
Abstract
Objectives
To analyze factors predicting mandibular cortical width (MCW) and mandibular cortical index (MCI) in adult females and males.
Material and methods
Data on 427 females and 335 males aged 40–84 from The Tromsø study: Tromsø7 were used. T-score, age, menopausal status (for females), remaining teeth, and periodontal status were analyzed in linear and logistic regression analyses as predictors of MCW and MCI, respectively.
Results
T-score, age, and the number of remaining teeth significantly predicted MCW in females but not males. Standardized β coefficients were 0.286, −0.231, and 0.131, respectively. The linear regression model explained 24% of MCW variation in females. MCI in females was significantly predicted by T-score, age, and remaining teeth with the Wald values of 9.65, 6.17, and 5.83, respectively. The logistic regression model explained 16.3−23% of the variation in MCI in females. In males, T-score was the only significant predictor of the eroded cortex, and the logistic model explained only 4.3–5.8% of the variation in MCI.
Conclusions
The T-score demonstrated a stronger relationship with MCW and MCI than other factors in females, which supports the usefulness of those indices for osteoporosis screening. Conversely, the T-score exhibited no association with MCW and remained the only significant predictor of MCI in males, yet to a lesser extent than in females.
Clinical relevance
Understanding factors affecting mandibular cortical morphology is essential for further investigations of MCW and MCI usefulness for osteoporosis screening in females and males.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a chronic, non-communicable disease that deteriorates bone tissue and makes bones fragile and prone to fractures which are considered a public health problem due to increased mortality risk and considerable health costs [1,2,3]. Genetic factors and sex define bone mass and structure to a great extent, and osteoporosis is more prevalent in females than in males [3, 4]. Both males and females reach their peak bone mass approximately in their 20s; after that, gradual bone loss starts in both sexes in their third decade due to reduced osteoblast activity [3, 5], and accelerates faster in females in post-menopause due to declining estrogen levels [6].
There are associations between jawbone morphology and the state of bone tissue in the whole body. For example, a moderate positive correlation was found between the mandible’s bone mineral density (BMD), specifically BMD of the buccal mandibular cortex, and femoral neck BMD [7]. Furthermore, the morphology of the mandibular cortex assessed on dental panoramic radiographs was associated with skeletal bone turnover in elderly females [8]. These findings were supported by further research collected in two systematic reviews showing that changes in mandibular cortical morphology on dental panoramic radiographs could predict low BMD or osteoporosis in women [9,10,11]. Two radiomorphometric indices, i.e., mandibular cortical width (MCW) and mandibular cortical index (MCI), were extensively studied as potentially useful for osteoporosis screening [12].
Nevertheless, little is known about the extent to which different factors are associated with the morphology of the mandibular cortex, while this knowledge is essential for supporting or arguing against using radiomorphometric indices for osteoporosis screening. Such studies are specifically lacking in males [13, 14]. Some studies have shown that age and gender are significant predictors of the thin and eroded cortex; however, their analyses did not account for T-score or other possible factors [15, 16].
Mechanical loading is also important for building and maintaining bone tissue [17]. An animal study showed that rats with a soft diet had lower BMD of mandibles than rats eating solid food [18]. Dental practitioners observe alveolar bone loss after tooth extraction, although it occurs to various extents in different individuals [17]. Tooth loss may affect parts of the mandible other than the alveolar ridge; Taguchi et al. found that the number of remaining teeth adjusted for age was related to mandibular cortex morphology in women [19]. Dutra et al. found an association between remaining teeth and cortical thickness in the antegonial region of the mandible, which might confound relationships between cortical thickness and osteoporosis [20].
One of the most common reasons for tooth loss is periodontitis — an inflammatory disease affecting tooth-supportive structures called periodontium. Dental plaque bacteria induce inflammation in the periodontium, which is subsequently modified by a host immune response. Inflammatory cells release cytokines that activate osteoclasts, while the latter initiate resorption of the alveolar bone surrounding teeth [21]. The mechanistic links between osteoporosis and periodontitis have been studied but remained unclear [22]. There is emerging evidence that patients with periodontitis exhibit a general inflammatory response with elevated levels of C-reactive protein and inflammatory cytokines, including those activating osteoclasts, while osteoclasts are responsible for bone resorption [21, 23,24,25]. Thus, periodontitis might also be a factor influencing the mandibular cortical bone.
To our knowledge, none of the previous studies have examined the contribution of different factors to the morphology of the mandibular cortex. This study aimed to analyze the relationship between general factors such as skeletal BMD, age, and menopausal status (for females), local factors, such as the number of teeth and periodontal status, and the morphology of mandibular cortex measured by MCW and MCI on dental panoramic radiographs in males and females.
Material and methods
The Tromsø Study is an ongoing population-based study initiated in 1974 and carried out as repeated cross-sectional surveys in Tromsø, Norway. The data from the seventh survey (Tromsø7) was used in the current study. All inhabitants of Tromsø aged over 40 (n=32,591) were invited to participate in Tromsø7, and 21,083 consented, yielding a response rate of 65% [26]. They filled out extensive questionnaires on various health-related topics. All study participants reported their ages and sex, and females reported their menopausal status in the questionnaires. Further information on the Tromsø7 sampling procedure and data collection is available elsewhere [26].
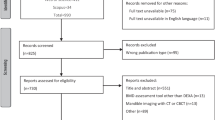
Three thousand nine hundred fifty-one randomly selected participants (Fig. 1) underwent a dental panoramic radiograph (DPR) examination and extensive dental clinical examination during the first visit. Planmeca ProMax 2-Dimensional S3 Dimax-4 panoramic unit (Planmeca Oy, Helsinki, Finland) was used for DPRs acquisition. During a dental examination, bleeding on probing (BOP) and periodontal probing depth (PPD) were recorded at four sites of each toot at all teeth except the third molars. PPD was measured to the closest millimeter with a periodontal probe (WHO probe LM555B). Radiographic marginal bone level (RBL) of interproximal surfaces of all teeth except third molars was measured on DPRs, according to Holde et al. [27]. Periodontitis was defined according to the classification by the American Academy of Periodontology and European Federation of Periodontology, launched in 2017 [28]. Prevalent periodontitis was determined and further classified by stages if RBL was observed at two or more non-adjacent teeth and further classified by stages. Stage I was defined as RBL<15% and PPD ≤4 mm, stage II as RBL of 15–33% and PPD ≤5 mm, or RBL<15% and PPD 5 mm, and stage III–IV as RBL>33%, or <33% RBL and PPD ≥6 mm. Stage III and IV collapsed due to a few cases. Information on the reason for tooth loss, complexity factors, vertical bone loss, furcation involvement, ridge defects, tooth mobility, masticatory dysfunction, and bite collapse/drifting/flaring was unavailable. Non-periodontitis cases were defined as BOP at less than 10% of sites, and gingivitis cases as BOP ≥10% [29]. Periodontal stability was defined as RBL detectable at two or more non-adjacent teeth but no PPD >3 mm.

Selection of the study participants
At the second visit, another 3600 participants, who were randomly selected from the 21,083 Tromsø7 participants attending the first visit, received bone mineral density examination (BMD) using dual-energy x-ray absorptiometry (DEXA) (Fig. 1). Lunar Prodigy device (GE Health-care Lunar, Madison, WI, USA) was used to measure BMD and T-scores at the left and right femoral necks. T-score is a ratio of the difference between the patient’s BMD and the mean BMD of the young sex-matched adult (reference BMD) to the standard deviation of the reference BMD. This study used a Lunar reference from the US reference population. The T-score was expressed in standard deviations (S.D.). The minimum T-score from either the left or right femoral neck of each participant was used in this study.
Seven hundred seventy-three participants aged 40 to 84 underwent DEXA and DPR examinations and were included in our cross-sectional study (Fig. 1). Eleven DPRs were excluded due to inferior quality or being used as reference images for MCI assessment. We measured MCW and MCI using ImageJ 1.8.0172 software (U.S. National Institutes of Health, Bethesda, MD, USA) [30] on the rest 762 DPRs. MCW was measured bilaterally along the line drawn through the middle of the mental foramen and perpendicular to the lower mandibular border, as proposed by Ledgerton et al. [31], where MCW is the shortest distance between the upper and the lower borders. In this study, we use an average MCW value of the left and the right side of individuals, and the unit of MCW is a millimeter. Since no reference object was used to control for magnification, all linear measurements were adjusted for a magnification factor of 20%, indicated by the manufacturer. MCI of the cortex was classified into three categories: C1, even and sharp endosteal margin on both sides of the mandible (normal cortex); C2, some endosteal cortical residues, and semilunar defects on one or both sides (mildly eroded cortex); and C3, heavy endosteal cortical residues, the cortical bone is porous on one or both sides (severely eroded cortex). Details of image processing, MCW, and MCI measurements are available from our previous study [32].
Statistical analyses were conducted using IBM SPSS Statistics for Windows version 26.0. MATLAB (version R2021b, The MathWorks Inc., Natick, Massachusetts) was used to make plots. The normality of distribution was assessed by visual examinations of histograms, Q-Q plots, skewness, and kurtosis values. All continuous predictors were normally distributed except the number of remaining teeth. Inter- and intra-observer reliabilities of MCW and MCI were reported in the previous study [32].
Person and Spearman’s correlation coefficients were calculated for normally and non-normally distributed continuous predictors to analyze their correlations with MCW. Hierarchical linear regression analysis was used to analyze relationships among general predictors (T-score, age, and menopausal status), local predictors (remaining teeth and periodontal status), and MCW. Age was added to the first block, T-score, and menopausal status were added to the second block, while remaining teeth and periodontal status were added to the third block. Standardized β coefficients were used to compare the strength of associations between the predictors and MCW. The linear model assumptions were met, and influential cases were detected in neither females nor males.
Hierarchical logistic regression analysis with the same blocks was used to assess relationships among general, oral predictors, and MCI. MCI was used as a binary outcome (C1 – even and smooth cortex vs. C2, C3 – mildly or severely eroded cortex) due to the low number of participants having the C3 category (55 females and one male). Wald statistics were used to compare the strength of associations between the predictors and MCI. The logistic model assumptions were met.
All regression analyses were carried out separately for males and females. Age was used as a continuous predictor in linear regression and a categorical predictor in logistic regression with the following groups: 40–49; 50–59; 60–69; 70–79; 80+. T-score was used as a continuous predictor with a 0.1 SD increment. Periodontal status was divided into three following groups: non-periodontitis or mild periodontitis (health, gingivitis, stage I), moderate periodontitis (stage II), or severe periodontitis (stage III, IV) in both linear and logistic regression analyses. Missing values were excluded pairwise. Data on menopausal status was available for 419 females. Periodontal status for edentulous individuals and individuals with periodontal stability was not included in the regression model, while there were 15 females and 6 males for whom periodontal data was missing. Thus, the total number of females and males having data on periodontal status and included in the regression analysis was 310 and 272, respectively. Other predictors did not have missing values.
Results
Table 1 presents the characteristics of the study participants by sex. The average MCW was 3.3 mm in females and 4.0 mm in males. Most females (57%) had mildly eroded cortexes, 12.9% had severely eroded, and 30.1% had dense cortexes. Most males (59.1%) had dense cortexes, 40.6% had mildly eroded cortexes, and only one male had severely eroded cortex.
All continuous predictors were significantly correlated with MCW in females (Table 2). Age showed a negative correlation with MCW, with a coefficient of −0.38. Figure 2a presents the means and the distributions of MCW in females by age, showing a tendency to have a thinner cortex with age. T-score and the number of remaining teeth showed positive correlations with MCW with coefficients of 0.40 and 0.34, respectively (Table 2). Figure 2b shows a tendency for a thinner cortex with a decreasing T-score. In the simple linear regression analyses in females, all predictors except periodontal status were significantly associated with MCW, as suggested by unadjusted β coefficients with their confidence intervals (Table 2). In multiple linear regression analysis, T-score, age, and the number of teeth remained significantly associated with MCW. Every 0.1 SD lowered T-score resulted in 0.25-mm thinner MCW. One year increase in age was associated with a 0.02-mm reduction in MCW in females. Each additional remaining tooth was associated with having a 0.01-mm thicker cortex. T-score contributed the most to the variation in MCW in females, with the standardized β of 0.286, followed by age and remaining teeth with the standardized β’s of −0.231 and 0.131, respectively. The multiple linear regression model for females significantly predicted MCW (F=18.7, p<0.001). The model explained 24.0% of the variation in MCW in females (R2=0.240).

Box plots show mean MCW (filled triangles), its confidence intervals (boxes), and its distribution (vertical lines) in different ages in females (a) and males (c) and for different T-scores in females (b) and males (d). Solid lines are regression lines, while dotted lines are confidence intervals for the regression lines
In males, only T-score correlated with MCW (r=0.14, p=0.009) (Table 2). Males did not tend to have thinner cortexes with older age (Fig. 2c). A significant association between the T-score and MCW with an unadjusted β coefficient of 0.09 was observed in males in simple linear regression analysis. Figure 2d shows that males tended to have a thinner cortex with decreasing T-score. However, this tendency was less pronounced in males than females. In the multiple linear regression analysis, none of the predictors showed associations with MCW in males (Table 2). The overall model did not predict MCW in males (F=2.2, p=0.059).
In females, all predictors except periodontal status showed significant associations with MCI in the binary logistic regression analysis (Table 3), while multiple logistic regression analysis suggests that T-score, age, and the number of remaining teeth were significantly associated with C2 or C3. A 0.1 SD reduction in T-score increased the odds of having C2 or C3 by 38% (OR 0.62, 95% CI, 0.46; 0.84). Being a decade older resulted in 1.65 (95% CI, 1.11; 2.44) times higher odds of having mildly or severely eroded cortex in females. Every remaining tooth was associated with a significant reduction of 7% in the odds of having C2 or C3 (OR=0.93, 95% CI, 0.87; 0.98). T-score was the strongest predictor of MCI in females, as demonstrated by the Wald statistic value of 9.65. The overall model significantly predicted mildly or severely eroded cortices (p <0.001) and explained 16.3–23.0% of the variation in MCI, as suggested by Cox&Snell and Negelkerke tests.
Binary logistic regression analyses in males show a similar result to females in which all predictors except periodontal status were significantly associated with MCI (Table 3). Multiple logistic regression analysis suggests that T-score remained significantly associated with MCI with an odds ratio of 0.73 (95% CI, 0.56; 0.96). The overall model significantly predicted mildly (C2) or severely (C3) eroded cortex in males (p=0.017) but explained only 4.3-5.8% of the variation in MCI.
Discussion
This study analyzed the relationship among general (sex, age, T-score, menopausal status), local factors (remaining teeth and periodontal status), and morphology of the mandibular cortex assessed by MCW or MCI. All factors together explained the variation in MCW and MCI in females more than in males.
T-score was the strongest predictor of MCW and MCI in females, while in males, T-score was the only significant factor associated with MCI. Previous studies mainly assessed the diagnostic efficacy of radiomorphometric indices for osteoporosis screening [9, 11]. Fewer studies explored the association between MCW, MCI, and BMD in females or males [13, 33, 34]. Analyzing the relationships between radiomorphometric indices and BMD and considering relevant confounding factors is necessary to support using these indices for osteoporosis screening, specifically in males, in whom such studies are lacking. Even though we cannot directly compare the odds ratios and β coefficients from other studies with ours due to different methods and regression models used, it is evident from previous research that females with lower skeletal BMD have thinner and more eroded cortexes [34,35,36,37]. A positive correlation between T-score and MCW in females ranging from 0.33 to 0.45 in previous studies was consistent with our findings [34,35,36]. Our study found no significant association between T-score adjusted for other factors and MCW in males. In contrast, two previous studies found an association of thin MCW in males with osteoporosis (T-score ≤ −2.5 SD) [13, 38]. Unlike our study, Leite et al. also found a correlation coefficient of 0.29 for MCW and BMD at the femoral neck in males [13]. Nevertheless, MCI was associated with T-score in males in this study, which was consistent with Leite et al. [13], while another study did not find such an association [38]. This divergence in findings might be related to smaller study samples, differences in sampling procedures, or a lack of adjustment for other factors in previous studies.
Age was another major contributor to MCW and MCI in females but not males. Our results align with previous studies that found an interaction between age and sex in the way that cortical thickness reduced more prominently in females than males [15, 19, 20, 39]. Similar trends were observed in other studies exploring the bone geometry and cortical thickness at different skeletal sites in relation to age and sex [40, 41]. A plausible biological explanation for maintaining mandibular cortical thickness in older men could be sex hormones, which play a crucial role in bone formation and resorption. Estrogens increase endosteal and reduce periosteal bone formation in females during puberty, while androgens accelerate periosteal bone formation in growing males [4, 5]. These physiological mechanisms contribute to sex dimorphism in the adult skeleton. After a certain age, bone resorption exceeds bone formation at the inner bone surface in both sexes. However, bone formation continues at the outer bone surface faster in males than in females due to androgens. Thus, males maintain their cortical bone not because they lose less endosteal bone than women but due to a greater periosteal formation [5]. Our study also found that age was a significant predictor for MCI in females but not males (Tables 2 and 3). On the contrary, several studies found that MCI became more eroded with age, regardless of gender [39, 42, 43]. At the same time, those studies did not consider other confounding factors, which may partly explain the disagreement between ours and previous findings. However, one of the studies was longitudinal, which strengthened their results compared to ours [43].
In our study, the number of remaining teeth was significantly associated with MCW and MCI in females but not males (Tables 2 and 3). It is well established in previous research that mechanical strains and subsequent osteocyte response define the geometry and morphology of skeletal bones [44,45,46]. Thus, it would be appropriate to hypothesize that the lack of loading forces in edentulous people or those with fewer teeth can independently influence the mandibular cortex. Several studies have found an association between remaining teeth and mandibular cortical morphology, even when controlling for age [16, 19, 20, 42]. Okabe et al. found that the number of remaining teeth was weakly correlated with MCW equally for both sexes (0.19 male and 0.14 female) [14]. Dutra et al. found that the number of remaining teeth was related to the thickness of the mandibular cortex, irrespective of gender [20]. Unlike Okabe et al. and Dutra et al., we did not find relationships between remaining teeth and radiomorphometric indices in males. Our results were consistent with Taguchi et al., who also found no relationships between remaining teeth on both the upper and lower jaws and MCW in males [19]. However, considering only mandibular teeth might be more logical, like some previous studies, since we assess the mandibular cortex [16, 20]. Despite the significant association in females, remaining teeth contributed to the thin and eroded cortex to a minor extent. Similar to our study, Legerton et al. and Gulsahi et al. showed that the influence of dentition on cortical erosion and cortical thickness in the antegonial region was weaker than that of age [16, 42].
In our study, menopausal status was significantly associated with MCW and MCI in univariate analysis but not after adjustments, meaning that the other factors confounded this association greatly. Unlike our results, two previous studies found an association between menopausal status and MCW and MCI but did not consider other relevant confounding factors [47, 48].
The association between periodontitis and mandibular cortical morphology is poorly studied. Recent systematic reviews have shown that many studies have explored the effect of osteoporosis on periodontal health [22, 49]. However, some researchers hypothesized the opposite relationship. Two longitudinal studies explored the independent effect of periodontal disease on skeletal bone tissue and found an increased risk of osteoporosis among people diagnosed with periodontitis after accounting for confounders [50, 51]. The rationale behind those hypotheses was that patients with periodontitis exhibit higher systemic levels of inflammatory mediators such as interleukin (IL-2, IL-6) and tumor necrosis factor (TNF-α) [24]. Those inflammatory mediators affect the remodeling of bone tissue and may thus increase the risk of osteoporosis development [52, 53]. One can also speculate that periodontitis may influence the mandibular cortex via systemic inflammation mechanisms. Tooth loss and mobility due to severe periodontitis leading to a lack of mechanical loading may also influence mandibular cortex morphology.
Unlike few existing studies on the subject, this study found no relationship between mandibular cortical morphology (MCW and MCI) and periodontal status for females or males [47, 48]. That might be due to the difference in study design, the wide variation of periodontal measurements, and case definitions in the literature, which makes comparisons between studies difficult. A recent study exploring the utility of the new periodontal disease classification found that different classification systems affect association estimates in epidemiological studies to a great extent, and the utility of the new classification is not well-studied [54]. The 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions came to a consensus that staging in periodontitis diagnosis should be based on clinical attachment loss (CAL), RBL, PPD, and other factors like teeth missing due to periodontitis [28]. First, CAL and the reason for tooth loss were unavailable in our study. Had we obtained this additional information, the classification of study participants into the periodontal disease categories would probably have changed. Second, PPD is a parameter that reflects the extent of current inflammatory processes, while RBL reflects patients’ periodontal disease experience in the past. It is unclear which parameter is most appropriate when exploring the link between periodontal disease and mandibular cortical morphology. Common sense suggests that cortical bone loss does not occur quickly under an inflammatory process; therefore, RBL as a sign of periodontitis history rather than PPD should be used to explore the abovementioned link. In support of this statement, the systematic review of the association between periodontitis and osteoporosis found that most studies using radiological criteria to define a periodontal case showed significant associations with osteoporosis. At the same time, results were more controversial for studies using clinical measurements for case definition [22].
Another factor that can potentially influence mandibular cortical morphology but has not been included in this study is the mechanical bone load produced by masticatory muscles. It has been previously reported that masticatory load affects both the trabecular and cortical bone in different mandibular regions but predominantly in the angle of the mandible [55,56,57]. Different types of face anatomy are associated with various masticatory loads: individuals with a short face type (hypo-divergent) have a small mandibular angle and short masticatory muscles with increased masticatory function. In contrast, those with long face types (hyper-divergent) have a large mandibular angle, longer muscles, and decreased masticatory function [58]. A study by Gonca et al., published in 2023, found that individuals with hyper-divergent type exhibited less dense trabecular bone at ramus, condyle, sigmoid notch, and mandibular angle, while mandibular cortical width was thinner only in the second molar projection [59]. Since only DPRs were available in this study, while lateral cephalometric radiographs are commonly used to assess vertical facial type, we could not assess the potential association of masticatory load with the morphology of the mandibular cortex. It might be worthwhile to study this association in future research.
The current study has several limitations. First, it is a cross-sectional study. Despite the arguments regarding the possible links between sex, bone mineral density, age, remaining teeth, periodontitis, and mandibular cortex, we cannot infer the directions of these relationships. Another limitation is the suboptimal inter- and inter-observer agreement of radiomorphometric indices reported in our previous work [32]. Moreover, the panoramic radiographs in this study were not standardized using reference objects, i.e., we could not make precise corrections of MCW for magnification. In addition, the classification of periodontitis is likely to be biased because RBL measurements were performed on DPRs, which distort spatial relationships between anatomical structures to some extent. At the same time, the superimposed cervical spine often hinders bone measurements in the anterior region of the jaws. Suboptimal observer agreement, spatial distortion inherent to DPRs, and image distortion due to the patient’s head misalignment were likely to produce random errors and a substantial unexplained variation in mandibular cortical morphology.
Conclusion
T-score followed by age contributed most to variation in MCW and MCI in females, supporting the idea of using MCW and MCI for osteoporosis screening for females. Nonetheless, neither general nor local predictors explained the variation in MCW in males. Only the T-score was associated with male MCI, though the association was weaker than in females.
Data Availability
The data supporting this study's findings is available from the Tromsø Study but is not publicly accessible due to licensing restrictions. Researchers affiliated with the institutions with research expertise can access the data upon application to the Data and Publication Committee for the Tromsø Study (https://uit.no/research/tromsostudy).
References
Kanis JA, Cooper C, Rizzoli R, Reginster J-Y (2019) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 30(1):3–44. https://doi.org/10.1007/s00198-018-4704-5
Kanis JA, Norton N, Harvey NC, Jacobson T, Johansson H, Lorentzon M et al (2021) SCOPE 2021: a new scorecard for osteoporosis in Europe. Arch Osteoporos 16(1):82. https://doi.org/10.1007/s11657-020-00871-9
Epidemiology of osteoporosis and fragility fractures 9, rue Juste-Olivier, CH-1260 Nyon, Switzerland: International Osteoporosis Foundation; [cited 2023 Feb 15]. Available from: https://www.osteoporosis.foundation/facts-statistics/epidemiology-of-osteoporosis-and-fragility-fractures.
Callewaert F, Sinnesael M, Gielen E, Boonen S, Vanderschueren D (2010) Skeletal sexual dimorphism: relative contribution of sex steroids, growth hormone-insulin-like growth factor-I (GH-IGF-I) and mechanical loading. J Endocrinol 207(2):127–134. https://doi.org/10.1677/JOE-10-0209
Seeman E (2001) Sexual Dimorphism in Skeletal Size, Density, and Strength. J Clin Endocrinol Metabol 86(10):4576–4584. https://doi.org/10.1210/jcem.86.10.7960
Weaver CM, Gordon CM, Janz KF, Kalkwarf HJ, Lappe JM, Lewis R et al (2016) The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: a systematic review and implementation recommendations. Osteoporos Int 27(4):1281–1386. https://doi.org/10.1007/s00198-015-3440-3
Klemetti E, Vainio P, Lassila V, Alhava E (1993) Cortical bone mineral density in the mandible and osteoporosis status in postmenopausal women. Eur J Oral Sci 101(4):219–223. https://doi.org/10.1111/j.1600-0722.1993.tb01108.x
Morita IDDSP, Nakagaki HDDSP, Taguchi ADDSP, Kato KDDSP, Murakami TDDSP, Tsuboi SDDSP et al (2009) Relationships between mandibular cortical bone measures and biochemical markers of bone turnover in elderly Japanese men and women. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108(5):777–783. https://doi.org/10.1016/j.tripleo.2009.03.043
Calciolari E, Donos N, Park JC, Petrie A, Mardas N (2015) Panoramic measures for oral bone mass in detecting osteoporosis: a systematic review and meta-analysis. J Dent Res 94:17–27. https://doi.org/10.1177/0022034514554949
Taguchi A, Tanaka R, Kakimoto N, Morimoto Y, Arai Y, Hayashi T et al (2021) Clinical guidelines for the application of panoramic radiographs in screening for osteoporosis. Oral Radiol 37(2):189–208. https://doi.org/10.1007/s11282-021-00518-6
Kinalski MA, Boscato N, Damian MF (2020) The accuracy of panoramic radiography as a screening of bone mineral density in women: a systematic review. Dentomaxillofacial Radiol 49(2):20190149. https://doi.org/10.1259/dmfr.20190149
Yeung AWK, Mozos I (2020) The innovative and sustainable use of dental panoramic radiographs for the detection of osteoporosis. Int J Environ Res Public Health 17(7):2449. https://doi.org/10.3390/ijerph17072449
Leite AF, de Souza Figueiredo PT, Barra FR, de Melo NS, de Paula AP (2011) Relationships between mandibular cortical indexes, bone mineral density, and osteoporotic fractures in Brazilian men over 60 years old. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 112(5):648–656. https://doi.org/10.1016/j.tripleo.2011.06.014
Okabe S, Morimoto Y, Ansai T, Yoshioka I, Tanaka T, Taguchi A et al (2008) Assessment of the relationship between the mandibular cortex on panoramic radiographs and the risk of bone fracture and vascular disease in 80-year-olds. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106(3):433–442. https://doi.org/10.1016/j.tripleo.2007.09.013
Roberts M, Yuan J, Graham J, Jacobs R, Devlin H Changes in mandibular cortical width measurements with age in men and women. Osteoporosis Int. [Internet]. 2011 [cited 2022 Jan 9] 22(6):1915–1925. https://doi.org/10.1007/s00198-010-1410-3
Ledgerton D, Horner K, Devlin H, Worthington H Radiomorphometric indices of the mandible in a British female population. Dento-Maxillo-Facial Radiol 28(3):173–181 Available from: https://www.ncbi.nlm.nih.gov/pubmed/107404731999 [cited 2021 Nov 25]
Jonasson G, Skoglund I, Rythén M (2018) The rise and fall of the alveolar process: Dependency of teeth and metabolic aspects. Arch Oral Biol 96:195–200. https://doi.org/10.1016/j.archoralbio.2018.09.016
Kiliaridis S, Bresin A, Holm J, Strid K-G (1996) Effects of masticatory muscle function on bone mass in the mandible of the growing rat. Cells Tissues Organs 155(3):200–205. https://doi.org/10.1159/000147805
Taguchi A, Tanimoto K, Suei Y, Wada T (1995) Tooth loss and mandibular osteopenia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 79(1):127–132. https://doi.org/10.1016/S1079-2104(05)80088-5
Dutra V, Yang J, Devlin H, Susin C (2005) Radiomorphometric indices and their relation to gender, age, and dental status. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99(4):479–484. https://doi.org/10.1016/j.tripleo.2004.09.013
Hienz SA, Paliwal S, Ivanovski S (2015) Mechanisms of bone resorption in periodontitis. J Immunol Res 2015:615486. https://doi.org/10.1155/2015/615486
Martínez-Maestre MÁ, González-Cejudo C, Machuca G, Torrejón R, Castelo-Branco C (2010) Periodontitis and osteoporosis: a systematic review. Climacteric 13(6):523–529. https://doi.org/10.3109/13697137.2010.500749
Demmer RT, Trinquart L, Zuk A, Fu BC, Blomkvist J, Michalowicz BS et al (2013) The influence of anti-infective periodontal treatment on C-reactive protein: a systematic review and meta-analysis of randomized controlled trials. PLoS One 8(10):e77441. https://doi.org/10.1371/journal.pone.0077441
Hajishengallis G, Chavakis T (2021) Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat Rev Immunol 21(7):426–440. https://doi.org/10.1038/s41577-020-00488-6
Souza PP, Lerner UH (2013) The role of cytokines in inflammatory bone loss. Immunol Investig 42(7):555–622. https://doi.org/10.3109/08820139.2013.822766
Hopstock LA, Grimsgaard S, Johansen H, Kanstad K, Wilsgaard T, Eggen AE (2022) The seventh survey of the Tromsø study (Tromsø7) 2015–2016: study design, data collection, attendance, and prevalence of risk factors and disease in a multipurpose population-based health survey. Scand J Public Health 50(7):919–929. https://doi.org/10.1177/14034948221092294
Holde GE, Oscarson N, Trovik TA, Tillberg A, Jönsson B (2017) Periodontitis prevalence and severity in adults: a cross-sectional study in norwegian circumpolar communities. J Periodontol 88(10):1012–1022. https://doi.org/10.1902/jop.2017.170164
Tonetti MS, Greenwell H, Kornman KS (2018) Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol 89:S159–SS72. https://doi.org/10.1002/JPER.18-0006
Trombelli L, Farina R, Silva CO, Tatakis DN (2018) Plaque-induced gingivitis: Case definition and diagnostic considerations. J Clin Periodontol 45:S44–S67. https://doi.org/10.1111/jcpe.12939
Schneider CA, Rasband WS, Eliceiri KW (2012) NIH Image to ImageJ: 25 years of image analysis. Nat Methods 9(7):671–675. https://doi.org/10.1038/nmeth.2089
Ledgerton D, Horner K, Devlin H, Worthington H Panoramic mandibular index as a radiomorphometric tool: an assessment of precision. Dento-Maxillo-Facial Radiol 26(2):95–100. Available from: [Internet]. 1997 [cited 2021 Nov 25]. https://doi.org/10.1038/sj.dmfr.4600215
Teterina A, Niratisairak S, Morseth B, Bolstad N (2023) Diagnostic efficacy of radiomorphometric indices for predicting osteoporosis in a Norwegian population in the Tromsø Study: Tromsø7. Oral Surg Oral Med Oral Pathol Oral Radiol 135(3):444–455. https://doi.org/10.1016/j.oooo.2022.10.039
Vlasiadis KZ, Damilakis J, Velegrakis GA, Skouteris CA, Fragouli I, Goumenou A et al (2008) Relationship between BMD, dental panoramic radiographic findings and biochemical markers of bone turnover in diagnosis of osteoporosis. Maturitas. 59(3):226–233. https://doi.org/10.1016/j.maturitas.2008.01.006
Leite AF, Figueiredo PT, Guia CM, Melo NS, de Paula AP (2010) Correlations between seven panoramic radiomorphometric indices and bone mineral density in postmenopausal women. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109(3):449–456. https://doi.org/10.1016/j.tripleo.2009.02.028
Marandi S, Bagherpour A, Imanimoghaddam M, Hatef M, Haghighi A (2010) Panoramic-based mandibular indices and bone mineral density of femoral neck and lumbar vertebrae in women. J of Dentist (Tehran, Iran) 7(2):98–106
Devlin H, Horner K (2002) Mandibular radiomorphometric indices in the diagnosis of reduced skeletal bone mineral density. Osteoporos Int 13(5):373–378. https://doi.org/10.1007/s001980200042
Taguchi A, Suei Y, Ohtsuka M, Otani K, Tanimoto K, Hollender LG (1999) Relationship between bone mineral density and tooth loss in elderly Japanese women. Dentomaxillofacial Radiol 28(4):219–223. https://doi.org/10.1038/sj/dmfr/4600445
Dagistan S, Bilge O (2010) Comparison of antegonial index, mental index, panoramic mandibular index and mandibular cortical index values in the panoramic radiographs of normal males and male patients with osteoporosis. Dentomaxillofacial Radiology 39(5):290–294. https://doi.org/10.1259/dmfr/46589325
Kavitha MS, Park SY, Heo MS, Chien SI (2016) Distributional variations in the quantitative cortical and trabecular bone radiographic measurements of mandible, between male and female populations of Korea, and its utilization. PLoS One 11(12):e0167992. https://doi.org/10.1371/journal.pone.0167992
Wang L, Cheng XG, Su YB, Brown K, Xu L, Li K et al (2017) Sex-related variations in cortical and trabecular bone of the femoral neck in an elderly Chinese population. Osteoporos Int 28(8):2391–2399. https://doi.org/10.1007/s00198-017-4043-y
Yates LB, Karasik D, Beck TJ, Cupples LA, Kiel DP (2007) Hip structural geometry in old and old-old age: similarities and differences between men and women. Bone 41(4):722–732. https://doi.org/10.1016/j.bone.2007.06.001
Gulsahi A, Yüzügüllü B, Imirzalioglu P, Genç Y (2008) Assessment of panoramic radiomorphometric indices in Turkish patients of different age groups, gender and dental status. Dentomaxillofacial Radiol 37(5):288–292. https://doi.org/10.1259/dmfr/19491030
Al-Dam A, Haydar Y, Rashad A (2020) Is there a change in the mandibular cortical shape index in panoramic radiographs over time? A longitudinal retrospective study. Dent Res J (Isfahan) 17(6):465–471
Lang T, LeBlanc A, Evans H, Lu Y, Genant H, Yu A (2004) Cortical and trabecular bone mineral loss from the spine and hip in long-duration spaceflight. J Bone Miner Res 19(6):1006–1012. https://doi.org/10.1359/jbmr.040307
Heinonen A, Oja P, Kannus P, Sievänen H, Haapasalo H, Mänttäri A et al (1995) Bone mineral density in female athletes representing sports with different loading characteristics of the skeleton. Bone 17(3):197–203. https://doi.org/10.1016/8756-3282(95)00151-3
Eastell R, O’Neill TW, Hofbauer LC, Langdahl B, Reid IR, Gold DT et al (2016) Postmenopausal osteoporosis. Nat Rev Dis Primers 2(1):1–16. https://doi.org/10.1038/nrdp.2016.69
Mudda JA, Bajaj M, Patil VA (2010) A Radiographic comparison of mandibular bone quality in pre- and post-menopausal women in Indian population. J Ind Soc Periodontol 14(2):121–125. https://doi.org/10.4103/0972-124x.70833
Kolte RA, Kolte AP, Potey AM (2017) Risk assessment of osteoporosis in pre- and postmenopausal periodontally healthy and chronic periodontitis women with digital panoramic radiographs. J Indian Soc Periodontol 21(6):461–465. https://doi.org/10.4103/jisp.jisp_238_17
Goyal L, Goyal T, Gupta ND (2017) Osteoporosis and periodontitis in postmenopausal women: a systematic review. J Mid-life Health 8(4):151–158. https://doi.org/10.4103/jmh.JMH_55_17
Choi JK, Kim YT, Kweon HI, Park EC, Choi SH, Lee JH (2017) Effect of periodontitis on the development of osteoporosis: results from a nationwide population-based cohort study (2003-2013). BMC Womens Health 17(1):77. https://doi.org/10.1186/s12905-017-0440-9
Mau LP, Kuan YC, Tsai YC, Lin JJ, Huynh-Ba G, Weng PW et al (2017) Patients with chronic periodontitis present increased risk for osteoporosis: a population-based cohort study in Taiwan. J Periodontal Res 52(5):922–929. https://doi.org/10.1111/jre.12464
Brincat SD, Borg M, Camilleri G, Calleja-Agius J (2014) The role of cytokines in postmenopausal osteoporosis. Minerva Ginecol 66(4):391–407
Wei S, Kitaura H, Zhou P, Ross FP, Teitelbaum SL (2005) IL-1 mediates TNF-induced osteoclastogenesis. J Clin Investig 115(2):282–290. https://doi.org/10.1172/jci23394
Ke L, Nogueira G, Thomson WM (2023) Influence of case definitions on epidemiological estimates of periodontitis prevalence and its associations with smoking and OHRQoL. Commun Dent Oral Epidemiol 51(2):194–200
Koizumi Y, Ishii T, Nishii Y, Nojima K, Sueishi K (2010) Influence of experimental hemi-occlusion on mandibular morphology and internal structure in growing rabbit. Orthodontic Waves 69(2):58–65
Guerreiro FS, Diniz P, Carvalho PEG, Ferreira EC, Avancini SRP, Ferreira-Santos RI (2013) Effects of masticatory hypofunction on mandibular morphology, mineral density and basal bone area. Brazil J Oral Sci 12:205–211
Masumoto T, Hayashi I, Kawamura A, Tanaka K, Kasai K (2001) Relationships among facial type, buccolingual molar inclination, and cortical bone thickness of the mandible. Eur J Orthodon 23(1):15–23
Gomes SGF, Custodio W, Jufer JSM, Cury AADB, Garcia RCMR (2010) Mastication, EMG activity and occlusal contact area in subjects with different facial types, CRANIO®. J Craniomandibul Sleep Pract 28(4):274–279. https://doi.org/10.1179/crn.2010.035
Gonca M, Gunacar DN, Kose TE, Beser B (2023) Evaluation of trabecular bone and mandibular cortical thickness in adults with different vertical facial types. Oral Surg Oral Med Oral Pathol Oral Radiol 135(2):282–293
World Medical Association (2013) World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. World Med Assoc JAMA 310(20):2191–2194. [cited 2021 Oct 13] 20.Available from:. https://doi.org/10.1001/jama.2013.281053
Acknowledgements
We are very grateful to Gro Eirin Holde, Ph.D., associate professor at the Department of Clinical Dentistry at UiT, The Arctic University of Norway, and The Public Dental Health Service Competence Centre of Northern Norway (TkNN), for classifying the data on periodontal disease and making them available. We are also grateful to Professor Hans-Peter Műller for his invaluable advice.
Funding
Open access funding provided by UiT The Arctic University of Norway (incl University Hospital of North Norway) The Arctic University of Norway (UiT), Northern Norway Regional Health Authority (Helse Nord RHF), the University Hospital of North Norway (UNN), and different research funds financed the Tromsø Study. The current study was entirely financed by the Department of Clinical Dentistry, the Faculty of Health Science (UiT).
Author information
Authors and Affiliations
Contributions
Conceptualization: Anna Teterina (A.T.), Napat Bolstad (N.B.), Bente Morseth (B.M.). Methodology: A.T., B.M., Sanyalak Niratisairak (S.N.). Validation: A.T., N.B.. Formal analysis: A.T.. Writing an original draft: A.T.. Review: editing and supervision: S.N., B.M., N.B.. Project administration and funding acquisition: N.B. All authors have read and agreed to publish the manuscript. Author contribution. Conceptualization: Anna Teterina (A.T.), Napat Bolstad (N.B.), Bente Morseth (B.M.). Methodology: A.T., B.M., Sanyalak Niratisairak (S.N.). Validation: A.T., N.B.. Formal analysis: A.T.. Writing an original draft: A.T.. Review, editing, and supervision: S.N., B.M., N.B.. Project administration and funding acquisition: N.B. All authors have read and agreed to publish the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Tromsø Study was conducted in accordance with the World Medical Association Declaration of Helsinki [60]. The Regional Committee on Research and Ethics North, REK North (reference 2014/940), and the Norwegian Data Protection Authority (reference 14/01463-4/CGN) approved Tromsø7. In addition, the current study was approved by REK North (reference number 68128) and Norwegian Centre for Research Data (NSD). All the participants gave written informed consent before the Tromsø7 data were collected. The data on each study participant were anonymized and de-identified. All individuals have the right to withdraw their personal data from the Tromsø7.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Teterina, A., Niratisairak, S., Morseth, B. et al. General and local predictors of mandibular cortical bone morphology in adult females and males: the seventh survey of the Tromsø Study. Clin Oral Invest 27, 6577–6587 (2023). https://doi.org/10.1007/s00784-023-05263-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-023-05263-0