
Abstract
Objectives
The aim of this study is to investigate vascular and neurosensory complications in edentulous patients following the installation of mandibular midline single implants in relation to lingual canals.
Materials and methods
After performing a cone beam computed tomography scan for the 50 recruited patients, the relationship between the potential implant site and the lingual canals was assessed, and all vascular and neurosensory complications were recorded.
Results
Six patients (12%) reported profuse bleeding during implant placement, and 13 (26%) reported transient neurosensory changes, which were resolved after 3 months. According to the virtual implant planning, 44 patients (88%) would have their implants touching the lingual canals, six of them reported vascular changes (14%), and 12 out of 44 patients reported neurosensory changes (27%). For the six patients who would have their implants not touching the lingual canals, one patient reported transient neurosensory changes.
Conclusions
The mandibular lingual canals are constant anatomic landmarks. Injury to the supra-spinosum lingual canals may occur during midline implant placement, depending on the implant length and the bone height.
Clinical relevance
Despite that injury to the supra-spinosum lingual canals during implant insertion does not result in permanent vascular or neurosensory complications, caution is required to avoid the perforation of the lingual cortices.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Two dental implants in the edentulous mandible have become a standard treatment option for retaining mandibular complete dentures [1]. Installing a single implant in the midline of an edentulous mandible to retain an overdenture was introduced to make the treatment more cost-effective and less invasive [2]. Promising medium- to long-term survival rates have been reported with this treatment option [2,3,4,5,6].
The interforaminal region has been the most commonly used area for implant installation. However, this region contains important anatomic structures, as well as important arterial anastomoses, including multiple accessories of the lingual canals (LCs) [7, 8]. Nevertheless, the presence of the LCs has not been clearly described in dental anatomy textbooks [9], despite it has been reported even in ancient mandibles [10]. The terminology for LCs has included median lingual canal, lingual vascular canal, and mandibular genial spinal canal [11]. Moreover, they have been classified by their location in the mandible into the median lingual foramen (MLF), which is located in the midline and the lateral lingual foramen (LLF), which is laterally positioned. The associated canals of each foramen are termed as the median lingual canal and the lateral lingual canal. The median vascular canal is named according to its relationship with the genial tubercles, that is, the superior spinosum or supra-spinosum, above the genial tubercles and the inferior spinosum or infra-spinosum below the genial tubercles [12].
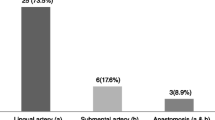
The supra-spinosum LC of the median lingual foramen has vascular and nerve supply that are branches of the lingual artery, sublingual artery, lingual vein, and lingual nerve [4, 9, 13, 14]. The infra-spinosum LC of the median lingual foramen has a branch of the submental or sublingual artery [13] and a branch of the mylohyoid nerve [14].
Severe hemorrhage accompanied by hematoma of the floor of the mouth has been reported during implant placement in the anterior region of the mandible [15,16,17,18] as a result of the rupture of the lingual periosteum and perforation of the lingual cortex [19]. To avoid such complications, the LCs of the mandible have been studied using cadaveric studies, panoramic radiographs, multi-slice computed tomography (MSCT), cone beam computed tomography (CBCT), and ultrasound/Doppler. Panoramic radiographs have been reported to show the LC only in 6.1% of the patients [19]. MSCT will eliminate anatomic superimposition and will give better visualization of the soft tissue, but the radiographic dose of MSCT is up to ten times higher than that of CBCT (MSCT: 430–1160 µSv and CBCT: 27–674 µSv) [20,21,22]. CBCT is more convenient to use and provides higher resolution on all three axes compared with the spiral CT because of the use of a 0.3-mm isotropic voxel or less [23, 24].
The submental and the lingual arteries are considered to be the two main sources of arterial blood supply to the anterior mandible. Occasionally, the arterial supply may be accompanied by nerves [25], which could lead to postoperative complications following implant installations, including anesthesia, paresthesia, or dysesthesia, depending on the degree of injury to the nerve [26]. Various methods have been used to detect such sensory disturbances, either subjectively by using questionnaires [27,28,29], objectively by performing physical tests [27], or by both [26]. The physical tests most often used to detect sensory changes in the anterior mandible are the two-point discrimination, the pain perception, and the temperature sensitivity tests [27].
Several studies reported major complications and life-threatening hemorrhages that occur during implant installation, but very few addressed the vascular and neurosensory changes that occur during implant installation in proximity to the LC at the midline of the mandible. Therefore, the main objective of this prospective clinical study was to investigate whether vascular complications and/or neurosensory impairment would occur following the installation of implants in the midline of edentulous mandibles in relation to the anatomy and proximity of the LCs.
Materials and methods
The ethical committee of the Faculty of Dentistry, Cairo University, Egypt approved the study on June, 2016 (Ethical Approval Number: 16/6/10). The current study was prepared in accordance with the SPIRIT statement for reporting clinical trials [30], and performed according to the Good Clinical Practice (GCP) and to the principles of the Declaration of Helsinki (2008). Moreover, the study was registered at the PAN AFRICAN CLINICAL TRIALS REGISTRY (Trial number: PACTR20183003085193).
Eighty completely edentulous participants, seeking to improve the retention of their mandibular complete dentures by installing a single implant in the midline of the mandible, were recruited by following strict inclusion/exclusion criteria (Table 1). All participants gave informed consent prior to inclusion in the study. The 50 participants included in the current study were the first included 50 patients to receive an implant, meaning they were the first enrolled in a larger randomized clinical trial, which finally included 80 participants. These 50 participants had to sign an additional informed consent form to approve the use of neurosensory tests after implant installation. Their medical history was recorded, and a simple test was performed to assess whether there was any neuro-sensory deficiency. A cotton roll was rubbed along the right and left sides of the patient’s mandibular ridge, and the participant was asked whether they felt any difference in sensation between the right and left sides, or whether they noticed any kind of sensory disturbance. Participants were included in the randomized clinical trial according to the healing protocol and later to the attachment system. Participant age ranged from 50 to 69 years (38 men and 12 women), with a mean age of 60.9 years for men and 58 years for women. The participants’ complete sufficient dentures were duplicated to fabricate transparent radiographic stents, with radio-opaque acrylic resin placed in the anterior central incisor area. The radiographic stent was checked inside the patient mouth to be stable.
All participants were then referred to the Oral and Maxillofacial Radiology Department for CBCT examination while wearing their radiographic stent (ProMax 3D Mid, Planmeca, Helsinki, Finland) using the standard patient positioning protocol. All participants were scanned using a tube potential of 90 kVp, a tube current of 10 mA, a cylindrical field of view of 20 × 6 cm, and a voxel size of 400 µm. The acquired images were processed and measured (Planmeca Romexis Viewer 3.5.1 software, Planmeca). All observations and measurements were carried out independently by two oral and maxillofacial radiologists experienced in CBCT scan interpretation in separate sessions.
In order to detect the LCs, the midline was defined on the axial image by a line running between the pogonion and the apex of the mental spine of each mandible [18]. Thereafter, it was adjusted from the convexity of the genial tubercle (mental spine) and mental ridge on the axial cut using a slice thickness and slice gap of 0.4 mm each (Fig. 1), so that five consecutive sagittal cuts were assessed on each side of the midline to investigate the following aspects:
-
1.
The LCs were classified according to their relation to the mental spine and were divided into supra-spinosum and infra-spinosum depending upon the level of opening of the canal above or below the genial spines. Supra-spinosum canals include the foramina at the level of the genial spines (Fig. 2) [33]. The morphological variations of the lingual canals in the current study were classified according to Ali and Ahmad [34]
-
2.
The distance between the upper borders of both the buccal and the lingual terminal ends of each canal and the alveolar crest (Fig. 3a, b)
-
3.
The length of each canal (Fig. 4)
-
4.
The diameter of both the lingual and the buccal terminal ends of each canal (Fig. 5a, b)

Detection of the midline from the convexity of the genial tubercle (mental spine) and mental ridge on an axial cut (slice thickness 0.4 mm and slice gap 0.4 mm)

The presence, distribution, and number of canals

a Distance between the upper border. b Distance between the upper border of the lingual terminal end of the canal of the buccal terminal end of the canal and the alveolar crest and the alveolar crest

Measurement of the canal length

a The diameter of the buccal terminal end. b The diameter of the lingual terminal end
The assessment of the appearance and the morphological variations of the LCs were agreed upon by the two investigators, while an average of the two readings of both investigators was reported for the linear measurements.
For virtual implant planning, the same Blue Sky Bio software was used. All implants were virtually placed, guided by the radio-opaque acrylic resin positioned in the midline of the mandible (Fig. 6a, b). The relationship between the potential implant site and the LC was assessed. According to the proximity between the potential implant site and the canals, the authors proposed the following classification:
-
1.
Touching (≤ 2 mm) (Fig. 6a), with possible injury of the LC
-
2.
Not touching (> 2 mm) (Fig. 6b), with no possible injury of the LC

a Implant touching the canal. b Implant not touching the canal
All patients were instructed to take 2000 mg of Amoxicillin as a single dose 2 h before surgery [35]. Local infiltration anesthesia was given at the mandibular anterior area, and a crestal incision (20 mm) was then made at the area of the implant installation, guided by the radiographic stent, which was converted into a surgical stent. A special attention was paid to preserve an adequate width of keratinized attached mucosa around the installed implants, particularly for non-submerged implants, which would help to have better soft and hard tissue stability, less plaque accumulation, limited soft tissue recession, and lower incidence of peri-implant mucositis and periimplantitis [36, 37].
All implants were 3.7 mm in diameter and 10 mm in length (Tapered screw vent, Zimmer Dental GmbH, Warsaw, Indiana, USA). The implant stability quotient (ISQ) was measured for all implants (Osstell, Integration Diagnostics Ltd., Sävedalen, Sweden) using the Osstell corresponding abutment (Type 32 used for Zimmer implant, Osstell), which should give a reading of at least 60 ISQ in all four directions (right, left, lingual, buccal) to be able to randomize the participant for the two healing protocols (submerged and non-submerged). In the case of lower ISQ values, the participant was excluded from the study. During implant installation, care was taken not to perforate the bone cortex and any vascular disturbance was recorded. A score (0) was given as (absent) to the absence of arterial injury (normal bleeding). While if profuse pulsating bleeding was detected and stopped (applying gauze pressure for 5 min), a score (1) was given as (present).
On the day of implant installation, the participant’s mandibular denture was relieved to avoid pressure on the underlying tissues and relined with a resilient denture liner (COE-SOFT, GC AMERICA INC, IL, USA). After 10 to 14 days from implant installation, all participants were recalled for suture removal provided that the incision site had healed properly with no signs of pain or swelling. Any vascular or sensory complications were recorded. On the day of suture removal, the following physical tests were carried out and recorded in the participant’s neurosensory chart:
-
1.
Pin pressure: An explorer was used to exert pin pressure intra-orally at the area of implant installation and extra-orally around the lips and chin to detect the presence of sensation.
-
2.
Static touch detection test: With the participant’s eyes closed, a cotton tip applicator was used to determine sensation in the area of the implant installation inside the mouth and extra-orally around the lips and chin.
-
3.
Direction of movement test: With the participant’s eyes closed, a soft brush was used to determine the ability to detect both sensation and direction of movement. The soft brush was moved over the buccal and lingual mucosa at the area of implant installation and extra-orally over the lips and chin.
-
4.
Two-point discrimination test: With the participant’s eyes closed, calipers were used to determine the ability to discriminate the varying distance between the two points of the calipers, which were about 6 mm apart. The calipers were placed over the chin, and the participant was asked whether it was felt as one point or two points.
The results of these tests were recorded, so that a score of (0) was given if there was no change detected in all the sensory tests (absent). If any change was detected, a score of (1) was given, denoting the presence of neurosensory changes.
All participants were then recalled 3 months after implant installation for the pickup stage (prosthetic loading), and the neurosensory changes were reassessed.
The detected vascular and neurosensory complications for all participants were then separately correlated with all of the following variables: gender, age, number of lingual canals, anatomic lingual foramen morphology, distance between the upper border of the buccal terminal and alveolar crest (mm), distance between the upper border of the lingual terminal and alveolar crest (mm), canal length (mm), diameter of the lingual terminal (mm), diameter of the buccal terminal (mm), as well as proximity of the virtually planned implant to the LCs in order to evaluate whether any of the variables correlated with the vascular and neurosensory changes encountered.
Data management and statistical analysis were performed using the Statistical Package for Social Sciences (IBM SPSS for Windows, Version 21.0, IBM SPSS, Inc., Chicago, IL, USA). Data were explored for normality using the Kolmogorov–Smirnov test and Shapiro–Wilk test. A two-way analysis of variance with repeated measure was used accordingly. Categorical data were summarized as percentages; differences were analyzed with χ2 (chi square) tests and the Fisher exact test when appropriate. Adjustments of p value were done using the Bonferroni method for multiple testing. To compare vascular and neurosensory complications, the Mann–Whitney was used.
Results
No drop-out and no implant failure were reported within the healing period of three months of the 50 participants of the current study.
Intra-class correlation of the measurements
The distance between the upper border of the buccal terminal and alveolar crest (mm), the distance between the upper border of the lingual terminal and alveolar crest (mm), the canal length (mm), the diameter of the lingual terminal (mm), and the diameter of the buccal terminal (mm) were determined by the two radiologists. They revealed a strong agreement (greater than 0.7) as shown in Table 2. Regarding a possible nerve injury, the two radiologists discussed whether the planned implant would touch or would not touch the canal to reach a consensus.
Anatomic morphology of LCs
The anatomic morphology of the LCs was classified [34]. The canal morphology was of type A for 7 participants, type B for 3 participants, type D for 7 participants, type E for 8 participants, and of other type for 15 participants (Fig. 7a–e). The lingual canal classification was used in order to view the number of supra-spinosum and infra-spinosum canals with their buccal and lingual terminals.

a–e Variety of canal morphology recorded in the present study. a Type A = one supra-spinosum canal in which the lingual terminal is higher than the buccal terminal. b Type B = One supra-spinosum canal in which the lingual terminal is higher than the buccal terminal and one infra-spinosum canal. c Type D = One supra-spinosum canal in which the lingual terminal is higher than the buccal terminal and one infra-spinosum canal that runs horizontally. Both are connected to each other. d Type E = One supra-spinosum canal in which the lingual terminal is higher than the buccal terminal and one infra-spinosum canal in which the lingual terminal is at a lower level than the buccal terminal. Both are connected to each other. e Other = that does not suit all of the above type
Number and measurements of the LCs
All participants showed at least one canal. A supra-spinosum canal was found in 49 participants, eight of them showed two supra-spinosum canals. The mean value of the supra-spinosum canals number was (1.1 ± 0.4). An infra-spinosum canal was found in 38 participants, ten of them showed two infra-spinosum canals (Table 3). The mean value of infra-spinosum canals number was (1 ± 0.7).
Linear measurements of the LCs
All the linear measurements of the lingual canals are summarized in Table 4.
Correlation of different variables with vascular complications
Only 6 participants (4 men and 2 women) experienced vascular complications during implant installation, one of them experienced sensory complications. When correlating the effect of age and gender with the vascular complications, no statistically significant effect was found (Table 5). When analyzing the morphology and the anatomy of the LCs, neither the number of canals nor the distance to the anatomic outlines had a statistically significant effect on the vascular complications reported in the present clinical study (p > 0.05) (Table 6). The data of both the vascular complications and sensory changes, which are presented as median and range, were not normally distributed. Thus, all p values were two-sided, so that a p ≤ 0.05 was considered statistically significant.
When correlating the proximity of the virtually placed implant to the LCs, 44 participants had their implants within 2 mm to the canal (with possible injury), and 6 participants had their implants away from the canal (with no possible injury). Even so, only 6 participants showed vascular complications in the group who had their planned implants in close proximity to the canal. In the group who had their planned implant away from the canal, no vascular complications were reported. Being in close proximity to the LC (possible injury of the canal) showed no statistically significant correlation with the reported vascular complications (p > 0.05) (Table 6).
Correlation of the different variables to neurosensory changes
Overall, 13 participants (26%; 6 women and 7 men) out of all 50 participants reported transient neurosensory changes following implant placement, all of which disappeared within 3 months. Only one participant experienced both vascular complications and sensory changes. Age did not show significant effect on the neurosensory complications. However, concerning the gender of the participants, the neurosensory complications were statistically significantly higher in females (50%) than in males (18.6%) (p = 0.03) (Table 7).
Likewise, the number of canals, the proximity to the anatomic outlines, the canal length, the diameter of the lingual terminal, and the diameter of the buccal terminal showed no statistically significant effect on the reported neurosensory changes (Table 6).
Forty-four participants had their virtually placed implants touching the lingual canal, 12 of whom experienced neurosensory changes and 32 of whom did not. Of the 6 participants who had their implants virtually away from the canal (not touching), only one experienced neurosensory change. The virtual proximity of the planned implants to the lingual canal showed no statistically significant correlation with the neurosensory changes (p > 0.05) (Table 8).
Discussion
Implant installation in the midline of the mandible may be very challenging due to the presence of lingual canals and their associated blood vessels and nerve innervation [9, 11]. Several studies reported complications such as life-threatening hemorrhages and other neurosensory complications [15,16,17, 26]. Therefore, the main aim of this clinical trial was to try to understand the correlation between the reported vascular and neurosensory complications and the proximity to the lingual canals and their anatomy, which of high clinical relevance to guide clinicians during implant planning and placement.
In order to report the vascular complications and neurosensory changes related to implant installation in proximity to the LCs of the midline of a completely edentulous mandible, different factors were considered, including age, gender, location/anatomy of the LCs, and proximity of the virtually planned implants to the canals.
The LCs were detected using CBCT scans as they have been reported to be 4–20 times more accurate than panoramic radiographs [21, 38]. One study concluded that CBCT is more accurate in detecting the various maxillary and mandibular anatomic structures than panoramic x-rays [36]. Moreover, to overcome variation in the quality of the image due to slice thickness, two oral and maxillofacial radiologists independently detected and measured all of the LCs following a defined protocol to give more consistent evaluation [39]. Moreover, standardized settings were used for all CBCT scans.
During the osteotomy and implant installation, only 6 of 50 participants (12%) exhibited profuse bleeding, which was easily arrested by applying gauze pressure for 5 min; no hemorrhagic complications were reported postoperatively. Overall, 13 (26%) of the participants experienced transient neurosensory changes after implant installation, which disappeared within 3 months. Both the vascular and neurosensory complications showed a non-statistically significant correlation with the considered factors (patient and LC related).
According to the results of this study and given that 88% of the installed implants were probably touching the lingual canal (based on the virtual planning), no serious vascular or permanent neurosensory complications were encountered. One explanation is that all installed implants were 10 mm in length, which is considered an optimum implant length in the anterior inter-foraminal region [7]. The life-threatening hemorrhages reported in the literature mostly occurred with an implant length and osteotomy preparation of greater than 15 mm [7]. Moreover, most of them occurred because the lingual cortical plate was perforated [40], resulting in hematoma and swelling in the floor of the mouth and leading in turn to obstruction of the upper airway space [12, 22, 24, 41,42,43]. An interesting review of literature concluded that during implant installation in the mandible, a proper planning is mandatory to avoid perforation of the lingual cortex otherwise severe bleeding could occur, which would require specialized care [44]. Furthermore, one study reported after macro-anatomic dissection of 20 mandibles, the close proximity of blood vessels to the lingual cortical plate of the midline of the mandibular, which would increase the risk of bleeding even with minimal perforation of the mandibular lingual plate [9]. Therefore, during implant installation in the mandible, proper planning is mandatory to avoid the perforation of the lingual cortex and its associated severe bleeding. No hemorrhages were reported in the current study, which is in agreement with other studies that reported hemorrhages following implant installation in a completely edentulous mandible but in other regions, i.e., two patients hemorrhaged in the first premolar region, seven in the canine region, and only one in the region of the lateral incisor, indicating the least number of hemorrhages in the lateral incisor area [43,44,45,46,47,48,49,50]. Another explanation could be that in elderly and edentulous patients, the central blood supply could be compromised [51, 52].
The neurosensory change was described as temporary, according to the classification of Seddon and Sunderland and may be classified as “Neurapraxia” and defined as temporary when the interruption of nerve transmission is caused by nerve compression, edema, hematoma, and minor stretching. Furthermore, the recovery rate is fast, ranging from days to 12 weeks [53, 54]. However, keeping a safe distance of 2 mm between implants and the neurovascular bundle of the lingual foramen is still recommended to avoid these transient vascular/neurosensory complications [55].
In edentulous patients, the need to reduce the vertical bone height because of limited crestal bone thickness might result in close proximity to the LCs during implant installation. The average distance calculated in the present study of the supra-spinosum median LC to the crest of the ridge was 9.6 ± 3.8 mm, which means that the supra-spinosum LC should always be taken into consideration during midline implant planning and placement. The average distance of the infra-spinosum median lingual canal to the crest of the ridge was 19.9 ± 4.8 mm, which appears to be a safe distance, and is in agreement with other studies [12, 24, 42, 56,57,58,59] that have reported an average safe distance of 15.5 mm from the median lingual foramen to the crest.
The diameter of the median lingual foramen can also put the patient at higher risk of hemorrhage if it is greater than 1 mm, but only if the lingual cortex is perforated [9]. The average diameter of the supra-spinosum median lingual canal and that of the infra-spinosum median lingual canal in the present study was 0.6 ± 0.2 mm and 0.5 ± 0.2, respectively, which is considered to be within the safe range. A systematic review concluded that the diameter of the LC is an important anatomic variation to be considered during implant installation in the midline of the mandible [60]. A similar study using CBCT scans was carried out on edentulous cadaveric mandibles to detect possible contact between virtually placed single midline implants and the lingual canals and concluded that the risk of midline implants contacting the lingual canal is high [61]. Likewise, another macro- and microanatomical study concluded after the dissection of 12 intact cadaver mandibles that the superior and inferior genial spinal foramina have different neurovascular contents, determined by their anatomical location above or below the genial spines [13].
They recommended to carry out further clinical studies to report the possible complications of midline implant installation and their clinical relevance. A clinical trial using CBCT scans investigated the importance of detecting the presence, position, and size of the lingual foramina before implant installation in dentate patients and reported that the lingual foramina were present below and above the tooth apex, that those above the tooth apex were of smaller diameter, and that the distance between them and the tooth apex changed with increasing age [58].
Moreover, a recent anatomical study curried on dentate and edentulous cadaveric mandibles investigated the genial spinal canal histologically concluded that the genial spinal canal in the dentate specimen contained a neurovascular bundle, which branched into a nerve innervating the incisor and a neurovascular bundle, whereas that in the edentulous specimen contained some nerves for vestibular gingival innervation and a vascular bundle [62]. The results propose differences in the genial spinal canal between dentate and edentulous mandibles and may explain the low incidence of both vascular or neurosensory complications in the current study. Hence, our clinical study was carried out to report the complications of midline implant installation in the completely edentulous mandible in relation to lingual canals, which is of greater clinical relevance than the detection itself.
A limitation of the current study was the lack of a postoperative CBCT scans to evaluate the actual proximity and possible injury of placed implants to the LCs and their relationship to the reported vascular and neurosensory complications. A second CBCT scan was not possible as it was not clinically justified and therefore not approved by the ethics committee. Only a standardized peri-apical radiograph was approved to evaluate the bone height changes.
Conclusions
From the present study, it can be concluded that the mandibular lingual canals are constant anatomic landmarks that are present at the midline of the mandible, as all participants showed at least one canal and 98% of them had a supra-spinosum canal (49 of 50 participants). There is considerable potential for injury to the supra-spinosum lingual canals during midline implant placement, depending on the implant length and the available bone height. Injuries of the supra-spinosum lingual canals during implant insertion in the midline of the mandible without perforation of bone cortices did not result in permanent vascular or neurosensory complications.
References
Feine JS, Carlsson GE, Awad MA et al (2002) The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology 19:3–4
Cordioli G, Majzoub Z, Castagna S (1997) Mandibular overdentures anchored to single implants: a five-year prospective study. J Prosthet Dent 78:159–165. https://doi.org/10.1016/s0022-3913(97)70120-3
Passia N, Kern M (2014) The single midline implant in the edentulous mandible: a systematic review. Clin Oral Investig 18:1719–1724. https://doi.org/10.1007/s00784-014-1248-8
Passia N, Wolfart S, Kern M (2019) Ten-year clinical outcome of single implant retained mandibular overdentures a prospective pilot study. J Dent 82:63–65. https://doi.org/10.1016/j.dent.2019.01.006
Bryant SR, Walton JN, MacEntee MI (2015) A 5-y randomized trial to compare 1 or 2 implants for implant overdentures. J Dent Res 94:36–43. https://doi.org/10.1177/0022034514554224
Kern M, Behrendt C, Fritzer E, Kohal RJ et al (2021) 5-year randomized multicenter clinical trial on single dental implants placed in the midline of the edentulous mandible. Clin Oral Implants. https://doi.org/10.1111/clr.13692
Kalpidis CDR, Setayesh RM (2004) Hemorrhaging associated with endosseous implant placement in the anterior mandible: A review of the literature. J Periodontol 75:631–645. https://doi.org/10.1902/jop.2004.75.5.631
Ramanauskaite A, Becker J, Sader R (2000) Schwarz F (2019) Anatomic factors as contributing risk factors in implant therapy. Periodontol 81:64–75. https://doi.org/10.1111/prd.12284
Rosano G, Taschieri S, Gaudy JF, Testori T, Del Fabbro M (2009) Anatomic assessment of the anterior mandible and relative hemorrhage risk in implant dentistry: A cadaveric study. Clin Oral Implants Res 20:791–795. https://doi.org/10.1111/j.1600-0501.2009.01713.x
Demiralp KO, Bayrak S, Orhan M, Alan A, KursunCakmak ES, Orhan K (2018) Anatomical characteristics of the lingual foramen in ancient skulls: a cone beam computed tomography study in an Anatolian population. Folia Morphol 77:514–520. https://doi.org/10.5603/FM.a2018.0009
Tagaya A, Matsuda Y, Nakajima K, Seki K, Okano T (2009) Assessment of the blood supply to the lingual surface of the mandible for reduction of bleeding during implant surgery. Clin Oral Implants Res 20:351–355. https://doi.org/10.1111/j.1600-0501.2008.01668.x
Scaravilli MS, Mariniello M, Sammartino G (2010) Mandibular lingual vascular canals (MLVC): Evaluation on dental CTs of a case series. Eur J Radiol 76:173–176. https://doi.org/10.1016/j.ejrad.2009.06.002
Liang X, Jacobs R, Lambrichts I, Vandewalle G (2007) Lingual foramina on the mandibular midline revisited: A macroanatomical study. Clin Anat 20:246–251. https://doi.org/10.1002/ca.20357
Liang X, Jacobs R, Corpas LS, Semal P, Lambrichts I (2009) Chronologic and geographic variability of neurovascular structures in the human mandible. Forensic Sci Int 190:24–32. https://doi.org/10.1016/j.forsciint.2009.05.006
Flanagan D (2003) Important arterial supply of the mandible, control of an arterial hemorrhage, and report of a hemorrhagic incident. J Oral Implantol 29:165–173. https://doi.org/10.1563/1548-1336(2003)029<0165:IASOTM>2.3.CO;2
Fujita S, Ide Y, Abe S (2012) Variations of vascular distribution in the mandibular anterior lingual region: a high risk of vascular injury during implant surgery. Implant Dent 21:259–264. https://doi.org/10.1097/ID.0b013e31825cbb7dF
Jo JI-HO, Kim SU-G, Oh JI-SU (2011) Hemorrhage related to implant placement in the anterior mandible. Implant Dent 20:33–37. https://doi.org/10.1097/ID.0b013e3182181c6b
Kawai T, Asaumi R, Sato I, Yoshida S, Yosue T (2007) Classification of the lingual foramina and their bony canals in the median region of the mandible: cone beam computed tomography observations of dry Japanese mandibles. Oral Radiol 23:42–48. https://doi.org/10.1007/s11282-007-0064-0
Jalili MR, Esmaeelinejad M, Bayat M, Aghdasi MM (2012) Appearance of anatomical structures of mandible on panoramic radiographs in Iranian population. Acta Odontol Scand 70:384–389. https://doi.org/10.3109/00016357.2011.629625
Li G (2013) Patient radiation dose and protection from cone-beam computed tomography. Imaging Sci Dent 43:63. https://doi.org/10.5624/isd.2013.43.2.63
Ludlow JB, Ivanovic M (2008) Comparative dosimetry of dental CBCT devices and 64-slice CT for oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol. Oral Radiol 106:106–114. https://doi.org/10.1016/j.tripleo.2008.03.018
Kim DH, Kim MY, Kim C-H (2013) Distribution of the lingual foramina in mandibular cortical bone in Koreans. JKAOMS 39:263–268. https://doi.org/10.5125/jkaoms.2013.39.6.263
von Arx T, Matter D, Buser D, Bornstein MM (2011) Evaluation of location and dimensions of lingual foramina using limited cone beam computed tomography. J Oral Maxillofac Surg 69:2777–2785. https://doi.org/10.1016/j.joms.2011.06.198
Sheikhi M, Mosavat F, Ahmadi A (2012) Assessing the anatomical variations of lingual foramen and its bony canals with CBCT taken from 102 patients in Isfahan. Dent Res J 9:45–51
Vasconcellos HA, de Siqueira Campos AE, de Almeida GH, de Tan Maia ML, Barros de Vasconcellos PH (2000) The anatomy of the lingual foramen canal and it’s related to the mandibular symphysis. Rev chil Anat 18:47–51. https://doi.org/10.4067/S0716-98682000000100006
Walton JN (2000) Altered sensation associated with implants in the anterior mandible: a prospective study. J Prosthet Dent 83:443–449. https://doi.org/10.1186/s40902-018-0170-4
Bartling R, Freeman K, Kraut RA (1999) The incidence of altered sensation of the mental nerve after mandibular implant placement. J Oral Maxillofac Surg 57:1408–1412. https://doi.org/10.1016/s0278-2391(99)90720-6
Ellies LG (1992) Altered sensation following mandibular implant surgery: a retrospective study. J Prosthet Dent 68:664–671. https://doi.org/10.1016/0022-3913(92)90384-m
Wismeijer D, van Waas MA, Vermeeren JI, Kalk W (1997) Patients’ perception of sensory disturbances of the mental nerve before and after implant surgery: a prospective study of 110 patients. Br J Oral Maxillofac Surg 35:254–259. https://doi.org/10.1016/s0266-4356(97)90043-7
Chan AW, Tetzlaff JM, Altman DG et al (2013) SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med 158:200–207. https://doi.org/10.7326/0003-4819-158-3-201302050-00583
Naujokat H, Kunzendorf B, Wiltfang J (2016) Dental implants and diabetes mellitus-a systematic review. Int J Implant Dent 2:5. https://doi.org/10.1186/s40729-016-0038-2
McGarry TJ, Nimmo A, Skiba JF, Ahlstrom RH, Smith CR, Koumjian JH (1999) Classification system for complete edentulism. J Prosthodont 8:27–39. https://doi.org/10.1111/j.1532-849X.2004.04019.x
Liang X, Jacobs R, Lambrichts I (2006) An assessment on spiral CT scan of the superior and inferior genial spinal foramina and canals. Surg Radiol Anat 28:98–104. https://doi.org/10.1007/s00276-005-0055-y
Ali A, Ahmad M (2008) Anatomical variations of the lingual mandibular canals and foramina. Northwest Dent 87:36–37
Lund B, Hultin M, Tranaeus S, Naimi-Akbar A, Klinge B (2015) Complex systematic review—perioperative antibiotics in conjunction with dental implant placement. Clin Oral Implants Res 26:1–14
Chackartchi T, Romanos GE (2000) Sculean A (2019) Soft tissue-related complications and management around dental implants. Periodontol 81:124–138. https://doi.org/10.1111/prd.12287
Fu JH, Wang HL (2020) Breaking the wave of peri-implantitis. Periodontol 2000 84:145–160. https://doi.org/10.1111/prd.12335
Zhang C, Zhuang L, Fan L, Mo J, Huang Z, Gu Y (2018) Evaluation of mandibular lingual foramina with cone-beam computed tomography. J Craniofac Surg 29:e389–e394. https://doi.org/10.1097/SCS.0000000000004390
Jaju P, Jaju S (2011) Lingual vascular canal assessment by dental computed tomography: A retrospective study. Indian J Dent Res 22:232–236. https://doi.org/10.4103/0970-9290.84293
Mraiwa N, Jacobs R, van Steenberghe D, Quirynen M (2003) Clinical assessment and surgical implications of anatomic challenges in the anterior mandible. Clin Implant Dent Relat Res 5:219–225. https://doi.org/10.1111/j.1708-8208.2003.tb00204.x
Wang YM, Ju YR, Pan WL, Chan CP (2015) Evaluation of location and dimensions of mandibular lingual canals: a cone beam computed tomography study. Int J Oral Maxillofac Surg 44:1197–1203. https://doi.org/10.1016/j.ijom.2015.03.014
Yildirim YD, Güncü GN, Galindo-Moreno P, Velasco-Torres M, Juodzbalys G, Kubilius M, Tözüm TF (2014) Evaluation of mandibular lingual foramina related to dental implant treatment with computerized tomography: a multicenter clinical study. Implant Dent 23:57–63. https://doi.org/10.1097/ID.0000000000000012
Boyes-Varley JG, Lownie JF (2002) Haematoma of the floor of the mouth following implant placement. SADJ 57:64–65
Tomljenovic B, Herrmann S, Filippi A, Kühl S (2016) Life-threatening hemorrhage associated with dental implant surgery: a review of the literature. Clin Oral Implants Res 27:1079–1084. https://doi.org/10.1111/clr.12685
Krenkel C, Holzner K (1986) Lingual bone perforation as causal factor in a threatening hemorrhage of the mouth floor due to a single tooth implant in the canine region. Quintessenz 37:1003–1008
Laboda G (1990) Life-threatening hemorrhage after placement of an endosseous implant: report of case. J Am Dent Assoc 121:599–600
Mason ME, Triplett RG, Alfonso WF (1990) Life-threatening hemorrhage from placement of a dental implant. J Oral Maxillofac Surg 48:201–204. https://doi.org/10.1016/S0278-2391(10)80211-3
Mordenfeld A, Andersson L, Bergström B (1997) Hemorrhage in the floor of the mouth during implant placement in the edentulous mandible: a case report. Int J Oral Maxillofac Implants 12:558–561
Niamtu J (2001) Near-fatal airway obstruction after routine implant placement. Oral Surg. Oral Med Oral Pathol Oral Radiol 92:597–600. https://doi.org/10.1067/moe.2001.116503
Ten Bruggenkate CM, Krekeler G, Kraaijenhagen HA, Foitzik C, Oosterbeek HS (1993) Hemorrhage of the floor of the mouth resulting from lingual perforation during implant placement: a clinical report. Int J Oral Maxillofac Implants 8:329–334
Molly L (2006) Bone density and primary stability in implant therapy. Clin Oral Implants Res 17:124–135. https://doi.org/10.1111/j.1600-0501.2006.01356.x
Tolstunov L (2007) Implant zones of the jaws: Implant location and related success rate. J Oral Implantol 33:211–220. https://doi.org/10.1563/1548-1336(2007)33[211:IZOTJI]2.0.CO;2
Seddon HJ (1943) Three types of nerve injury. Brain 66:237–288. https://doi.org/10.1093/brain/66.4.237
Sunderland S (1951) A classification of peripheral nerve injuries producing loss of function. Brain 74:491–516. https://doi.org/10.1093/brain/74.4.491
Sener E, Onem E, Akar GC, Govsa F, Ozer MA, Pinar Y, Baksi Sen BG (2018) Anatomical landmarks of mandibular interforaminal region related to dental implant placement with 3D CBCT: Comparison between edentulous and dental mandibles. Surg Radiol Anat 40:615–623. https://doi.org/10.1007/s00276-017-1934-8
Babiuc I, Tărlungeanu I, Păuna M (2011) Cone beam computed tomography observations of the lingual foramina and their bony canals in the median region of the mandible. Rom J Morphol Embryol 52:827–829
Choi DY, Woo YJ, Won SY, Kim DH, Kim HJ, Hu KS (2013) Topography of the lingual foramen using micro-computed tomography for improving safety during implant placement of anterior mandibular region. J Craniofac Surg 24:1403–1407. https://doi.org/10.1097/SCS.0b013e31828b75da
He X, Jiang J, Cai W, Pan Y, Yang Y, Zhu K, Zheng Y (2016) Assessment of the appearance, location and morphology of mandibular lingual foramina using cone beam computed tomography. Int Dent J 66:272–279. https://doi.org/10.1111/idj.12242
Oettlé AC, Fourie J, Human-Baron R, van Zyl AW (2015) The midline mandibular lingual canal: Importance in implant surgery. Clin Implant Dent Relat Res 17:93–101. https://doi.org/10.1111/cid.12080
Bernardi S, Bianchi S, Continenza MA, Macchiarelli G (2017) Frequency and anatomical features of the mandibular lingual foramina: systematic review and meta-analysis. Surg Radiol Anat 39:1349–1357. https://doi.org/10.1007/s00276-017-1888-x
Birkenfeld F, Becker M, Sasse M, Gassling V, Lucius R, Wiltfang J, Kern M (2015) Detection of the genial spinal canal in atrophic mandibles with a CBCT: A cadaver study. Dentomaxillofac Radiol 44:20140290. https://doi.org/10.1259/dmfr.20140290
Passia M, Oberbillig F, Goulioumis V, Naumova EA, Kern M, Arnold W (2020) Three-dimensional reconstruction of the genial spinal canal. Clin Anat 33:1102–1108. https://doi.org/10.1002/ca.23512
Acknowledgements
We would like to thank the participants for their compliance with the study recalls, and Enid Rosenstiel for her English language editing assistance.
Funding
Open Access funding enabled and organized by Projekt DEAL. This clinical study is a part of GESEED program, which is a research collaboration between the Department of Prosthodontics, Propaedeutics and Dental Materials, Christian-Albrechts University at Kiel in Germany and the Faculty of Dentistry, Cairo University in Egypt, and was partially funded by the German Academic Exchange Service (Deutscher Akademischer Austauschdienst, DAAD, Germany) and the Science and Technology Development Fund (STDF, Egypt).
Author information
Authors and Affiliations
Contributions
MSC and MK contributed to the study conception and design. Data acquisition and collection were performed by AMA and DFA. MSC, AAN, and NA drafted and revised the manuscript. Recruitment of the participants was staged by NA. All authors read, revised, and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval
The ethical committee of the Faculty of Dentistry, Cairo University, Egypt approved the study on June, 2016 (Ethical Approval Number: 16/6/10). The current study was prepared in accordance with the SPIRIT statement for reporting clinical trials [29], and performed according to the Good Clinical Practice (GCP) and to the principles of the Declaration of Helsinki (2008). Moreover, the study was registered at the PAN AFRICAN CLINICAL TRIALS REGISTRY (Trial number: PACTR20183003085193).
Informed consent
All individual participants gave informed consent prior to inclusion in the current study.
Conflict of interest
The authors declare no conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chaar, M.S., Naguib, A.A., Abd Alsamad, A.M. et al. Vascular and neurosensory evaluation in relation to lingual canal anatomy after mandibular midline implant installation in edentulous patients. Clin Oral Invest 26, 3311–3323 (2022). https://doi.org/10.1007/s00784-021-04312-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-021-04312-w