
Abstract
Purpose
Mortality rates after pancreatic resection are now lower than 5% in high-volume centers; however, morbidity remains high. This stresses the importance of identifying accurate predictors of operative morbidity after pancreatic resection. The Estimation of Physiologic Ability and Surgical Stress (E-PASS) scoring system was developed for a comparative audit of general surgical patients. Our previous study confirmed its usefulness for predicting morbidity after pancreaticoduodenectomy. In the present study, we evaluated whether the E-PASS scoring system can predict the occurrence of complications after distal pancreatectomy (DP).
Methods
The subjects were 46 patients who underwent DP for pancreatic disease. We studied correlations between the incidence of postoperative complications and the preoperative risk score (PRS), surgical stress score (SSS), and comprehensive risk score (CRS) of the E-PASS scoring system.
Results
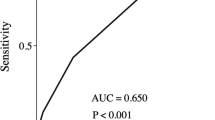
A collective total of 20 postoperative complications developed in 13 (28.3%) of the 46 patients. All E-PASS scores, particularly PRS and CRS, were significantly higher in the patients with postoperative complications than in those without complications. The complication rate increased with increasing PRS, SSS, and CRS scores.
Conclusion
The E-PASS scoring system is useful for predicting morbidity after DP.
Similar content being viewed by others


References
Benzoni E, Saccomano E, Zompicchiatti A, Lorenzin D, Baccarani U, Adani G, et al. The role of pancreatic leakage on rising of postoperative complications following pancreatic surgery. J Surg Res 2008;149:272–277.
Kooby D, Gillespie T, Bentrem D, Nakeeb A, Schmidt M, Merchant N, et al. Left-sided pancreatectomy. A multicenter comparison of laparoscopic and open approaches. Ann Surg 2008;248:438–446.
Kleeff J, Diener M, Z’graggen K, Hinz U, Wagner M, Bachmann J, et al. Distal Pancreatectomy. Risk factors for surgical failure in 302 consecutive cases. Ann Surg 2007;245:573–582.
Mohebati A, Schwarz R. Extended left-sided pancreatectomy with spleen preservation. J Surg Oncol 2008;97:150–155.
Abe N, Sugiyama M, Suzuki Y, Yamaguchi T, Mori T, Atomi Y. Preoperative endoscopic pancreatic stenting: a novel prophylactic measure against pancreatic fistula after distal pancreatectomy. J Hepatobiliary Pancreat Surg 2008;15:373–376.
Kawai M, Tani M, Yamaue H. Transection using bipolar scissors reduces pancreatic fistula after distal pancreatectomy. J Hepatobiliary Pancreat Surg 2008;15:366–372.
Okano K, Kakinoki K, Yachida S, Izushi K, Wakabayashi H, Suzuki Y. A simple and safe pancreas transection using a stapling device for a distal pancreatectomy. J Hepatobiliary Pancreat Surg 2008;15:353–358.
Kitagawa H, Ohta T, Tani T, Tajima H, Nakagawara H, Ohnishi I, et al. Nonclosure technique with saline-coupled bipolar electrocautery in management of the cut surface after distal pancreatectomy. J Hepatobiliary Pancreat Surg 2008;15:377–383.
Diener M, Knaebel H, Witte S, Rossion I, Kieser M, Buchler M, et al. DISPACT trial: a randomized controlled trial to compare two different surgical techniques of DIStal PAnCreaTectomy — study rationale and design. Clinical Trials 2008;5:534–545.
Irani J, Ashley S, Brooks D, Osteen R, Raut C, Russell S, et al. Distal pancreatectomy is not associated with increased perioperative morbidity when performed as part of a multivisceral resection. J Gastrointest Surg 2008;12:2177–2182.
Ferrone C, Warshaw A, Rattner D, Berger D, Zheng H, Rawal B, et al. Pancreatic fistula rates after 462 distal pancreatectomies: staplers do not decrease fistula rates. J Gastrointest Surg 200812:1691–1697.
Truty M, Sawyer M, Que F. Decreasing pancreatic leak after distal pancreatectomy: saline-coupled radiofrequency ablation in a porcine model. J Gastrointest Surg 2008;11:998–1007.
Koukoutsis I, Tamijmarane A, Bellagamba R, Bramhall S, Buckels J, Mirza D. The impact of splenectomy on outcomes after distal and total pancreatectomy. World J Surg Oncol 2007;5:61.
Carrere N, Abid S, Julio C, Bloom E, Pradere B. Spleen-preserving distal pancreatectomy with excision of splenic artery and vein: a case-matched comparison with conventional distal pancreatectomy with splenectomy. World J Surg 2007;31:375–382.
Sasaki A, Nitta H, Nakajima J, Obuchi T, Baba S, Wakabayashi G. Laparoscopic spleen-preserving distal pancreatectomy with conservation of the splenic artery and vein: report of three cases. Surg Today 2008;38:955–958.
Iso Y, Sawada T, Tagaya N, Kato M, Rokkaku K, Shimoda M, et al. Pancreatic juice leakage is a risk factor for deep mycosis after pancreatic surgery. Surg Today 2009;39:326–331.
Haga Y, Ikei S, Ogawa M. Estimation of physiologic ability and surgical stress (E-PASS) as a new prediction scoring system for postoperative morbidity and mortality following elective gastrointestinal surgery. Surg Today 1999;29:219–225.
Oka Y, Nishijima J, Oku K, Azuma T, Inada K, Miyazaki S, et al. Usefulness of an estimation of physiologic ability and surgical stress (E-PASS) scoring system to predict the incidence of postoperative complications in gastrointestinal surgery. World J Surg 2005;29:1029–1033.
Hashimoto D, Takamori H, Sakamoto Y, Ikuta Y, Nakahara O, Furuhashi S, et al. Is Estimation of physiologic ability and surgical stress (E-PASS) able to predict operative morbidity after pancreaticoduodenectomy? J Hepatobiliary Pancreat Surg 2009; Online First. DOI: 10.1007/s00534-009-0116-4.
Japan Pancreas Society. General rules for the study of pancreatic cancer. 5th ed. April 2002.
Furue H. Criteria for the direct effect of chemotherapy against solid cancer by Japanese Society for Cancer Therapy (in Japanese). J Jpn Soc Cancer Ther 1986;21:931–942.
Haga Y, Wada Y, Takeuchi H, Kimura O, Furuya T, Sameshima H, et al. Estimation of physiologic ability and surgical stress (E-PASS) for a surgical audit in elective digestive surgery. Surgery 2004135:586–594.
http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_v30
Baba Y, Haga Y, Hiyoshi Y, Imamura Y, Nagai Y, Yoshida N, et al. Estimation of physiologic ability and surgical stress (E-PASS system) in patients with esophageal squamous cell carcinoma undergoing resection. Esophagus 2008;5:81–86.
Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: An international study group (ISGPF) definition. Surgery 2005;138:8–13.
Tang T, Walsh S, Fanshawe T, Seppi V, Sadat U, Hayes P, et al. Comparison of risk-scoring methods in predicting the immediate outcome after elective open abdominal aortic aneurysm surgery. Eur J Vasc Endovasc Surg 2007;34:505–513.
Tang T, Walsh S, Fanshawe T, Gillard J, Sadat U, Varty K, et al. Estimation of physiologic ability and surgical stress (E-PASS) as a predictor of immediate outcome after elective abdominal aortic aneurysm surgery. Am J Surg 2007;194:176–182.
Kaneko H, Takagi S, Otsuka Y, Tsuchiya M, Tamura A, Katagiri T, et al. Laparoscopic liver resection of hepatocellular carcinoma. Am J Surg 2005;189:190–194.
Goh B, Tan Y, Chung Y, Cheow P, Ong H, Chan W, et al. Critical appraisal of 232 consecutive distal pancreatectomies with emphasis on risk factors, outcome, and management of the postoperative pancreatic fistula: a 21-year experience at a single institution. Arch Surg 2008;143:956–965.
Sierzega M, Niekowal B, Kulig J, Popiela T. Nutritional status affects the rate of pancreatic fistula after distal pancreatectomy: a multivariate analysis of 132 patients. J Am Coll Surg 2007205:52–59.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Hashimoto, D., Takamori, H., Sakamoto, Y. et al. Can the physiologic ability and surgical stress (E-PASS) scoring system predict operative morbidity after distal pancreatectomy?. Surg Today 40, 632–637 (2010). https://doi.org/10.1007/s00595-009-4112-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-009-4112-8