of people’s access to material and social resources and the ability to participate in society. The SEIFA score was assessed from the patient’s postcode and analysed in conjunction with the ABS framework. The score of the residential statistical local area of each person was used as the area-based composite measure of socioeconomic status from the index of relative socioeconomic advantage and disadvantage (IRSAD) [7]. Overseas adults were excluded from the socioeconomic parametric analysis. The Australian Statistical Geography Standard (ASGS) defines Remoteness Areas into five classes of relative remoteness across Australia: major cities, inner regional, outer regional, remote, and very remote. This index uses distances to population centres as the basis for quantifying service access [8]
Aetiology and type of injury: mechanism of injury (assault, road traffic accident (RTA), sports, falls, work, other), type of injury [9] (orbit, orbitozygomatic, mandible, zygomatic arch, nasal, naso-orbito-ethmoidal (NOE), frontal sinus, panfacial, dentoalveolar middle cranial base, posterior cranial base), multiple fractures, recurrent fractures, and associated injuries.
Treatment, complications, and hospitalisation: treatment [conservative, surgery, open reduction internal fixation (ORIF)], complications, re-operations, and length of stay (LoS).
A statistical analysis using SPSS (Version 26, IBM Corporation, Armonk, NY, USA) was computed for continuous variables assessing the relationship between linear data and correlation based on a level of significance set at P value of 0.05. Continuous variables were expressed as mean, median and standard deviation (SD). A paired independent t test and Pearson chi test were conducted to assess differences between young females (18–65 years) and elderly females for continuous and categorical variables. A binary and multivariate logistic regression analysis was conducted to analyse odds between age groups expressed as odds ratios (ORs) and 95% confidence intervals (95% CI).
Results
Demographic
Of 2559 patients from 2012 to 2017, there were 583 females who presented with facial fractures (22.8%) (Table 1). The average age was 48.6 years with a bimodal distribution (Shapiro–Wilk test < 0.001) peaking at 25–35 years (13.6%) and 65 + years (32.4%). The indigenous female population rate of facial fractures was 6.7% ranging from 3–54 years (Shapiro Wilk test = 0.799). Indigenous females were 19.5 years younger than non-indigenous females (30.5 vs 49.9, P < 0.0001). The most prevalent season for facial fractures was autumn (26.6%). Alcohol consumption at the time of injury was reported in 66 patients (11.3%). The most frequented time for presentation to an emergency department occurred in the morning and afternoon (29.5%), respectively. The most disadvantage socioeconomic group had the highest incidence of facial fractures (34.0%). Approximately two thirds of persons from the study population largely represented facial fractures from major cities.
Approximately half the cohort had a fall-related facial fracture, followed by assault (26.2%), and sports (10.3%). Orbitozygomatic fractures were the most common type of facial fracture (30.2%) with the midface representing over half the cases. Multiple fractures were identified in 97 patients (16.6%). One hundred and eighty-eight (32.2%) patients had an associated injury attributed mainly by falls resulting in neurological injury (n = 36), soft tissue injury (n = 36), cardiovascular events (n = 31), upper and lower injuries (n = 26, n = 26), and other injuries. There were fourteen patients with a cervical spine fracture (seven falls, four assaults, two RTAs, and one sport). There were 18 recurrent fractures. The operative rate was 61.6% and the remaining 38.4% were managed conservatively with serial reviews. There were twenty-seven (4.6%) post-operative complications related to infection, plate exposure, enophthalmos, nerve injury, and analgesic opioids. There were eleven re-operations (five orbits, three mandibles, and three panfacials). The mean hospital LoS was 3.8 days (SD ± 15.0).
Younger females and elderly females
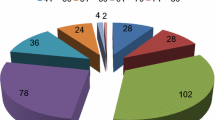
Younger females had a higher proportion of alcohol-related facial trauma compared to elderly females (18.8% vs 2.1%, Table 2). However, there was a higher proportion of non-alcohol-related trauma from assaults than alcohol-related assaults (72.5% vs 27.5%, P < 0.001, Fig. 1). There was a significant difference in proportions between types of fractures from assaults between young and elderly females with the midface commonly afflicted [orbit, n = 51; orbitozygomatic, n = 27] than mandible (n = 36, Table 2). The elderly had higher proportion of facial fractures in winter, largely from falls, with increased odds of 1.9 compared to younger women (Table 3). Young women from the most and more disadvantaged socioeconomic areas had greater proportions of facial fractures compared to elderly counterparts. Elderly women from the least disadvantage areas had 2.9 times the risk of a facial fracture compared to younger counterparts. Elderly women from major cities were 1.8 times more likely to have a facial fracture than younger counterparts. With increasing remoteness, younger women were more likely to have a facial fracture compared to their counterparts.

Assaults amongst women by age groups and alcohol intoxication
Almost all (92.6%) elderly facial fractures were from falls with an increased risk of 34.7 times compared to younger women. Younger women had significantly greater proportions of assaults, sports, RTA, and animal-related facial fractures (Table 2). The mandible and orbitozygomatic fractures represented half the facial fractures amongst younger women. Elderly women were 42.4% less likely to have a mandibular fracture, but 2.5 times more likely to have an orbitozygomatic fracture. Younger women had greater proportions for multiple fractures (19.7% vs 11.6%) with elderly women 53.7% less likely. Associated injuries were present in almost half the elderly with a 2.6 times risk compared to younger women. Younger women had higher incidences of surgical intervention (52.6% vs 14.3%) with elderly women 15.0% less likely compared to their counterparts. Multivariate analysis for surgery when accounted for ASGS, ISRAD, seasons, alcohol, facial fractures, and aetiology showed elderly women were 44.3% less likely to have surgery compared to younger women (Table 3). Post-operative complications showed a trend towards statistical significance with younger women having greater proportions compared to elderly (6.5% vs 2.6%, P = 0.057).
Discussion
In South Australia, the three most vulnerable groups for facial trauma in females include young women related to assault, elderly women with falls, and indigenous women with disproportionately higher rates. An Irish study of 1190 female facial fractures reported peaks at 20–39 years and 70–89 years with the midface commonly afflicted [10], whereas Gerber’s British study reported peaks at 20–29 years and a third over 60 years caused mainly by accidents, assaults, and then falls [11]. The aetiology of facial fractures has changed over the decades and influenced heavily by sociocultural values and laws pertaining to the country. In the 1990s, RTA was reported as the most common cause of facial fractures in the USA for women, followed by assaults, with the mandible frequently afflicted [12]. Our previous work on mandibular fractures compared the aforementioned period to the present with stark differences: assaults (45% vs 35%), RTA (27% vs 6.8%), and falls (22% vs 43.7%) [13, 14]. Consistent with the literature [15,16,17], a bimodal age distribution for young and elderly women who present with facial trauma can assist surgeons in establishing a risk profile and management plan.
Younger women, notably 26–35 years, from lower socioeconomic backgrounds had higher rates of non-alcohol-related assaults and multiple fractures compared to elderly women. This is consistent with the national data on assaults reporting 56 cases per 100,000 population with the 30–34 age group most frequently affected [18]. There was an alarming proportion of non-alcohol-related assaults for women involving partners, family members, and/or friends. Retrospective analysis of the data did not consistently document the circumstances of the events as the victim often did not disclose exact details. In some cultures, it has been reported that assaulted females may provide inadequate documentation because of sociocultural reasons indirectly causing harm [19]. Arosarena’s study recognised patterns of assaults to where intimate partner violence was more likely to have zygomatic complex fractures, orbital blow-out fractures, and intracranial injuries, whereas women assaulted by unknown or unidentified assailants were more likely to have mandible fractures [20]. Our experience identified an overall higher proportion of midface than mandibular fractures (78 vs 36), but indigenous proportions were inversely affected (12 vs 9) suggesting the mechanism of injury and assault were different. One of the challenges in clinical history and assessment is the validity of sensitive information to distinguish between partners or unknown assailants. Nevertheless, if features are suggestive of domestic violence in vulnerable groups like younger women, indigenous women, or pregnant women, providing appropriate referral and supportive services should be simultaneously offered at the time of trauma assessment.
The profile of violence against women has been associated with degree of suburban living, education, marital status, and residency with higher rates for younger ethnic minority women [21,22,23]. We recognised two distinct groups of socioeconomic disadvantage where younger women from most disadvantaged areas had higher rates of injury from assault, but older women from least disadvantaged areas were 2.9 times more likely to have fall-related facial fractures (Table 2). Australian and New Zealand national data have identified twice the rate of injury for indigenous and even greater in remote areas compared to non-indigenous [24,25,26,27]. We similarly reported two trends where elderly women from major cities had 1.8 times the rate compared to younger women, but with increasing remoteness younger women, notably indigenous women, had higher risks of facial fractures largely from assaults. Oberdan’s mandibular study affirmed these findings with alarmingly high facial fractures in indigenous females from assaults with higher levels of recurrent trauma than non-indigenous [28]. In a younger indigenous population, alcohol and assault were more likely to result in facial fractures, whereas sport or fall-related facial fractures had higher rates in non-indigenous women. We have previously identified that indigenous people aged 26–35 years were 1.5 times more likely to have a facial fracture with greater rates in remote areas; they experienced higher rates of mandibular fractures with higher rates of operative intervention, post-operative complications, and extended LoS compared to non-indigenous women [29].
Falls are a common cause of injury in the elderly with highest incidences in developing countries compared to developing countries [21, 30, 31] A Japanese study on falls reported the mandible was commonly afflicted with an overall conservative approach compared to younger women (55.0% vs 86.4%) [32]. Our multivariate analysis showed that elderly women were 44.3% less likely to have surgery compared to younger women (14.3% vs 52.6%) with no difference in complications or re-operations. This is reflective of the difference in aetiology and facial fractures experienced amongst age groups where the midface was commonly afflicted from falls and assaults, respectively. Seasonality is an important contributor to the presentation of facial fractures often relating to warmer weather, outdoor activities, and frailty. A decade review of Chinese maxillofacial fractures identified an increase in trauma for females during summer with more frequent condylar fractures than men [33]. In contrast, we established elderly women were twice as likely to have a fall-related facial fracture during winter compared to younger women (Table 3). The impact of seasonality is seldom established in maxillofacial studies, as it is multifactorial with frailty, environmental hazards, and malnutrition superimposed on comorbidities and sociodemographic factors [34, 35]. With an older population commonly presenting with falls, associated injuries are more frequent and directly impact LoS (OR = 2.3). The rate and types of associated injuries differ depending on the mechanism such as orthopaedic secondary to RTA (23.2%) [36], neurological secondary to RTA (19.2%) [37], and soft tissue injuries from falls (67.6%) [38]. Our rate was 32.2% with the elderly 2.3 times more likely to have different types of associated injuries compared to younger females. The most common types of injuries for the elderly included cardiovascular, neurological, and upper limb injury, whereas younger women suffered soft tissue, neurological, and upper and lower limb injuries.
The operative rate was significantly higher in younger females attributed mainly by the mandible, whereas fall-related fractures in elderly females resulted in orbitozygomatic fractures managed non-operatively (OR = 0.443, Table 3). Sport is another popular growing subgroup that was increasingly common amongst younger females with disproportionate rates compared to men. Females aged 36–55 years have approximately five times the risk of a sport-related facial fracture principally from cycling, whereas males have decreasing risks of approximately 20% compared to 18–25 year olds [39]. Other studies with comparable demographic and fracture profiles have also reported similar operative rates [40]; however, we have further established significant risk profiling for elderly women with mandibular and orbitozygomatic fractures (OR = 0.424, OR = 2.493, Table 3). Operative intervention varies greatly depending on the fracture and age, which we generally favoured conservative measures for elderly women balancing comorbidities, function, and quality of life. With a higher operative rate amongst younger women, there was a trend to statistical significance to suggest higher post-operative complications reflective of the type of facial fracture (mandible vs orbitozygomatic).
This is the first statewide and national paper that presents a risk profile analysis for facial fractures in women providing the clinician with key socioeconomic parameters and clinical points. The three major vulnerable groups discussed highlight important aspects of assessment and intervention with facial trauma. Opportunities for government and community-based programs targeted for domestic violence and fall prevention is key to a growing elderly population. There are salient differences in aetiology and presentation compared to men that surgeons and trainees should incorporate in their assessment and management of maxillofacial fractures for young women and the elderly. Key limitations include retrospective and selection bias, however, future studies on differences in associated injuries would provide more insight into prevention and management. Ongoing surveillance for trends in women, particularly indigenous, would provide invaluable indicators of clinical outcomes and standard of service.
Conclusion
Younger females are more likely to have mandibular fractures with operative intervention from assaults, whereas elderly females principally present with fall-related facial fractures with higher rates of associated injuries. Surgeons should employ a holistic risk profile assessment for women who present with facial trauma in their trauma service.
Data availability
The data cannot be shared due to ethics.
Code availability
IBM SPSS V 26.0 was used for statistical analysis.
References
Jayaraj R, Thomas M, Thomson V, Nagel T (2012) High risk alcohol-related trauma among the Aboriginal and Torres Strait Islanders in the Northern Territory. Subst Abuse Treat Prev Policy 7(1):33
Kieser J, Stephenson S, Liston PN, Tong DC, Langley JD (2002) Serious facial fractures in New Zealand from 1979 to 1998. Int J Oral Maxillofac Surg 31(2):206–209
Karmali S, Laupland K, Harrop AR, Findlay C, Kirkpatrick AW, Winston B et al (2005) Epidemiology of severe trauma among status Aboriginal Canadians: a population-based study. CMAJ 172(8):1007–1011
KPMG 2016. The cost of violence against women and their children in Australia: final report May 2016. Canberra: Department of Social Services. Viewed 15 November 2020, https://www.dss.gov.au/women/publications-articles/reducing-violence/the-cost-of-violence-against-women-and-their-children-in-australiamay- 2016.
Snell B, Grave B (2018) The multidisciplinary management of complex facial trauma at Royal Adelaide Hospital. Australas J Plast Surg Sep.24;1(2):31–2.
Australian Bureau of Statistics. 2016 Census: Aboriginal and/or Torres Strait Islander Peoples QuickStats. Website: https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/IQS4. Accessed 23/2/2021.
Australian Bureau of Statistics. Information paper. An introduction to Socio- Economic Indexes for Areas (SEIFA) 2006(2039.0). ABS: Canberra, Australia, 2008.
Australian Bureau of Statistics, Australian Statistical Geography Standard (ASGS): Volume 5 - Remoteness Structure, July 2016. Accessed 12/1/2021: https://www.abs.gov.au/ausstats/abs@.nsf/Latestproducts/1270.0.55.005Main%20Features15July%202016?opendocument&tabname=Summary&prodno=1270.0.55.005&issue=July%202016&num=&view=
David DJ, Simpson DA (1995) Craniomaxillofacial trauma: a system of multidisciplinary management by members of the Australian craniofacial unit. Churchill Livingstone, Edinburgh
Ogunbowale A, Costello L, McCormack D, Ekanayake K, Kearns GJ (2021) Maxillofacial fractures in females: a 5-year retrospective review. Ir J Med Sci. Feb 22.
Gerber B, Ahmad N, Parmar S (2009) Trends in maxillofacial injuries in women, 2000–2004. Br J Oral Maxillofac Surg 47(5):374–377
Huang V, Moore C, Bohrer P, Thaller SR (1998) Maxillofacial Injuries in Women. Ann Plast Surg 41:482–484
Diab J, Grave B, Flapper W, Anderson P, Moore MH (2021) Patterns of mandibular fractures in South Australia: epidemiology, treatment, and clinical outcomes. Journal of Craniofacial surgery.
Edwards TJ, David DJ, Simpson DA, Abbott AA (1994) Patterns of mandibular fractures in Adelaide, South Australia. Aust N Z J Surg 64(5):307–311
Verma S, Chambers I (2015) Update on patterns of mandibular fracture in Tasmania. Australia Br J Oral Maxillofac Surg 53(1):74–77
Ellsberg M, Jansen HA, Heise L, Watts CH, Garcia-Moreno C (2008) WHO Multi-country Study on Women’s Health and Domestic Violence against Women Study Team. Lancet 371(9619):1165–1172
Stevens JA, Sogolow ED (2005) Gender differences for non-fatal unintentional fall related injuries among older adults. Inj Prev 11:115–119
Australian Institute of Health and Welfare 2017. Hospitalised assault injuries among women and girls fact sheet. Cat. no. INJCAT 184. Canberra: AIHW.
Alghamdi S, Alhabab R, Alsalmi S (2017) The epidemiology, incidence and patterns of maxillofacial fractures in Jeddah city, Saudi Arabia. Int J Oral Maxillofac Surg 46:32–36
Arosarena OA, Fritsch TA, Hsueh Y, Aynehchi B, Haug R (2009) Maxillofacial injuries and violence against women. Arch Facial Plast Surg 11(1):48–52
Mayrink G, Araújo S, Kindely L, Marano R, Filho ABM, de Assis TV, Jadijisky M Jr, de Oliveira NK (2021) Factors associated with violence against women and facial trauma of a representative sample of the Brazilian population: results of a retrospective study. Craniomaxillofac Trauma Reconstr 14(2):119–125
Conceição LD, da Silveira IA, Nascimento GG, Lund RG, da Silva RHA, Leite FRM (2018) Epidemiology and risk factors of maxillofacial injuries in Brazil, a 5-year retrospective study. J Maxillofac Oral Surg 17(2):169–174
da Nóbrega LM, Bernardino ÍM, Barbosa KGN, e Silva JAL, Massoni ACLT, d’Avila S, (2017) Pattern of oral-maxillofacial trauma from violence against women and its associated factors. Dent Traumatol 33:181–188
Australian Institute of Health and Welfare 2018. Aboriginal and Torres Strait Islander adolescent and youth health and wellbeing 2018: in brief. Cat. no. IHW 198. Canberra: AIHW.
Koorey AJ, Marshall SW, Treasure ET, Langley JD (1992) Incidence of facial fractures resulting in hospitalisation in New Zealand from 1979 to 1988. Int J Oral Maxillofac Surg 21:77–79
Kieser J, Stephenson S, Liston P, Tong D, Langley J (2002) Serious facial fractures in New Zealand from 1979 to 1998. Int J Oral Maxillofac Surg 31:206–209
AIHW: Pointer SC (2019) Hospitalised injury among Aboriginal and Torres Strait Islander people, 2011–12 to 2015–16. Injury research and statistics series no. 118. Cat. no. INJCAT 198. Canberra: AIHW
Oberdan W, Finn D (2007) Mandibular fractures in Far North Queensland: an ethnic comparison. Australia and New Zealand J Surg 77:73–79
Diab J, Grave B, Flapper WJ, Anderson PJ, David DJ, Moore MH (2021) South Australian facial trauma: a population analysis of social economic deprivation and facial fractures-part one. Australas J Plast Surg 4(2):22–35
Abdul Rahman N, Ramli R, Abdul Rahman R et al (2010) Facial trauma in geriatric patients in a selected Malaysian hospital. Geriatr Gerontol Int 10:64–69
Peel NM, Kassulke DJ, McClure RJ (2002) Population based study of hospitalised fall related injuries in older people. Inj Prev 8:280–283
Ito R, Kubota K, Inui A et al (2017) Oral-maxillofacial trauma of a geriatric population in a super-ageing country. Dent Traumatol 33:433–437
Zhou HH, Liu Q, Yang RT, Li Z, Li ZB (2015) Maxillofacial fractures in women and men: a 10-year retrospective study. J Oral Maxillofac Surg 73(11):2181–2188
Duckham RL, Procter-Gray E, Hannan MT et al (2013) Sex differences in circumstances and consequences of outdoor and indoor falls in older adults in the MOBILIZE Boston cohort study. BMC Geriatr 13:133
Werning JW, Downey NM, Brinker RA, Khuder SA, Davis WJ, Rubin AM, Elsamaloty HM (2004) The impact of osteoporosis on patients with maxillofacial trauma. Arch Otolaryngol Head Neck Surg 130(3):353–356
Roccia F, Bianchi F, Zavattero E, Tanteri G, Ramieri G (2010) Characteristics of maxillofacial trauma in females: a retrospective analysis of 367 patients. J Craniomaxillofac Surg 38(4):314–319
Huang V, Moore C, Bohrer P, Thaller SR (1998) Maxillofacial injuries in women. Ann Plast Surg 41(5):482–484
Costa MC, Cavalcante GM, Nóbrega LM, Oliveira PA, Cavalcante JR, d’Avila S (2014) Facial traumas among females through violent and non-violent mechanisms. Braz J Otorhinolaryngol 80(3):196–201
Diab J, Grave B, Flapper WJ. et al. (2021) Sport-related maxillofacial fractures in South Australia. Eur J Plast Surg.
Ogunbowale A, Costello L, McCormack D, Ekanayake K, Kearns GJ. (2021) Maxillofacial fractures in females: a 5-year retrospective review. Ir J Med Sci. Feb 22.
Acknowledgements
We would like to acknowledge the members of the craniofacial, plastics and oral maxillofacial unit whom provided ongoing support in the project and collection of the data.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions There was no funding for this project.
Author information
Authors and Affiliations
Contributions
Both authors have contributed substantially to the following aspects of the present study: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be submitted.
Corresponding author
Ethics declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration. This project has been approved by the Human Research Ethics Committee at South Australia [HREC/17/RAH/402].
Consent to participate
Informed consent was obtained from the parents or legal guardians. Patient consent has been obtained for data registry.
Consent to publication
Consent for publication was permitted from the local human research ethics committee at South Australia.
Conflict of interest
Jason Diab and Mark Moore both declare to have no conflicts of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Diab, J., Moore, M.H. Patterns and characteristics of maxillofacial fractures in women. Oral Maxillofac Surg 27, 459–468 (2023). https://doi.org/10.1007/s10006-022-01085-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10006-022-01085-8