
Abstract
Attention deficit hyperactivity disorder (ADHD) is a developmental disorder affecting up to 5% of children and adults and is underdiagnosed in many European countries. The process of access to care for this disorder is complex and variable across countries. In general, those affected, or their caregiver, will seek help through their primary care practitioners who are then often responsible for referral to other professionals for diagnosis and provision of treatment. Previous studies have highlighted that many barriers to recognition exist in primary care settings (such as misconceptions, lack of education or lack of resources), preventing access to care for this population and potentially affecting diagnosis rate. This systematic review aims to establish the barriers and facilitators with regard to attitudes, beliefs and experiences of ADHD within primary care. Electronic searches of multiple databases identified 3898 articles of which 48 met our inclusion criteria—primary care professionals from any country, understanding, knowledge, awareness, attitude and recognition of ADHD. Four main themes were identified: (1) need for education, (2) misconceptions and stigma, (3) constraints with recognition, management and treatment, and (4) multidisciplinary approach. The findings suggest many interacting factors are at play in the recognition of ADHD by primary care practitioners with a strong recurring theme of a significant need for better education on ADHD. Implications for research and practice are discussed, suggesting that educational interventions for primary care practitioners could improve the recognition of ADHD in this setting.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder affecting approximately 4% of children [1] leading to considerable functional impairment [2, 3] and often continuing on into adulthood. While evidence-based treatments can help manage ADHD, studies have shown that children with ADHD are underdiagnosed [4]. According to The National Institute for Health and Care Excellence (NICE) guidelines, 3–5% of children and 2% of adults in the UK population should be eligible for an ADHD diagnosis; however, in 2010, a diagnostic prevalence of only 0.506% was estimated for children and 0.016% in adults [5]. A greater understanding of the reasons behind these discrepancies is urgently required [6].
Although many factors influence service utilisation, such as parents and teachers’ perceptions, willingness to engage in help-seeking, or comorbid disorders [7,8,9], the first port of call in many countries is primary care and usually General Practitioners (GPs) who act as gatekeepers to care in the UK, for example. To receive an ADHD assessment and diagnosis if appropriate, children are referred to a psychiatrist or paediatrician through their GPs [10]; once a diagnosis has been made, GPs are then often involved in supporting the further management of children with ADHD and in liaising with parents and specialists. Their understanding of the condition is, therefore, crucial [11].
While there is no cure for ADHD, it can be managed with medication and non-pharmacological interventions [12]. However, unmanaged ADHD results in long-term impairments in many cognitive and behavioural domains [13]. Gaining timely access to care is, therefore, of great importance and research has demonstrated that this can be influenced by the knowledge and attitudes of health professionals [3], with limited GP recognition being a key barrier [8, 14, 15]. Most GPs will have undergone very limited training on ADHD, if any. In many countries, very few GPs have received official training [16]. Many GPs are not confident in recognising and managing ADHD, with lack of education about the disorder being a key component of their lack of confidence [17]. This limited recognition and education could be due to the lack of accurate knowledge and understanding of the disorder, scepticism and misconceptions, [18, 19] and many stigmas still associated with ADHD [12, 20].
A specific definition of what this review considers as primary care is given below but to facilitate the narrative of this review, due to the varied terminologies used across different countries, all terms referring to primary care personnel considered in this review such as GPs, family practitioners, and doctors will be described as primary care professionals (PCPs).
Some studies have looked at the attitudes of PCPs in relation to ADHD and two systematic literature reviews have summarised this evidence [6, 21]. The first review [21] looked at attitudes and knowledge of ADHD since 1994 when the Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM IV) was published, focused only on General Practitioners and only included studies about children. By not including all professionals in primary care and focussing on GPs only, this review missed studies published in the US which does not use the term GPs to refer to primary care professionals. This might have influenced the results as a considerable proportion of ADHD studies are from US research groups (i.e. half of the studies in our review). This review also excluded adults which is important as underdiagnosis of ADHD is even more prominent in adults [22] with stronger stigma and misconceptions as many health professionals still believe ADHD to be a childhood-only disorder [20]. The second review [6] looked broadly at the barriers and facilitators in the pathway to care for ADHD. While PCPs’ attitudes were part of the themes developed from the review, broader determinants were established such as parental involvement or issues with treatment. This review did not focus solely on PCPs’ understanding, the impact related to primary care being a small component of the review.
Goals of the current review
The present systematic review aims to build on these two reviews [6, 22] by enhancing the focus on primary care through amending the selection criteria to include all primary health care settings in all countries, adult ADHD studies, all studies from inception of the databases and establishing facilitators and barriers to access to care for ADHD within the context of primary care. It sought to develop a segregated synthesis [23] of quantitative and qualitative research in an attempt to identify and synthesise current barriers and facilitators to the understanding of ADHD in primary healthcare, ultimately leading to improved recognition of ADHD.
Methods
This review was written in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols (PRISMA-P) guidelines [24]. A protocol for the review was registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42017071426) in July 2017.
Inclusion criteria
Type of studies
Published and peer-reviewed quantitative and qualitative studies were included. The qualitative component of this review considered qualitative studies of any design exploring ADHD in primary care, including beliefs, understanding, attitudes, and experiences.
The quantitative component of this review included quantitative studies of experimental and observational designs (including, but not limited to cohort studies, case–control studies, randomised controlled trials).
Mixed methods studies were also included, and relevant qualitative and quantitative components were extracted separately.
Type of population
This review covered studies in primary care. Primary care is defined as the day-to-day health care provided in the community for people making an initial approach to clinics for advice or treatment [25]. Within the context of this review, primary care includes all public services health professionals that act as a first port of call for families and patients seeking medical advice (referred to as PCPs in this review). Therefore, professions such as physicians, family doctors, GPs, paediatricians, nurses and practitioners were considered depending on the country in which the study was conducted. Each study was thoroughly examined to determine, depending on the country of origin, whether the professionals studied were the initial approach healthcare providers. For example, in the UK, PCPs are often referred to as general practitioners but in the US they might be referred as paediatricians or family practitioners or physicians. However, US paediatricians can have primary and secondary care roles; therefore, careful consideration was given to the role when the term paediatrician was used in US-based studies. Studies involving private practices were excluded from countries where a public health system was available.
If more than one professional population was studied, primary care findings were extracted and reported separately if the study reported different professional groups separately. Studies from countries where PCPs are not gatekeepers and part of the primary care system were excluded if no reference to primary care settings was given.
Type of phenomenon of interest
This review examined the understanding of ADHD in primary care and looked at beliefs, attitude and knowledge, focusing on barriers and facilitators within these contexts. For the purpose of this study, barriers and facilitators were defined as perceived factors that hinder or facilitate the recognition or management of ADHD. As these definitions and concepts varied between studies, this review looked at these concepts broadly in the context of wider aspects of ADHD. This review considered studies focusing on understanding of ADHD throughout the lifespan and, therefore, included adult, adolescent and child studies.
Context
This review included any primary care settings. It took an international perspective and was not restricted to the English language, including relevant studies of all languages, translation being produced on an ad hoc basis. The time period of the review was not restricted and the search strategy covered all publications from database inception up to the 29th of January 2018.
Exclusion criteria
Unpublished studies, literature reviews, case studies, opinion pieces, grey literature and non-peer-reviewed studies were excluded. Studies were also excluded if they did not specify the type of health professionals examined or did not report PCPs’ results separately from other groups. Studies focusing solely on ADHD medication and treatment effectiveness or evaluation were also excluded.
Search strategy
Databases (PsychInfo, Embase, Scopus, ASSIA, Medline and Google scholar) were searched from inception to extract published studies. Following the search of the five main databases and removal of duplicates, an initial search and preliminary analysis were conducted of the subject headings (MeSH) and text words related to ADHD contained in the title and abstract (Supplementary Table S1). PROSPERO was also checked for ongoing or already published systematic reviews on the subject.
The search strategy comprised a combination of key words (e.g. ‘ADHD’, ‘Primary care’) and controlled vocabulary (e.g. ‘doctors’, ‘general practitioners’). The search was first performed on the 1st of May 2017 and updated on the 29th of January 2018. Date and language limits were not imposed.
While hand searching was not a major component of our planned search strategy, the reference lists of all selected papers that met the inclusion criteria were hand searched to check for additional studies.
Study selection
Following the search, all identified citations were uploaded into Endnote and duplicates were removed. Two authors (BF and DD) screened the titles and then abstracts against the search inclusion criteria with 100% agreement. Full reports were obtained for all titles that appeared to meet inclusion criteria and imported into a dedicated folder on Endnote.
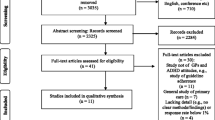
The same two review authors screened and assessed the full text in detail against the inclusion criteria. Disagreement on selected studies was resolved through discussion without the need to seek guidance from a third reviewer (KS). Studies that did not meet the inclusion criteria were excluded and are presented in the flow diagram below (Fig. 1), one full-text article was not available despite multiple requests from inter-library loan.

Flow diagram of the different selection processes
Data extraction and outcomes
Data extraction
Two reviewers (BF and DD) extracted qualitative and quantitative data from the 48 included studies informed by a standardised data extraction tool for qualitative studies (JBI-QARI, [26]) and for quantitative studies (JBI-MAStARI, [26]), aiming to answer the review’s primary objectives. In the instance of studies reported in a foreign language, French studies were translated by the lead reviewer, a native French speaker, and translation was sought for other languages. Primary authors of relevant studies were contacted when additional information was needed.
Outcomes
The main outcome is the description and interpretation of PCPs’ understanding of ADHD including what hinders and facilitates their recognition of the condition. Multiple factors reported in the selected studies were evaluated such as beliefs, attitudes, knowledge and understanding. These factors were grouped into themes within the synthesis phase and are discussed in the context of barriers and facilitators.
Assessment of methodological quality
Following mixed-method review guidelines [27], the process of quality assessment was separated between qualitative and quantitative studies. Two authors (BF and DD) critically appraised all selected studies for methodological quality using standardised quality appraisal tools for qualitative studies and quantitative studies [28]. These instruments assessed the quality of evidence across studies, including but not limited to criteria such as sampling strategy, analysis and sample size. Any disagreement between reviewers was resolved through discussion.
Data synthesis
Due to the mixed-method nature of this review, a segregated synthesis was conducted where two distinct analyses involving qualitative and quantitative evidence were made prior to conducting a mixed-method synthesis [27].
A meta-synthesis summarised the qualitative findings, informed by JBI-QARI [26]. This aggregation or synthesis of findings generated a set of statements representing the aggregation, through assembling the findings rated according to their quality, and categorising them on the basis of similarity in meaning. These categories were then subjected to a thematic analysis informed by Braun and Clarke [29] to produce a single comprehensive set of synthesised findings that can be used as a basis for evidence-based practice. Where textual pooling was not possible the findings were presented in narrative form.
Quantitative data were synthesised in a comparable manner as statistical pooling was not possible due to high levels of heterogeneity within the included studies. The findings are presented in narrative form including tables.
The two analyses were aggregated by means of configuration [27]. The results of the syntheses were combined in the form of qualitative themes. The synthesised findings of the qualitative syntheses served as themes and together with the quantitative synthesis were summarised in thematic statements by the reviewers, involving the configurative conversion of all numerical results into qualitative thematic statements. These ‘converted’ findings and the qualitative thematic statements were then assembled. The aggregation/configuration of all themes generated a set of statements that represent the final aggregation, qualitative and quantitative findings complementing each other.
Two reviewers (BF and DD) conducted the syntheses in a sequential order, one reviewer developing the synthesis and the second checking the findings. Any disagreements were discussed and/or mediated by a third reviewer (KS).
The barriers and facilitators extracted for this review were categorised into four themes:
-
Need for education—issues discussing the lack of training on ADHD for PCPs, lack of accurate awareness and a lack of confidence around ADHD.
-
Misconceptions and stigmas—issues linking ADHD to general stigmatisation and misconceptions and the role of labels and media.
-
Constraints with recognition, management and treatment—issues with time constraints and complexity of ADHD as well as issues with treatment options for ADHD.
-
Multidisciplinary approach—issues with the role of different specialists, the role of the school, the parents and people with ADHD themselves.
Results
Study selection
The study selection process is shown in Fig. 1. Reasons for excluding trials after full-text assessment are provided in Supplementary Table S2. In total, 48 studies published between 1987 and 2017 met the inclusion criteria, of which 6 were qualitative, 2 mixed methods and 40 quantitative. The quantitative studies were all based on surveys and questionnaires with the exception of one free-listing exercise; while the qualitative studies were based on interviews (n = 4), focus groups (n = 2), no observational studies were identified. Characteristics of each study and their review themes are given in Table 1.
A range of countries were represented with most of the studies originating from the US (23 studies), UK (eight), Australia (3), Canada (4), Netherlands (2), South Africa (2) and 1 each from Iran, Brazil, Finland, France, Pakistan, Switzerland and Singapore.
Data methodological quality
Results of study quality are reported in Table 1. Following Kmet, Lee and Cook’s guidelines [28], an original quality score from 0 to 1 was calculated for each study. Scores were then classified into low (0–0.44), moderate (0.45–0.69) and high (0.70–1.00). Study quality was assessed by two reviewers (BF and DD). Agreement between reviewers was 88% overall (92% for quantitative studies, 85% for qualitative studies).
The studies showed some variation in their quality. The average quality score was 0.73 with 36 studies receiving a high-quality rating, 10 a moderate rating and 2 a low rating, (quantitative studies mean score of 0.75; qualitative studies mean score of 0.70). The two studies that received a low-quality rating were not used to inform our review results and conclusions.
Data extraction and summary of results
Need for education
The main theme highlighted by this review related to the need for education on ADHD. Thirty-seven papers identified issues related to a lack of education on ADHD, representing a wide range of countries, 14 from the US [30,31,32,33,34,35,36,37,38,39,40,41,42,43], 7 from the UK [3, 11, 16, 44,45,46,47], 3 from Australia [48,49,50], 2 from the Netherlands [51, 52], 2 from South Africa [53, 54], 2 from Canada [55, 56] and 1 each from France [57], Singapore [58], Pakistan [59], Finland [60], Brazil [61], Iran [62] and Switzerland [63]. These papers highlighted both a lack of initial training, as well as inadequate training on ADHD. They also highlighted a lack of awareness, experience, understanding and knowledge of ADHD. Most PCPs also reported a lack of confidence about ADHD and in treating ADHD. These factors often hindered general knowledge and understanding of ADHD.
-
Lack of initial training and inadequate training
Lack of training on ADHD was recorded by many studies. This included studies reporting a lack of training especially at undergraduate and postgraduate medical education levels [3, 16, 30, 38, 45, 53, 57] with studies suggesting that 1% [53] to 28% [57] of PCPs received specific training about ADHD. In a quantitative study from the UK, Ball [16] found that only 6% of 150 PCPs surveyed received formal training on ADHD and 80% reported wanting further training. This was more prominent for adult ADHD with two studies reporting a greater lack of education [30, 53]. Even when studies reported training on ADHD, the training was often considered by PCPs to be inadequate [11, 31, 59] with up to two-third of PCPs feeling inadequately trained to evaluate children with ADHD [31]. While a strong need for training on ADHD in general was observed, three studies also highlighted the importance of updated training incorporating new knowledge [37, 39, 42]. This lack of education affected many aspects of the primary care experience of patients from referral and diagnosis [44, 59] to management [50] of ADHD.
-
Lack of awareness, experience, understanding and knowledge of ADHD
The need for education was also highlighted through the lack of general awareness, experience, understanding and accurate knowledge of ADHD. While two studies directly reported a lack of knowledge and experience [36, 52] as a barrier to dealing with people with ADHD, eight investigated these concepts through knowledge of the DSM criteria or clinical guidelines [31, 33, 34, 47, 64,65,66,67]. Accurate knowledge of guidelines and procedures for identification of ADHD were low; for instance, only 20% [33] —27% [31] of PCPs were using DSM criteria and only 20% were using official guidelines [65]. One study from the UK [11], using a mixed-method approach, found that 75% of PCPs could not identify ADHD DSM criteria correctly and all PCPs were unsure of ADHD prevalence and diagnostic procedures. Two studies investigated these concepts through questions about several factors including treatments, prevalence and symptoms, reporting different levels of knowledge and awareness throughout, with inaccurate beliefs such as believing that there is no need for treatment [61] or that ADHD was not a medical problem [3]. Additionally, very few studies reported a majority of PCPs in their sample being able to accurately identify ADHD characteristics. Two studies reported that PCPs did not know what the acronym TDHA (ADHD in French) stood for [57] or that they did not know about ADHD even after reading its definition [61] demonstrating that a lack of general knowledge about ADHD was highly evident.
-
Lack of confidence about ADHD and its treatment
The final aspect relating to the need for education highlighted PCPs’ lack of confidence about ADHD, most specifically in treating ADHD. This review and the included studies focus principally on the recognition of ADHD but a few studies also raised the issue of a lack of confidence, encompassing treatment and management. In these studies, it is unclear whether the lack of confidence is solely around recognition or all aspects of ADHD management; therefore, it was important to include this aspect in our findings. While two studies reported a general lack of confidence [30, 49], three [36, 55, 63] reported low confidence and competence in diagnosis and management of ADHD. Some studies reported a lack of confidence toward treatments, with PCPs reporting being uncomfortable with medication for ADHD. Goodman et al. [36] reported that 38% of PCPs had no confidence in treating ADHD, Alder et al. [30] also highlighted a considerable lack of confidence in treating adults with ADHD and Ball [16] reported that 11% of PCPs were not willing to prescribe medication at all due to lack of knowledge, while 88% of PCPs wanted further training in the drug treatment of ADHD.
Facilitators
While the need for education underpinned many barriers and issues towards the overall understanding and knowledge of ADHD, a few positive outcomes were also observed. In contrast to our overall findings where a lack of knowledge and confidence was evident, three studies reported above-average ratings of confidence and high knowledge of ADHD [41, 42, 60] and Evink et al. [64] reported that all paediatricians in their studies used DSM criteria. The reasons for these different findings are unclear but could be due to the high number of paediatricians in the studies who might have received specialist paediatric training.
Despite the overall lack of training and awareness of ADHD, studies reported that PCPs had a keen interest in wanting to gain more knowledge [42], with strategies such as asking colleagues, self-education, and online enquiries. [16, 40, 53, 57, 62]. Two studies [52, 56] explored the benefits of educational programs for PCPs and reported an increased awareness and confidence in ADHD after taking part; the first study [52] focused on an educational program for prescription and monitoring of ADHD medication, while Ward et al. [56] evaluated a 1-day course which aimed to teach PCPs to manage ADHD and observed a significant difference between pre-test and post-test knowledge. Furthermore, Wolraich et al. [43] reported a marked increase in the use of APA guidelines between 1999 and 2005 by PCPs (13%–50%), suggesting an increased interest and awareness in ADHD.
Misconceptions and stigmas
Linking to the previous theme, misconceptions and stigmatisation surrounding ADHD were often strongly present in the literature. This notion was explored by different studies, either directly reporting the experience of stigma within primary care or reporting inaccurate facts about ADHD; reflecting gender biases (‘it only happens in boys’), misleading causes of ADHD (due to high sugar level or lead poisoning) or most prominently, that ADHD is primarily caused by bad parenting. Seventeen studies discussed elements related to misconceptions, five from the US [36, 38, 67,68,69], four from the UK [3, 11, 46, 47], two from Australia [49, 50], and one each from the Netherlands [51], Iran [62], Brazil [61], Singapore [58], France [57] and South Africa [54].
-
General stigmas and misconceptions
Most studies reported general misconceptions about ADHD. In a mixed-method study in the UK, Salt et al. [11] reported that over 50% of PCPs agreed on the controversial nature, the strong stigmatisation of ADHD and the disadvantages the diagnosis brought. In a quantitative survey of 380 US PCPs, Kwasman et al. [69] reported strong misconceptions about ADHD, including: ADHD is “caused by poor diet” (21% agreed), “the child does it on purpose” (15%), “medications can cure ADHD”(10%) and “ADHD medications are addictive” (48%). Many studies reported participant views that sugar levels were a cause of ADHD [58, 62, 69] while others reported a gender misconception that ADHD was only present in boys [38, 68]. Other misconceptions were more surprising with Ghanizadeh and Zarai [62]; for instance, reporting that 82% of PCPs believed children with ADHD misbehaved primarily because they do not want to obey rules and do their assignments, while Quiviger and Caci [57] stated that 24% of the PCPs surveyed thought it was a disorder constructed abroad and imported into France.
While it could be expected that PCPs should not hold stigma towards ADHD due to their expected knowledge of the disorder, in a quantitative study in the Netherlands on stigmatisation towards ADHD, Fuermaier et al. [51] reported no difference in stigmatisation levels between physicians and a control group of non-medical professionals.
-
Bad parenting
Ten studies reported that PCPs believed ADHD was due to bad parenting [11, 36, 46, 47, 49, 50, 54, 62], numbers varying from 15% [57] to over half [36, 62] of PCPs surveyed believing that dysfunctional families were predominately to blame for ADHD symptom expression. In semi-structured interviews with UK PCPs and parents, Klasen and Goodman [3] reported that most GPs saw symptoms of hyperactivity (one of the three symptom clusters of ADHD) as an effect of dysfunctional families and many felt that parents’ views of hyperactivity as a medical problem were an attempt to avoid dealing with possible shortcomings in their parenting practices.
-
The role of the media and labels
Four studies linked the presence of misconceptions with negative media coverage and the use of labels. Klasen and Goodman [3], for instance, reported that parents felt PCPs were against labels, trying to normalise hyperactive behaviours, while Klasen [46] reported that 25% of PCPs felt labelling was not useful. Salt et al. [11] highlighted, through a targeted questionnaire, the influence of the media in the general public’s conception of ADHD, whereas Shaw et al. [50] argued that negative media coverage and labels affect the representation of medication and had led to labelling bad parenting as ADHD.
Facilitators
Although very few facilitators can be observed within this theme, it is important to note that the concepts of misconception and stigma were only explored in a third of included studies suggesting stigma about ADHD did not emerge from studies as much as might have been anticipated. Studies identifying stigma reported stigma from a wide variety of different countries and cultures, suggesting that stigma surrounding ADHD is not specifically culturally determined.
Internal and resource constraints with recognition, management and treatment
As PCPs are often responsible for the recognition and management of ADHD, a few barriers were observed surrounding these procedures. The first considered the barriers experienced around recognition, referral and diagnosis of ADHD, mainly referring to resource constraints such as time and the need for appropriate screening tools. With regard to treatment options, the main barriers observed included the limited treatment options available and uneasiness around medications. Twenty studies discussed aspects related to recognition and treatment, with eleven studies from the US [30, 31, 34,35,36,37, 41, 66, 69,70,71], three from the UK [3, 44, 46], two from Australia [49, 50] and one each from Brazil [61], the Netherlands [52], France [57] and South Africa [53].
-
Time constraint and complexity of ADHD
The resource constraint mainly experienced in the recognition and management of ADHD is in relation to time and the complexity of ADHD. Many studies found that the time necessary to gain all the relevant information was often too demanding [31, 34, 35, 49, 50, 52, 53, 69] especially taking into consideration the complex nature of ADHD [34, 36, 41]. After interviewing 19 PCPs in focus groups in the US, Guevara et al. [37] reported that limited resources and lack of time to communicate with schools led to limited access to care, whilst Klasen and Goodman [3] found in their interviews in the UK that information necessary for management and recognition is often conflicting and ambiguous. Five other studies mentioned the need for better assessment tools [3, 35, 54, 71], especially for adults [30]. Finally, one other barrier experienced in relation to time and resource constraints is that PCPs make decisions on assessment for referral based on the child’s behaviour in their office [33, 57, 65], which can lead to potential misdiagnosis as the child might behave very differently at home or school [72].
-
Treatment
Considerable issues were also highlighted around treatment: the lack of available treatment options as well as uneasiness around medication. While studies reported a general uneasiness with ADHD medication [36, 38, 41, 50], this at times led to resistance or refusal to grant prescriptions by PCPs [16, 52, 66]. In a series of interviews with 128 PCPs, Gomes et al. [61] reported high levels of uneasiness around medication, limited knowledge of treatment options, and a lack of knowledge of the pros and cons of medication and other treatments. This reflected other findings describing confusion around treatment options in relation to professionals’ knowledge of what is available and limited availability of treatment [3, 36, 70].
Facilitators
Despite the constraints explored in these studies, attempts to address these issues were reported in only two studies. After participating in a 1-h educational online course on ADHD medication, Hassink-Franke et al. [52] found that most PCPs felt more confident and competent about prescribing and monitoring medication. As this was a qualitative study, information was not available on the degree of change of confidence in the participating PCPs. Ward et al. [56] evaluated a 1-day course which aimed to help PCPs to manage ADHD. Results demonstrated some impact on practice in the form of increased levels of ADHD referrals. However, the study was based on only 34 clinicians, was not controlled and did not verify the appropriateness of referrals.
Multidisciplinary approach: the role of other specialists, teachers, parents and patients
The final theme encompassed the concepts of a multidisciplinary approach. This mainly referred to the role of different specialists and the importance of shared care. However, it also included the role of other parties involved such as the people with ADHD, parents and teachers. Twenty-two studies explored issues pertaining to a multidisciplinary approach, twelve from the US [31, 36,37,38,39,40,41, 64, 66, 69, 70, 73], five from the UK [3, 43, 454, 12, 15], two from Australia [49, 50], two from South Africa [53, 54] and one from the Netherlands [52].
-
The role of specialist and the importance of shared care
When discussing the concept of the multidisciplinary approach, many studies explored the communication between specialists, principally between primary and secondary care. With the belief that integrated care pathways and a collaborative approach is essential [15, 40, 44, 64], issues with communication between specialists was expressed as a major barrier [36, 39, 49, 50, 69]. In semi-structured interviews in the US [70], PCPs reported the importance of involvement of other stakeholders, psychiatrists, and schools in decision-making and over half of the professionals interviewed mentioned difficulties in communicating with other specialists. Furthermore, Ross [73] reported that only 15% of PCPs surveyed received communication from psychiatrists. Guevara [37] found similar issues with communication and a need for shared care; however, this paper acknowledged the breakdown of communication between parents, schools and physicians but not from a lack of will or desire, rather as a ‘System failure’—lack of accountability, discontinuity of care, lack of support, limited resources and finger pointing.
Ambiguity about the role of different professionals [11, 40, 41, 52] was also noted as a barrier to access to care. Klasen and Goodman [3] highlighted that most PCPs were not aware of specialist help available in their area and were not certain of whom to refer to.
-
The role of the school, parents and patients
Communication with other parties such as schools, parents and people with ADHD themselves was also reported as being a barrier. Four studies, for instance, mentioned that patients failing to turn up for appointments limited the PCPs’ ability to assess them and provide the right care [36, 44, 45, 69]. Other studies found that PCPs experienced considerable difficulties in getting information from parents and schools [31, 39, 73] as well as reporting feeling continued pressure for diagnosis from schools and parents [53, 54, 64]. In a US survey of 723 PCPs, Rushton et al. [66] found that 55% felt a strong pressure from teachers to diagnose ADHD while 70% felt pressure to prescribe medication. Kwasman et al. [38] reported that their large sample of school nurses highlighted a lack of multidisciplinary communication between PCPs and school staff and suggested that PCPs and schools would benefit from a greater understanding of the contributing that each could make to an effective ADHD assessment.
Facilitators
An integrated pathway between primary care and secondary care may provide the optional solution for ADHD assessment. Hassink-Franke et al. [52] in their study of Dutch PCPs highlighted that greater support and more constructive long-term relationships with secondary care enhanced PCP’s confidence about ADHD. Greater support for Dutch PCPs also allowed families of children with ADHD to received care from PCPs with whom they had a long-lasting relationship and allowed care to be provided in a more informal primary care context rather than more formal secondary care.
Discussion
This review concurs with findings from previous reviews [6.21] on the subject but by adding a larger body of literature, two new themes of internal and resource constraints and multidisciplinary approach were explored. It has found that a considerable number of barriers and facilitators such as lack of education, time and resource constraints, misconceptions and integrated pathways prevent PCPs from effectively supporting ADHD patients. By identifying these factors affecting access to care, this review establishes multiple areas of needs, enabling recommendations to facilitate PCPs’ ability in identifying and managing ADHD.
The need for education was the most highly endorsed factor overall, with PCPs reporting a general lack of education on ADHD. This need for education was observed on a worldwide scale; this factor was discussed in over 75% of our studies, in 12 different countries, suggesting that lack of education and inadequate education was the main barrier to understanding of ADHD in primary care. While this review reported both barriers and facilitators, barriers were mostly identified with very few facilitators. Overall, PCPs held a keen interest in gaining knowledge on ADHD, educational programs helped increase this knowledge and, over time, improved knowledge has been noticed. Studies investigating the presence of shared cared and integrated pathways reflect it to be the optimal solution. In conclusion, the main facilitator encompassing all themes in this review highlights the importance of providing any form of resources that would help PCPs facilitate access to care for individuals with ADHD.
However, resource constraints overall were an important barrier. While this factor was discussed as a separate theme, it also encompasses several other themes. Indeed, time and financial constraints affect the opportunities for PCPs to seek extra training and education but also affect the communication with other professionals such as secondary care workers, teachers and parents. This highlights further the difficulties faced daily by PCPs in recognising and managing patients with ADHD.
Strength and limitations
This review included different methodologies, qualitative, mixed methods and quantitative studies. Following the methods presented in our analyses, studies were considered separately (according to their methodology) at the analysis stage. We expected different methodologies to highlight different findings with one adding extra information to the other; however, for the majority of results, this was not the case. The different methodologies highlighted similar factors in understanding access to care for people with ADHD.
This review included a broad sample of studies from a worldwide perspective. Similar barriers were identified internationally, highlighting that these factors may not be culture dependent and appear to be widely generalisable. However, the majority of the studies were based in developed, western countries and more research in this area from developing countries in Asia and South America may allow subtler differences to emerge.
In many countries, pathways to care for adults and children are very distinct; therefore, divergent findings within adult and child studies might have been expected. However, no distinction was observed, with similar factors affecting both children and adults alike, determining that the barriers discussed in this review are relevant to different age groups and systems to care.
This review focused primarily on PCPs’ understanding and knowledge of ADHD, by including studies principally focusing on PCPs. A small but significant number of studies also included views from other parties such as parents and other professionals. It was interesting to notice that their views were in agreement with the findings generally observed and were not conflicting, adding validity to our overall observations.
By including different methodologies from multiple languages and following a strict systematic approach with clear transparency of the review process (including quality assessment, multiple reviewers and thorough data extraction method) this review included all relevant published studies on the subject and minimised the risk of biases.
However, a few limitations can be observed in this review. There was considerable variability in the quality of the included studies. Studies also varied considerably in the extent to which they contributed to the review, with some studies bearing more weight on our observations.
Barriers and facilitators were initially defined in order for this review to identify them as accurately as possible. However, most studies did not explicitly mention the terms ‘barriers’ and ‘facilitators’ and, therefore, these concepts were subject to our interpretations.
Only a small proportion of studies included in this review were published recently (11/48 studies since 2010). Thus, it is possible that while these findings were more relevant a decade or so ago, they might not be as significant if focused only on recent studies. While unlikely, possible reasons for fewer recent studies in this area might be that these issues are no longer as salient or that fewer studies are required as existing findings are still felt to be relevant. Further research is required in this important area.
Studies adopted different methodological approaches, including six qualitative and two mixed-method studies. While direct comparison between different methodological approaches was limited, most of this review’s findings were supported by both quantitative and qualitative studies with the exception of the role of the media which was only highlighted by qualitative studies.
It is important to note that the sample selected by these studies is selective. It has been observed that some PCPs do not believe in ADHD [74]. Therefore, it could be assumed that participating PCPs would likely have some openness or strong views about ADHD to take part. PCPs having strong beliefs about the existence (or not) of ADHD might not have been willing to partake in these studies and, therefore, their representation will be lacking from our findings. Finally, as this was a systematic review rather than a meta-analysis it was not possible to explore publication bias and its impact on study conclusions and our review.
Implication for practice
The potential barriers faced with knowledge of ADHD in primary care may lead to underdiagnosis or misdiagnosis, delays in being referred and lack of access to the right support [15]. Highlighting knowledge gaps can inform the development of future research, targeted interventions or psychoeducation programs for established PCPs as well as professionals in training. Increasing accurate knowledge of ADHD within this chosen population could improve recognition rates, benefiting patients and healthcare workers alike. Improvement in diagnosis could subsequently follow, either by more timely referral to secondary care services which are responsible for diagnosis (for instance, in UK population) or by quicker diagnosis in settings where PCPs are able to make a diagnosis (for instance, in US population). Better training of PCPs on ADHD is, therefore, necessary but to facilitate this, dedicated time and resources towards education needs to be put in place by service provider and local authorities. While the development of educational programs for PCPs seems to be the most characterised need, this issue requires further exploration and investigation as only two studies that investigated the benefits of an interventional program on PCPs [52, 56] were identified in this review, both with limited generalisability.
Implications for research
Although the need for the development of educational programs is strongly present, before instituting such programs in primary care settings, research on relevant and appropriate methods needs to be conducted. Developing the right intervention is essential as PCPs have very limited time and a lengthy full-day workshop, for instance, would not be easily accessible or provided for this population. Future research will also need to address more specifically the factors of resource constraints, misconceptions and multidisciplinary approaches, to overcome more specific challenges. These findings can then be used to develop more targeted strategies in enhancing access to care for ADHD.
While most studies in this review were quantitative, we believe mixed methods studies would be more beneficial in investigating these factors. Quantifying the effect of such factors on access to care is important but gaining an insight into the experience and attitudes of PCPs adds valuable knowledge on their individual beliefs, awareness and experience that is difficult to access through quantitative methods. In the context of this review, for instance, the link made between misconceptions and the role of the media and label was only made through the use of qualitative enquiries, quantitative methods might not have allowed this theme to emerge.
It is important to note that while this review focuses on primary care, our findings and previous studies [6] suggest that training teachers and parents could also be strongly beneficial in the process of continuing access to care for ADHD.
References
NICE (2013) Attention deficit hyperactivity disorder: diagnosis and management of ADHD in children, young people and adults. http://publications.nice.org.uk/attention-deficit-hyperactivity-disorder-cg72. Accessed 05 April 2017. National Institute for Clinical Excellence
Weiss M (2015) Functional impairment in ADHD. Attention-deficit hyperactivity disorder in adults and children, 42–52
Klasen H, Goodman R (2000) Parents and GPs at cross-purposes over hyperactivity: a qualitative study of possible barriers to treatment. Br J Gen Pract 50(452):199–202
Polanczyk G, De Lima MS, Horta BL, Biederman J, Rohde LA (2007) The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 164(6):942–948
Holden SE, Jenkins-Jones S, Poole CD, Morgan CL, Coghill D, Currie CJ (2013) The prevalence and incidence, resource use and financial costs of treating people with attention deficit/hyperactivity disorder (ADHD) in the United Kingdom (1998–2010). Child Adolesc Psychiatry Ment Health 7(1):34
Wright N, Moldavsky M, Schneider J, Chakrabarti I, Coates J, Daley D, Kochhar P, Mills J, Sorour W, Sayal K (2015) Practitioner review: pathways to care for ADHD—a systematic review of barriers and facilitators. J Child Psychol Psychiatry 56(6):598–617
Sayal K, Ford T, Goodman R (2010) Trends in recognition of and service use for attention-deficit hyperactivity disorder in Britain, 1999–2004. Psychiatr Serv 61(8):803–810
Sayal K, Hornsey H, Warren S, MacDiarmid F, Taylor E (2006) Identification of children at risk of attention deficit/hyperactivity disorder: a school-based intervention. Soc Psychiatry Psychiatr Epidemiol 41(10):806–813. https://doi.org/10.1007/s00127-006-0100-0
Sayal K, Taylor E, Beecham J (2003) Parental perception of problems and mental health service use for hyperactivity. J Am Acad Child Adolesc Psychiatry 42(12):1410–1414
Report NIoHCDC (2000) Diagnosis and treatment of attention deficit hyperactivity disorder (ADHD). J Pharm Care Pain Symptom Control 8(3):75–89
Salt N, Parkes E, Scammell A (2005) GPs’ perceptions of the management of ADHD in primary care: a study of Wandsworth GPs. Prim Health Care Res Dev 6(2):162–171. https://doi.org/10.1191/1463423605pc239oa
Bussing R, Zima BT, Gary FA, Garvan CW (2003) Barriers to detection, help-seeking, and service use for children with ADHD symptoms. J Behav Health Serv Res 30(2):176–189
Shaw M, Hodgkins P, Caci H, Young S, Kahle J, Woods AG, Arnold LE (2012) A systematic review and analysis of long-term outcomes in attention deficit hyperactivity disorder: effects of treatment and non-treatment. BMC Med 10(1):99
Sayal K, Mills J, White K, Merrell C, Tymms P (2015) Predictors of and barriers to service use for children at risk of ADHD: longitudinal study. Eur Child Adolesc Psychiatry 24(5):545–552. https://doi.org/10.1007/s00787-014-0606-z
Sayal K, Taylor E, Beecham J, Byrne P (2002) Pathways to care in children at risk of attention-deficit hyperactivity disorder. Br J Psychiatry 181(1):43–48
Ball C (2001) Attention-deficit hyperactivity disorder and the use of methylphenidate. Psychiatrist 25(8):301–304
Salmon G, Kirby A (2007) Attention deficit hyperactivity disorder: new ways of working in primary care. Child Adolesc Ment Health 12(4):160–163
Angermeyer MC, Dietrich S (2006) Public beliefs about and attitudes towards people with mental illness: a review of population studies. Acta Psychiatr Scand 113(3):163–179
Throckmorton PH (2000) Perceptions of practicing psychologists toward colleagues diagnosed with psychological problems. Dissertation Abs Int Sect B Sci Eng 61(3-B):1657
Asherson P, Akehurst R, Kooij JS, Huss M, Beusterien K, Sasané R, Gholizadeh S, Hodgkins P (2012) Under diagnosis of adult ADHD: cultural influences and societal burden. J Atten Disorders 16(5_suppl):20S–38S
Tatlow-Golden M, Prihodova L, Gavin B, Cullen W, McNicholas F (2016) What do general practitioners know about ADHD? Attitudes and knowledge among first-contact gatekeepers: systematic narrative review. BMC Fam Pract 17(1):129. https://doi.org/10.1186/s12875-016-0516-x
Kooij SJ, Bejerot S, Blackwell A, Caci H, Casas-Brugué M, Carpentier PJ, Edvinsson D, Fayyad J, Foeken K, Fitzgerald M (2010) European consensus statement on diagnosis and treatment of adult ADHD: the European network adult ADHD. BMC Psychiatry 10(1):67
Sandelowski M, Leeman J, Knafl K, Crandell JL (2013) Text-in-context: a method for extracting findings in mixed-methods mixed research synthesis studies. J Adv Nurs 69(6):1428–1437
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4(1):1
Van Lerberghe W (2008) The world health report 2008: primary health care: now more than ever. World Health Organization, Geneva
JBI (2014) Joanna Briggs Institute reviewers’ manual 2014 edition [Internet]. Adelaide: JBI; 2014 [cited 2015 May 15]. http://joannabriggs.org/assets/docs/sumari/ReviewersManual-2014.pdf. Accessed 14 Nov 2017
Pearson A, White H, Bath-Hextall F, Salmond S, Apostolo J, Kirkpatrick P (2015) A mixed-methods approach to systematic reviews. Int J Evid Based Healthc 13(3):121–131
Kmet LM, Lee RC, Cook LS (2004) Standard quality assessment criteria for evaluating primary research papers from a variety of fields, vol 22. Heritage Foundation for Medical Research Edmonton, Alberta
Braun V, Clarke V (2006) Using thematic analysis in psychology. Qual Res Psychol 3(2):77–101
Alder Lenard SD, David Sitt, Erica Maya, Morrill Melinda Ippolito (2009) Issues in the diagnosis and treatment of adult ADHD by primary care physicians. Prim Psychiatry 16(5):57–63
Chan E, Hopkins MR, Perrin JM, Herrerias C, Homer CJ (2005) Diagnostic practices for attention deficit hyperactivity disorder: a national survey of primary care physicians. Ambul Pediatr 5(4):201–208. https://doi.org/10.1367/A04-054R1.1
Clements AD, Polaha J, Dixon WE Jr, Brownlee J (2008) The assessment and treatment of attention-deficit hyperactivity disorder in primary care: a comparison of pediatricians and family practice physicians. J Rural Ment Health 32(1):5
Copeland L, Wolraich M, Lindgren S, Milich R, Woolson R (1987) Pediatricians’ reported practices in the assessment and treatment of attention deficit disorders. J Dev Behav Pediatr 8(4):191–197
Daly ME, Rasmussen NH, Agerter DC, Cha SS (2006) Assessment and diagnosis of attention-deficit/hyperactivity disorder by family physicians. Minn Med 89(3):40–43
Fiks AG, Gafen A, Hughes CC, Hunter KF, Barg FK (2011) Using freelisting to understand shared decision making in ADHD: parents’ and pediatricians’ perspectives. Patient Educ Couns 84(2):236–244. https://doi.org/10.1016/j.pec.2010.07.035
Goodman DW, Surman CB, Scherer PB, Salinas GD, Brown JJ (2012) Assessment of physician practices in adult attention-deficit/hyperactivity disorder. Prim Care Companion CNS Disorders. 14(4). https://doi.org/10.4088/PCC.11m01312
Guevara JP, Feudtner C, Romer D, Power T, Eiraldi R, Nihtianova S, Rosales A, Ohene-Frempong J, Schwarz DF (2005) Fragmented care for inner-city minority children with attention-deficit/hyperactivity disorder. Pediatrics 116(4):e512–e517. https://doi.org/10.1542/peds.2005-0243
Kwasman A, Tinsley B, Thompson S (2004) School nurses’ knowledge and beliefs about the management of children with ADD. J Sch Nurs 20(1):22–28
Power TJ, Mautone JA, Manz PH, Frye L, Blum NJ (2008) Managing attention-deficit/hyperactivity disorder in primary care: a systematic analysis of roles and challenges. Pediatrics 121(1):e65–e72. https://doi.org/10.1542/peds.2007-0383
Stein RE, Horwitz SM, Storfer-Isser A, Heneghan AM, Hoagwood KE, Kelleher KJ, O’Connor KG, Olson L (2009) Attention-deficit/hyperactivity disorder: how much responsibility are pediatricians taking? Pediatrics 123(1):248–255. https://doi.org/10.1542/peds.2007-3198
Thomas M, Rostain A, Corso R, Babcock T, Madhoo M (2015) ADHD in the college setting: current perceptions and future vision. J Atten Disord 19(8):643–654. https://doi.org/10.1177/1087054714527789
Williams J, Klinepeter K, Palmes G, Pulley A, Foy JM (2004) Diagnosis and treatment of behavioral health disorders in pediatric practice. Pediatrics 114(3):601–606. https://doi.org/10.1542/peds.2004-0090
Wolraich ML, Bard DE, Stein MT, Rushton JL, O’Connor KG (2010) Pediatricians’ attitudes and practices on ADHD before and after the development of ADHD pediatric practice guidelines. J Atten Disorder 13(6):563–572
Ayyash H, Colin-Thomé D, Sankar S, Merriman H, Vogt C, Earl T, Shah K, Banerjee S (2013) Multidisciplinary consensus for the development of ADHD services: the way forward. Clin Gov 18(1):30–38. https://doi.org/10.1108/14777271311297939
Baverstock A, Finlay F (2003) Who manages the care of students with attention deficit hyperactivity disorder (ADHD) in higher education? Child Care Health Dev 29(3):163–166
Klasen H (2000) A name, what’s in a name? The medicalization of hyperactivity, revisited. Harv Rev Psychiatry 7(6):334–344
Murray G, McKenzie K, Brackenridge R, Glen S (2006) General practitioner knowledge about psychological approaches to ADHD. In: Clinical psychology forum, vol 158. British Psychological Society, pp 13–16
Dryer R, Kiernan MJ, Tyson GA (2006) Implicit theories of the characteristics and causes of attention-deficit hyperactivity disorder held by parents and professionals in the psychological, educational, medical and allied health fields. Aust J Psychol 58(2):79–92. https://doi.org/10.1080/00049530600730443
Shaw K, Mitchell G, Wagner I, Eastwood H (2002) Attitudes and practices of general practitioners in the diagnosis and management of attention-deficit/hyperactivity disorder. J Paediatr Child Health 38(5):481–486
Shaw K, Wagner I, Eastwood H, Mitchell G (2003) A qualitative study of Australian GPs’ attitudes and practices in the diagnosis and management of attention-deficit/hyperactivity disorder (ADHD). Family Pract 20(2):129–134
Fuermaier AB, Tucha L, Koerts J, Mueller AK, Lange KW, Tucha O (2012) Measurement of stigmatization towards adults with attention deficit hyperactivity disorder. PLoS ONE 7(12):e51755. https://doi.org/10.1371/journal.pone.0051755
Hassink-Franke LJ, Janssen MM, Oehlen G, van Deurzen PA, Buitelaar JK, Wensing M, Lucassen PL (2016) GPs’ experiences with enhanced collaboration between psychiatry and general practice for children with ADHD. Eur J Gen Pract 22(3):196–202. https://doi.org/10.1080/13814788.2016.1177506
Louw C, Oswald M, Perold M (2009) General practitioners’ familiarity, attitudes and practices with regard to attention deficit hyperactivity disorder in children and adults. South African Family Pract 51:(2)
Venter A, Van der Linde G, Joubert G (2003) Knowledge, attitudes and practices of general practitioners in the free state regarding the management of children with attention deficit hyperactivity disorder (ADHD). South African Family Pract 45(5):12–17
Miller AR, Johnston C, Klassen AF, Fine S, Papsdorf M (2005) Family physicians’ involvement and self-reported comfort and skill in care of children with behavioral and emotional problems: a population-based survey. BMC family practice 6(1):12
Ward R, Fidler H, Lockyer J, Toews J (1999) Physician outcomes and implications for planning an intensive educational experience on attention-deficit hyperactivity disorder. Acad Med 74(10):S31–S33
Quiviger S, Caci H (2014) A survey on attention deficit hyperactivity disorder. Archives de pediatrie: organe officiel de la Societe francaise de pediatrie 21(10):1085–1092
Lian W, Ho S, Yeo C, Ho L (2003) General practitioners’ knowledge on childhood developmental and behavioural disorders. Singap Med J 44(8):397–403
Jawaid A, Zafar A, Naveed A, Sheikh S, Waheed S, Zafar M, Syed E, Fatmi Z (2008) Knowledge of primary paediatric care providers regarding attention deficit hyperactivity disorder and learning disorder: a study from Pakistan. Singap Med J 49(12):985
Heikkinen A, Puura K, Ala-Laurila EL, Niskanen T, Mattila K (2002) Child psychiatric skills in primary healthcare–self-evaluation of Finnish health centre doctors. Child Care Health Dev 28(2):131–137
Gomes M, Palmini A, Barbirato F, Rohde LA, Mattos P (2007) Knowledge about attention-deficit hyperactivity disorder in Brazil. J Brasileiro de Psiquiatria 56(2):94–101
Ghanizadeh A, Zarei N (2010) Are GPs adequately equipped with the knowledge for educating and counseling of families with ADHD children. BMC Family Pract 11:5
Gamma AX, Müller A, Candrian G, Eich D (2017) Attention deficit/hyperactivity disorder in Swiss primary care. Swiss Arch Neurol Psychiatry Psychother 168(2):41–47
Evink B, Crouse BJ, Elliott BA (2000) Diagnosing childhood attention-deficit/hyperactivity disorder Do family practitioners and pediatricians make the same call? Minn Med 83(6):57–62
Lanham JS (2006) The evaluation of attention deficit/hyperactivity disorder in family medicine residency programs. South Med J 99(8):802–806
Rushton JL, Fant KE, Clark SJ (2004) Use of practice guidelines in the primary care of children with attention-deficit/hyperactivity disorder. Pediatrics 114(1):e23–e28
Wasserman RC, Kelleher KJ, Bocian A, Baker A, Childs GE, Indacochea F, Stulp C, Gardner WP (1999) Identification of attentional and hyperactivity problems in primary care: a report from pediatric research in office settings and the ambulatory sentinel practice network. Pediatrics 103(3):e38
Gardner W, Pajer KA, Kelleher KJ, Scholle SH, Wasserman RC (2002) Child sex differences in primary care clinicians’ mental health care of children and adolescents. Arch Pediatr Adolesc Med 156(5):454–459
Kwasman A, Tinsley BJ, Lepper HS (1995) Pediatricians’ knowledge and attitudes concerning diagnosis and treatment of attention deficit and hyperactivity disorders: a national survey approach. Arch Pediatr Adolesc Med 149(11):1211–1216
Fiks AG, Hughes CC, Gafen A, Guevara JP, Barg FK (2011) Contrasting parents’ and pediatricians’ perspectives on shared decision-making in ADHD. Pediatrics 127(1):e188–e196. https://doi.org/10.1542/peds.2010-1510
Leslie LK, Stallone KA, Weckerly J, McDaniel AL, Monn A (2006) Implementing ADHD guidelines in primary care: does one size fit all? J Health Care Poor Underserved 17(2):302–327. https://doi.org/10.1353/hpu.2006.0064
Sleator EK, Ullmann RK (1981) Can the physician diagnose hyperactivity in the office? Pediatrics 67(1):13–17
Ross WJ, Chan E, Harris SK, Goldman SJ, Rappaport LA (2011) Pediatrician-psychiatrist collaboration to care for children with attention deficit hyperactivity disorder, depression, and anxiety. Clin Pediatr 50(1):37–43
Saul R (2014) ADHD does not exist: the truth about attention deficit and hyperactivity disorder. New York-Harper Wave
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Daley reports grants, personal fees and non-financial support from Shire, personal fees and non-financial support from Medice, personal fees and non-financial support from Eli Lilly, non-financial support from QbTech, other from Jessica Kingsley from, outside the submitted work. Ms French reports personal fees and non-financial support from Shire. Dr Sayal reports no conflicts of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
French, B., Sayal, K. & Daley, D. Barriers and facilitators to understanding of ADHD in primary care: a mixed-method systematic review. Eur Child Adolesc Psychiatry 28, 1037–1064 (2019). https://doi.org/10.1007/s00787-018-1256-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-018-1256-3