
Abstract
Introduction
Infantile myofibromatosis is a rare mesenchymal disorder that occurs predominantly in infancy and early childhood, in either solitary or multicentric form. It can affect soft tissue, muscle, skeleton, and occasionally, visceral organs. Infantile myofibromatosis without visceral involvement frequently undergoes spontaneous regression. Multicentric infantile myofibromatosis with involvement exclusively of the calvarium is extremely rare.
Discussion
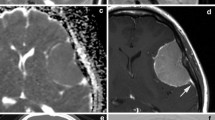
We report an 8-month-old girl who presented with multifocal calvarial lesions. The child underwent total excision of the temporal mass, and histopathological study gave a diagnosis of infantile myofibromatosis. Serial follow-up by neuroimaging was obtained at 3, 6, 12, and 24 months postoperatively. Three months after surgery, a new lesion in the midline of frontal bone was found, and there was partial regression of the occipital lesion. Complete regression of the untreated lesions was shown at 24 months. Illustrated by our patient and literature review, we emphasize the importance of recognition and proper intervention for this rare, nonmalignant disorder.


Similar content being viewed by others


References
Cardia E, Molina D, Zaccone C, La Rosa G, Napoli P (1993) Intracranial solitary-type infantile myofibromatosis. Childs Nerv Syst 9:246–249. doi:10.1007/BF00303579
Chapman PR, Judd CD, Felgenhauer JL, Gruber DP, Mornin D (2005) Infantile myofibromatosis of the posterior fossa. AJR 184:1310–1312
Chung EB, Enzinger FM (1981) Infantile myofibromatosis. Cancer 48:1807–1818. doi:10.1002/1097-0142(19811015) 48:8<1807::AID-CNCR2820480818&>3.0.CO;2-G
Cruz AA, Maia EM, Burmamm TG, Perez LC, Santos AN, Valera ET, Tone LG (2004) Involvement of the bony orbit in infantile myofibromatosis. Ophthal Plast Reconstr Surg 20:252–254. doi:10.1097/01.IOP.0000123501.30336.2C
Detwiler PW, Porter RW, Coons SW, Spetzler RF, Carrion CA, Rekate HL (1999) Sporadic unifocal infantile myofibromatosis involving the skull. Case report. J Neurosurg 90:1129–1132
Fukasawa Y, Ishikura H, Takada A, Yokoyama S, Imamura M, Yoshiki T, Sato H (1994) Massive apoptosis in infantile myofibromatosis. A putative mechanism of tumor regression. Am J Pathol 144:480–485
Hasegawa M, Kida S, Yamashima T, Yamashita J, Takakuwa S (1995) Multicentric infantile myofibromatosis in the calvarium: case report. Neurosurgery 36:1200–1203
Hutchinson L, Sismanis A, Ward J, Price L (1991) Infantile myofibromatosis of the temporal bone: a case report. Am J Otol 12:64–66
Ikediobi NI, Iyengar V, Hwang L, Collins WE, Metry DW (2003) Infantile myofibromatosis: support for autosomal dominant inheritance. J Am Acad Dermatol 49:S148–S150. doi:10.1067/mjd.2003.333
Inwards CY, Unni KK, Beabout JW, Shives TC (1991) Solitary congenital fibromatosis (infantile myofibromatosis) of bone. Am J Surg Pathol 15:935–941. doi:10.1097/00000478-199110000-00003
Kaplan SS, Ojemann JGM, Grange DK, Fuller C, Park TS (2002) Intracranial infantile myofibromatosis with intraparenchymal involvement. Pediatr Neurosurg 36:214–217. doi:10.1159/000056059
Léauté-Labrèze C, Labarthe MP, Blanc JF, Sanyas P, Dosquet C, Taïeb A (2001) Self-healing generalized infantile myofibromatosis with elevated urinary bFGF. Pediatr Dermatol 18:305–307. doi:10.1046/j.1525-1470.2001.01933.x
Niimura K, Shirane R, Yoshimoto T (1997) Infantile myofibromatosis located in the temporal bone. Childs Nerv Syst 13:629–632. doi:10.1007/s003810050157
Okamoto K, Ito J, Takahashi H, Emura I, Mori H, Furusawa T, Sakai K, Higuchi T, Tokiguchi S (2000) Solitary myofibromatosis of the skull. Eur Radiol 10:170–174. doi:10.1007/s003300050028
Queralt JA, Poirier VC (1995) Solitary infantile myofibromatosis of the skull. AJNR Am J Neuroradiol 16:476–478
Roggli VL, Kim HS, Hawkins E (1980) Congenital generalized fibromatosis with visceral involvement. A case report. Cancer 45:954–960. doi:10.1002/1097-0142(19800301)45:5<954::AID-CNCR2820450520>3.0.CO;2-Q
Rutigliano MJ, Pollack IF, Ahdab-Barmada M, Pang D, Albright AL (1994) Intracranial infantile myofibromatosis. J Neurosurg 81:539–543
Söylemezoglu F, Tezel GG, Köybaşoglu F, Er U, Akalan N (2001) Cranial infantile myofibromatosis: report of three cases. Childs Nerv Syst 17:524–527. doi:10.1007/s003810100486
Stout AP (1954) Juvenile fibromatosis. Cancer 7:953–978. doi:10.1002/1097-0142(195409)7:5<953::AID-CNCR2820070520>3.0.CO;2-W
Tamburrini G, Gessi M, Colosimo C, Lauriola L, Giangaspero F, Di Rocco C (2003) Infantile myofibromatosis of the central nervous system. Childs Nerv Syst 19:650–654. doi:10.1007/s00381-003-0744-y
Tsuji M, Inagaki T, Kasai H, Yamanouchi Y, Kawamoto K, Uemura Y (2004) Solitary myofibromatosis of the skull: a case report and review of literature. Childs Nerv Syst 20:366–369. doi:10.1007/s00381-003-0874-2
Weinberger CH, Dinulos JG, Perry AE (2007) An enlarging tender nodule on the finger of a 4-year-old boy: an unusual presentation of infantile myofibromatosis. J Am Acad Dermatol 57:S30–S32. doi:10.1016/j.jaad.2006.12.008
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
The case is well imaged and I found the review of historical cases useful to confirm the attitude to a “wait and see” policy for multiple (solitary) skull lesions after diagnosis, a thing that also a first reader on this subject will find helpful for the management of occasionally observed cases.
Gianpiero Tamburrini,
Rome, Italy
Comment
The rarity of this pathological entity, the particular multifocal location to the calvaria justifies its knowledge.
It is important to recognize this lesion from the differential diagnosis with others pathological entities as eosinophilic granuloma, fibrosarcoma, fibrous dysplasia, epidermoid cyst, diploic meningioma, osteomyelitis.
The authors have done a exhaustive revision of literature and the discussion about the strategy to choose the treatment of this non malignant pathology is important to avoid surgical extensive removal for a disease that can regress spontaneously because it is a self-limited disorder.
If the calvaria location is very rare as single location, the intraparenchymal extension is exceptional as reported in literature.
The natural history is characterized by a period of initial rapid growth followed by a stabilisation and a spontaneous regression.
The role of surgery is admitted to take a sample to establish a true diagnosis mainly in solitary lesion.
The paper is well written and well documented and so can help all neurosurgeons to think of this lesion in case of pathological disease of the calvaria either in a single or in multiple locations.
Carmine Mottolese,
Lyon, France
Rights and permissions
About this article
Cite this article
Zhou, DB., Zhao, JZ., Zhang, D. et al. Multicentric infantile myofibromatosis: a rare disorder of the calvarium. Acta Neurochir 151, 641–646 (2009). https://doi.org/10.1007/s00701-009-0264-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-009-0264-y