
Abstract
Selective mutism (SM) is an anxiety disorder (prevalence 1–2%), characterized by the consistent absence of speaking in specific situations (e.g., in school), while adequately speaking in other situations (e.g., at home). SM can have a debilitating impact on the psychosocial and academic functioning in childhood. The use of psychometrically sound and cross-culturally valid instruments is urgently needed.
The aim of this paper is to identify and review the available assessment instruments for screening or diagnosing the core SM symptomatology. We conducted a systematic search in 6 databases. We identified 1469 studies from the last decade and investigated the measures having been used in a diagnostic assessment of SM. Studies were included if original data on the assessment or treatment of SM were reported. It was found that 38% of published studies on SM reporting original data did not report the use of any standardized or objective measure to investigate the core symptomatology. The results showed that many different questionnaires, interviews and observational instruments were used, many of these only once. The Selective Mutism Questionnaire (SMQ), Anxiety Disorders Interview Schedule (ADIS) and School Speech Questionnaire (SSQ) were used most often. Psychometric data on these instruments are emerging. Beyond these commonly used instruments, more recent developed instruments, such as the Frankfurt Scale of SM (FSSM) and the Teacher Telephone Interview for SM (TTI-SM), are described, as well as several interesting observational measures. The strengths and weaknesses of the instruments are discussed and recommendations are made for their use in clinical practice and research.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
Selective mutism (SM) is a psychiatric condition characterized by persistent failure to speak in specific social situations (usually in school) despite speaking adequately in other situations (usually with close family members). The disorder was categorized as an anxiety disorder in the DSM-5 and ICD-11 [1, 2] (see Table 1 for the current diagnostic criteria for selective mutism), based on multiple studies showing an overlap in behavioral characteristics and etiological factors in children with SM and high comorbidity with other anxiety disorders, specifically social anxiety [3, 4].
SM is not as rare as once believed, with reported prevalence rates between 0.7 and 2% [5,6,7]. The broad prevalence range may be attributed to differences in sampling strategies, such as the inclusion of clinical or community samples, sample characteristics such as age range or immigrant status, or to the diagnostic methods used. SM usually has an onset between 2 and 4 years, but often remains unrecognized until the child enters school [8]. If left untreated, SM can take a chronic course and affect social–communicative capacity, mental health and quality of life in adolescence and adulthood [9,10,11,12,13].
Given the interference with social, communicational and academic development and wellbeing, it is important to identify and treat SM timely and accurately. Valid and reliable diagnostic instruments are needed to further advance research into the behavioral characteristics, possible subgroups, treatment efficacy and long-term outcome of individuals with SM. Several diagnostic instruments have been developed over the last two decades that can be used to classify SM and/or to investigate the severity of symptoms in different contexts. Recommendations for a thorough diagnostic assessment have been described [14] and include information from multiple informants, e.g., parental information, teacher information, direct assessment of the child’s behavior and self-reported information from the child if possible. Some children are able to complete self-report measures or communicate about their difficulties via parents, drawings or cards [14, 15]. The diagnostic instruments for the assessment of SM include questionnaires, structured diagnostic interviews and observational measures to be used in clinical settings, the classroom or in daily life situations. These measures were designed for, or used in studies on, screening, diagnostic assessment and classification or the assessment of symptom severity and treatment progress. Obviously, a full diagnostic assessment involves more than examining speaking behavior alone, and includes the medical and developmental history of the child, family history, parenting and family functioning, life events, the examination of other behavioral difficulties or comorbid psychiatric symptoms and direct assessment of cognitive, academic and language skills [14, 15]. In addition to the core characteristics of SM, e.g., the amount of speaking behavior in different situations, a broader assessment is needed to differentiate SM from other disorders, to investigate comorbid disorders or associated developmental difficulties, and to examine familial and contextual factors that may play a role in the development or persistence of the disorder.
In clinical practice, valid and reliable measures are crucial for an accurate diagnosis which is an essential step for providing effective treatment and evaluate treatment progression [14]. In research, the use of standardized measures improves the comparability of studies. However, currently in clinical practice and in research, different instruments are used to classify SM and to investigate symptom severity, or sometimes no specific measures are used that specifically target SM. Therefore, the aim of this systematic review is to describe and identify which assessment tools have been used for the purpose of screening, classification or monitoring treatment outcomes on speaking behavior and SM symptomatology in in the past decade. In this review we focus on the core criterion of SM, i.e., speaking behavior (criterion A of the DSM-5 classification). In addition, methodological strengths and limitations of the assessment instruments will be reviewed to provide recommendations to the usefulness of the instruments for clinical practice and research.
Methods
For this review, we selected all articles about SM that reported original data in the last decade.
Search strategy and selection criteria
An electronic literature search was performed by an information specialist of a University Medical Library. The following databases were searched three times, in January 2019, March 2020 and July 2021: Embase, Medline (Ovid), PsycINFO, Web of Science, Cochrane Central and Google Scholar. Titles and abstracts were searched with a combination of keywords and subcategories, shown in Table 2.
Studies were included in this review if they (1) were published in English between 2010 and July 2021 and accessible in full-text format, (2) reported original data on the assessment of SM.
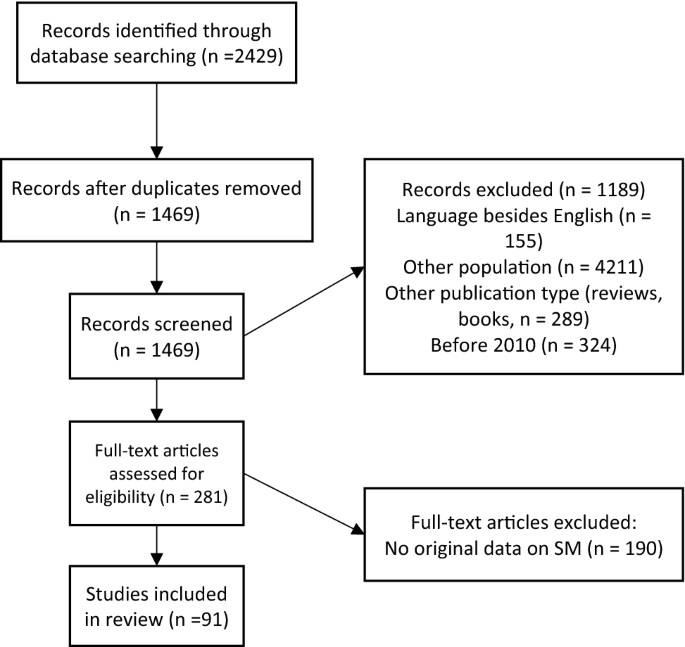
We excluded studies that did not discuss SM, as well as studies that did not report original data on SM, such as reviews and meta-analyses. Doctoral theses, conference papers or abstracts were also excluded. A detailed overview of the study selection process is displayed in Fig. 1. For the psychometric description of the instruments, we searched for source articles describing the instrument and its psychometric properties through reference lists.
Flowchart
In line with the Prisma Guidelines [16], two authors (CRP and JE) independently screened the titles and abstracts of the retrieved citations. A third author (MdJ) was consulted in case the screeners had different ratings or doubt to include or exclude a paper, thereafter consensus was established. In case of doubt on the basis of the abstract screening, the article was included for full-text screening. Next, all selected full-text articles were screened to verify the selection. The data collection from relevant studies was performed using a pre-designed extraction spreadsheet.
Results
Search results
Figure 1 shows that (after correction for duplication) 1469 studies were identified. After screening, 1189 studies were excluded because based on the title and abstract the inclusion criteria were not met. Thereafter, the remaining 281 articles were screened in full text and 91 studies were included in the review.
Descriptive data
From the 91 articles reporting original data on the assessment and/or treatment of children with SM, 35 articles (38%) did not report use of objective or standardized measures for SM symptomatology. In these articles the diagnosis was often based on a clinical assessment. In 56 articles, one or more standardized measures were used to classify SM and/or quantify severity (see Table 3).
In total, these 56 articles describe the use of 29 different instruments (see Table 4).
Selective mutism assessment measures
Questionnaires
The Selective Mutism Questionnaire (SMQ [17]) was used most often (in 32 articles, see Table 3, Study ID: 1–5, 7–10, 12–15, 17–21, 24, 25, 29, 30, 33, 36, 38, 40, 41, 46, 48, 53–56).
The SMQ is a parent rating scale, measuring the severity of SM rated speaking behavior in different contexts (17 items) and impediment associated with nonspeaking behavior (six additional items). Items are scored on a 4-point Likert scale ranging from 0 (never speaking) to 3 (always speaking). The SMQ was developed and validated in the United States, in 3- to 11-year-old children with and without SM. Exploratory Factor Analyses revealed a three-factor structure; speaking in the context of: school (6 items), home/family (6 items), and community (5 items) [17, 18]. The three-factor structure was confirmed in an independent study but only after removing 4 items [18]. Internal consistency was good–excellent in the original sample (α = 0.97 total scale, subscales respectively α = 0.97, 0.88, 0.96) [17] and moderate–excellent in above-mentioned independent clinical and community sample, based on the 13-item version (α = 0.78 total scale, subscales α = 0.91, 0.65, 0.73) [18]. The internal consistency of the total scale ranged from α = 0.70 to 0.91 in subsequent samples in the US [19,20,21]. The SMQ was translated into different languages. Studies in the Norwegian population reported internal consistencies ranging from α = 0.77 to 0.93 on the Total scale and α = 0.68 to 0.90 on the subscales [22, 23]. A recent study by Oerbeck et al. reported internal consistency of α = 0.96 on the total scale in a clinical sample and a typically developing control group [24]. The internal consistency of the total SMQ scale in a Spanish clinical sample was found to be α = 0.90 [25]. Additionally, the three-factor structure as found by Bergman et al. [17] was replicated. Furthermore, the SMQ has been translated and used in Italy [26, 27], Israel [28, 29] (reported Cronbach’s α = 0.77), and Turkey ([30] Cronbach’s α = 0.87).
Convergent validity of the SMQ was indicated by significant correlations with two (social) anxiety scales (SASC-R and MASC-P) for children and with the ADIS severity score (r = − 0.67) [17]. Letamendi et al. found moderate correlations between the 13-item SMQ total severity scale and the interference scale and the clinician rated ADIS severity score (respectively, r = 0.42 and r = 0.48) [18]. Discriminant validity was supported by a weak non-significant correlation with the Harm Avoidance, Separation Anxiety, and Physical Symptoms subscales of the MASC [17]. However, in a previous study, the total SMQ scale did not differentiate 14 SM children from 9 children with social anxiety disorder [31]. Finally, the SMQ was found to be sensitive to treatment change in small samples of children with SM [17, 32,33,34]. Incremental validity of the 13-item SMQ was supported by a significant additional explained variance in SM diagnosis over Anxious/Depressed Syndrome Scale of the CBCL [18].
The School Speech questionnaire (SSQ [5]) is a modified version of the SMQ measuring speech at school as rated by the teacher. It was used in 11 publications (see Table 3, Study ID: 3, 4, 7, 9, 17–20, 25, 38, 54). The original version comprised 11 items, but 2 items related to nonverbal communication with low item-total correlations were dropped. Internal consistency of the 9-item version was α = 0.96 [5]. In subsequent studies, 6–10 item versions have been used, but authors provide no explanation for the decision to use certain items. The first 6 items are identical to the parent-rated SMQ school items and form the Total severity scale. The items are scored on the same 0–3-point scale as the SMQ. The additional items address nonverbal behavior and interference with academic and social functioning and are often not used in analyses [21,22,23, 33,34,35,36]. Internal consistency ranged between α = 0.76 and 0.81 in Canada and the US, and between α = 0.64 and 0.84 in Norway. The SSQ was found to be sensitive to treatment change [19, 21, 22, 34].
The Frankfurter Scale of SM (FSSM [37]) was validated in a German-speaking clinical sample (SM n = 95, social phobia n = 74, internalizing problems n = 46), and a community sample (n = 119) for use in children ages 3–18 (see Table 3, Study ID: 52). The FSSM was used in subsequent publications (see Table 3, Study ID: 44, 45, 49). The FSSM has three age versions: 3–7, 6–11 and 12–18 years. The questionnaire is freely available online in English, German, Norwegian and Finnish. It comprises a diagnostic scale (10 items, yes or no) and a severity scale (41 items in the 3–7 version; 42 items in the 6–11 and 12–18 version). The severity subscale measures speaking in three contexts: school, public and home (5-point Likert scale; 0 = speaks without problems, to 4 = speaks not at all). Internal consistency of the diagnostic scale was α = 0.90 (FSSM 3–7, FSSM 12–18) and 0.92 (FSSM 6–11). Internal consistency of the total severity scale was excellent (α = 0.98) in the total (clinical and community) sample and good (α = 0.88) in the SM group.
Exploratory factor analysis of the severity scale showed a one-factor solution. ROC curve analyses of the diagnostic scale revealed an optimal cutoff score to differentiate the SM group from the group with social phobia, other internalizing disorders and the non-clinical group. Areas under the curve were between 0.94 and 0.99 for the three age versions, indicating satisfactory to excellent discriminant validity. Convergent validity based on correlations with Evaluation of the Socially interactive Communication in Mutism scale developed by Hartmann [38] showed significant correlations with the total score on the severity scale (r = 0.48–0.72), indicating good convergent validity.
The Speech situations questionnaire (SpSQ-P and SpSQ-T) was used in 4 publications (see Table 3, Study ID: 27, 31, 42, 43). The questionnaire for parents comprises 15 items and measures the extent to which the child speaks to different people in different settings including home, school, and community. It is scored on a 3-point scale (0 = never talks, 1 = whispers, 2 = talks normally). The teacher version is scored on the same scale and comprises 7 items asking about speech in different situations and people at school. Internal consistency of the SpSQ-P was found to be good in the original sample of 58 children with SM and 52 community control children (Cronbach’s α = 0.82) ([39], and excellent in subsequent studies α = 0.92 [40,41,42]. Internal consistency of the SpSQ-T was excellent (Cronbach’s α = 0.95–0.96 [40, 42]. No further psychometrics are reported on these instruments.
The Verbal and Nonverbal Social Interactions Skills [39] was used in one study (see Table 3, Study ID: 27) [40]. The scale was derived from the SSRS-Parent and SSRS-Teacher, first described by Cunningham and colleagues [39] and comprises three subscales: verbal social skills, nonverbal social skills, and nonverbal cooperation. The internal consistency in the clinical and community samples of Carbone [37] and Cunningham [38], respectively, ranged from Cronbach’s a = 0.58 to 0.78, a = 0.71 to 0.83, and a = 0.78 to 0.85 for the three scales in parents. The same three subscales were computed in teachers and internal consistency ranged between Cronbach’s a = 0.80–0.90, a = 0.86–0.94, and a = 0.88–0.92 for these three scales. No further psychometrics have been reported.
The Parental questionnaire on mute behavior [43] was used in one study (see Table 3, Study ID: 47[43]). The questionnaire comprises 18 items. Speaking behavior was rated on a 5-point Likert scale. The items covered social situations in the family context, neighborhood, and in public. In the study, the instrument was used at four time points within one year and the internal consistency for the total scale was good to excellent (ranging from: α = 0.89 to 0.95 over the four time points). No further psychometrics have been reported.
The Evaluation of the Socially interactive Communication in Mutism (ESCM [38]) is a 23-item questionnaire measuring verbal and nonverbal communication in different situations, rated on a 3-point Likert-type scale (0 = uninhibited communication, 1 = communication moderately stressful or on request only, 2 = stressful/selectively mute). It has been used in two studies (see Table 3, Study ID: 22, 52) to investigate symptom severity in the study of Gensthaler et al. [37] and to investigate improvement over time and treatment outcome in the case study of Plener et al. [44]. The ESCM is online available in German and English. No further psychometrics have been reported.
Other questionnaires were used in six studies. Each questionnaire was used only once and the instruments have been minimally described. Mitchell and Kratochwill [45] used a Severity of Behavior Form derived from items from the Parent/School Screening Questionnaires [46]. The form was used on a weekly basis to investigate change over time, but the items were not described in the article. The Dortmund Mutism Screening [43] is a 17-item preschool teacher-reported questionnaire used in one study by Starke [43] and is available in German only. In the study of Klein et al., a therapist-created questionnaire for DSM-IV SM criteria was used, but not further described (see Table 3, Study ID: 35)[47].
A few studies report the use of self-report measures. Oerbeck et al. [23] described using an adaptation of the Inventory of Life Quality in Children and Adolescents (ILC) [48] where children could rate their difficulties with speaking at school/outside/home on a Likert scale (1 = very easy, 3 = mixed, 5 = difficult). No further psychometrics have been reported. In two studies, the SMQ was used as a self-report measure. Muris et al. [49] described that children rated the SMQ items on a four-point scale (0 = totally disagree, 1 = somewhat disagree, 2, somewhat agree, 3 = totally agree), reporting Cronbach’s α = 0.82 in a non-clinical sample. The study of Muris et al. also used the Youth Anxiety Measure for DSM-5 (YAM-5). The YAM-5 is a questionnaire for children aged 8 to 18 years and their parents. The self-report version is answered on a Likert scale (0 = never, 1 = sometimes, 2 = often, and 3 = always). Muris et al. reported Cronbach’s α = 0.41 for the SM segment and a correlation of r = -0.63 for the SM segment and the SMQ [49]. In the study of Milic et al. [50], the SMQ-Child (SMQ-C) was introduced as a 20-item measure of frequency of speech, using a two stage pictorial response scale. Internal consistency is reported for the subscales (α = school 0.82, home/family 0.67, public/social 0.80), referring to an unpublished doctoral thesis. No further psychometrics have been reported.
Clinical interviews
The Anxiety Disorders Interview Schedule—SM section (ADIS [51]) was used in 23 publications (see Table 3, Study ID: 3, 5–7, 9, 11, 14, 15, 17–20, 23–25, 29, 34, 36, 38, 48, 51, 53, 55). The ADIS is a clinician-administered, semi-structured interview to assess the presence of a broad range of anxiety, mood and behavioral disorders, consisting of a parental and a child interview version. The SM subsection is part of the parental interview and encompasses 8 items, questioning the speaking behavior of the child and the school functioning (i.e., dysfunction related to difficulties with speaking at school). Parents rate on a 9-point scale (i.e., 0–8) to what extent the symptoms interfere with the daily life of the child. The interviewer rates the level of impairment on the same 9-point scale (Clinician Severity Rating, CSR), with a CSR of 4 or more, indicating a clinically significant problem. The interview has good reliability and validity ([29] [52]). The ADIS (adapted to the DSM-IV criteria) is frequently used in studies on SM to assess comorbid (anxiety) disorders. However, specific information about the psychometric properties of the ADIS to differentiate SM from other anxiety disorders has not been reported. The SM section is mostly used to assess the classification SM for inclusion in the study. In seven studies, the CSR was used as a measure of severity or outcome measure [19, 21, 27, 29, 34, 53,54,55]. In these studies, the ADIS was sensitive to treatment change. Good inter-rater reliability between the ADIS and the clinical global impression scales was found [29].
The Kiddie Schedule for Affective Disorders and Schizophrenia–Present and Lifetime Version (K-SADS-PL[56]) has been used in studies into SM to assess comorbidity. Until recently SM could not be investigated with the K-SADS-PL. The latest version (K-SADS-PL-DSM-5; [57]) has a SM supplement. The reliability and validity of the SM supplement was found to be excellent in a Turkish study that included 10 children with SM (see Table 3, Study ID: 56) [30]. In addition to the studies identified in our search, a recently published Japanese research group (n = 4) found good criterion validity, adequate construct validity and excellent convergent validity was for the SM supplement. Due to the very small sample size, these results should be interpreted with great caution [58].
The Preschool Age Psychiatric Assessment (PAPA [59]) is a clinical DSM-screening interview used in two studies (see Table 3, Study ID: 26, 50)[60, 61]. SM is screened using a single item rated as 0 = SM is absent, 1 = limited speech/volume or 2 = absence of speech in specific situations. The interview is available online: Preschool Age Psychiatric Assessment 2.0.7 (duke.edu).
The Teacher Telephone Interview (TTI-SM [62]) is described and evaluated by Martinez et al. (see Table 3, Study ID: 53) [63] to assess SM and anxiety in the school. The authors refer to an unpublished article of Tannock et al. [62] as a source of the interview. The TTI-SM is a standardized phone interview that can be conducted with teachers to include the perspective of the teacher in the assessment of SM. The TTI-SM comprises five subscales: SM (15 items), Verbal/Nonverbal Communication with Teachers (14 items), Verbal and Nonverbal Communication with Peers (10 items), School and Classroom Social Participation Behaviors (8 items), and Externalizing Behaviors (7 items). Martinez et al. [63] only evaluated the SM subscale and the School and Classroom Social Participation Behaviors subscale. The items are shown in their article (p. 90–91). After exclusion of four items from the SM subscale due to low item-subscale correlations, the internal consistency of the 11-item subscale was excellent (Cronbach’s α = 0.96). Convergent validity of the TTI-SM subscale was indicated by significant correlations with the SMQ (r = 0.72 and r = 0.85 for the mother and father reported SMQ). Discriminant validity was supported by low–moderate non-significantly correlation with the total SASC-R and MASC total scores, although there were some correlations on subscale levels. Concurrent validity was supported by significant differences on the TTI-SM subscale between 33 children with SM and 10 children with mixed anxiety disorders. Predictive validity was supported by a significant correlation between the TTI-SM subscale and the ADIS classification [63].
Other interviews were briefly described and are summarized here. A German online open access DSM-interview (Kinder-DIPS, [64]) was used in three studies. This interview is not available in other languages (see Table 3, Study ID: 28, 32, 52)[65]. The SM Brief Child and Family Phone Interview (SM-BCFPI, [66]) was used by Edison et al. [67] and Poole et al. [68] (see Table 3, Study ID: 31, 43). This is a SM-specific version of the BCFPI. As far as known to the authors, the BCFPI does not encompass a scale for SM. It has not been described how the BCFPI was adjusted to assess SM in their study.
Observation measures
The SM-Behavioral Observation Task (SM-BOT [69]) was used in one treatment evaluation study (see Table 3, study ID: 7) [34]. To refer to the SM-BOT, the authors of this study cite Carpenter et al. [70], who described the SM-BOT as an instrument to assess parent–child interactions. In this context, Carpenter et al. refer to an unpublished manuscript from Kurtz [69], without further clarification of this instrument. In a publication of Catchpole [34], the SM-BOT is coded on the basis of an interaction task involving parent–child interactions in the presence and absence of a stranger and child-stranger interaction tasks. The child’s behavior is coded as having: (a) no interaction with the stranger, (b) non-verbal interaction only, or (c) non-verbal and verbal interaction. In sum, no further description or psychometric information on the SM-BOT was found.
The SM-Social Communication Comfort Scale (SM-SCCS [71]): is used in one study (see Table 3, Study ID: 14) [54]. The SM-SCCS is a clinician-administered observation scale that can be retrieved from the website of the Smart Center [71]. Klein et al. [54] describe the instrument for use in the therapy sessions, for assessing therapist-child interactions and progress. Four stages of communicative behavior are distinguished, each comprising 2 levels (responding and/or initiating): stage 0 no communication, stage 1 non-verbal communication, stage 2 transition into verbal communication (whispering, making sounds) and stage 3 verbal communication. No psychometric properties were mentioned.
The Goal Attainment Scaling (GAS [72]) was used in one study to monitor progress of an intervention targeting SM (see Table 3, Study ID: 16). The GAS allows for quantifying progress toward a specific individualized goal. Usually GAS-scales comprise 5 points with 0 meaning no change, negative scores indicating deterioration and positive scores meaning improvement. In the study of Mitchell and Kratochwill into SM [45], the GAS-scale used ranged from: − 2 (failure to speak) to + 2 (normal speech in all situations) and was rated by parents and teachers.
The Parent’s Daily Rating of Child Behavior (DRCB-P) and Teacher’s Daily Rating of Student Behavior (DRSB-T [73]) were used by Bork & Bennet [33] describing three children with SM (see Table 3, Study ID: 4). The original goal was to ask parents and teachers to record the frequency in number of words and the volume of speech (on a 0–10 audible scale) on a daily basis. However, it appeared to be too difficult for parents and teachers to report the exact number of words. Instead they were then asked to record new verbal behaviors (e.g., speaking to a new person, spontaneous speech instead of on request). There is no psychometric information available for these rating scales.
A Direct Behavior Rating measure was used by Barterian et al. [74] (see Table 3, Study ID: 2) to measure speaking behavior and social anxiety symptomatology in naturalistic situations three times per week. Parents were trained and asked to observe their child during social interaction with an unfamiliar adult. Frequency and ease of social engagement, and spontaneous and responsive speech were rated on a 10-point scale (from 0 = never to 10 = always).
An Independent Evaluator Behavioral Evaluation (IEBE [19]) of verbal and non-verbal behavior during 10 structured interactional tasks was used by Bergman et al. [19] (see Table 3, Study ID: 3). It can be administered during a 10–15 min playful interaction. No further psychometric information was provided.
The Strong Narrative Assessment Procedure-Retell (SNAP[75]) is a standardized narrative elicitation task and was adapted to assess narrative abilities in children with SM [76]. It was used in two studies (see Table 3, Study ID: 3 and 7) as a treatment outcome measure. In this task, the teacher was asked to read a storybook to the child and the child was asked to retell the story. The narrative of the child was audio-recorded, so that the length of the story could be analyzed. The SNAP appeared to be sensitive to change in this study. The psychometric properties of the task are unknown [19].
Other observational measures were minimally described and are summarized here. In the study of Mitchell and Kratochwill [45], parent and teachers were asked to rate the number of spoken words and independent raters were mobilized twice a week to code the words spoken during classroom one-hour observations. The procedure was adapted from the Revised Behavioral Observation Code for Selective Mutism (RBOCSM; [77]). The adaptations or coding schemes were not described [45]. Edison et al. [67] coded speech from video during parent–child interaction play in a laboratory setting. Bunnell and colleagues used video software to observe and analyze treatment process by means of percentage of time that the child spoke during a task [78] and the latency to respond to communicative prompts [79].
Other instruments
A small number of studies used severity scales originally designed to measure general functioning, to specifically assess severity or improvement of the core speaking symptom of SM (criterion A). The Global Assessment of Functioning (GAF, [80]) or the Children’s Global Assessment Scale (CGAS, [81]), rated on a 0–100 scale, were adaptively used to assess SM severity [55, 60, 82] and improvement after treatment [21, 44, 70]. Accordingly, the Clinical Global Impression—Severity (CGI-S) and Improvement (CGI-I) Scales [83] were used to investigate specific SM behavior and behavioral change. The scales are rated on 7-point scales. The CGI-S ranges from “Not At All Ill” to “Extremely Ill”, and the CGI-I ranges from “Very Much Improved” to “Very Much Worse”[19, 21, 29, 35, 36, 70, 74]. Finally, the teacher version of the Impairment Rating Scale (IRS; [84]) was used to measure specific impairment at school as a result of SM. The IRS has 8 items and is measured on a 7-point scale (0 = no problem tot 6 = extreme problem)[21].
Discussion
The aim of this systematic review was to identify and evaluate the assessment instruments that have been used in the past decade for the purpose of screening and assessing severity of SM symptomatology, classification of the disorder and monitoring treatment outcomes on speaking behavior. The number of studies on SM increased over the past years, and studies with larger samples are emerging. However, the majority of samples are still small. To enhance insight in SM and treatment outcomes, comparability of methodology and instruments between groups is utterly important.
Our review revealed that the majority of studies published in the last decade, used one or more standardized or quantified measures. Interestingly, 38% of studies did not use any standardized diagnostic instrument for SM.
To classify SM in clinical practice or to confirm the diagnosis for the purpose of inclusion in research, questionnaires and clinical interviews have been used. The measure used most often in research is the SMQ [17]. This measure is short and comprises a severity scale investigating speaking in three different contexts and a scale to investigate interference of the symptoms on the child’s and family functioning. The reliability of the measure has been assessed in different cultural samples, showing acceptable to excellent internal consistency [19,20,21, 24,25,26,27,28,29,30]. There is support for adequate convergent, discriminant and incremental validity [17, 18]. Because of the few studies to date, there is limited validity. The questionnaire had been translated into different languages and publications represented in the present review came from the US, Norway, Italy, Israel, Turkey and Spain. Although developed for 3–11-year-old children, the SMQ has been used in older children as well. However, some of the items may not be appropriate for the very young children or for older adolescents. In future research, it is important to further investigate the correlation of SM severity and age. In most studies, the majority of children are young and larger SMQ datasets about adolescents are lacking. The SMQ does not provide cut-off scores and is therefore not easily applicable to classify groups, although some studies use the mean and standard deviation of the SM group in the original sample. Most studies used a clinical interview (ADIS) in addition to the SMQ to confirm the clinical diagnosis [19]. The SMQ can be used to differentiate between children with and without SM [24]. The use of cut-off scores, and the use of the SMQ in typically developing children (TDs) can be investigated in larger samples. Research is emerging but still quite limited.
An interesting questionnaire for teachers is the SSQ, adapted from the SMQ [5]. The number of items varies somewhat between studies, without further explanation in the articles. Differing item numbers of the SSQ can hamper the comparability of results. Internal consistency varied from questionable to acceptable [19, 21, 22, 36]. The low number of items is both an advantage for teachers who often struggle with time and a disadvantage because only a few situations in school are investigated. The SMQ and SSQ were used in most treatment studies and were found sensitive to treatment changes [19, 22, 34]. Detailed psychometric information is limited regarding non-English speaking samples, the teacher rated SSQ, and also regarding cut-off scores and the use of the SSQ in typically developing children (TDs).
More recently, the FSSM has been developed [37]. The FSSM includes both a diagnostic scale that can be used to classify groups and severity scales that can be used to measure symptom changes. The FSSM has three age versions (3–7, 6–11 and 12–18 years), with items that have been adapted to the developmental stages of the children. The questionnaire is longer than the SMQ (51 items in the preschool version and 52 items in the other versions). The FSSM is a parent-rated measure and parents are encouraged to ask the teacher for help if they have difficulties answering questions about the speaking behavior of their child in school or kindergarten. This may be a disadvantage in treatment studies when an independent teacher rating is wanted. The psychometric properties of the measure are promising with high internal consistency and good convergent and discriminant validity. With the diagnostic scale a SM group was successfully differentiated from children with social phobia and other internalizing disorders. The questionnaire is freely available online in different languages. The other questionnaires evaluated in this review have been less often used, are less well described and/or the psychometric properties have been insufficiently investigated and reported. The advantage of the FSSM is that different age groups are divided. The advantage of the SMQ is that it is used widely, but studied in a young age group.
The clinical interview most often used to investigate the presence and severity of SM, as well as comorbid disorders, is the ADIS [51]. The ADIS has most often been used for inclusion in studies. The severity rating has also been used in seven studies as an outcome measure and was found to be sensitive to change [21, 29, 53]. An alternative for the ADIS is the K-SADS-PL-DSM-5 [57]. Previous versions of this instrument did not have a SM section but the newest version has a SM supplement. The reliability and validity of this SM supplement was found promising in Turkey and Japan [30, 58], but needs to be investigated further in other countries.
For very young children, who fall below the age ranges of the ADIS (4–18 y) and the K-SADS-PL-DSM-5 (6–18), the PAPA; [59] can be used, which is available online. Using PAPA, SM is screened using a single item. Finally, the TTI-SM [62] is of interest to get clinical information from the teacher using a standardized phone interview. Promising psychometric properties have been found in one study for the 11-item SM subscale with high internal consistency and good convergent, predictive and concurrent validity [63]. These psychometrics have to be confirmed in larger new studies in other countries.
Several observational instruments for speaking behavior were developed, but most measures are used in one study only and psychometric information is lacking. Multiple measures comprise the observation and coding of speaking behavior in controlled laboratory settings (SM-BOT; [69], IEBE; [19], SNAP; [75], parent–child interactive play; [67], communicative behavior during interaction tasks; [78, 79]). With the exception of the SNAP story-tell task for children aged 6–13 years, these tasks were too briefly described so that replication of findings or the use in other studies is not possible. Other observation tasks have been designed to rate speaking behavior in daily situations at home or at school (DRSB; [73], DBR; [74], Adapted RBOCSM; [45]). These scales allow for repeated measurements over time for single case experimental designs. The Direct Behavior Rating (DBR) measure described by Barterian et al. [74] is probably the most feasible procedure in naturalistic situations. Hierarchy scales such as the SM-SCCS [71] can also be used to observe and rate behavior for naturalistic situations and to investigate treatment outcome. Of interest is the Goal Attainment Scaling (GAS; [72]). This measure allows for setting individual goals and measuring improvement over time. Finally, other widely used general measures to assess global functioning, impairment and improvement (GAF; [80], CGAS; [81], CGI-S/I; [83]) have been used in several studies as severity and treatment outcome measures [19, 21, 29, 35, 36, 44, 55, 60, 70, 74, 82]. When choosing an observational measure for a study, the observer as well as the setting can be taken into account. However, all observational instruments need more investigation and validation to be valuable measures in clinical practice and research.
Unfortunately, self-report measures for SM are still scarce. Although children with SM often are very young, making parent and teacher ratings necessary, it is known from research that SM can take a chronic course and also affects adolescents and to a lesser extent even adults [9, 10, 85]. The SMQ appears to be a promising measure for self-report as has been shown by Muris et al. in a non-clinical population (8–12 years old) [49] and Milic et al. with an adapted pictorial version in young children (3–7 years old) [50]. We recommend further studying the use of validated SM-specific self-report measures for use in clinical practice and research. In children with SM and/or social anxiety, it was found that parents and clinicians often report higher anxiety levels than the children themselves [55, 86]. Difficulties to speak at school may be more reliably reported by adolescents themselves than by parents or secondary school teachers.
We consider the results of this review as a plea for multi-informant diagnostics using questionnaires, interviews and observation. Although the importance of a multi-informant approach in the assessment of SM has been underlined [55, 86, 87], in many of the reviewed studies only one informant is asked to complete a standardized quantitative measure. To obtain clearer insight in SM and its underlying mechanisms, a multi-informant approach is recommended. We recommend the use of parallel questionnaire or observational versions (parent, teacher, clinician and attuned age-adequate self-reports). As to the content of SM assessment instruments, we recommend to extend and include the range of social settings in which children find themselves (school, after school activities, swimming lessons, play dates, playgrounds, family occasions, shops or restaurants etc.).
This review showed an important shortcoming that over a third of studies (38%) did not report any objective measure to classify SM. This limits the replicability of these studies and psychometrically sound foundation of instruments to be used in clinical practice. Few studies described psychometric properties or validation of the reported instruments in detail.
Another problem was that the instruments used were not always validated for the same population as they are used in (as to age, general vs. clinical population). The majority of measures has not been evaluated in different samples. This may hamper the conclusions since it is not warranted to generalize the applicability of an instrument to another population than it is aimed for, without studying the psychometrics and validity in that population. As there is still a marked lack of evaluated measures, we recommend that a selection of instruments, such as one or two promising questionnaires, parent and teacher interviews and direct observational measures, will be used in combination more often. A smaller set of instruments that are used across studies will increase comparability, facilitate replication and move the field of SM research forward. Furthermore, it is important to note that the instruments used most frequently, were still based on the DSM-IV. However, since core criteria for SM were not changed in the DSM-5 version, we consider our findings as still clinically relevant.
Finally, very little is known about cultural differences in SM characteristics and cross-cultural appropriateness of the instruments used, especially regarding discrepancies between western and different non-western cultures. This is not surprising considering the low prevalence of SM. SM specifically and taciturnity in general may be unrecognized, underreported or perceived from a different perspective in different areas of the world. In this context, we refer to our previous reaction to a Turkish article focusing on speech delay where the diagnosis of selective mutism appeared to be overlooked [88, 89]. It is encouraging to see that studies into SM are emerging and that some of the measures are translated into different languages. Even more encouraging is the fact that several newly developed and validated measures are open access and can be freely derived from the internet. That enlarges the possibilities for researchers around the world to collect and share data.
Conclusion
This systematic review shows that the SMQ and the teacher-version SSQ [5, 17] are the questionnaires used most often for SM severity ratings. The FSSM is a promising new questionnaire providing a subscale for classification and severity subscales for SM [37]. As to clinical interviews investigating DSM criteria for SM, the ADIS is used most often and also provides a severity rating. There is a need for a well-validated standardized observational measure that can be used in daily situations by parents and teachers. The vast majority of instruments used in different studies were used only once, hampering comparability of findings over studies. In a large part of the articles, no instruments were described at all. We recommend the use of multi-informant measures to investigate SM behavioral characteristic and to classify the disorder, both in clinical practice and in research studies. Several measures with strong or promising psychometrical qualities are available. The use of these measures in different settings allows comparability among studies and will help to understand cross-cultural differences. In addition, we stress the importance of investigating the usability and psychometric properties of self-report measures and observational measures for children and adolescents with SM. For future research, we recommend measures with a broad age range to enable long-term follow-up studies.
Data availability
Not applicable.
Code availability
Not applicable.
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5®): American Psychiatric Pub; 2013.
World Health Organization. ICD-11 for mortality and morbidity statistics (2018). 2018.
Muris P, Ollendick TH (2015) Children who are anxious in silence: a review on selective mutism, the new anxiety disorder in DSM-5. Clin Child Fam Psychol Rev 18(2):151–169
Muris P, Ollendick TH (2021) Current challenges in the diagnosis and management of selective mutism in children. Psychol Res Behav Manag 14:159
Bergman RL, Piacentini J, McCracken JT (2002) Prevalence and description of selective mutism in a school-based sample. J Am Acad Child Adolesc Psychiatry 41(8):938–946
Elizur Y, Perednik R (2003) Prevalence and description of selective mutism in immigrant and native families: a controlled study. J Am Acad Child Adolesc Psychiatry 42(12):1451–1459
Kumpulainen K, Räsänen E, Raaska H, Somppi V (1998) Selective mutism among second-graders in elementary school. Eur Child Adolesc Psychiatry 7(1):24–29
Viana AG, Beidel DC, Rabian B (2009) Selective mutism: a review and integration of the last 15 years. Clin Psychol Rev 29(1):57–67
Steinhausen HC, Wachter M, Laimböck K, Metzke CW (2006) A long-term outcome study of selective mutism in childhood. J Child Psychol Psychiatry 47(7):751–756
Remschmidt H, Poller M, Herpertz-Dahlmann B, Hennighausen K, Gutenbrunner C (2001) A follow-up study of 45 patients with elective mutism. Eur Arch Psychiatry Clin Neurosci 251(6):284–296
Crundwell RMA (2006) Identifying and teaching children with selective mutism. Teach Except Child 38(3):48–54
Ford MA, Sladeczek IE, Carlson J, Kratochwill TR (1998) Selective mutism: Phenomenological characteristics. Sch Psychol Q 13(3):192
Stone BP, Kratochwill TR, Sladezcek I, Serlin RC (2002) Treatment of selective mutism: a best-evidence synthesis. Sch Psychol Q 17(2):168
Oerbeck B, Manassis K, Overgaard KR, Kristensen H. Selective Mutism. In: M. RJ, Martin A, editors. JM Rey’s IACAPAP e-Textbook of Child and Adolescent Mental health. Geneva: International Association for Child and Adolescent Psychiatry and Allied Professions; 2019.
Keen DV, Fonseca S, Wintgens A (2008) Selective mutism: a consensus based care pathway of good practice. Arch Dis Child 93(10):838–844
Moher D, Liberati A, Tetzlaff J, Altman DG (2010) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 8(5):336–341
Bergman RL, Keller ML, Piacentini J, Bergman AJ (2008) The development and psychometric properties of the selective mutism questionnaire. J Clin Child Adolesc Psychol 37(2):456–464
Letamendi AM, Chavira DA, Hitchcock CA, Roesch SC, Shipon-Blum E, Stein MB (2008) Selective mutism questionnaire: Measurement structure and validity. J Am Acad Child Adolesc Psychiatry 47(10):1197–1204
Bergman RL, Gonzalez A, Piacentini J, Keller ML (2013) Integrated behaviour therapy for selective mutism: a randomized controlled pilot study. Behav Res Ther 51(10):680–689
Diliberto R, Kearney CA (2018) Latent Class symptom profiles of selective mutism: identification and linkage to temperamental and social constructs. Child Psychiatry Hum Dev 49(4):551–562
Cornacchio D, Furr JM, Sanchez AL, Hong N, Feinberg LK, Tenenbaum R et al (2019) Intensive group ehavioural treatment (IGBT) for children with selective mutism: a preliminary randomized clinical trial. J Consult Clin Psychol 87(8):720–723
Oerbeck B, Stein MB, Wentzel-Larsen T, Langsrud Ø, Kristensen H (2014) A randomized controlled trial of a home and school-based intervention for selective mutism–defocused communication and behavioural techniques. Child Adolesc Mental Health 19(3):192–198
Oerbeck B, Overgaard KR, Stein MB, Pripp AH, Kristensen H (2018) Treatment of selective mutism: a 5-year follow-up study. Eur Child Adolesc Psychiatry 27(8):997–1009
Oerbeck B, Overgaard KR, Bergman RL, Pripp AH, Kristensen H (2020) The selective mutism questionnaire: data from typically developing children and children with selective mutism. Clin Child Psychol Psychiatry 25(4):754–765
Olivares-Olivares PJ, Rosa-Alcazar A, Nunez R, Olivares J. Psychometric propierties of the Selective Mutism Questionnaire in Spanish children. Int j clin health psychol. 2021;21(3):100249.
Esposito M, Gimigliano F, Barillari MR, Precenzano F, Ruberto M, Sepe J, et al. Pediatric selective mutism therapy: a randomized controlled trial. Eur J Phys Rehabil Med. 2016;11.
Serra A, Di Mauro P, Andaloro C, Maiolino L, Pavone P, Cocuzza S (2015) A selective mutism arising from first language attrition, successfully treated with paroxetine-cbt combination treatment. Psychiatry Investig 12(4):569
Henkin Y, Bar-Haim Y (2015) An auditory-neuroscience perspective on the development of selective mutism. Dev Cogn Neurosci 12:86–93
Lang C, Nir Z, Gothelf A, Domachevsky S, Ginton L, Kushnir J et al (2016) The outcome of children with selective mutism following cognitive ehavioural intervention: a follow-up study. Eur J Pediatr 175(4):481–487
Ünal F, Öktem F, ÇETİN ÇUHADAROĞLU F, ÇENGEL KÜLTÜR SE, AKDEMİ D, FOTO ÖZDEMİR D, et al. Reliability and Validity of the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version, DSM-5 November 2016-Turkish Adaptation (K-SADS-PL-DSM-5-T). Turkish Journal of Psychiatry. 2019;30(1).
Manassis K, Fung D, Tannock R, Sloman L, Fiksenbaum L, McInnes A (2003) Characterizing selective mutism: Is it more than social anxiety? Depress Anxiety 18(3):153–161
Bergman R. Treatment for children with selective mutism: An integrative behavioral approach. 2013;137.
Bork P, Bennett S. Video self-modeling, fading, and reinforcement: An effective treatment package for children with selective mutism. Clin child psychol. 2019;psychiatry.:1359104519855110.
Catchpole R, Young A, Baer S, Salih T. Examining a novel, parent child interaction therapy-informed, behavioral treatment of selective mutism. J Anxiety Disord. 2019;66.
Oerbeck B, Kristensen H (2011) How to help when silence is not golden? Treatment of 24 children with selective mutism-preliminary results. Eur Child Adolesc Psychiatry 20:S15
Oerbeck B, Stein MB, Pripp AH, Kristensen H (2015) Selective mutism: follow-up study 1 year after end of treatment. Eur Child Adolesc Psychiatry 24(7):757–766
Gensthaler A, Dieter J, Raisig S, Hartmann B, Ligges M, Kaess M, et al. Evaluation of a Novel Parent-Rated Scale for Selective Mutism. Assessment. 2018:1073191118787328.
Hartmann B. Evaluationsbogen für das sozialinteraktive Kommunikationsverhalten bei Mutismus [Evaluation sheet for the socially interactive communication behavior in mutism]. 2005 [Available from: https://www.boris-hartmann.de/nl/mutismus/diagnostikbogen.html.
Cunningham CE, McHolm AE, Boyle MH (2006) Social phobia, anxiety, oppositional ehaviour, social skills, and self-concept in children with specific selective mutism, generalized selective mutism, and community controls. Eur Child Adolesc Psychiatry 15(5):245–255
Carbone D, Schmidt LA, Cunningham CC, McHolm AE, Edison S, St. Pierre J, et al. Behavioral and socio-emotional functioning in children with selective mutism: A comparison with anxious and typically developing children across multiple informants. J Abnorm Child Psychol. 2010;38(8):1057–67.
Nowakowski ME, Tasker SL, Cunningham CE, McHolm AE, Edison S, Pierre JS et al (2011) Joint attention in parent-child dyads involving children with selective mutism: a comparison between anxious and typically developing children. Child Psychiatry Hum Dev 42(1):78–92
Nowakowski ME, Cunningham CE, McHolm AE, Evans MA, Edison S, Pierre JS et al (2009) Language and academic abilities in children with selective mutism. Infant Child Dev 18(3):271–290
Starke A (2018) Effects of anxiety, language skills, and cultural adaptation on the development of selective mutism. J Commun Disord 74:45–60
Plener PL, Gatz SA, Schuetz C, Ludolph AG, Kölch M (2012) A case of selective mutism in an 8-year-old girl with thalassaemia major after bone marrow transplantation. Pharmacopsychiatry 45(1):37–39
Mitchell AD, Kratochwill TR (2013) Treatment of selective mutism: Applications in the clinic and school through conjoint consultation. J Educ Psychol Consult 23(1):36–62
Black B, Uhde TW (1994) Treatment of elective mutism with fluoxetine: a double-blind, placebo-controlled study. J Am Acad Child Adolesc Psychiatry 33(7):1000–1006
Klein ER, Armstrong SL, Shipon-Blum E (2013) Assessing spoken language competence in children with selective mutism: Using parents as test presenters. Commun Disord Q 34(3):184–195
Jozefiak T. Inventory of life quality in children and adolescents. Hogrefe Psykologiförlaget AB, Stockholm. 2011.
Muris P, Mannens J, Peters L, Meesters C (2017) The Youth Anxiety Measure for DSM-5 (YAM-5): correlations with anxiety, fear, and depression scales in non-clinical children. J Anxiety Disord 51:72–78
Milic MI, Carl T, Rapee RM. Similarities and differences between young children with selective mutism and social anxiety disorder. Behav Res Ther. 2020;133.
Silverman WK, Saavedra LM, Pina AA (2001) Test-retest reliability of anxiety symptoms and diagnoses with the Anxiety Disorders Interview Schedule for DSM-IV: child and parent versions. J Am Acad Child Adolesc Psychiatry 40(8):937–944
Wood JJ, Piacentini JC, Bergman RL, McCracken J, Barrios V (2002) Concurrent validity of the anxiety disorders section of the Anxiety Disorders Interview Schedule for DSM-IV: child and parent versions. J Clin Child Adolesc Psychol 31(3):335–342
Reuther ET, Davis ITE, Moree BN, Matson JL (2011) Treating selective mutism using modular CBT for child anxiety: a case study. J Clin Child Adolesc Psychol 40(1):156–163
Klein ER, Armstrong SL, Skira K, Gordon J (2017) Social Communication Anxiety Treatment (S-CAT) for children and families with selective mutism: a pilot study. Clin Child Psychol Psychiatry 22(1):90–108
Young BJ, Bunnell BE, Beidel DC (2012) Evaluation of children with selective mutism and social phobia: a comparison of psychological and psychophysiological arousal. Behav Modif 36(4):525–544
Kaufman J, Birmaher B, Brent D, Rao U. Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (KSADS-PL): Initial Reliability and Validity Data J Am Acad Child Adolesc Psychiatry. Issue; 1997.
Kaufman J, Birmaher B, Axelson D, Perepletchikova F, Brent D, Ryan N. K-SADS-PL DSM-5. Pittsburgh: Western Psychiatric Institute and Clinic. 2016.
Nishiyama T, Sumi S, Watanabe H, Suzuki F, Kuru Y, Shiino T, et al. The Kiddie Schedule for Affective Disorders and Schizophrenia Present and Lifetime Version (K-SADS-PL) for DSM-5: A validation for neurodevelopmental disorders in Japanese outpatients. Compr Psychiatry. 2020;96.
Egger HL, Angold A. The Preschool Age Psychiatric Assessment (PAPA): a structured parent interview for diagnosing psychiatric disorders in preschool children. 2004.
Bufferd SJ, Dougherty LR, Carlson GA, Bromet E, Klein DN. Parent-reported mental health in preschoolers: Findings using a Diagnostic Interview. Compr Psychiatry. 2010;51(6):e2.
Wichstrøm L, Berg-Nielsen TS, Angold A, Egger HL, Solheim E, Sveen TH (2012) Prevalence of psychiatric disorders in ehaviourals. J Child Psychol Psychiatry 53(6):695–705
Tannock R, Fung DSS, Manassis K. Teacher Telephone Interview: Selective Mutism & Anxiety in the School Setting (TTI-SM). Unpublished instrument. 2003.
Martinez YJ, Tannock R, Manassis K, Garland EJ, Clark S, McInnes A (2015) The teachers’ role in the assessment of selective mutism and anxiety disorders. Can J Sch Psychol 30(2):83–101
Schneider S, Unnewehr S, Margraf J (2009) Kinder-DIPS–Diagnostisches Interview bei Kindern und Jugendlichen mit psychischen Störungen. Springer, Berlin Heidelberg
Cholemkery H, Mojica L, Rohrmann S, Gensthaler A, Freitag CM (2014) Can autism spectrum disorders and social anxiety disorders be differentiated by the social responsiveness scale in children and adolescents? J Autism Dev Disord 44(5):1168–1182
Cunningham CE, Boyle MH, Hong S, Pettingill P, Bohaychuk D. The Brief Child and Family Phone Interview (BCFPI): 1. Rationale, development, and description of a computerized children’s mental health intake and outcome assessment tool. Journal of Child Psychology and Psychiatry. 2009;50(4):416–23.
Edison SC, Evans MA, McHolm AE, Cunningham CE, Nowakowski ME, Boyle M et al (2011) An investigation of control among parents of selectively mute, anxious, and non-anxious children. Child Psychiatry Hum Dev 42(3):270–290
Poole KL, Cunningham CE, McHolm AE, Schmidt LA. Distinguishing selective mutism and social anxiety in children: a multi-method study. Eur Child Adolesc Psychiatry. 2020.
Kurtz S. Selective mutism behavioral observation task (SM-BOT). Unpublished manuscript. 2008.
Carpenter AL, Puliafico AC, Kurtz SM, Pincus DB, Comer JS (2014) Extending parent–child interaction therapy for early childhood internalizing problems: New advances for an overlooked population. Clin Child Fam Psychol Rev 17(4):340–356
Shipon-Blum E. Selective Mutism Stages of social communication comfort scale. Jenkintown, PA: Selective Mutism Anxiety Research and Treatment Center; 2002 [Available from: Retrieved from http://www.selectivemutismcenter.org/Media_Library/Stages.SM.pdf.
Kiresuk TJ, Smith A, Cardillo JE (1994) Goal attainment scaling: applications, theory and measurement. Erlbaum, Hillsdale
Kearney CA. Helping children with selective mutism and their parents: A guide for school-based professionals: Oxford University Press; 2010.
Barterian JA, Sanchez JM, Magen J, Siroky AK, Mash BL, Carlson JS (2018) An examination of fluoxetine for the treatment of selective mutism using a nonconcurrent multiple-baseline single-case design across 5 cases. J Psychiatr Pract 24(1):2–14
Strong CJ, Mayer M, Mayer M. The strong narrative assessment procedure (SNAP): Thinking Publications; 1998.
McInnes A, Fung D, Manassis K, Fiksenbaum L, Tannock R. Narrative Skills in Children With Selective Mutism. American Journal of Speech-Language Pathology. 2004.
Sheridan S, Kratochwill T. Behavioral observation code for elective mutism. Unpublished manuscript. 1986.
Bunnell BE, Beidel DC (2013) Incorporating technology into the treatment of a 17-Year-old female with selective mutism. Clin Case Stud 12(4):291–306
Bunnell BE, Mesa F, Beidel DC (2018) A two-session hierarchy for shaping successive approximations of speech in selective mutism: pilot study of mobile apps and mechanisms of ehaviour change. Behav Ther 49(6):966–980
Endicott J, Spitzer RL, Fleiss JL, Cohen J (1976) The global assessment scale: a procedure for measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry 33(6):766–771
Shaffer D, Gould MS, Brasic J, Ambrosini P, Fisher P, Bird H et al (1983) A children’s global assessment scale (CGAS). Arch Gen Psychiatry 40(11):1228–1231
Sharkey L, McNicholas F (2012) Selective Mutism: a prevalence study of primary school children in the Republic of Ireland. Ir J Psychol Med 29(1):36–40
Guy W, Bonato R. CGI: The clinical global impression scale. Chevy Chase, MD: National Institute of Mental Health. 1970.
Fabiano GA, Pelham J, William E, Waschbusch DA, Gnagy EM, Lahey BB, Chronis AM et al (2006) A practical measure of impairment: Psychometric properties of the impairment rating scale in samples of children with attention deficit hyperactivity disorder and two school-based samples. J Clin Child Adolesc Psychol 35(3):369–385
Gensthaler A, Khalaf S, Ligges M, Kaess M, Freitag CM, Schwenck C (2016) Selective mutism and temperament: the silence and ehavioural inhibition to the unfamiliar. Eur Child Adolesc Psychiatry 25(10):1113–1120
Yeganeh R, Beidel DC, Turner SM, Pina AA, Silverman WK (2003) Clinical distinctions between selective mutism and social phobia: an investigation of childhood psychopathology. J Am Acad Child Adolesc Psychiatry 42(9):1069–1075
Dow SP, Sonies BC, Scheib D, Moss SE, Leonard HL (1995) Practical guidelines for the assessment and treatment of selective mutism. J Am Acad Child Adolesc Psychiatry 34(7):836–846
Zengin-Akkus P, Celen-Yoldas T, Kurtipek G, Ozmert EN. Speech delay in toddlers: Are they only" late talkers"? 2018.
Rodrigues Pereira C, Ensink JB, De Jonge MV, Wippo E, Lindauer RJ, Utens EM (2019) Letter to the editor: Speech problems and speech delay: possible underdiagnosis of selective mutism. Turk J Pediatr 61(5):817–819
Acknowledgements
We gratefully acknowledge Fonds Stichting Gezondheidszorg Spaarneland who funded this research project, and the information specialists of the Erasmus Medical Center Medical Library.
Funding
This research project is funded by Fonds Stichting Gezondheidszorg Spaarneland (grant number: 2017284). The funding source had no role in the design of the study, and did not have any role in its execution, analysis, interpretation of the data, or decision to submit results.
Author information
Authors and Affiliations
Contributions
All authors critically reviewed the manuscript for intellectual content and provided intellectual input. All authors have read and approved the manuscript. The idea for this article was first formed by CRP, JE, MG and RL, MdJ and EU. CRP performed the literature search with help from the Medical Library, CRP and JE performed the data screening. MdJ and EU performed the full-text screening and data analysis. CRP drafted the article, which was critically revised by JE, MdJ, RL, EU.
Corresponding author
Ethics declarations
Conflict of interests
The authors declare that they have no conflict of interest.
Ethics approval
The study was conducted according to the Helsinki Declaration and its later amendments or comparable ethical standards.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rodrigues Pereira, C., Ensink, J.B.M., Güldner†, M.G. et al. Diagnosing selective mutism: a critical review of measures for clinical practice and research. Eur Child Adolesc Psychiatry 32, 1821–1839 (2023). https://doi.org/10.1007/s00787-021-01907-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-021-01907-2