
Abstract
Introduction
The aim of this study was to evaluate the outcome of endovascular coiling of ruptured anterior communicating artery (AcomA) aneurysms followed by intracerebral hematoma (ICH) evacuation with burr hole trephination and catheterization.
Methods
Twelve patients treated by coiling with subsequent ICH drainage with burr hole trephination and catheterization were recruited from 290 patients with ruptured AcomA aneurysm in our hospital between January 2001 and June 2007. The clinical and radiographic characteristics and outcomes of the 12 patients were retrospectively analyzed.
Results
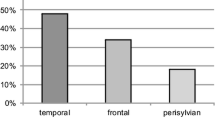
All 12 patients were male, aged from 29 to 62 years, and had ICHs with 16-ml to 45-ml volumes; nine (75%) of them had frontal ICHs on the opposite side of the dominant A1. Admission Hunt-Hess (HH) grade was 4 in eight patients, 3 in two, and 5 in two. The treatment outcomes in 8 of the 12 patients were good recovery or moderately disabled (Glasgow Outcome Scale; GOS 5 or 4), and functionally dependent (GOS 3 or 2) in the other 4 patients at the 6-month clinical follow-up. There was no rebleeding during the follow-up (mean, 22.9 months; range, 7 to 68 months).
Conclusion
The result of our series suggests that coiling with subsequent evacuation of the ICH with burr hole trephination and catheterization may be an alternative treatment option for ruptured AcomA aneurysm with an ICH requiring evacuation on the opposite side of the dominant A1.


Similar content being viewed by others


References
Abbed KM, Oglivy CS (2003) Intracerebral hematoma from aneurysm rupture. Neurosurg Focus 15:E4
Aoyagi N, Hayakawa I, Iai S, Tsuchida T, Furihata S (1985) Study of ruptured intracranial aneurysms with intracerebral hematomas–with special reference to operative indication. No Shinkei Geka (Japanese) 13:511–518
Hauerberg J, Eskesen V, Rosenorn J (1994) The prognostic significance of intracerebral hematoma as shown on CT scanning after aneurysmal subarachnoid haemorrhage. Br J Neurosurg 8:333–339
Heiskanen O, Poranen A, Kuurne T, Valtonen S, Kaste M (1988) Acute surgery for intracerebral haematomas caused by rupture of an intracranial arterial aneurysm. A prospective randomized study. Acta Neurochir 90:81–83
Jeong JH, Koh JS, Kim EJ (2007) A less invasive approach for ruptured aneurysm with intracranial hematoma: coil embolization followed by clot evacuation. Kor J Radiol 8:2–8
Niemann DB, Wills AD, Maartens NF, Kerr RS, Byrne JV, Molyneux AJ (2003) Treatment of intracerebral hematomas caused by aneurysm rupture: coil placement followed by clot evacuation. J Neurosurg 99:843–847
Nowak G, Schwachenwald D, Schwachenwald R, Kehler U, Muller H, Arnold H (1988) Intracerebral hematomas caused by aneurysm rupture. Experience with 67 cases. Neurosurg Rev 21:5–9
Pasqualin A, Bazzan A, Cavazzani P, Scienza R, Licata C, Da Pian R (1986) Intracranial hematomas following aneurysmal rupture: experience with 309 cases. Surg Neurol 25:6–17
Shimoda M, Oda S, Mamata Y, Tsugane R, Osamu S (1997) Surgical indications in patients with an intracerebral hemorrhage due to ruptured middle cerebral artery aneurysm. J Neurosurg 87:170–175
Tapaninaho A, Hernesniemi J, Vapalahti M (1988) Emergency treatment of cerebral aneurysms with large haematomas. Acta Neurochir (Wien) 91:21–24
Tokuda Y, Inagawa T, Katoh Y, Kumano K, Ohbayashi N, Yoshioka H (1995) Intracerebral hematoma in patients with ruptured cerebral aneurysms. Surg Neurol 43:272–277
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
Chung et al. reported an interesting retrospective study dealing with 12 patients, all males, showing a ruptured AcomA with ICH requiring no “ultra-early” evacuation, so that they opted first for coil embolization (CE) immediately followed by ICH evacuation (burr hole and catheterization). These 12 cases showed an aneurysm suitable for CE and/or an ICH on the opposite side of the dominant A1. The indication for ICH drainage required that the ICH volume was >20 ml, a midline shift >5 mm, and/or clinical deterioration. Two patients in three showed a favorable outcome (GOS scores of 5 or 4). No mortality was reported.
While the authors introduced their paper by reporting that they experienced 31 patients with ICH from 218 patients with a ruptured ICA, it was confusing to read further that they recruited 53 patients with a ruptured AcomA aneurysm with an associated frontal hematoma from a population of 290 ruptured AcomA treated either by embolization or surgery. Other points are also confusing. First, this series came from a population of 53 ruptured AcomA aneurysms with ICH of whom only 10 (19%) were urgently treated by surgical clipping and ICH evacuation. This low rate is clearly unusual; in our group among 22 AcomA aneurysms with ICH, 9 (41%) went for surgery, 11 for CE, and 2 died rapidly. Second, it is surprising to read that while the authors stressed that ICAs with ICH are prone to rebleeding, the majority (31/53) of their ruptured AcomA aneurysms with ICH were initially treated conservatively. Third, they indicated that an ICH volume >20 ml was required to evacuate the ICH, while in their series two patients (Table 1, patients 2 and 8) did not fulfill this criterion. These three points in particular would have required reporting the clinical results for the entire population (53 patients) and not exclusively for a particular selected group. In our experience, all ruptured AcomA aneurysms with a mass effect ICH were accessed through the hematoma side, and temporarily clipping the opposite A1 when required has so far never been a problem.
On the other hand, it was interesting to learn that patients with ruptured AcomA and significant ICH but not requiring “ultra-urgent” evacuation can be effectively treated by first CE followed by ICH evacuation through a burr hole. However, this strategy still needs to be confirmed in a prospective study reporting the clinical results for all ruptured AcomAs with an ICH.
C. Raftopoulos,
G. Vaz
Rights and permissions
About this article
Cite this article
Chung, J., Kim, B.M., Shin, Y.S. et al. Treatment of ruptured anterior communicating artery aneurysm accompanying intracerebral hematomas: endovascular coiling followed by hematoma evacuation with burr hole trephination and catheterization. Acta Neurochir 151, 917–923 (2009). https://doi.org/10.1007/s00701-009-0328-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-009-0328-z