
Abstract
Background
To examine the factors contributing to persistent and recurrent hemifacial spasms (HFS) following a microvascular decompression (MVD) procedure and to suggest technical improvements to prevent such failures.
Methods
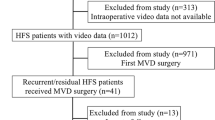
A retrospective review was conducted on fifty-two cases of repeat surgery. The extent of the previous craniotomy and the location of neurovascular compression (NVC) were investigated. The operative findings were categorized into two groups: “Missing Compression” and “Teflon Contact”. The analysis included long-term outcomes and operative complications after repeat MVD procedures.
Results
Missing compression was identified in 29 patients (56%), while Teflon contact was observed in 23 patients (44%). Patients with missing compression were more likely to experience improper craniotomy (66%) compared to those with Teflon contact (48%). Medially located NVC was a frequent finding in both groups, mainly due to compression by the anterior inferior cerebellar artery. In the missing compression group, during the repeat MVD, Teflon sling retraction was utilized in 79% of cases, while in the Teflon contact group, the most common procedure involved removing the Teflon in contact (65%). After the repeat MVD procedure, immediate spasm relief was achieved in 42 patients (81%), with six (12%) experiencing delayed relief. After a median follow-up of 54 months, 96% of patients were free from spasms. Delayed facial palsy, facial weakness, and hearing impairment were more frequently observed in the Teflon contact group.
Conclusions
A proper craniotomy that provides adequate exposure around the REZ is crucial to prevent missing the culprit vessel during the initial MVD procedure. Teflon contact on the REZ should be avoided, as it poses a potential risk of procedure failure and recurrence.



Similar content being viewed by others


Data availability
Data is available upon reasonable request.
Code availability
Not applicable.
References
Amagasaki K, Nishimura S, Uchida T, Tatebayashi K, Nakaguchi H (2021) Infrafloccular approach effectively prevents hearing complication in microvascular decompression surgery for hemifacial spasm. Br J Neurosurg 8:1–4
Barker FG 2nd, Jannetta PJ, Bissonette DJ, Shields PT, Larkins MV, Jho HD (1995) Microvascular decompression for hemifacial spasm. J Neurosurg 82:201–210
Bigder MG, Kaufmann AM (2016) Failed microvascular decompression surgery for hemifacial spasm due to persistent neurovascular compression: an analysis of reoperations. J Neurosurg 124:90–95
Bozkurt B, Kalani MYS, Yağmurlu K, Belykh E, Preul MC, Nakaji P, Spetzler RF (2018) Low retrosigmoid infratonsillar approach to lateral medullary lesions. World Neurosurg 111:311–316
El Refaee E, Fleck S, Matthes M, Marx S, Baldauf J, Schroeder HWS (2021) Outcome of endoscope-assisted microvascular decompression in patients with hemifacial spasm caused by severe indentation of the brain stem at the pontomedullary sulcus by the posterior inferior cerebellar artery. Oper Neurosurg (Hagerstown) 20:399–405
Engh JA, Horowitz M, Burkhart L, Chang YF, Kassam A (2005) Repeat microvascular decompression for hemifacial spasm. J Neurol Neurosurg Psychiatry 76:1574–1580
Holste K, Sahyouni R, Teton Z, Chan AY, Englot DJ, Rolston JD (2020) Spasm freedom following microvascular decompression for hemifacial spasm: systematic review and meta-analysis. World Neurosurg 139:e383–e390
Inoue T, Goto Y, Shitara S, Keswani R, Prasetya M, Arham A, Kikuta K, Radcliffe L, Friedman AH, Fukushima T (2022) Indication for a skull base approach in microvascular decompression for hemifacial spasm. Acta Neurochir 164:3235–3246
Inoue T, Shitara S, Goto Y, Arham A, Prasetya M, Radcliffe L, Fukushima T (2021) Bridge technique for hemifacial spasm with vertebral artery involvement. Acta Neurochir 163:3311–3320
Inoue T, Shitara S, Shima A, Goto Y, Fukushima T (2021) Double collagen matrix grafting for dural closure in microvascular decompression: an alternative use of autologous fascial grafting. Acta Neurochir 163:2395–2401
Jannetta PJ (1975) The cause of hemifacial spasm: definitive microsurgical treatment at the brainstem in 31 patients. Trans Sect Otolaryngol Am Acad Ophthalmol Otolaryngol 80:319–322
Jannetta PJ (1983) Hemifacial spasm: treatment by posterior fossa surgery. J Neurol Neurosurg Psychiatry 46:465–466
Jannetta PJ, Abbasy M, Maroon JC, Ramos FM, Albin MS (1977) Etiology and definitive microsurgical treatment of hemifacial spasm. Operative techniques and results in 47 patients. J Neurosurg 47:321–328
Jeon C, Jung NY, Kim M, Park K (2023) Intraoperative monitoring of the facial nerve during microvascular decompression for hemifacial spasm. Life (Basel) 13:1616
Jiang C, Xu W, Dai Y, Lu T, Jin W, Liang W (2017) Failed microvascular decompression surgery for hemifacial spasm: a retrospective clinical study of reoperations. Acta Neurochir 159(2):259–263
Lee S, Park SK, Lee JA, Joo BE, Park K (2019) Missed culprits in failed microvascular decompression surgery for hemifacial spasm and clinical outcomes of redo surgery. World Neurosurg 129:e627–e633
Liebelt BD, Huang M, Britz GW (2018) A comparison of cerebellar retraction pressures in posterior fossa surgery: extended retrosigmoid versus traditional retrosigmoid approach. World Neurosurg 113:e88–e92
Matsushima T, Yamaguchi T, Inoue TK, Matsukado K, Fukui M (2000) Recurrent trigeminal neuralgia after microvascular decompression using an interposing technique. Teflon felt adhesion and the sling retraction technique. Acta Neurochir 142:557–561
Mercier P, Sindou M (2018) The conflicting vessels in hemifacial spasm: Literature review and anatomical-surgical implications. Neurochirurgie 64:94–100
Polo G, Fischer C, Sindou MP, Marneffe V (2004) Brainstem auditory evoked potential monitoring during microvascular decompression for hemifacial spasm: intraoperative brainstem auditory evoked potential changes and warning values to prevent hearing loss--prospective study in a consecutive series of 84 patients. Neurosurgery 54:97–104
Quiñones-Hinojosa A, Chang EF, Lawton MT (2006) The extended retrosigmoid approach: an alternative to radical cranial base approaches for posterior fossa lesions. Neurosurgery 58:208–214
Raso JL, Gusmão SN (2011) A new landmark for finding the sigmoid sinus in suboccipital craniotomies. Neurosurgery 68:1–6
Rawlinson JN, Coakham HB (1988) The treatment of hemifacial spasm by sling retraction. Br J Neurosurg 2:173–178
Sindou M, Leston JM, Decullier E, Chapuis F (2008) Microvascular decompression for trigeminal neuralgia: the importance of a noncompressive technique--Kaplan-Meier analysis in a consecutive series of 330 patients. Neurosurgery 63:341–350
Sindou M, Mercier P (2018) Microvascular decompression for hemifacial spasm: outcome on spasm and complications. A review. Neurochirurgie 64:106–116
Sindou M, Mercier P (2018) Microvascular decompression for hemifacial spasm: Surgical techniques and intraoperative monitoring. Neurochirurgie 64:133–143
Wang X, Thirumala PD, Shah A, Gardner P, Habeych M, Crammond D, Balzer J, Burkhart L, Horowitz M (2013) Microvascular decompression for hemifacial spasm: focus on late reoperation. Neurosurg Rev 36:637–643
Wanibuchi M, Fukushima T, Zenga F, Friedman AH (2009) Simple identification of the third segment of the extracranial vertebral artery by extreme lateral inferior transcondylar-transtubercular exposure (ELITE). Acta Neurochir 151:1499–1503
Xu X, Su S, Cai L, Wang L, Fan H, Wu C, Chen Y (2022) Hemifacial spasm caused by distal neurovascular compression confirmed by lateral spread response monitoring. J Craniofac Surg 3:2555–2559
Zhong J, Li ST, Zhu J, Guan HX, Zhou QM, Jiao W, Ying TT, Yang XS, Zhan WC, Hua XM (2012) A clinical analysis on microvascular decompression surgery in a series of 3000 cases. Clin Neurol Neurosurg 114:846–851
Author information
Authors and Affiliations
Contributions
Study concept and design: Takuro Inoue. Data collection and analysis: Takuro Inoue, Yukihiro Goto, Yasuaki Inoue, Mustaqim Prasetya, and Takanori Fukushima. Data interpretation: Peter Adidharma. Writing the manuscript: Takuro Inoue. Reviewing and editing: Yukihiro Goto, Yasuaki Inoue, and Mustaqim Prasetya. Supervision: Takanori Fukushima. All authors approved the final version of the submitted manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Inoue, T., Goto, Y., Inoue, Y. et al. Potential reasons for failure and recurrence in microvascular decompression for hemifacial spasm. Acta Neurochir 165, 3845–3852 (2023). https://doi.org/10.1007/s00701-023-05861-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-023-05861-7