
Abstract
Adolescents often look to their peers for emotional support, so it is critical that they are prepared to take on a supportive role, especially during a health crisis. Using a randomised controlled trial (ISRCTN99248812, 28/05/2020), we tested the short-term efficacy of an online training programme to equip young people with skills to support to their peers’ mental wellbeing during the COVID-19 pandemic. In June 2020, one-hundred UK adolescents (aged 16–18) recruited through social media were randomly allocated (1:1) to immediate 5-day peer support training or a wait-list, via an independently generated allocation sequence. Primary outcomes were indicators of ability to help others (motivation, perceived skills, frequency of help provided, compassion to others and connectedness to peers). Secondary outcomes included emotional symptoms, mental wellbeing, and indicators of agency (civic engagement and self-efficacy). We also collected qualitative reports of participants’ experience. Assessments were completed at baseline and 1 week post randomisation (primary endpoint), and up to 4 weeks post randomisation (training group only). The training increased support-giving skills, frequency of providing support, compassion and peer connectedness (medium–large-effect sizes), but not motivation to provide support, 1 week post randomisation, compared to controls. Gains in the training group were maintained 4 weeks post randomisation. Training also improved adolescents’ mental health and agency, and qualitative reports revealed further positive outcomes including increased self-care and empowerment. Leveraging digital platforms that are familiar to young people, peer support training has the potential to enable adolescents to support their own and their peers’ mental wellbeing during a health crisis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The COVID-19 outbreak has had a major psychosocial impact on the lives of young people [1, 2]. The challenges posed by the pandemic have given rise to feelings of lack of control, loneliness and anxiety, and significant increases in mental ill-health [3, 4], posing an urgent need for targeted interventions. To ensure their specific needs are addressed, it is critical that young people are involved as active stakeholders in priority setting, as well as in the design, testing and delivery of interventions, rather than as passive ‘recipients’ of support [5, 6].
In March 2020, as the pandemic accelerated, we conducted patient and public involvement (PPI) consultations with adolescents aged 14–25 from two UK-based Young People’s Advisory Groups (YPAGs) to help set priorities for intervention research. The young people consulted expressed a clear desire to be active stakeholders in easing the mental health burdens of the pandemic. While many aspired to provide emotional support to their friends and peers during this time, they felt that they lacked the skills to do so. In direct response to these expressed needs, we focused this project on peer support, aiming to equip young people with the skills to reach out to their peers and support their mental health and wellbeing.
Peer support is defined as the process of help-giving and help-receiving between individuals who share characteristics or lived experiences [7]. In the context of mental health, it has been framed as an approach that foregrounds values-led relationships [8, 9]. Evidence indicates that having positive peer relationships in adolescence predicts greater wellbeing [10]. However, evidence from intervention studies is mixed: while some studies suggest positive outcomes for supported peers, others indicate null results (see [11, 12] for systematic reviews of online and school interventions, respectively). This inconsistency may be partly due to the training young people receive to carry out the role [13].
Peer support training programmes are rarely examined in isolation. Existing studies, exclusively school-based, suggest that training brings marginal improvements to peer supporters’ self-confidence [12]. However, to our knowledge, only one study evaluated outcomes directly related to adolescents’ ability to help others. The results showed social connectedness and support-giving increased among adolescent peer supporters who received training, compared to controls [14]. Peer support training also has the potential to heighten young people’s ‘agency capabilities’ (i.e. their ability to pursue valued outcomes, such as making a difference to the community) [15] and bring benefits for their own mental wellbeing, but these outcomes remain largely unexplored. To develop effective peer support interventions, it is first critical to develop and evaluate training to prepare young people for the role. Moreover, COVID-19 restrictions and disruptions have magnified the need for virtual training models [16].
Goals and aims
Our study addresses the need for peer support training programmes targeted to the COVID-19 pandemic, and the lack of evidenced outcomes of peer supporter training. The project focused on young people aged 16–18 years, an age group experiencing significant disruption to their education or early working life during the COVID-19 pandemic [17]. We partnered with Youth Era, a charity specialising in online peer support for youth (www.youthera.org), and YPAG set up for this project, to design an online training course to equip young people with skills to support the mental health and wellbeing of their friends and peers. The course equipped young people to provide peer support to their communities and social networks in naturally occurring instances, outside of professional services.
Through a randomised controlled trial, we investigated whether being trained as a peer supporter promotes:
-
i.
young people’s ability to support others during the COVID-19 pandemic, including motivation to provide peer support, perceived support-giving skills, frequency of support provided, compassion to others, and connectedness to peers,
-
ii.
their own mental wellbeing and reduces emotional symptoms, and
-
iii.
their sense of agency, including self-efficacy and civic engagement
We investigated short-term benefits, relative to a wait-list control, and explored young people’s experiences of the online training and self-reported impacts.
Methods
Co-producing research with young people
A YPAG was formed specifically for this project, comprising six young people aged 16–28 (2 males, 4 females). Young people were recruited from three existing advisory groups that contributed to our initial PPI work: The McPin Young People’s Network (https://mcpin.org/young-peoples-network/), the NeurOX YPAG (https://oxneurosec.com/involvement/young-peoples-advisory-group-ypag/) and the Lancet Young Leaders for Global Mental Health (https://globalmentalhealthcommission.org/youth-campaign/). The YPAG informed all aspects of the study, from design to dissemination (Table S1). The McPin Foundation led the youth involvement, with support from the Oxford Neuroscience, Ethics and Society Group.
Recruitment
The study protocol was approved by the University of Oxford Interdivisional Medical Sciences Ethics Committee (R69810/RE001). Participants were recruited through posters and advertisements on social media, from May 23 to May 28, 2020. To help overcome potential sampling bias, we used three different adverts on social media, including an illustration and two posters (one depicting a female and another a male model); adverts were set up to target adolescents aged 16–18 years, anywhere in the UK. To be eligible, participants needed: to be aged 16–18, UK resident, have sufficient English and ability to complete training and measures independently, consent to randomisation, and access to Wi-Fi, computer, camera and speakers. Interested participants completed an online “Expression of Interest Form”. Those identified as potentially eligible were invited for a short call with the training instructors to confirm eligibility and suitability for the course. Once confirmed, written informed consent was obtained and participants completed baseline measures. Recruitment ceased once the target sample size was achieved.
Randomisation and masking
After baseline measures were completed, participants were randomly assigned to immediate training or wait-list control in a 1:1 ratio. The random allocation sequence was computer-generated by an independent researcher who had no contact with research participants. Post-randomisation questionnaires were circulated via email by a researcher blind to allocation. Participants completed all assessments independently online.
Procedures
Participants randomised to the training arm completed the peer support training course between the 8 and 12 June 2020. Both arms were reassessed 1 week post randomisation, and wait-list participants were then offered the peer support training (22–26th June). Three weekly follow-up assessments of the primary outcomes were circulated to the training arm only. All participants received a certificate of course completion and a £15 voucher for completing study measures.
Peer support training
The training course, titled Uplift Peer Support Training, was designed by Youth Era with input from the YPAG and researchers. The course was delivered via Zoom by a team of specialist Youth Era peer supporters over 5 consecutive days (4 h/day). Interactive and informative sessions were delivered by peer support experts to the full group of 50 youth, and sharing and hands-on activities were mostly delivered in small groups of 7 via breakout rooms or WhatsApp, each led by a group facilitator. Participants were asked to keep their cameras on during the Zoom sessions, and encouraged to participate actively in the WhatsApp discussions. The course included modules on establishing rapport, active listening, grief and trauma, confidentiality, self-care, coping strategies, crisis management, signposting and referrals, and making a difference to the community. Examples and activities reflected challenges of the pandemic from the perspective of UK youth. Further information about training content is available from authors on request.
Quantitative outcomes
Assessment points were baseline (before randomisation), 1-week post randomisation (primary endpoint), and 2, 3 and 4 weeks post randomisation (training arm only). Measures assessing all outcomes were administered at baseline and the primary endpoint in both arms; training arm follow-ups included measures of primary outcomes. To characterise the sample, participants reported their age, gender and ethnicity, and completed the Family Affluence Scale [18], an adolescent self-report measure of socioeconomic status.
Primary outcomes
Our primary outcomes were the following indicators of the ability to provide support to peers during the COVID-19 pandemic among both arms 1 week post randomisation: (i) motivation to provide support; (ii) perceived support-giving skills; (iii) frequency of support provided; (iv) compassion towards others; and (v) connectedness to peers.
Motivation to provide support, perceived support-giving skills and frequency of support provided were each established using corresponding items from the Adolescent Social Connection Coping During COVID Scale [19] (motivation: 4 items; total score: 4–24; skills: 4 items, total score: 4–28; frequency: 4 items, total score: 4–28). Compassion towards others was assessed using the Compassion to others-Engagement subscale (6 items; total score: 6–60) and the Compassion to others-Action subscale (4 items; total score: 4–40) [20]. Minor amendments were made to the wording of the Action subscale items to assess perceived ability to take actions, rather than to actual behaviours which participants were unlikely to have had the opportunity to engage in within the short-assessment period (Table S2). Connectedness to peers was determined using the Inclusion of Other in the Self [21] single item pictorial measure of closeness (scored 1–7).
Secondary outcomes
Secondary outcomes included mental wellbeing and emotional symptoms, and indicators of agency (self-efficacy and civic engagement) among both arms 1 week post randomisation. The Warwick–Edinburgh Mental Wellbeing Scale [22] (WEMWS; 14 items; total score: 14–70), and the Strengths and Difficulties Questionnaire-Emotional symptoms subscale [23] (SDQ-E; 5 items, total score: 0–10) were used to assess mental wellbeing and emotional symptoms, respectively. Self-efficacy was established with the General Self-Efficacy Scale [24] (GESS; 10 items, total score: 10–40) and civic engagement was assessed using the Attitudes and Behaviour subscales of the Civic Engagement Scale [25] (CES-Attitudes; 8 items, total score: 8–56; CES-Behaviour; 6 items; total score 6–42). We made minor amendments to the wording of the CES-Behaviour items to assess perceived ability to engage in behaviours, rather than actual behaviours (Table S2). Further, secondary outcomes assessed in the training arm only included indicators of the ability to provide support (motivation, skills, frequency and connectedness to peers) and who participants reported helping (e.g., friends), up to 4 weeks post randomisation.
Qualitative outcomes
Open-ended questions assessed participants’ perceived impact of training, use of peer support skills and intentions to use peer skills in the future in the training arm. Participants were asked (i) whether the training impacted their life in any way, and prompted to describe positive and negative impacts (1 week post randomisation); (ii) to provide an example of how they used their “peer support skills” over the past week (2, 3 and 4 weeks post randomisation); and (iii) if and how they planned to use what they learnt from the training in their “life moving forward” (1 week and 4 weeks post randomisation).
Statistical analysis
Sample size
The target sample size was determined to provide 80% power to detect a meaningful difference between the two groups on primary and secondary outcomes. We assumed that we would retain 90% of participants to 1 week post randomisation, and the sample of 100 provided 80% power and (2 sided) 5% significance levels to detect differences between training and control groups of F = 0.3 (medium-effect size).
Analysis
An analysis plan detailing all pre-specified statistical analyses was published (http://www.isrctn.com/ISRCTN99248812), before analyses were conducted. Baseline characteristics were summarised for each group and the total sample using descriptive statistics. A series of analysis of covariance (ANCOVAs) were used to compare training and control groups on each primary and secondary outcome 1 week post randomisation, adjusting for corresponding baseline score, gender and age. Partial eta-squared was used to measure the effect size for each outcome. To assess the robustness of the results, ANCOVAs were repeated using pre–post change scores and participants aged 16 only. The results of these sensitivity analyses were similar to the main analyses and did not alter the conclusions so are not reported here.
To examine indicators of the ability to provide support up to four weeks post randomisation for the training group, we used a series of repeated measures analysis of variance. We used the last observation carried forward approach to manage missing follow-up data. To assess the impact of these missing data, we repeated these analyses using participants with complete data only (n = 39). The results of these complete data analyses were similar to the main analyses and did not alter the conclusions, so are not reported here.
To maintain an overall type 1 family error rate of 0.05 for the primary outcomes, a Bonferroni adjustment method was used and a p value < 0.0083 (0.05/6) was considered statistically significant for each primary outcome. Secondary outcomes were treated as exploratory and so no adjustment for multiple testing was made [26, 27] and p < 0.05 was considered statistically significant for each secondary outcome.
Statistical analyses were done with SPSS version 26. The trial was registered on the ISCRN registry, number ISRCTN99248812, on 28 May 2020 (https://www.isrctn.com/ISRCTN99248812).
Qualitative analysis
To analyse the training group’s responses to open-ended questions, we used a directed content-analysis approach [28], guided by the impact and outcomes theorised as relevant. The YPAG co-produced the initial framing framework and co-analysed the data. The framework was iterated and refined into a final version after discussion meetings. The scheme was validated by two independent coders and reliability calculated on 25% of the data, adopting a threshold of κ = 0.6 (substantial agreement [29]). Disagreements were resolved by discussion between original coders or adjudication by a third reviewer. The presence/absence of each code was recorded for each response. We separately analysed responses to questions related to: (a) impact of training, (b) use of peer support skills and (c) intentions to use skills. We also checked whether overarching categories emerged across the three sections.
Results
Participants
We randomised 100 participants to either training (n = 50) or wait-list control (n = 50). Participants completed baseline assessments (30th May–3rd of June) and 1-week post-randomisation assessments (12–16th June 2020) during a lockdown period in the UK (with face-to-face teaching suspended from 20 March to 15 June 2020). Recruitment and retention rates are displayed in Fig. 1. All training group participants attended all training sessions, with the exception of one participant who missed one session. There were no dropouts in the 1-week assessment; however, one participant was lost to follow-up and others missed one or two follow-up questionnaires.

Progress of participants through the trial
Baseline demographic characteristics are displayed in Table 1. Across both groups, most participants were aged 16 or 17 years (> 90%), self-identified as female (> 80%), and lived in England (> 80%). Both groups were ethnically diverse (< 50% White British), with similar levels of family affluence.
Quantitative results
Results from the ANCOVAs comparing training and wait-list groups on each primary and secondary outcome 1 week post randomisation, controlling for corresponding baseline score, gender and age are detailed in Table 2.
Primary outcomes
Ability to provide support
There was no difference between the training and the wait-list groups on motivation to provide support to others (F1,95 = 2.60, p = 0.110). However, there was a significant effect of training on perceived support-giving skills (F1,95 = 15.83, p < 0.0001, ηp2 = 0.14) and how often participants provided support to others (F1,95 = 13.99, p < 0.0001, ηp2 = 0.13). Self-reported compassion towards others was also significantly greater among those who received training, compared to wait-list controls, both in relation to engaging with others and perceived ability to take action (F1,95 = 12.03, p = 0.001, ηp2 = 0.11 and F1,95 = 23.21, p < 0.0001, ηp2 = 0.20, respectively). The training group also reported feeling significantly more connected to their peers than wait-list controls (F1,95 = 19.48, p < 0.0001, ηp2 = 0.17). With the exception of motivation, effect sizes across indicators of ability to provide support to others ranged from medium to large.
Secondary outcomes
Mental wellbeing and emotional symptoms
We also found evidence of an effect of training on self-reported mental wellbeing and emotional symptoms. Those who received training reported significantly better mental wellbeing and significantly lower negative emotional symptoms compared to the wait-list, with large- and medium-effect sizes, respectively (F1,95 = 62.51, p < 0.0001, ηp2 = 0.40, F1,95 = 8.26, p = 0.005, ηp2 = 0.08).
Agency (self-efficacy and civic engagement)
Relative to the wait-list group, the training group reported significantly greater self-efficacy, with a medium-effect size (F1,95 = 7.91, p = 0.006, ηp2 = 0.08). Compared to wait-list controls, the training group also reported more positive civic attitudes and greater perceived ability to engage in civic behaviours, each with a large-effect size (F1,95 = 25.82, p < 0.0001, ηp2 = 0.21 and F1,95 = 20.86, p < 0.0001, ηp2 = 0.18, respectively).
Training group follow-up
Participants most frequently reported helping close others: all training participants reported helping friends at least once over the follow-up period; 88% (n = 44) helped family members; 80% (n = 40) helped other peers and 38% (n = 19) helped young people they did not know. Figure 2 displays self-reported motivation to provide support to others, perceived support-giving skills and how often participants provided support to others at each assessment point among the training group. Repeated measures ANOVAs indicated perceived support-giving skills and how often participants provided support differed significantly across assessment points (F2.65, 129.88 = 6.13, p = 0.001; F2.82, 138.08 = 10.39, p < 0.001), and both increased from baseline to 4 weeks post randomisation (p = 0.018 and p = 0.006, respectively), although motivation at 4 weeks did not significantly differ from baseline (p = 0.49). The training group’s connectedness to their peers also differed across assessments (F4, 196 = 8.41, p < 0.0001), and participants reported feeling significantly more connected to their peers at 4 weeks compared to baseline (p = 0.001).

Indicators of ability to provide support among the training group from baseline to 4 weeks post randomisation; †no significant difference between baseline and 4 weeks; *significant difference between baseline and 4 weeks
Qualitative results
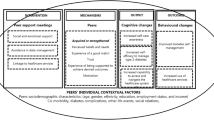
Across the three open-ended questions, three main clusters emerged from participants’ responses: supporting and connecting with peers, empowerment and civic engagement, and self-care. Figure 3 provides a summary of the results; additional quotes and frequencies are provided in Table S3.

Impact of training, application of peer support skills and intended future use; content analysis main codes
Perceived impact of training
Increased ability to support and connect with peers was the main impact of the training. In particular, three-quarters of participants indicated that the training increased their ability and confidence in supporting others. For instance, Holly (all names are pseudonyms) expressed that the training made her “feel more prepared to help my friends and peers when they need me.” Two-fifths indicated that the training helped them build stronger relationships. For Paige, the training made her more “present within my friendships and relationships.”
About a third mentioned that the training made them feel empowered and more confident in themselves (“it made me see that I am more powerful and I can really make a change”; Rebecca), and had renewed aspirations to help the community (“I'm hoping to help my community increase the number of diverse Peer Supporters”, Charlotte). Equally frequent were references to increased self-awareness and self-care (“It has made me … more aware and more capable to deal with my own emotions and problems”; Stephanie).
Negative impacts of the training were rarely mentioned; only three participants indicated the training caused some fatigue (“made me tired due to lots of socialising and concentrating”; Kirsty), but no further negative experiences or harms were reported.
Use of peer support skills
All participants reported at least one instance of using the skills to emotionally support others. Many young people described situational challenges peers faced, including lockdown, exam stress and family conflict (e.g., “I helped a friend who was struggling with being isolated in COVID-19 lockdown and just had a few conversations with them”; Georgia). Participants also reported specific emotional difficulties among their peers, and often mentioned techniques used to help others cope. Laura, for instance, supported a friend who “was having a panic attack and I tried to help her to calm down by suggesting that she did things which would distract her, I was referring to the emergency action plan which is something I learnt on the course.” Lastly, participants described using active listening skills; Jade, for example reported that “when having meaningful conversations I remembered to use a gentle tone and the mirroring technique.”
Two-fifths mentioned how their skills had been useful in helping the community and communicating around civic responsibilities. For example, Chloe reported that she used the skills “to help to educate others about the importance of understanding and fighting for the rights of those less privileged.” In addition, about a third mentioned using the skills for self-care and setting personal boundaries. Anna reported that “rather than shooting into panic mode, I reasoned with myself to think logically rather than emotionally, which had helped me calm down”.
Intention to use the skills
All but one participant reported planning to use their new skills in the future, both immediately after the course (100%) and at the last follow-up (98%). The vast majority described plans to use the skills to support others (e.g., “I will try and help more of my peers even after all of this COVID-19 stuff has died down”; Georgina). Roughly half mentioned aspirations to improve their relationships and communication skills (e.g., “I plan to use some of the techniques like mirroring to help build stronger rapport with people”; Paul).
Many participants also reported a motivation to advocate for mental health and plans to contribute to community wellbeing. Paige reported she hoped to “set up a student organisation in my school, aiming to empower and educate younger students — with a focus on battling misogyny and sexual assault.” Participants also planned to continue to focus on self-care; for example, Samantha planned to “balance what I want to do and my own mental health.” Finally, an additional code identified in this section related to academic or professional aspirations, mentioned by about a fifth of participants. Alexandra, for instance, reported that “I hope to be a doctor so these skills will be extremely useful.”
Discussion
This RCT documents benefits of an online peer support training model for young people during the COVID-19 pandemic across a range of outcomes. Although both the training and control participants expressed high motivation to support their peers, those who received training felt more able and likely to do so. These gains were maintained in the training group 3 weeks following course completion. The training group also felt more connected to other young people their age than controls. They most commonly reported using their skills to support friends with emotional difficulties and help them feel heard and appreciated. Critically, the training also improved participants’ own self-reported emotional symptoms and mental wellbeing, self-efficacy and civic engagement, relative to controls. Free text responses mirrored these findings, with qualitative analysis indicating that the training fostered support-giving skills, self-care, feelings of empowerment and a desire to help the community. Encouragingly, 3 weeks after training, participants continued to express intentions to apply the learned skills, not only to support themselves and others, but also to advocate for better mental health.
These results speak to the potential value of structured, targeted courses to train young people to provide peer support. While most peer support training courses are delivered face-to-face, our findings provide preliminary evidence of the potential benefits of delivering such courses online, leveraging platforms that are familiar to young people. This offers the potential to increase reach, and allows safe delivery during crises such as the COVID-19 pandemic [16]. Equipping young people with support-giving skills seemed to enable them to translate their motivation to help others into action. Although we did not provide youth with a structured opportunity to support others after the course, participants reported spontaneously offering help to their peers and family members, and felt more confident in doing so. Some indicated aspirations to pioneer peer support initiatives (e.g., discussion groups in schools) as a result of this training. It is possible that this opportunity to focus pro-socially on others, and to actively contribute to the pandemic response, alleviated feelings of uncertainty and honed young people’s sense of purpose during the pandemic, which may have contributed to the observed improvements in wellbeing [30, 31]. Our qualitative results also indicated that peer support training encouraged participants to practise self-care tactics in their daily life, which possibly also improved their wellbeing [32, 33].
Limitations and future directions
To ascertain the short-term benefits of the course before a larger trial, our sample size was limited, and only immediate outcomes were assessed against a control group. Short-term follow-up assessments were evaluated in the training group only; therefore, it is difficult to determine whether the changes observed are due to the peer support training or other external factors. Future research should include a larger sample, and investigate potential medium- to long-term benefits of peer support training compared to controls. It would also be important to examine potential benefits for the supported peers and wider community. This is particularly relevant in the context of restrictions easing and young people returning to school and other social environments.
Our sample presented some diversity in ethnicity and socioeconomic status but lacked male representation. In addition, our sample was biased towards individuals who were already highly motivated to help others, which may have influenced their commitment to the course and positive outcomes. Approaches to widen participation co-directed through youth involvement will be important in future studies, and help ascertain whether gains are similar when training is delivered universally (e.g., through schools or primary care). Similarly, our sample size was not sufficient to explore outcomes among different subgroups of young people, for example outcomes among young people with high versus low wellbeing at baseline, and this will be an important consideration for future trials. Future research should also aim to compare the effects of peer support training and active controls. Similarly, is it also important to identify the mechanisms through which peer support training improves wellbeing, self-efficacy and civic engagement in young people, and what aspects of the course best predict these outcomes. A more comprehensive understanding of what works can help target training courses to particular populations and outcomes.
Lessons learned and consequences for the future
Whilst the principle of youth involvement in designing research and interventions is increasingly accepted, young people's participation in priority setting is still limited. In this project we worked with groups of young people to identify how they wished to contribute to the pandemic response and co-created an online peer support training programme to facilitate this contribution. The active involvement of young people in setting the research agenda, and throughout the project, was key to meeting their aspirations and addressing their specific needs. Peer support training led to improvements in young people’s ability to help others, with additional benefits to their mental health and wellbeing and dimensions of agency (self-efficacy and civic engagement). These encouraging results suggest that online peer support training is a valuable tool to promote emotional support-giving skills in emergency situations such as COVID-19, paving the way for effective peer support interventions for youth wellbeing. Our research process, including mapping aspirations and supporting adolescents to take an active role in responding to a health crisis, provides a valuable model for co-creating effective research and interventions during times of instability and uncertainty.
Availability of data and material (data transparency)
The quantitative dataset is available at https://osf.io/c2tk3/. Qualitative data are available upon reasonable request by emailing the corresponding author.
Code availability (software application or custom code)
Available upon request.
References
Children’s Commissioner (2020) Stress among Children in England during the Coronavirus Lockdown. London, UK. https://www.childrenscommissioner.gov.uk/wp-content/uploads/2020/09/ cco-stress-among-children-in-england-during-the-coronavirus-lockdown.pdf
Dewa LH, Crandell C, Choong E et al (2021) CCopeY: A mixed-methods coproduced study on the mental health status and coping strategies of young people during COVID-19 UK Lockdown. J Adolesc Heal 68:666–675. https://doi.org/10.1016/j.jadohealth.2021.01.009
Nearchou F, Flinn C, Niland R et al (2020) Exploring the impact of COVID-19 on mental health outcomes in children and adolescents: a systematic review. Int J Environ Res Public Health 17:8479. https://doi.org/10.3390/ijerph17228479
Young Minds (2021) Coronavirus: Impact on young people with mental health needs. London, UK https://youngminds.org.uk/media/4350/coronavirus-report-winter.pdf
Pavarini G, Lyreskog D, Manku K et al (2020) Promoting capabilities for young people’s agency in the COVID-19 outbreak. Child Adolesc Ment Health. https://doi.org/10.1111/camh.12409
Singh I, Pavarini G, Juma D et al (2020) Correspondence: Multidisciplinary research priorities for the COVID-19 pandemic. The Lancet Psychiatry 7:e36. https://doi.org/10.1016/S2215-0366(20)30228-5
Mead S, Hilton D, Curtis L (2001) Peer support: A theoretical perspective. Psychiatr Rehabil J 25:134–141. https://doi.org/10.1037/h0095032
Side by Side Research Consortium (2017) Developing peer support in the community: a toolkit. London, UK
Watson E, Meddings S (2019) Peer support in mental health. London, UK: Red Globe Press
Steiner RJ, Sheremenko G, Lesesne C et al (2019) Adolescent connectedness and adult health outcomes. Pediatrics 144:e20183766. https://doi.org/10.1542/peds.2018-3766
Ali K, Farrer L, Gulliver A et al (2015) Online peer-to-peer support for young people with mental health problems: a systematic review. JMIR Ment Heal 2:e19. https://doi.org/10.2196/mental.4418
King T, Fazel M (2021) Examining the mental health outcomes of school-based peer-led interventions on young people: A scoping review of range and a systematic review of effectiveness. PLoS ONE 16:e0249553. https://doi.org/10.1371/journal.pone.0249553
Gopalan G, Lee SJ, Harris R et al (2017) Utilization of peers in services for youth with emotional and behavioral challenges: A scoping review. J Adolesc 55:88–115. https://doi.org/10.1016/j.adolescence.2016.12.011
Wyman PA, Brown CH, LoMurray M et al (2010) An outcome evaluation of the sources of strength suicide prevention program delivered by adolescent peer leaders in high schools. Am J Public Health 100:1653–1661. https://doi.org/10.2105/AJPH.2009.190025
Sen A (1993) Capability and well-being. In: Nussbaum M, Sen A, Eds. The quality of life. Oxford: Clarendon Press 30–53 https://doi.org/10.1093/0198287976.001.0001
Torous J, Jän Myrick K, Rauseo-Ricupero N et al (2020) Digital mental health and COVID-19: using technology today to accelerate the curve on access and quality tomorrow. JMIR Ment Heal 7:e18848. https://doi.org/10.2196/18848
Mansfield K, Jindra C, Geulayov G, et al (2021) Self-reported wellbeing and sample characteristics in a survey of 19000 school pupils during the first UK COVID-19 school closures. https://doi.org/10.31234/osf.io/gtbfm
Torsheim T, Cavallo F, Levin KA et al (2016) Psychometric validation of the revised family affluence scale: a latent variable approach. Child Indic Res 9:771–784. https://doi.org/10.1007/s12187-015-9339-x
Pfeifer J (2020) adolescent social connection & coping during COVID-19 Questionnaire (ASC)
Gilbert P, Catarino F, Duarte C et al (2017) The development of compassionate engagement and action scales for self and others. J Compass Heal Care 4:4. https://doi.org/10.1186/s40639-017-0033-3
Aron A, Aron EN, Smollan D (1992) Inclusion of Other in the Self Scale and the structure of interpersonal closeness. J Pers Soc Psychol 63:596–612. https://doi.org/10.1037/0022-3514.63.4.596
Tennant R, Hiller L, Fishwick R et al (2007) The Warwick-Edinburgh mental well-being scale (WEMWBS): development and UK validation. Health Qual Life Outcomes 5:63. https://doi.org/10.1186/1477-7525-5-63
Goodman R (2001) Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry 40:1337–1345. https://doi.org/10.1097/00004583-200111000-00015
Luszczynska A, Scholz U, Schwarzer R (2005) The general self-efficacy scale: multicultural validation studies. J Psychol 139:439–457. https://doi.org/10.3200/JRLP.139.5.439-457
Doolittle A, Faul AC (2013) Civic engagement scale. SAGE Open 3:215824401349554. https://doi.org/10.1177/2158244013495542
Feise RJ (2002) Do multiple outcome measures require p-value adjustment? BMC Med Res Methodol 2:8. https://doi.org/10.1186/1471-2288-2-8
Schulz KF, Grimes DA (2005) Multiplicity in randomised trials I: endpoints and treatments. Lancet 365:1591–1595. https://doi.org/10.1016/S0140-6736(05)66461-6
Hsieh H-F, Shannon SE (2005) Three approaches to qualitative content analysis. Qual Health Res 15:1277–1288. https://doi.org/10.1177/1049732305276687
O’Connor C, Joffe H (2020) Intercoder reliability in qualitative research: debates and practical guidelines. Int J Qual Methods 19:160940691989922. https://doi.org/10.1177/1609406919899220
Ballard PJ, Ozer EJ (2016) Implications of youth activism for health and well-being. Contemp Youth Act Adv Soc Justice United States 1–31. https://www.researchgate.net/publication/303895913
Hayhurst JG, Hunter JA, Ruffman T (2019) Encouraging flourishing following tragedy: The role of civic engagement in well-being and resilience. New Zeal J Psychol 48(48):71–79
de Mooij B, Fekkes M, Scholte RHJ et al (2020) Effective components of social skills training programs for children and adolescents in nonclinical samples: a multilevel meta-analysis. Clin Child Fam Psychol Rev 23:250–264. https://doi.org/10.1007/s10567-019-00308-x
Bjørnsen HN, Espnes GA, Eilertsen MEB et al (2019) The relationship between positive mental health literacy and mental well-being among adolescents: implications for school health services. J Sch Nurs 35:107–116. https://doi.org/10.1177/1059840517732125
Acknowledgements
This publication arises from activities funded by the Higher Education Innovation Fund and ESRC Impact Acceleration Account through the University of Oxford’s COVID-19: Economic, Social, Cultural, & Environmental Impacts – Urgent Response Fund (PI: GP). IS is supported by the Wellcome Trust (104825/Z/14/Z and 203132/Z/16/Z); GP and VB are supported by a Wellcome Trust investigator award to IS (104825/Z/14/Z); IS and VB are further supported by the NIHR Oxford Health Biomedical Research Centre [IS-BRC-1215-20005]. For the purpose of open access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission. We thank Youth Era, in particular, Tia Barnes, Jammie Gardner and Martin Rafferty for leading the co-design and delivery of the Uplift Peer Support Training. We thank Timothy Knowlson, Nina Kruglikova, Geoffrey Mawdsley, Lindsay Dewa, James Okulaja, the NeurOX Young People’s Advisory Group, the McPin Foundation Young People’s Network and the Lancet Young Leaders for Global Health for their input. This work was presented as a poster at the 2020 Grand Challenges Annual Meeting. The funder of the study had no role in study design, data collection, data analysis, data interpretation, decision to publish or writing of the report. Youth Era gave minimal input into the study design, had no access to the data or the survey platform for the duration of the study, and were not involved in data analysis, decision to publish or paper writing.
The following are members of the Peer Support Young People's Advisory Group: Ellie Brooks-Hall, Ashley Foster-Estwick, Damian Omari Juma, Peter Lewis, Lucy Power, Maia Rogers.
Funding
This work was funded by the Higher Education Innovation Fund and ESRC Impact Acceleration Account through the University of Oxford’s COVID-19: Economic, Social, Cultural, & Environmental Impacts – Urgent Response Fund; Wellcome Trust [104825/Z/14/Z and 203132/Z/16/Z]; and NIHR Oxford Health Biomedical Research Centre [IS-BRC-1215–20005].
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethics approval
Approval was obtained by the University of Oxford Interdivisional Medical Sciences Ethics Committee (R69810/RE001).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
All participants consented to the publication of their data.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pavarini, G., Reardon, T., Hollowell, A. et al. Online peer support training to promote adolescents’ emotional support skills, mental health and agency during COVID-19: Randomised controlled trial and qualitative evaluation. Eur Child Adolesc Psychiatry 32, 1119–1130 (2023). https://doi.org/10.1007/s00787-021-01933-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-021-01933-0