
Abstract
An outbreak of COVID-19 in Shanghai, China, in March 2022 was caused by the Omicron variant. The epidemic lasted for more than 3 months, and the cumulative number of infected people reached 626,000. We investigated the impact of clinical factors on disease outcomes in patients with COVID-19. Using a case-control study design, we examined cases from fever clinics with confirmed Omicron variant infection, analyzed their population and laboratory diagnostic characteristics, and provided theoretical support for subsequent epidemic prevention and control. Logistic regression was used to identify factors associated with infection with the Omicron variant. The results of this study show that the COVID-19 vaccine can protect against infection with the Omicron variant, and more than 50% of infected people had not been vaccinated. Compared with the epidemic in Wuhan 2 years ago, most of the patients in the hospital in the Shanghai epidemic had underlying diseases (P = 0.006). A comparison of patients infected with the Omicron variant in Shanghai and patients with other respiratory tract infections showed no significant difference in the levels of neutrophils, lymphocytes, eosinophils, white blood cells, hemoglobin, or platelets (P > 0.05). People over 60 years old and those with underlying diseases were at risk for pneumonia (OR = 14.62 (5.49-38.92), P < 0.001; OR = 5.29 (2.58-10.85), P < 0.001, respectively), but vaccination was a protective factor (OR = 0.24 (0.12-0.49), P < 0.001). In summary, vaccination has a potential effect on infection with Omicron variant strains and provides protection against pneumonia. The severity of illness caused by the Omicron variant in 2022 was significantly lower than that of the original SARS-CoV-2 variant from two years previously.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Omicron variant was first detected in South Africa on November 9, 2021 [1]. It then rapidly spread to the United States, Europe, and other regions and was declared by WHO to be the fifth "variant of concern" [2]. The Omicron variant spread widely in March 2022 in Shanghai, China [3], with its first local case detected March 2, 2022, and the cumulative number of SARS-CoV-2 infections reaching more than 626,000 [4, 5]. The Omicron epidemic began earlier in Shanghai than in 71 other cities in 21 provinces in China, so it is of great significance to analyze the characteristics of this epidemic in Shanghai. Omicron lineage BA.2 was primarily responsible for the coronavirus outbreak in Shanghai in the first half of 2022, which had a severe disease rate of 0.27% and a case fatality rate of 0.09% [6]. Despite vaccination, the elderly are at significant risk of progression to severe disease or death due to infection with Omicron. At present, residents of the Chinese mainland have three inactivated vaccine COVID-19 vaccines available (China's biological vaccine, Wuhan biological vaccine, and Beijing CoronaVac), as well as an adenovirus-vectored vaccine (Ad5-nCoV). Although the overall vaccination coverage of the population of Shanghai exceeds 90%, only 62% of the 5.8 million people over 60 years old have been vaccinated, and only 38% of the population has received a booster vaccine [7]. Despite the lower virulence of the Omicron BA.2 sublineage, the risk of progression to severe disease or death after infection remains high [8].
Earlier clinical studies on wild strains of SARS-CoV-2 showed that laboratory indicators of infection, such as lymphocyte count, T lymphocyte count, liver enzyme index, myocardial enzyme index, and D-dimer, are useful for predicting whether patients develop severe disease [9, 10]. The Omicron variant strain has been reported to have a shorter incubation period, higher infectivity, and pathogenicity and to produce a higher viral load than the original strain [11]. The local outbreak in Shanghai occurred after widespread vaccination of the population against COVID-19.
We compared the characteristics of patients in Shanghai fever clinics and patients in Wuhan in 2020. The general profiles of patients diagnosed with Omicron infection and those hospitalized due to influenza during the same period were compared. The susceptibility factors for pneumonia caused by Omicron variant strains were analyzed, and the protective effect of COVID-19 vaccination on patients infected with Omicron variant strains was assessed. This study will provide a reference for prevention and control of COVID-19.
Materials and methods
General information
COVID-19-positive patients attending the infection department of Shanghai Changzheng Hospital between 1 March 2022 and 30 May 2022 were included in this study. A total of 316 target cases were included in the initial stage. After screening by the inclusion and exclusion criteria, 144 patients were finally included in the study group (SH-C group), and 144 patients with similar clinical symptoms who visited a doctor due to other upper respiratory tract infections, such as influenza virus, adenovirus, or respiratory syncytial virus, were included as a control group (SH-N group) (Fig. 1).

Study flow chart
In addition, we retrospectively collected information on 173 positive cases of COVID-19 in Wuhan from February 1, 2020, to May 30, 2020, as a historical control (WH-C group). This retrospective study, supported by the General Program of Huoshenshan Hospital, complies with the Declaration of Helsinki, and all patients gave informed consent.
Diagnostic criteria
The diagnostic criteria for positive cases of COVID-19 in this study are based on the "COVID-19 Pneumonia Diagnosis and Treatment Program (Trial Version 9)" issued by the General Office of the National Health Commission [12]. The clinical classification of COVID-19-positive cases is also based on the above scheme, and the research subjects were divided into mild and severe groups.
Collection of information
The hospitalization history was collected, and general data (including epidemiological history, gender, age, underlying diseases), clinical symptoms, laboratory indicators, diagnosis, treatment, and outcomes were retrospectively analyzed and grouped by type for comparison. The flow chart for patient enrollment is shown in Fig. 1.
Statistical methods
Data were processed using SPSS 24.0. Enumeration data were expressed as cases (%), and the χ2 test or Fisher's exact test was used. Measurement data that conformed to a normal distribution were expressed as the mean ± standard deviation (x ± s), and were analyzed by t-test; those that did not exhibit a normal distribution were expressed as the median and interquartile interval (M, median; P25, 25 percent, P75, 75 percent), and the Mann-Whitney U test was used. Logistic regression was used to analyze the influencing factors of outcome variables, and the odds ratio (OR) represents the association strength. P < 0.05 indicates statistical significance.
Results
General information about the enrolled patients
A total of 461 subjects were enrolled in this study and divided into three groups: the 2022 Shanghai COVID-19 group (SH-C), the 2022 Shanghai non-COVID-19 group (SH-N), and the 2020 Wuhan COVID-19 group (WH-C). The general information about the three groups of subjects is shown in Table 1. Among the population included in this study, the WH-C group had the highest mean age (60.4 years), and SH-N had the lowest mean age (42.7 years). There was no significant difference in the male-female ratio among the three groups. The etiology of the three groups was significantly different, namely Omicron variant, respiratory infection, and the original SARS-CoV-2 strain. The rate of vaccination against COVID-19 in the SH-C group was significantly lower than in the SH-N group (49.65% vs. 72.73%, P < 0.001).
Differences between the Shanghai epidemic and the Wuhan epidemic
The COVID-19 outbreak in Shanghai was fundamentally different from the outbreak in Wuhan that occurred two years previously. Among the hospitalized patients, 34.0% of the patients in the SH-C group were less than 50 years old, which was a significantly higher percentage than that in WH-C group. There was no statistical difference in the percentage of each sex among the people with COVID-19 during the different periods. The mean body temperature of the SH-C group was 37.5℃, whereas in the WH-C group it was 38.0°C, and this difference was statistically significant (P < 0.001). In addition, the mean leukocyte count and incidence of pneumonia and symptoms were higher in the SH-C group than in the WH-C group (P < 0.05) (Table 2). The overall prevalence of underlying disease in the SH-C group was also higher than that in the WH-C group (P = 0.006). Ranked from high to low by prevalence, these diseases included hypertension, cerebrovascular disease, diabetes, heart disease, post-operative illness, liver disease, kidney disease, and autoimmune disease. The prevalence of heart disease was statistically different between the two groups (P = 0.032). However, no statistical differences were found among the groups for the other underlying diseases due to their low prevalence rates (P > 0.05) (Table 2). Underlying diseases often increase the impact of COVID-19 on the health of the patient.
Differences between COVID-19 and other respiratory infections
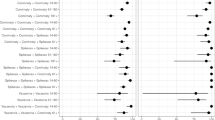
Comparative analysis showed that there was no significant difference in body temperature between patients with COVID-19-related pneumonia and those with other respiratory tract infections in Shanghai (P = 0.099). On average, patients with COVID-19 in Shanghai had lower white blood cell counts (WBCs) and lower C-reactive protein (CRP) levels than those with other respiratory tract infections, and the difference was statistically significant (P < 0.05). There was no significant difference in neutrophil rate (N%), lymphocyte rate (L%), eosinophils, red blood cell (RBC) count, hemoglobin (HB), or platelet (PLT) count between patients with COVID-19 and those with other respiratory tract infections (P > 0.05). However, monocytes were higher in patients with COVID-19 than in patients with other respiratory tract infections (P < 0.001) (Fig. 2).

Comparative analysis of patients with COVID-19-related pneumonia and respiratory tract infections in Shanghai. WBC white blood cell count, N% neutrophil rate, L% lymphocyte rate, RBC red blood cell count, HB hemoglobin, PLT platelet count, CRP C-reactive protein
Analysis of risk factors for pneumonia caused by Omicron
To identify risk factors for COVID-19-related pneumonia caused by Omicron, we use the internal control method. Among the 144 patients with COVID-19, 63 had pneumonia and 81 did not. Univariate analysis showed that age over 60 years was a risk factor for COVID-19-related pneumonia (OR = 14.62 (5.49-38.92), P < 0.001). Vaccination was a protective factor (OR = 0.24 (0.12-0.49), P < 0.001), and people with underlying diseases were more likely to develop pneumonia (OR = 5.29 (2.58-10.85), P < 0.001). No significant difference in body temperature was observed between pneumonia patients and non-pneumonia patients (P > 0.05). However, in terms of WBC and CRP indicators, the abnormal rate was significantly higher in pneumonia patients than in the control group (P < 0.05) (Table 3).
Discussion
The Omicron variant was first discovered in South Africa in November 2021 and soon spread around the world [13]. On June 2, 2022, the Shanghai Municipal Government Information Office reported that gene sequencing had confirmed that the Shanghai epidemic was caused mainly by the Omicron BA.2 and BA.2.2 variants [5, 14].
There was a larger proportion of the patients treated in the hospital during the Shanghai epidemic who had underlying diseases than in Wuhan two years previously. Most patients who come to the fever clinic have fever or other symptoms of respiratory tract infection, whereas many individuals with COVID-19 with no obvious symptoms and are identified by screening and sent to mobile hospital units.
In the comparative analysis of patients with COVID-19-related pneumonia and other respiratory tract infections in Shanghai, we found that there was no significant difference in body temperature between patients with COVID-19-related pneumonia and those with other respiratory tract infections. This shows that although the Omicron variant spreads rapidly and has a wide range, its symptoms are similar to those of other respiratory tract infections. Among people with COVID-19, age over 60 years old and having underlying diseases are risk factors for the occurrence of pneumonia, but vaccination against the Omicron variant is an important protective factor.
According to China's "Zero COVID-19" policy, active surveillance, epidemiological investigation, and timely nucleic acid testing can help to facilitate the rapid detection of new cases, minimize the scope of screening, and stop transmission [15]. Furthermore, enhanced health management of the elderly, especially those with underlying diseases, may help to reduce the incidence of severe and critical pneumonia [16].
Conclusions
The outbreak of local cases in Shanghai was caused by the Omicron variant, and vaccination with the COVID-19 vaccine provides protection against the development of severe disease after Omicron infection. Since this study did not include investigation of dynamic changes in laboratory parameters of patients during the treatment process, this needs to be addressed in future follow-up and research work.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
He X, Hong W, Pan X, Lu G, Wei X (2021) SARS-CoV-2 Omicron variant: Characteristics and prevention. MedComm (2020) 2(4):838–845. https://doi.org/10.1002/mco2.110
Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R (2022) Features, evaluation, and treatment of coronavirus (COVID-19). In: StatPearls [Internet]. StatPearls Publishing, Treasure Island
Cai J, Deng X, Yang J, Sun K, Liu H, Chen Z et al (2022) Modeling transmission of SARS-CoV-2 Omicron in China. Nat Med 28(7):1468–1475. https://doi.org/10.1038/s41591-022-01855-7
Huang L (2022) Adjusted control rate closely associated with the epidemiologic evolution of the recent COVID-19 wave in Shanghai, with 94.3% of all new cases being asymptomatic on first diagnosis. J Infect. https://doi.org/10.1016/j.jinf.2022.07.010
Chen Z, Deng X, Fang L, Sun K, Wu Y, Che T et al (2022) Epidemiological characteristics and transmission dynamics of the outbreak caused by the SARS-CoV-2 Omicron variant in Shanghai, China: a descriptive study. medRxiv [Preprint]. 2022. https://doi.org/10.1101/2022.06.11.22276273
Chen X, Yan X, Sun K, Zheng N, Sun R, Zhou J et al (2022) Estimation of disease burden and clinical severity of COVID-19 caused by Omicron BA.2 in Shanghai, February–June 2022. Emerg Microbes Infect 11(1):2800–2807. https://doi.org/10.1080/22221751.2022.2128435
Zhang X, Zhang W, Chen S (2022) Shanghai’s life-saving efforts against the current omicron wave of the COVID-19 pandemic. Lancet 399(10340):2011–2012. https://doi.org/10.1016/S0140-6736(22)00838-8
Cheung PH, Chan CP, Jin DY (2022) Lessons learned from the fifth wave of COVID-19 in Hong Kong in early 2022. Emerg Microbes Infect 11(1):1072–1078. https://doi.org/10.1080/22221751.2022.2060137
Ochani R, Asad A, Yasmin F, Shaikh S, Khalid H, Batra S et al (2021) COVID-19 pandemic: from origins to outcomes. A comprehensive review of viral pathogenesis, clinical manifestations, diagnostic evaluation, and management. Infez Med 29(1):20–36
Ai J, Zhang H, Zhang Y, Lin K, Zhang Y, Wu J et al (2022) Omicron variant showed lower neutralizing sensitivity than other SARS-CoV-2 variants to immune sera elicited by vaccines after boost. Emerg Microbes Infect 11(1):337–343. https://doi.org/10.1080/22221751.2021.2022440
Wu J, Wei Y, Shen F, Zhu S, Lu Y, Tian X et al (2022) Vaccination is associated with shorter time to target cycle threshold value in patients with SARS-CoV-2 omicron variant. Front Cell Infect Microbiol 12:943407. https://doi.org/10.3389/fcimb.2022.943407
National Health Commission. COVID-19 diagnosis and treatment plan (trial version 7) [BE/OL]. http://www.nhc.gov.a/yzygj/s7653p/202003/46c9294a7dfe4cef80dc7f5912eb1989.shtml,2020-03-03
Aleem A, Akbar Samad AB, Slenker AK (2022) Emerging variants of SARS-CoV-2 and novel therapeutics against coronavirus (COVID-19). In: StatPearls [Internet]. StatPearls Publishing, Treasure Island
Guo Y, Han J, Zhang Y, He J, Yu W, Zhang X et al (2022) SARS-CoV-2 omicron variant: epidemiological features, biological characteristics, and clinical significance. Front Immunol 13:877101. https://doi.org/10.3389/fimmu.2022.877101
Shi Y, Jiang HL, Yang MX, Dong LJ, Chen Y, Zhou YB et al (2021) The precision of epidemiological investigation of COVID-19 transmission in Shanghai, China. Infect Dis Poverty 10(1):58. https://doi.org/10.1186/s40249-021-00849-w
Yu X, Sun X, Cui P, Pan H, Lin S, Han R et al (2020) Epidemiological and clinical characteristics of 333 confirmed cases with coronavirus disease 2019 in Shanghai, China. Transbound Emerg Dis 67(4):1697–1707. https://doi.org/10.1111/tbed.13604
Acknowledgements
This work was funded by the General Program of Huoshenshan Hospital (zhuanyuan [2020]52).
Author information
Authors and Affiliations
Contributions
Huilan Tu, Sheng Tu, and Shiqi Gao wrote the paper; Huilan Tu made the figures and tables; Anwen Shao and Jifang Sheng revised the paper.
Corresponding authors
Ethics declarations
Conflict of interest
The authors state that there was no conflict of interest in the preparation of this study.
Ethical approval
The study protocol conformed to the ethical guidelines of the 2013 Helsinki Declaration and was approved by the Institutional Ethical Review Board of Second Military Medical University. Each study participant provided written informed consent.
Additional information
Handling Editor: Pablo Pineyro .
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhang, Y., Wang, J., Xie, Y. et al. Epidemiological characteristics of patients from fever clinics during the COVID-19 epidemic in 2022 in Shanghai, China. Arch Virol 168, 164 (2023). https://doi.org/10.1007/s00705-023-05755-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00705-023-05755-0