
Summary
Background
We aimed to assess coping and vegetative reactivity in uveal melanoma (UM) patients compared to controls with benign nevi of the uvea.
Material and methods
In total, 20 patients with recently diagnosed uveal melanoma were recruited and matched for age and gender to 20 controls with benign nevi of the uvea. Heart rate variability (HRV) and blood pressure variability (BPV) were monitored throughout an initial period of rest (POR1), a mental stress test (DT), and another period of rest (POR2). Coping strategies were assessed for both groups using a stress-coping questionnaire.
Results
The LF/HF ratio (low-/high-frequency component of total spectral power) of HRV showed decreasing values in the UM group and increasing values in controls throughout the measurement sequence (p = 0.025). Diastolic BPV revealed declining values of the low-frequency component in normalized units (LFnu) between POR1 and DT in UM patients compared to rising values between POR1 and DT in controls (p = 0.006). There were no intergroup differences in coping strategies (p > 0.05).
Conclusions
Coping mechanisms are unaltered in patients with uveal melanoma compared to controls, but vegetative reactivity may show a different pattern once patients are diagnosed.
Zusammenfassung
Hintergrund
Coping und vegetative Reaktivität wurden zwischen Patient*innen mit Aderhautmelanomen und Kontrollen mit benignen Aderhautnävi verglichen.
Material und Methode
In die Studie wurden 20 Patient*innen mit kürzlich diagnostizierten Aderhautmelanomen eingeschlossen und mit 20 Kontrollen, bei denen benigne Aderhautnävi vorlagen, verglichen. Die Herzfrequenzvariabilität und die Blutdruckvariabilität wurden als Indikatoren der vegetativen Reaktivität während einer initialen Ruheperiode, eines Stresstests sowie einer zweiten Ruheperiode erhoben. Anhand eines Fragebogens wurden zudem vorhandene Coping-Strategien aller Proband*innen ermittelt.
Ergebnisse
Das Verhältnis zwischen der Niederfrequenz- und der Hochfrequenzkomponente der Herzfrequenzvariabilität zeigte über die Testsequenz sinkende Werte in der Aderhautmelanomgruppe und steigende Werte in der Kontrollgruppe (p = 0,025). Die normierte Niederfrequenzkomponente der diastolischen Blutdruckvariabilität wies sinkende Werte zwischen der initialen Ruheperiode und dem Stresstest in der Aderhautmelanomgruppe sowie steigende Werte in der Kontrollgruppe auf (p = 0,006). Es gab keine Unterschiede im Coping beider Gruppen (p > 0,05).
Schlussfolgerung
In der vorliegenden Studie zeigten sich keine Unterschiede im Coping beider Gruppen, jedoch könnte das Vegetativum nach Diagnose eines Aderhautmelanoms verändert auf Stress reagieren.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Uveal melanoma (UM) is the most common ocular malignancy in adults. Traditional epidemiologic risk factors for UM include Caucasian ethnicity, male gender, older patient age, and the presence of choroidal nevi or ocular/oculodermal melanocytosis [1]. Genetic features of UM have been increasingly investigated in recent years and have improved tumor classification and prediction of metastatic disease [2]. A trend toward conservative treatment options [3] was validated by the Collaborative Ocular Melanoma Study that reported no significant differences in survival for patients assigned to either enucleation or brachytherapy [4]. Combined immunotherapy has demonstrated higher response rates compared to single-agent checkpoint inhibitors and new agents such as Tebentafusp have shown promising results [5, 6]. Despite these advances, the annual age-adjusted incidence of UM (5.1 per million) and the 5‑year relative survival (62–81.6%; [3, 7]) have both remained unchanged in recent decades [3].
The biopsychosocial model was established in 1977 and enabled physicians to recognize the psychosocial dimensions of disease [8]. It has since then been revealed that the immune system is particularly influenced by the nervous system and that both entities communicate constantly [9]. The psychosocial aspects of cutaneous melanoma (CM) have been extensively investigated in the past [10,11,12,13,14,15,16]. Compared to healthy controls, patients with atypical cutaneous nevi showed higher scores for mental tension and a higher vegetative arousal [15]. Furthermore, it was revealed that patients with CM use negative coping mechanisms more often than controls do [16].
With this investigation, we aimed to compare the vegetative reactivity of UM patients and controls with benign nevi of the uvea after a standardized stress test (Determination Stress Test). Furthermore, coping strategies of UM patient and controls were evaluated using an established questionnaire (SVF 120) that was previously used to assess stress-coping in CM patients [14, 16]. To our knowledge, this is the first exploration of stress-related psycho-vegetative reactivity and coping behavior in patients with uveal melanoma.
Material and methods
Study design and participants
In toral, 40 participants (20 women and 20 men) were recruited at the Department of Ophthalmology of the Medical University Graz, Austria. The study group consisted of 20 patients (10 women and 10 men) with recently diagnosed UM and was matched for age and gender to the control group consisting of 20 patients (10 women and 10 men) with benign nevi of the uvea. Patients aged between 18 and 99 years were eligible for inclusion if they were recently diagnosed (2–9 weeks prior to the study intervention) with UM (study group) or with benign nevi of the uvea (control group) and if they signed informed consent forms after an introductory patient briefing. Patients in the melanoma group did not receive information about their individual risk based on genetic testing. Exclusion criteria were cardiovascular disease, pregnancy or lactation in women, insufficient compliance or language skills, psychiatric disorders, other types of cancer (including non-recent UM) and distant metastasis. Exclusion criteria were identified based on the patients’ written clinical records and oral anamnesis. Explanatory information about UM and associated risks was given at the time of the initial presentation to avoid further confounding psychological factors at the time of the stress test. Patients with UM were scheduled for enucleation or radiation. All patients participated in the test procedure under equal conditions (see section “Measurement sequence”). Approval of the study protocol was obtained from the Ethics Committee of the Medical University Graz (EK-Number: 23 498 ex 10/11) and the study adhered to the tenets of the Declaration of Helsinki.
Determination Test
The Determination Test (DT; Schuhfried GmbH, Mödling, Austria) is an established tool in the fields of clinical, health, and neuropsychology. This test has previously been used to induce stress in patients with CM [11] and its validity has been demonstrated in several studies [17, 18]. It enables investigators to measure reactive stress tolerance and reaction speed. The mental strain for the test subject is generated by the requirement to sustain continuous or rapidly varying responses to changing stimuli. Participants were required to press specific buttons on a panel manually or by feet according to the color and acoustic stimuli presented. The intensity of the presented stimuli was adapted so that any participant was pressured until they were no longer able to perform the required tasks.
Vegetative monitoring
Vegetative monitoring was performed throughout the measurement sequence using an all-in-one workstation (Task Force® Monitor, CNSystems, Graz, Austria) and included electrocardiography (ECG), oscillometric blood pressure (oscBP), and continuous blood pressure (contBP). ContBP was measured directly using double finger sensors before being calibrated to oscillometric BP values. Vegetative parameters were subsequently calculated using an adaptive autoregressive parameter algorithm [19].
Vegetative reactivity was assessed using systolic and diastolic blood pressure variability (BPV) as well as heart rate variability (HRV). Heart rate variability was represented by the low-frequency (LF) component (frequency range 0.04–0.15 Hz) of total spectral power divided by its high-frequency (HF, frequency range 0.15–0.4 Hz) component (LF/HF ratio). As the LF component is mainly associated with sympathetic activity and the HF component with parasympathetic activity, the LF/HF ratio is a measure of the balance between both systems [20]. Blood pressure variability was described using the LF component for both systolic and diastolic blood pressure expressed in normalized units (LFnu = LF / (Total Power-VLF) × 100; VLF = Very low frequency component < 0.04 Hz). Again, the LF or LFnu component is mainly associated with sympathetic activity [21].
Stress-coping questionnaire SVF 120 (Stressverarbeitungsfragebogen 120)
The German stress-coping questionnaire SVF 120 was presented to all patients in its paper-and-pencil version to assess coping strategies. This widely utilized and validated instrument encompasses 120 items divided into 20 subtests. Each item can be answered on a 5-level rating scale and both positive and negative coping strategies are measured. The former result in efficient reduction of stress and are considered adequate coping strategies, whereas the latter are considered to be associated with stress-enhancing behavior. The questionnaire also evaluates strategies that cannot be assigned to either group. Positive/stress-reducing aspects include trivialization, disparagement, defense from guilt, diversion from the situation, substitute gratification, self-affirmation, relaxation, situation control, reaction control, and positive self-instruction. Negative/maladaptive strategies comprise escape, social withdrawal, intrusive thoughts, resignation, self-pity, and self-blame [16, 22].
Measurement sequence
Initially, the stress-coping questionnaire (SVF 120) was answered independently of the measurement sequence by each participant. Participants were then asked to rest in a sitting position for 5 min (period of rest 1, POR1), before performing the DT for about 15 min. The DT was followed by another period of rest (POR2, 5 min). The test procedure was conducted in a soundproof setting and vegetative parameters were monitored continuously throughout the whole process.
Statistical analysis
Metric parameters are descriptively summarized using mean, standard deviation (SD), and range (minimum—maximum). Categorical parameters are given as absolute and relative frequencies. Group differences in demographic data, patient characteristics and SVF 120 results were assessed using Student’s t test for independent groups. The distribution of psycho-vegetative data was evaluated and rank-transformed if the data were not normally distributed in any given measurement within any group. We performed a repeated measures analysis of variance (rmANOVA) with the original data or the rank-transformed data to analyze the effects of the measurement sequence (POR1, DT, POR2) and to compare both groups. If the effect of the measurement sequence was significant, we performed post hoc tests to specify these differences. Additionally, we defined contrasts to assess whether the testing conditions differed within each group. All p values for post hoc tests and contrasts were corrected for multiple comparisons according to Bonferroni. All analyses are regarded exploratory in nature and a p value of < 0.05 was considered significant. Calculations were performed using IBM SPSS Statistics (Release 21.0.0.0 2012, International Business Machines Corporation, Armonk, NY, USA).
Results
Demographics and patient characteristics are described in Table 1. In total, 40 participants (20 women and 20 men) with a mean age of 66.0 years (range 46.4–87.2) were recruited in accordance with the protocol. In the UM group, one patient was enucleated and 19 patients were treated using radiation. Of these, eight patients received LINAC-based (linear particle accelerator) stereotactic radiotherapy, ten patients were scheduled for ruthenium-106 plaque brachytherapy, and one for proton beam irradiation.
Vegetative monitoring
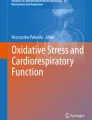
Descriptive analysis of vegetative parameters is summarized in Table 2. The heart rate, systolic blood pressure, and diastolic blood pressure increased from the first period of rest (POR1) to the stress test (DT, each p < 0.001), before decreasing back to baseline values in the second period of rest (POR2, each p < 0.001) without any differences between the two groups. The LF/HF ratio of HRV throughout the measurement sequence depended on the patient group and showed increasing values in controls and decreasing values in the UM group (p = 0.025). Systolic BPV (represented by LFnu) showed no significant intergroup differences or effects of the measurement sequence (p > 0.05). Similar to HRV, diastolic BPV (represented by LFnu) revealed an opposing trend for both groups throughout the measurement sequence (Fig. 1). The UM group showed declining values of LFnu (diastolic BPV) between POR1 and DT compared to rising values between POR1 and DT in controls (p = 0.006). Both the increase and the subsequent decrease of diastolic LFnu in the control group reached statistical significance (p = 0.014 and p = 0.016, respectively). Similar changes could not be observed in the UM group throughout the measurement sequence, i.e., diastolic BPV was unreactive to stress in the UM group (p > 0.05).

Diastolic blood pressure variability expressed as the mean low frequency component of total spectral power in normalized units (LFnu). Continuous line (1) = Uveal melanoma group, dotted line (2) = Control group; POR1 = Period of rest 1, DT = Determination Test, POR2 = Period of rest 2
Stress-coping questionnaire (Stressverarbeitungsfragebogen 120, SVF 120)
There were no intergroup differences in positive/stress-reducing coping strategies (trivialization, disparagement, defense from guilt, diversion from the situation, substitute gratification, self-affirmation, relaxation, situation control, reaction control, positive self-instruction) or negative/maladaptive coping strategies (escape, social withdrawal, intrusive thoughts, resignation, self-pity, self-blame; p > 0.05).
Summary
We assessed coping and vegetative reactivity in patients with uveal melanoma (UM) and controls. These aspects are important because they can reveal psychosocial dimensions of disease and because they can potentially be targeted using behavioral approaches. Coping is considered a habitual personality trait that is constant over time and unresponsive to acute stress [22]. Researchers have previously found that maladaptive coping is associated with faster glaucoma progression [23] and is more prevalent in patients with HLA-B27-associated acute anterior uveitis [24] and dry eye disease [25]. In our investigation, coping was evaluated using an established questionnaire that assesses positive and maladaptive strategies. We found no coping-related differences between UM patients and controls. This was unexpected, because previous studies revealed significant differences in coping between cutaneous melanoma (CM) patients and healthy controls: Trapp et al. showed that patients with CM use negative coping mechanisms more often compared to controls with benign dermatological disease and that the risk for CM with an initial thickness over 1 mm decreases in patients with positive coping strategies [16]. Furthermore, certain lymphocyte subpopulations showed positive correlations with negative coping strategies in CM patients, but were negatively correlated with healthy controls and their positive coping mechanisms [14]. Finally, positive coping styles were associated with both good psychosocial adjustment [13] and better outcomes [10].
Sufficient heart rate variability (HRV) is a desirable state in healthy individuals because it reflects parasympathetic (vagal) activity. The HRV decreases when the sympathetic system is activated due to stress. As the LF component of HRV is mainly associated with sympathetic activity and the HF component with parasympathetic activity, the LF/HF ratio is a measure of the balance between both systems [20]. Contrary to HRV, blood pressure variability (BPV) is associated with increased cardiovascular risk [26, 27]. The LF or LFnu component of BPV is mainly associated with sympathetic activity [21]. We opted to analyze BPV in addition to HRV, because HRV alone has been critically discussed as a marker for sympathetic activity [28, 29]. The LF/HF ratio of HRV showed increasing values throughout the measurement sequence in controls (increase of the sympathetic influence during the DT), but decreasing values in the UM group (unexpected decrease of the sympathetic influence during the DT). Similarly, the sympathetic influence on diastolic BPV increased in controls during activation (expressed as an increase of the LFnu component), but decreased in the UM group when mental stress was induced (decrease of the LFnu component). Our data therefore indicate a different pattern of sympathetic activity in UM patients compared to controls. This altered pattern could either be related to cancer pathogenesis (such as in CM) or the result of anxiety related to recent UM diagnosis. Because maladaptive coping (as an indicator of chronic vegetative dysfunction) was not relevant in our patients, we believe that the observed patterns may be interpreted as anxiety related to a life-altering diagnosis, although this is speculative. Heart rate variability has previously been explored in CM research and similar patterns were observed: Compared to healthy controls, patients with atypical cutaneous nevi showed higher questionnaire-based scores for mental tension and higher vegetative arousal after a paper–pencil-based stress test [15]. Furthermore, CM patients exhibited altered cytokine profiles and higher interleukin‑6 (a cytokine associated with stress) levels compared to healthy controls in response to the Determination Test [11]. Moreover, HRV is significantly reduced not only in various cancer types compared to healthy controls, but also in patients with metastases compared to non-metastatic patients [30]. A systematic meta-analysis previously reported that high HRV improves the survival in cancer patients with different etiologies [31]. Furthermore, it was revealed that patients with prostate and non-small lung cancer with low HRV show higher tumor marker levels compared to patients with high HRV [32].
Limitations
The main limitation of this study is its exploratory nature, its relatively small sample size, and the possibility of other confounding factors that were not inquired but may have influenced our results such as marital status and educational background. Autonomic testing is a complex field [33] and further investigations will be required to confirm our findings and to investigate possible effects of prognostic patient information (genetic testing) on our results.
Conclusion
In conclusion, this is the first investigation addressing coping and vegetative reactivity in patients with uveal melanoma (UM). Coping mechanisms are unaltered in UM patients compared to controls, but vegetative reactivity may show a different pattern once patients are diagnosed. Compared to cutaneous melanoma (CM), maladaptive coping seems to play a less important role in UM. However, sympathetic activity seems to be considerably changed once patients are diagnosed with UM, which makes it necessary to take interdisciplinary approaches to support patients in the best possible way.
Abbreviations
- BPV:
-
blood pressure variability
- CM:
-
cutaneous melanoma
- contBP:
-
continuous blood pressure
- DT:
-
Determination Test
- ECG:
-
electrocardiography
- HF:
-
high frequency
- HRV:
-
heart rate variability
- LF:
-
low frequency
- LFnu:
-
low frequency in normalized units
- LINAC:
-
linear particle accelerator
- oscBP:
-
oscillometric blood pressure
- POR:
-
period of rest
- rmANOVA:
-
repeated measures analysis of variance
- SD:
-
standard deviation
- SVF120:
-
Stressverarbeitungsfragebogen 120
- UM:
-
uveal melanoma
- VLF:
-
very low frequency
References
Yonekawa Y, Kim IK. Epidemiology and management of uveal melanoma. Hematol Oncol Clin North Am. 2012;26:1169–84.
Smit KN, Jager MJ, de Klein A, Kiliҫ E. Uveal melanoma: Towards a molecular understanding. Prog Retin Eye Res. 2020;75:100800.
Singh AD, Turell ME, Topham AK. Uveal melanoma: trends in incidence, treatment, and survival. Ophthalmology. 2011;118:1881–5.
Jampol LM, Moy CS, Murray TG, Reynolds SM, Albert DM, Schachat AP, u. a. The COMS Randomized Trial of Iodine 125 Brachytherapy for Choroidal Melanoma. IV. Local Treatment Failure and Enucleation in the First 5 Years after Brachytherapy. COMS Report No. Ophthalmology. 2020;127:S148–57.
Pelster MS, Gruschkus SK, Bassett R, Gombos DS, Shephard M, Posada L, et al. Nivolumab and Ipilimumab in Metastatic Uveal Melanoma: Results From a Single-Arm Phase II Study. J Clin Oncol. 2021;39:599–607.
Middleton MR, McAlpine C, Woodcock VK, Corrie P, Infante JR, Steven NM, et al. Tebentafusp, A TCR/Anti-CD3 Bispecific Fusion Protein Targeting gp100, Potently Activated Antitumor Immune Responses in Patients with Metastatic Melanoma. Clin. Cancer Res. 2020;26:5869–78.
Kujala E, Mäkitie T, Kivelä T. Very long-term prognosis of patients with malignant uveal melanoma. Invest Ophthalmol Vis Sci. 2003;44:4651–9.
Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129–36.
Dantzer R, Interactions N. From the Brain to the Immune System and Vice Versa. Physiol Rev. 2018;98:477–504.
Brown JE, Butow PN, Culjak G, Coates AS, Dunn SM. Psychosocial predictors of outcome: time to relapse and survival in patients with early stage melanoma. Br J Cancer. 2000;83:1448–53.
Richtig E, Trapp EM, Avian A, Brezinsek HP, Trapp M, Egger JW, et al. Psychological Stress and Immunological Modulations in Early-stage Melanoma Patients. Acta Derm Venereol. 2015;95:691–5.
Richtig E, Trapp M, Kapfhammer H‑P, Jenull B, Richtig G, Trapp E‑M. The Importance of a Biopsychosocial Approach in Melanoma ResearchExperiences from a Single-center Multidisciplinary Melanoma Working Group in Middle-Europe. Acta Derm Venereol. 2016;96:51–4.
Söllner W, Zschocke I, Zingg-Schir M, Stein B, Rumpold G, Fritsch P, et al. Interactive patterns of social support and individual coping strategies in melanoma patients and their correlations with adjustment to illness. Psychosomatics. 1999;40:239–50.
Trapp E‑M, Trapp M, Avian A, Rohrer PM, Weissenböck T, Kapfhammer H‑P, et al. Association of Stress Coping Strategies with Immunological Parameters in Melanoma Patients. Acta Derm Venereol. 2016;96:74–7.
Trapp M, Egger JW, Kapfhammer H‑P, Trapp E‑M, Rohrer PM, Hörlesberger N, et al. Higher psychological and psychovegetative strain in adolescents with atypical pigment naevi. Acta Derm Venereol. 2015;95:67–71.
Trapp M, Trapp E‑M, Richtig E, Egger JW, Zampetti A, Sampogna F, et al. Coping strategies in melanoma patients. Acta Derm Venereol. 2012;92:598–602.
Baur H, Müller S, Hirschmüller A, Huber G, Mayer F. Reactivity, stability, and strength performance capacity in motor sports. Br J Sports Med. 2006;40:906–10. discussion 911.
Brunnauer A, Laux G. Driving ability under sertindole. Pharmacopsychiatry. 2012;45:47–50.
Fortin J, Klinger Th, Wagner Ch, Sterner H, Madritsch Ch, Grüllenberger R, u. a. The Task Force Monitor—A Non-invasive Beat-to-beat Monitor for Hemodynamic and Autonomic Function of the Human Body [Internet]. [zitiert 8. August 2023]. Verfügbar unter: https://www.ni.com/pdf/csma/us/fortin.pdf
Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J. 1996;17:354–81.
Parati G, Saul JP, Di Rienzo M, Mancia G. Spectral analysis of blood pressure and heart rate variability in evaluating cardiovascular regulation. A critical appraisal. Hypertension. 1995;25:1276–86.
Erdmann G. SVF – Stressverarbeitungsfragebogen – Stress, Stressverarbeitung und ihre Erfassung durch ein mehrdimensionales Testsystem. Göttingen. Co: Hogrefe; 2008.
Freeman EE, Lesk MR, Harasymowycz P, Desjardins D, Flores V, Kamga H, u. a. Maladaptive coping strategies and glaucoma progression. Medicine (Baltimore). 2016;95:e4761.
Maca SM, Schiesser AW, Sobala A, Gruber K, Pakesch G, Prause C, et al. Distress, depression and coping in HLA-B27-associated anterior uveitis with focus on gender differences. Br J Ophthalmol. 2011;95:699–704.
Patel S, Felix ER, Levitt RC, Sarantopoulos CD, Galor A. Dysfunctional Coping Mechanisms Contribute to Dry Eye Symptoms. J Clin Med. 2019;8.
Parati G, Stergiou GS, Dolan E, Bilo G. Blood pressure variability: clinical relevance and application. J Clin Hypertens (greenwich). 2018;20:1133–7.
Stevens SL, Wood S, Koshiaris C, Law K, Glasziou P, Stevens RJ, et al. Blood pressure variability and cardiovascular disease: systematic review and meta-analysis. BMJ. 2016;354:i4098.
Frith J, Zalewski P, Klawe JJ, Pairman J, Bitner A, Tafil-Klawe M, et al. Impaired blood pressure variability in chronic fatigue syndrome—a potential biomarker. Qjm. 2012;105:831–8.
Goldstein DS, Bentho O, Park M‑Y, Sharabi Y. Low-frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp Physiol. 2011;96:1255–61.
Kloter E, Barrueto K, Klein SD, Scholkmann F, Wolf U. Heart Rate Variability as a Prognostic Factor for Cancer Survival—A Systematic Review. Front Physiol. 2018;9:623.
Zhou X, Ma Z, Zhang L, Zhou S, Wang J, Wang B, et al. Heart rate variability in the prediction of survival in patients with cancer: A systematic review and meta-analysis. J Psychosom Res. 2016;89:20–5.
De Couck M, van Brummelen D, Schallier D, De Grève J, Gidron Y. The relationship between vagal nerve activity and clinical outcomes in prostate and non-small cell lung cancer patients. Oncol Rep. 2013;30:2435–41.
Illigens BMW, Gibbons CH. Autonomic testing, methods and techniques. Handb Clin Neurol. 2019;160:419–33.
Acknowledgements
We thank Mag. Astrid Arbeiter and Mag. Brigitte Bliem for psychological support of our patients.
Funding
Open access funding provided by Medical University of Graz.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M. Gabriel, E.-M. Trapp, P. Rohrer, M. Trapp, G. Schwantzer, A. Mester, E. Richtig, C. Schwab, G. Langmann, J. Egger and C. Mayer-Xanthaki declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gabriel, M., Trapp, EM., Rohrer, P. et al. Coping and vegetative reactivity in uveal melanoma. Spektrum Augenheilkd. (2023). https://doi.org/10.1007/s00717-023-00552-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00717-023-00552-1