
Abstract
Objectives
Assess calcium silicate cement (Biodentine™) vs. glass ionomer cement (Fuji IX™, control) as indirect pulp capping (IPC) materials in patients with reversible pulpitis after a 2-year follow-up. Evaluate the integrity of the overlying resin composite restorations using modified USPHS criteria and FDI criteria. Investigate the sensitivity of the modified USPHS criteria compared to the FDI criteria in the assessment of the restorations.
Materials and methods
Seventy-two restorations (36 Biodentine™, 36 Fuji IX™) were placed randomly in 53 patients. Periapical radiographs were taken at pre-treatment (T0), 12-month (T12), and 24-month (T24) review. Restorations were assessed using the modified USPHS and FDI criteria at T12 and T24.
Results
At 24 months, 15 teeth had failed to maintain vitality (6 Biodentine™, 9 Fuji IX™). Clinical success rate of IPC for both materials was 72% and is related to the intensity of reversible pulpitis symptoms. No difference was found between T12 and T24 in the periapical (PA) radiographs and in the integrity of the resin composite restorations overlying Biodentine™ compared to Fuji IX™. There was no difference in the efficacy of the USPHS criteria compared to the FDI criteria in the assessment of the resin composite restorations.
Conclusions
Biodentine™ and Fuji IX™ were clinically effective when used as IPC materials in teeth with reversible pulpitis at T24. Resin composite restorations overlying both materials performed well at T24. Using the USPHS or FDI criteria is equally efficient at T24; however, longer term follow-up is needed to establish whether there are sensitivity differences between these assessment criteria.
Clinical significance
Teeth with deep carious lesions approaching the pulp and with signs of reversible pulpitis can be treated successfully by indirect pulp capping using either Biodentine™ or Fuji IX™. Using the USPHS or FDI criteria to assess restorations is equally effective at 2 years.
Trial registration
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dental caries is the most prevalent chronic condition of people worldwide, with individuals being susceptible to this disease throughout their lifetime [1, 2]. The treatment of dental caries has cost implications especially with deep carious lesions approaching the pulp [3, 4]. Reversible pulpal injury resulting from a deep carious lesion can now be treated effectively using a selective, minimally invasive caries removal approach [5]. However, distinguishing between diagnoses of reversible/irreversible pulpitis is fundamental for the treatment to be successful and this remains a challenge as current clinical and radiographic diagnostic methods do not give an accurate representation of the histological status of the pulp [6]. Furthermore, success of the treatment is also associated with the quality of the restoration which must be assessed to predict the long-term clinical performance.
Clinical guidelines have been developed upon which judgments could be based for the assessment of dental restorations. Cvar and Ryge [7] developed criteria for the clinical evaluation of dental restorative materials for use by the United States Public Health Service—commonly known as “Ryge” or “USPHS” criteria. These criteria, with their many modifications, quickly gained popularity due to their clarity and workability and have been used extensively in studies worldwide [8]. An alternative checklist introduced by Hickel et al. [9] and approved by the FDI World Dental Federation claimed to be a more sensitive assessment method with enhanced discriminative power compared with the original Ryge criteria. However, few studies have adopted these criteria to date and this could be because long-term clinical studies which have already used the USPHS criteria are committed to completing their trials using the same criteria [10]. There certainly remains a need for studies comparing the FDI criteria with other existing restorative assessment criteria, i.e. the USPHS criteria to establish its validity and benefit in permanent teeth.
The 12-month results of this randomised controlled clinical trial showed no clinical difference in the dentine-pulp response between Biodentine™ and Fuji IX™ [11]. Cone beam computed tomography (CBCT) scans had detected periapical changes associated with teeth initially diagnosed with reversible pulpitis using electric pulp testing, thermal stimulation, and periapical radiographs indicating its potential in this field. Teeth identified to be healing using CBCT had received Biodentine™ while the majority of teeth which had not healed had received Fuji IX™ [11].
The aims of the present study were to (1) investigate clinically and radiographically the dentine-pulp response to calcium silicate cement (Biodentine™) compared to glass ionomer cement (Fuji IX™) used as indirect pulp capping (IPC) agents in teeth with symptoms of reversible pulpitis after 24 months, (2) assess the overlying resin composite restoration using both the USPHS and FDI criteria, and (3) compare the efficacy of the USPHS compared to the FDI criteria in the assessment of the resin composite restorations overlying both pulp protective agents.
Materials and methods
This randomised controlled clinical trial compared calcium silicate cement (Biodentine™, Septodont, Saint-Maur-des-Fossés, France) as the test material and glass ionomer cement (Fuji IX™ GP, GC Corporation, Tokyo, Japan) as the control material in patients with deep carious lesions and signs of reversible pulpitis. The patients were recruited from King’s College Dental Institute at Guy’s Hospital, London, England. Randomisation was performed centrally by the Biostatistics Unit using tabular randomisation, with the unit being the tooth and cavity size considered as a prognostic factor (1 wall, 2 walls, or more). Inclusion and exclusion criteria are presented in Table 1. Intensity of the pulp symptoms was recorded. Patients’ description of sensitivity to hot/cold/sweet lasting up to 15–20 s and settling spontaneously were considered mild, while increased pain for more than several minutes and needing pain killers were considered severe [11]. The clinical operator was trained to ensure standardisation of the operative procedures. Methods of clinical assessment included evaluation of pulp status using electric pulp testing (Kerr Vitality Scanner 2006, SybronEndo, Orange, CA, USA) and thermal testing (Roeko Endo-Frost, Coltène/Whaledent, Germany), palpation and percussion tests, along with the presence of signs of inflammation (pain, abscess, sinus tract, and abnormal mobility). Caries removal was carried out under local anaesthetic and rubber dam isolation using a minimal invasive standardised operative intervention procedure. Chemo-mechanical gel (Carisolv™, Rubicon Lifesciences, Gothenburg, Sweden) aided in the quantity of caries removal between the different teeth. Residual caries-affected dentine was retained on the pulp aspect of the cavity as any additional excavation would lead to pulp exposure [12]. With randomisation of either Biodentine™ or Fuji IX™, the tooth was fully restored according to the manufacturer’s instructions for both materials.
The definitive resin composite veneer restoration (N’Durance®, Septodont, Louisville, KY, USA) was placed 1 month after baseline in a “closed sandwich” technique where clinically achievable. Follow-up was longitudinal at T1-, T6-, T12- (reported previously: Hashem et al. [11]), and T24-month (± 2-week) intervals. Clinical success was evaluated by a positive response to cold test and electric pulp testing, absence of spontaneous pain, negative sensitivity to percussion, absence of sinus/fistula/swelling and abnormal mobility, and absence of periapical (PA) radiolucencies as determined by PA radiographs.
Details of the study methodology including study design, sample size, selection criteria, randomisation, and intervention have been described in conjunction with the 12-month data published previously [11].
Radiographic assessment
PA and CBCT radiographs were taken at baseline (T0) and T12. Additional PA radiographs were taken at T24 consultation. Exposure parameters at T0, T12, and T24 were standardised for each patient.
A consensus panel of two trained, calibrated, experienced endodontists assessed the PA radiographs jointly. The intra-examiner reliability of the consensus panel was evaluated by jointly repeating the assessment of the radiographic images after 2 weeks. No inter-examiner assessment was carried out as the examiners did not assess the radiographs individually. The paired images of the roots of each tooth were viewed together by examiners blinded as to which image was taken at T12/T24 and blinded to the pulp capping material used by concealing the restorations. Each root was examined for the presence, absence, and change (increase/decrease) in size of any PA radiolucency. Further details of the radiographic assessment have been reported previously [11].
Clinical assessment of the restoration
In addition to the clinical evaluation of the pulp status during the follow-up visits at T1, T6, T12, and T24 months, assessments of the resin composite restoration overlying Biodentine™ and Fuji IX™ were carried out by two experienced, trained, and calibrated independent examiners. Both were blinded to the restorative protocols used. The two examiners recorded the results independently at the same appointment, and any disagreement was resolved immediately by discussion. Two assessment criteria were used: modified USPHS criteria [13] and the FDI criteria [10]. The surfaces were dried with an air stream before evaluation. Assessment was carried out under ample lighting using a mirror and probe, and evaluation of the contact points was done using waxed dental floss in a reproducible manner. A satisfactory proximal contact point has physiological strength when the dental floss passes through and was evaluated for a certain degree of resistance or “snap” effect.
Statistical analysis
The first outcome of the study was a binary variable indicating whether the restored tooth failed to maintain its vitality at T24. The second outcome was that the integrity of the composite resin restoration overlying Biodentine™ is either as good as Fuji IX™ or better or worse. The third outcome of the study is the effectiveness of the FDI criteria is either equally effective or more effective than the modified USPHS criteria.
Descriptive statistics were used to summarise various study variables. Using IBM SPSS Statistics version 23 (IBM, USA), radiographic assessment included Fleiss’s kappa analysis to evaluate intra-examiners’ agreement. The outcome measures taken at T12 and T24 months were compared using the Mcnemar-Bowker test.
With regard to the criteria used to assess the restoration, intra/inter-examiner variability was calculated using Fleiss’s kappa, considering different ratings for each material. The integrity of the resin composite restorations overlying both materials assessed using the two criteria was summarised using percentages. The efficacy was analysed by comparing the proportion of assessment using the USPHS and FDI criteria for Biodentine™ and Fuji IX™. The assessment for each category in both criteria was compared between the materials using Z test for proportions for each rating separately. For all the analyses, statistical significance was assumed at 5% level.
Results
Clinical and radiographic assessment of the indirect pulp capping agents
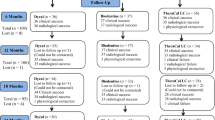
Seventy-two restorations (36 Biodentine™, 36 Fuji IX™) were placed in 53 patients at baseline, T0. After 24 months, recall rate was 70% where 42 restorations (21 Biodentine™ and 21 Fuji IX™) in 28 patients were followed up out of a total of 60 restorations (excluding the 12 failed teeth by T12) (Fig. 1). Reason for non-attendance was mainly due to loss of contact with the patient. A total of 15 teeth had failed to maintain vitality by T24 (6 Biodentine™/9 Fuji IX™) (Table 2), and there was no significant difference (p = 0.38) between the two materials (Biodentine™ and Fuji IX™) with respect to the failure rates. The further three teeth which had failed at T24 had received Fuji IX™ restorations.

Flow diagram indicating patient recruitment and follow-up. Adapted from the CONSORT flow diagram. Asterisks indicate that failed teeth are ones which developed irreversible pulpitis or pulp necrosis and underwent either root canal treatment or extraction
Clinical success rate of indirect pulp capping using both materials at 24 months was 72% (39/54). Clinical success rate for Biodentine™ was 77.8% (21/27) and for Fuji IX™ 66.7% (18/27) at 24 months. No significant difference (p = 0.07) was found in the success rate at 24 months between the two materials. A significant association (p = 0.001) was found between the failed teeth and the severity of the symptoms of reversible pulpitis (mild vs. severe). No significant association was found between the failed teeth and the extent of the cavity (p = 0.28) or gender (p = 0.19).
Twenty-eight paired (T12 + T24) PA radiographs were available for analysis. The kappa value for the intra-examiner reliability was 0.61, indicating substantial agreement between the two measurements. The Mcnemar-Bowker test, carried out to investigate the difference in outcome (healthy vs. PA radiolucency) at T12 and T24, showed a p value of 0.17 indicating that there is no significant difference between the two measurements. Only five teeth demonstrated difference in the PA radiographs between T12 and T24 (Table 3). It is worth noting that an area of radiolucency was observed subjectively and consistently subjacent to the Biodentine™ restorations coronally while this was less prominent beneath the Fuji IX™ restorations in the PA radiographs taken at T12 and T24 (Figs. 2 and 3).

Examples demonstrating radiolucent area subjacent to the Biodentine™ restorations (A, lower right 6; B, upper right 5; C, lower right 4)

Examples demonstrating radiolucent area subjacent to the Fuji IX™ restorations (D, lower left 6; E, lower left 6; F, upper left 7)
Clinical assessment of the integrity of the overlying restoration
Kappa values demonstrated good intra- and inter-examiner agreement using both assessment criteria for Biodentine™ and Fuji IX™ (Table 4). Overall, the integrity of the restoration was excellent to good when assessed using both the USPHS and FDI criteria. The p values for testing the proportion of ratings using the USPHS and FDI criteria for both Biodentine and Fuji IX™ were > 0.05 at baseline, 6, 12, and 24 months indicating that there is no statistically significant difference in the integrity of the resin composite restoration overlying Biodentine compared to Fuji IX™ when judged using the USPHS and FDI criteria.
Assessment of the efficacy of modified USPHS vs. FDI criteria
There was no statistically significant difference (p > 0.05) in the efficacy of the USPHS compared with the FDI criteria in the assessment of the Biodentine™ and Fuji IX™ restorations.
Discussion
There are several treatment methods available for the management of the pulp in extensively carious teeth. These range from conservative pulp capping procedures to root canal treatment. In this study, indirect pulp capping (protection) was carried out in teeth with signs of reversible pulpitis using Biodentine™ and Fuji IX™. After 12 months, the clinical success rate was 83.3% for both materials. This clinical success rate is similar to that of other materials such as calcium hydroxide and MTA when used as indirect pulp capping agents in permanent teeth [14, 15]. Studies on indirect pulp capping had clinical success ranging from 73 to 97% after a follow-up period of 2 weeks to 11 years [16]. In this study, the success rate for Biodentine™ after 24 months became 77.8% due to the lower recall rate and for Fuji IX™ was 66.7%. Indeed, the three teeth which had failed at 24 months had been restored with Fuji IX™. This difference was not statistically significant, perhaps due to the small number, but it should be noted that the distribution of mild and severe symptoms of reversible pulpitis was not equal between Biodentine™ and Fuji IX™ at baseline [11]. More teeth with severe symptoms had received Fuji IX™ at baseline which may contribute to the increased failure rate at T24. The boundary between severe symptoms of reversible pulpitis and irreversible pulpitis is blurred as the degree of pain does not necessarily reflect pulp histopathology [17]; this study recruited patients presenting to an acute dental care department, and therefore, symptoms were in general more intense than those associated with reversible pulpitis as defined by the American Association of Endodontists [18].
The long-term failure of glass ionomer cement (GIC) may be attributed to pulpal injury with chronic inflammatory exudate including lymphocytes, macrophages, and plasma cells indicating that pulpitis has been developed even in the absence of initial pain [19]. Certainly in all these cases, pulp necrosis had developed without clinical symptoms.
Earlier clinical studies on GIC placed in non-exposed deep cavities in human teeth reported no symptoms during the observation periods; however, when extracted, an increased inflammatory cell infiltrate in the odontoblast layer was found with more odontoblast aspiration and changes in the odontoblast layer which mostly resolved towards the end of the experiments [20,21,22]. It is worthy to note that the teeth used in these experiments were caries-free which may have contributed to the resolution of the inflammation at the end of the experiments.
Although Biodentine™ and Fuji IX™ are both two classes of water-based cement-type restorative materials with bioactive properties, their method of remineralisation and interaction with the underlying carious tissue is different [23, 24]. Biodentine™ induces an early form of reparative dentine synthesis through the modulation of pulp cell TGF-β1 secretion [25]. Furthermore, Biodentine™ induces cell proliferation and remineralisation by the increased uptake of calcium and silicon ions in addition to its caustic effect from the high alkalinity enhancing apatite formation and remineralisation [24, 26, 27]. Glass ionomer cements on the other hand lack this “caustic” effect as they are acidic in nature. However, this acidity promotes self-etching adhesion and, when placed on moist dentine, triggers an ionic exchange creating an intermediate ion-enriched layer derived from both substrates [23]. Their direct effect on pulp cells however has a cytotoxic effect. Although Fuji IX™ was not placed directly on the pulp in the present study, it may have aggravated a pre-existing compromised histopathological situation in the pulp. A histology analysis would be appropriate before a definitive explanation could be given.
The presence of a subjectively noticeable radiolucent area beneath the Biodentine™ restorations, and less obvious beneath the Fuji IX™ restorations, is an important finding on the T12 PA radiographs and has significant clinical implications. Both experimental groups underwent the same minimally invasive selective caries excavation procedure using Carisolv™ gel. The radiolucent band could be arrested and demineralised affected dentine due to the minimally invasive technique used in the excavation of caries, although if this theory is true, then the same extent of radiolucency should have been present beneath the Fuji IX™ restorations. Another theory could be an effect of the Biodentine™ caustically etching the underlying collagen matrix where mineral deposition may occur in the future. In either case, no re-entry is required and it is important to distinguish this from active caries adjacent to restorations and sealants (CARS) which requires re-entry. Further PA radiographs to monitor the radiolucency subjacent to the Biodentine™ restorations and comparing this with the Fuji IX™ restorations would be beneficial.
Both Biodentine™ and Fuji IX™ are not without limitations. While their therapeutic effect is well known, they are weak materials and are exposed to wear under load with time in addition to their poor aesthetic properties [28, 29]. Therefore, an overlay restoration is required to provide mechanical strength, wear resistance, and improved aesthetics. Resin composite is a popular choice as it is aesthetically pleasing and adheres well to glass ionomer cements [30] and potentially to Biodentine™ [29]. In this study, no difference was found in the resin composite restoration overlying both Biodentine™ and Fuji IX™. The resin composite restorations performed well during the 24 months which is to be expected due to the relatively short observation period. It has been shown that follow-up time needs to be longer, as differences between materials can emerge after more than 10 years [31]. No qualitative or quantitative wear measurement was carried out during the assessment of the composite restorations as this was outside the scope of this study and there are many studies available in the literature that discuss this aspect in detail.
Furthermore, there was no statistically significant difference in the efficacy of the USPHS criteria compared with the FDI criteria in the assessment of the composite restorations overlying Biodentine™ and Fuji IX™ restorations although the FDI criteria is more comprehensive and contains more detail. This could be due to the short follow-up period of 2 years which is insufficient to detect any changes to the composite restorations. Nevertheless, there were several observations regarding some of the subcategories in the FDI criteria noted during the assessment of the restorations. In the category “functional properties”, the subcategory “patient’s view” lacked a rating for sensitivity which was found to be a complaint by some of the patients. This could not be recorded in this specific subcategory although it was recorded in the subcategory “Postoperative (hyper)sensitivity and tooth vitality” found in the “biological property” category. Additionally, in the subcategory “Postoperative (hyper)sensitivity and tooth vitality”, it is not clear whether gingival hypersensitivity can be included in this subcategory which refers to tooth hypersensitivity rather than anything else. Furthermore, in the subcategory “radiographic examination”, no rating was available to note the radiolucent area beneath restorations which was consistent in many of the restorations but could not be recorded. Moreover, in the same subcategory “radiographic examination”, it was unclear what to rate any apical pathology not related directly to the restoration. Similarly, it was unclear what to rate slight gingival inflammation surrounding the tooth from plaque resulting from insufficient oral hygiene and not related to the restoration as the subcategory “periodontal response” in the biological properties referred to changes in the periodontium related to the restoration.
Consideration could be given to modify some aspects in the FDI criteria for improvement. From data analysis in the present study, this would include the addition of sensitivity in the subcategory “patient’s view”, adding gingival hypersensitivity to the subcategory “Postoperative (hyper)-sensitivity and tooth vitality”, and radiolucency beneath the restoration in the subcategory “radiographic examination”.
Conclusions
There is no significant difference in the dentine-pulp response between Biodentine™ and Fuji IX™ when assessed clinically and radiographically after 24 months. Furthermore, there is no difference in the integrity of the resin composite restorations overlying Biodentine™ compared to Fuji IX™ using both the USPHS and FDI criteria. The efficacy of the USPHS criteria compared to the FDI criteria in the assessment of the resin composite restorations was similar.
The intensity of the symptoms of reversible pulpitis seems to play a role in the success or failure of indirect pulp capping rather than the extent of the cavity or the choice of indirect pulp capping material. Failed indirect pulp capping is more related to severe symptoms of reversible pulpitis.
Using the USPHS or FDI criteria for the assessment of the restorations was both efficient during the short-time recall period; however, longer term follow-up is needed to establish whether the FDI criteria is more sensitive than the USPHS criteria.
References
Selwitz RH, Ismail AI, Pitts NB (2007) Dental caries. Lancet 369(9555):51–59
Marcenes W, Kassebaum NJ, Bernabé E, Flaxman A, Naghavi M, Lopez A, Murray CJ (2013) Global burden of oral conditions in 1990-2010 : a systematic analysis. J Dent Res 92(7):592–597
Ricketts D, Kidd E, Innes N, Clarkson J (2006) Complete or ultraconservative removal of decayed tissue in unfilled teeth. Cochrane Database Syst Rev 19(3):CD003808
Ricketts D, Lamont T, Innes NP, Kidd E, Clarkson JE (2013) Operative caries management in adults and children. Cochrane Database Syst Rev 28(3):CD003808
Tziafas D, Smith A, Lesot H (2000) Designing new treatment strategies in vital pulp therapy. J Dent 28(2):77–92
Dummer PMH, Hicks R, Huws D (1980) Clinical signs and symptoms in pulp disease. Int Endod J 13(1):27–35
Cvar JF, Ryge G (2005) Reprint of criteria for the clinical evaluation of dental restorative materials. Clin Oral Investig 9:215–232
Bayne SC, Schmalz G (2005) Reprinting the classic article on USPHS evaluation methods for measuring the clinical research performance of restorative materials. Clin Oral Investig 9:209–214
Hickel R, Roulet JF, Bayne S, Heintze SD, Mjör IA, Peters M, Rousson V, Randall R, Schmalz G, Tyas M (2007) Recommendations for conducting controlled clinical studies of dental restorative materials. Clin Oral Investig 11(1):5–33
Hickel R, Peschke A, Tyas M, Mjör I, Bayne S, Peters M, Hiller KA, Randall R, Vanherle G, Heintze SD (2010) FDI World Dental Federation: clinical criteria for the evaluation of direct and indirect restorations—update and clinical examples. Clin Oral Investig 14(4):349–366
Hashem D, Mannocci F, Patel S, Manoharan A, Brown JE, Watson TF, Banerjee A (2015) Clinical and radiographic assessment of the efficacy of calcium silicate indirect pulp capping: a randomized controlled clinical trial. J Dent Res 94(4):562–568
Kerkhove BJR, Herman S, Klein A, Mcdonald R (1967) A clinical and television densitometric evaluation of the indirect pulp capping technique. J Dent Child 34:192–201
Palaniappan S, Bharadwaj D, Mattar DL, Peumans M, Van Meerbeek B, Lambrechts P (2009) Three-year randomized clinical trial to evaluate the clinical performance and wear of a nanocomposite versus a hybrid composite. Dent Mater 25:1302–1314
Bjørndal L, Reit C, Bruun G, Markvart M, Kjældgaard M, Näsman P, Thordrup M, Dige I, Nyvad B, Fransson H et al (2010) Treatment of deep caries lesions in adults: randomized clinical trials comparing stepwise vs. direct complete excavation, and direct pulp capping vs. partial pulpotomy. Eur J Oral Sci 118(3):290–297
Leye Benoist F, Gaye Ndiaye F, Kane AW, Benoist HM, Farge P (2012) Evaluation of mineral trioxide aggregate (MTA) versus calcium hydroxide cement (Dycal®) in the formation of a dentine bridge: a randomised controlled trial. Int Dent J 62:33–39
Petrou MA, Alhamoui FA, Welk A, Altarabulsi MB, Alkilzy M, Splieth CH (2014) A randomized clinical trial on the use of medical Portland cement, MTA and calcium hydroxide in indirect pulp treatment. Clin Oral Investig 18:1383–1389
Mejàre IA, Axelsson S, Davidson T, Frisk F, Hakeberg M, Kvist T, Norlund A, Petersson A, Portenier I, Sandberg H, Tranaeus S, Bergenholtz G (2012) Diagnosis of the condition of the dental pulp: a systematic review. Int Endod J 45(7):597–613
Levin LG, Law AS, Holland GR, Abott PV, Roda RS (2009) Identify and define all diagnostic terms for pulpal health and disease states. J Endod 35:1645–1657
Gruythuysen R, Van Strijp G, Wu MK (2010) Long-term survival of indirect pulp treatment performed in primary and permanent teeth with clinically diagnosed deep carious lesions. J Endod 36(9):1490–1493
Tobias R, Browne R, Plant C, Ingram D (1978) Pulpal response to a glass ionomer cement. Br Dent J 144:345–350
Cooper I (1980) The response of the human dental pulp to glass ionomer cements. Int Endod J 13(2):76–88
Plant C, Browne R, Knibbs P, Britton A, Sorahan T (1984) Pulpal effects of glass ionomer cements. Int Endod J 17:51–59
Atmeh AR, Chong EZ, Richard G, Festy F, Watson TF (2012) Dentin-cement interfacial interaction: calcium silicates and polyalkenoates. J Dent Res 91(5):454–459
Watson TF, Atmeh AR, Sajini S, Cook RJ, Festy F (2014) Present and future of glass-ionomers and calcium-silicate cements as bioactive materials in dentistry: biophotonics-based interfacial analyses in health and disease. Dent Mater 30(1):50–61
Laurent P, Camps J, About I (2012) BiodentineTM induces TGF-β1 release from human pulp cells and early dental pulp mineralization. Int Endod J 45(5):439–448
Tran X, Gorin C, Willig C, Baroukh B, Pellat B, Decup F, Vital SO, Chaussain C, Boukpessi T (2012) Effect of a calcium-silicate-based restorative cement on pulp repair. J Dent Res 91(12):1166–1171
Han L, Okiji T (2013) Bioactivity evaluation of three calcium silicate based endodontic materials. Int Endod J 46(9):808–814
Davidson CL (2006) Advances in glass-ionomer cements. J Appl Oral Sci 14:3–9
Bachoo IK, Seymour D, Brunton P (2013) A biocompatible and bioactive replacement for dentine: is this a reality? The properties and uses of a novel calcium-based cement. Br Dent J 214:1–7
Van Dijken JW (1994) A 6-year evaluation of a direct composite resin inlay/onlay system and glass ionomer cement-composite resin sandwich restorations. Acta Odontol 52(6):368–376
Da Rosa Rodolpho PA, Donassollo TA, Cenci MS, Loguércio AD, Moraes RR, Bronkhorst EM, Opdam NJ, Demarco FF (2011) 22-year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dent Mater 27(10):955–963
Acknowledgements
The authors acknowledge the Saudi Cultural Office in London for sponsoring and supporting the work. Open access for this article was provided by King's College London.
Funding
This study was supported by the Centre of Excellence in Medical Engineering funded by the Wellcome Trust and by the Department of Health via the National Institute for Health Research (NIHR) comprehensive Biomedical Research Centre award to Guy’s and St. Thomas’ NHS Foundation Trust in partnership with King’s College London and King’s College Hospital NHS Foundation Trust.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The clinical trial was approved from the London Westminster research ethics committee (11/LO/1893) and is registered at ClinicalTrials.gov NCT02201641.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Hashem, D., Mannocci, F., Patel, S. et al. Evaluation of the efficacy of calcium silicate vs. glass ionomer cement indirect pulp capping and restoration assessment criteria: a randomised controlled clinical trial—2-year results. Clin Oral Invest 23, 1931–1939 (2019). https://doi.org/10.1007/s00784-018-2638-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2638-0