
Abstract
Aims
The effects of continuous subcutaneous insulin infusion (CSII) therapy with or without continuous glucose monitoring (CGM) on neonatal outcomes and glycemic outcomes of pregnant women with type 1 diabetes (T1D), living in Poland, were assessed.
Methods
This prospective observational study enrolled women with T1D (N = 481, aged 18–45 years) who were pregnant or planned pregnancy. All used CSII therapy and a subset used CGM with CSII (CSII + CGM). Neonatal outcomes (e.g., rate of large for gestational age [LGA] delivery [birth weight > 90th percentile]) and maternal glycemia (e.g., HbA1c and percentage of time at sensor glucose ranges) were evaluated.
Results
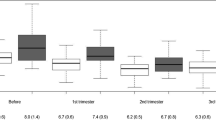
Overall HbA1c at trimesters 1, 2, and 3 was 6.8 ± 1.1% (50.9 ± 12.3 mmol/mol, N = 354), 5.8 ± 0.7% (40.1 ± 8.0 mmol/mol, N = 318), and 5.9 ± 0.7% (41.4 ± 8.0 mmol/mol, N = 255), respectively. A HbA1c target of < 6.0% (42 mmol/mol) at each trimester was achieved by 20.9% (74/354), 65.1% (207/318), and 58.0% (148/255), respectively. For women using CSII + CGM versus CSII only, HbA1c levels at trimesters 1, 2, and 3 were 6.5 ± 0.9% versus 7.1 ± 1.3% (47.8 ± 9.7 mmol/mol versus 54.3 ± 14.0 mmol/mol, p < 0.0001), 5.7 ± 0.6% versus 6.0 ± 0.9% (38.9 ± 6.5 mmol/mol versus 41.6 ± 9.3 mmol/mol, p = 0.0122), and 5.8 ± 0.6% versus 6.1 ± 0.8% (40.3 ± 6.9 mmol/mol versus 42.9 ± 9.1 mmol/mol, p = 0.0117), respectively. For the overall, CSII only, and CSII + CGM groups, rates of LGA delivery were 22.7% (74/326), 24.6% (34/138), and 21.3% (40/188), respectively.
Conclusions
Observational assessment of women with T1D using CSII therapy demonstrated low HbA1c throughout pregnancy and low rates of LGA. The addition of CGM to CSII therapy compared to CSII therapy alone was associated with some improved maternal glycemic and neonatal outcomes.
Clinicaltrials.gov identifier
NCT01779141 (January 2013).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Diabetes management technology (i.e., continuous subcutaneous insulin infusion [CSII] therapy or continuous glucose monitoring [CGM]) has been shown to improve outcomes in non-pregnant individuals living with T1D [1,2,3,4,5]. Pregnancies complicated by T1D warrant particularly careful management, given the risks of adverse outcomes for both mother and baby [6]. Compared to pregnant women without diabetes, women with T1D are at a particularly increased risk of hypoglycemia (especially in early pregnancy) [7], diabetic ketoacidosis [8], preeclampsia [9], miscarriage [10, 11], preterm birth [12], and other complications [10, 13]. Compared to neonates of women without diabetes, babies of mothers with T1D are at increased risk of negative neonatal composite outcomes including being large for gestational age (LGA, birth weight > 90th percentile for the population) [11, 14], macrosomia (neonate birth weight > 4000 g, regardless of gestational age) [10, 15] or congenital malformation [12, 16], and having increased rates of perinatal mortality [11, 12, 16] and neonatal hypoglycemia [10, 11]. A majority of these negative neonatal outcomes are primarily associated with increased fetal hyperglycemia exposure [17,18,19,20,21]. In consequence, macrosomia and LGA affect about half of all babies of mothers with T1D [14], and notably these children go on to live with increased risk of future obesity [19], diabetes [17], and cardiovascular disease [22].
Fortunately, pre-pregnancy planning that includes either CSII or MDI therapy has been reported to improve HbA1c and pregnancy outcomes [23, 24] and, significantly, compared to unplanned pregnancy [23]. Recent prospective observational study of maternal and neonatal outcomes in pregnant women receiving comprehensive preconception planning with either CSII or MDI demonstrated significantly reduced severe adverse pregnancy outcomes when compared with women who received routine care [25]. While good or improved glycemic control (a low or lowered HbA1c level) is observed with intensive insulin treatment and/or diabetes technology management therapies, high rates of LGA or macrosomia [21, 26] and other complications can still persist.
Given the reported impact of pre-pregnancy planning and CGM therapy in pregnancies complicated by T1D [21, 27,28,29], we report on the maternal glycemic and neonatal composite outcomes from an observational study of pregnant women with T1D who used CSII with or without CGM during the Orchestra Foundation (Fundacja Wielka Orkiestra Swiatecznej Pomocy) insulin pump donation program in Poland.
Methods
This prospective, observational study assessed Polish women (18–45 years of age) with pregestational T1D, who were pregnant or who planned pregnancy, and who were on MDI therapy for at least three months, before study start. Detailed inclusion and exclusion criteria of participants enrolled across 22 investigational centers throughout Poland have been published elsewhere [30]. Briefly, women with T1D were eligible to take part in the study if their physician recommended and prescribed CSII therapy or sensor-augmented insulin pump (SAP) therapy due to pregnancy or a plan to become pregnant. The decision to start CSII only or CSII with CGM (CSII + CGM) was made by the physician and study participant, independent of the study. Prior enrollment in and/or withdrawal from the Orchestra Foundation registry, current participation or participation in any other interventional clinical trial within the prior 3 months, in vitro fertilization assistance, pregnancy beyond 16 weeks of amenorrhea, any diabetes other than T1D, and inability to read or write were study exclusion criteria.
This study was conducted in compliance with the Declaration of Helsinki of 2008 by means of an informed consent process, Medical Ethics Committee approval (15/KBL/OIL/2013), study training, and clinical trial registration (CinicalTrials.gov identifier NCT01779141). The summary of study visits and points of data collection, including pump and blood glucose meter data uploads to CareLink™ clinical software (Medtronic, Northridge, California, USA), are listed in Supplementary Information S1. The informed consent form was signed at either the first (preconception) visit or first visit within the first trimester of pregnancy. The study protocol was approved by a Central Ethics Committee (Regional Chamber of Physicians at Krakow) for all investigational sites. Competent Authority approval was not required for observational studies in Poland. A STROBE cohort checklist [31] was completed for this report.
The Orchestra Foundation funded the CSII therapy for study participants. Approximately 60% were provided a MiniMed™ Paradigm™ REAL-Time 722 insulin pump (Medtronic) with or without a MiniMed™ Sof-sensor™ senor (Medtronic), and the remainder were provided a MiniMed™ Paradigm™ Veo™ system with the Enlite™ sensor (Medtronic). Participants provided the SAP system were not required to use the low-glucose suspend function.
Women participating in this study received intensive diabetes management that involved education and/or training on diet and carbohydrate counting, physical activity, folic acid supplementation, glycemic goals, self-monitoring of blood glucose (SMBG), and insulin dose adjustment, pump and CGM management (e.g., system calibrations and glucose sensor and infusion set changes). Care included frequent outpatient visits, and hospitalization if necessary. Participants underwent regular routine follow-up, without special requirements or regimens, which involved standard medical information collection into electronic clinical report forms and occasional data upload from devices (pumps and blood glucose meters) into CareLink™ clinical software (Medtronic). The study duration for each participant was up to 22 months (i.e., up to 12 months pre-conception and, if applicable, up to six weeks after delivery).
Statistical and safety outcomes analyses
The primary objective was to assess the effect of CSII therapy with or without CGM on the HbA1c of overall women and those who enrolled before and during pregnancy, in general. Secondary objectives included assessment of maternal glycemic outcomes (i.e., sensor glucose [SG], standard deviation [SD] of SG, coefficient of variation [CV] of SG, and the percentage of time spent at SG ranges [32]) during CSII CSII + CGM use. Exploratory post hoc analysis of HbA1c was performed during CSII only therapy versus CSII + CGM. Analyses were conducted with two-sample t test or Wilcoxon rank-sum test (for categorical data), and a p < 0.05 was considered statistically significant. Missing data may have not been available due to a study participant forgetting to upload to CareLink™ clinical or not uploading successfully due to a technical issue. However, no imputation was applied for missing data in this study. Data were not adjusted for confounding.
The prevalence of pregnancy complications (i.e., large for gestational age [LGA], macrosomia, jaundice, congenital malformation, and neonatal death]) and admissions to the neonatal intensive care unit were recorded. LGA was based on Polish percentile grids that calculated neonatal weight in relation to a newborn’s sex [33]. Pregnancy dating was calculated according to first trimester ultrasound scan (i.e., crown-rump length between 30 and 84 mm, which corresponds with the 9 + 5–14 + 1 weeks of pregnancy [according to https://fetalmedicine.org/research/pregnancyDating]).
Exploratory post hoc analysis assessed the association of maternal SG, SD of SG, percentage of time spent at target SG range (63–140 mg/dL [3.5–7.8 mmol/L]) and 1-h postprandial SG [34, 35] with non-LGA versus LGA delivery and positive versus negative composite neonatal outcomes. An odds ratio of mean (95% confidence interval) was used to determine the strength of association and was analyzed with logistic regression. A p < 0.05 was considered statistically significant. Positive neonatal composite outcomes were defined as deliveries that were without congenital malformation, did not require mechanical ventilation, and were not LGA. Negative neonatal outcomes deliveries involved congenital malformation, mechanical ventilation requirement, LGA delivery or admittance to the neonatal care unit.
Due to the observational study design, methods to reduce bias were limited and analyses were conducted with respect to intention to treat. Safety outcomes were summarized as the incidence of maternal severe hypoglycemia (hypoglycemia requiring third-party assistance); diabetic ketoacidosis; unanticipated adverse device effects (UADEs, any serious adverse device effect which by its nature, incidence, severity or outcome had not been identified in the current version of the risk analysis report); serious adverse events (SAEs, defined as an adverse event that led to death, serious deterioration in the health of the subject that either resulted in a life-threatening illness or injury, or a permanent impairment of a body structure or a body function, or hospitalization); a medical or surgical intervention to prevent life-threatening illness or injury or permanent impairment to a body structure or a body function; or fetal distress, fetal death, congenital abnormality or birth defect. In the present study, severe hypoglycemia and diabetic ketoacidosis were treated as severe adverse events. The SAE and UADE information was collected throughout the study and reported immediately to Medtronic Poland (Sp.z.o.o) via an SAE/UADE form incorporated in the electronic clinical record.
Results
A flow diagram (Supplementary Information S2) of participant disposition shows that a total of 481 women (mean age of 30.4 ± 4.0 years and diabetes duration of 12.3 ± 7.7 years) enrolled in the study; 216 of whom were not pregnant. There were 121 who dropped out or were withdrawn before pregnancy and 60 who dropped out or were withdrawn during pregnancy: the latter included 28 who miscarried, 10 early withdrawals prior to delivery, and 22 who gave birth but were lost to follow-up. Of the total 360 pregnant women, 190 (52.8%) used CGM with CSII therapy.
Table 1 summarizes the age, glycemic metrics, total daily insulin, and medical history of the overall group, at baseline. The same characteristics are shown for those who used CSII only or CSII + CGM. The rate of complications (macroangiopathy, nephropathy, neuropathy, and retinopathy) is also provided for each of the aforementioned groups.
Maternal glucose outcomes
Mean HbA1c at each trimester is shown for the overall group and those who enrolled before or during pregnancy, stratified by therapy use (Table 2). Women who enrolled during pregnancy made up a significant proportion of the overall group and their mean HbA1c at T1 trended higher (N = 262, 7.0 ± 1.2% [53.1 ± 12.9 mmol/mol]) than that of women who enrolled before pregnancy (N = 92, 6.2 ± 0.7% [44.5 ± 7.7 mmol/mol]). By T3, however, mean HbA1c for both groups (5.9 ± 0.7% [41.2 ± 8.1 mmol/mol] and 6.0 ± 0.7% [41.9 ± 7.7 mmol/mol], respectively) appeared relatively comparable. The use of CGM with CSII therapy by women who enrolled during pregnancy, compared with CSII alone, resulted in a statistically significant reduction in HbA1c over the course of pregnancy (Table 2). This trend was not observed in women who enrolled before pregnancy, although HbA1c reduced with time.
The proportion of women from all groups achieving mean HbA1c ranges throughout pregnancy, including the mean target HbA1c of < 6.0% (< 42.0 mmol/mol) [34, 35], is stratified by therapy use and shown in Supplementary Information S3. The percentage achieving target HbA1c tended to increase from trimesters 1 to 3 and were 20.9% (74/354), 65.1% (207/318), and 58.0% (148/255), respectively. By trimester 3, the proportion who achieved target HbA1c with CSII only was 49.1% (N = 53/108), while that for women who used CGM with CSII was 64.6 (N = 95/147).
Table 3 shows the CGM outcomes of all women who used CGM with CSII therapy. Average SG for all groups was < 120 mg/dL (< 6.7 mmol/L), CV of SG averaged < 33%, and a trending increase in time spent in target range from the first to the third trimester was observed. While time in hypoglycemic ranges (< 63 mg/dL [< 3.5 mmol/mol] and < 54 mg/dL [< 3.0 mmol/mol]) still averaged more than the targeted < 1 h/day and < 0.25 h/day, respectively, time in target range reached > 70% and the proportion of time spent at > 140 mg/dL (> 7.8 mmol/mol) remained below 25%, for all groups.
Neonatal status and outcomes
For the overall group and those who enrolled before or during pregnancy, a summary of neonatal status (i.e., sex, gestational delivery, mean birth length and weight), rates of blood glucose levels ≤ 40 mg/dL, and prevalence of complications ([e.g., large for gestational age, macrosomia, jaundice, congenital malformation, and death]) are detailed in Supplementary Information S4. Briefly, the rates of LGA (birth weight > 90th percentile) were 22.7% (74/326), 28.0% (23/82), and 20.9% (51/244) for each respective group. For women using only CSII, the rate was 24.6% (34/138), and for those using CGM with CSII it was 21.3% (40/188). Rates of neonatal hypoglycemia (BG ≤ 40 mg/dL) were also low across groups and were 20.1% (51/254), 17.9% (10/56), and 20.7% (41/198), respectively, and appeared relatively comparable between women who used CSII only (21.0% [21/100]) and CGM with CSII (19.5% [30/154]). This trend was also observed for Caesarean births, where women who used CGM demonstrated a rate of 22% (42/189) and those who used only CSII demonstrated a rate of 24.5% (34/139). The exploratory analysis of non-LGA versus LGA delivery and positive versus negative neonatal composite outcomes with respect to maternal CGM metrics demonstrated strong association with most of the recommended glycemic targets for pregnancy (Table 4).
Safety analyses
Regarding overall safety outcomes, there were 377 adverse events and 364 SAEs (Supplementary Information S5). Of the 364 SAEs, 97 were in the group that enrolled before pregnancy and 267 were in the group that enrolled during pregnancy. There were 357 non-device-related events that included three episodes of DKA and seven device-related events that included three episodes of DKA. There were eight episodes of severe hypoglycemia; three were in the group that enrolled before pregnancy and five were in the group that enrolled during pregnancy. All episodes of severe hypoglycemia occurred in participants who used CGM with CSII therapy. There were no reports of UADEs. There was one report of maternal death due to chronic kidney disease, 6 months after delivery.
Discussion
This observational study shows that CSII therapy helped women with T1D who were pregnant or planning pregnancy achieve glycemic targets throughout pregnancy. Specifically, HbA1c levels of the overall group were reduced from 6.8 ± 1.1% (50.9 ± 12.3 mmol/mol) at trimester 1 to 5.8 ± 0.7% (40.1 ± 8.0 mmol/mol) and 5.9 ± 0.7% (41.4 ± 8.0 mmol/mol) at trimesters 2 and 3, respectively. There was also a trending increase in the proportion of women achieving target HbA1c by the third trimester. For the group who enrolled during pregnancy and used CGM with CSII, mean HbA1c was significantly reduced over trimesters, when compared to the HbA1c of women using only CSII. The significant reduction in HbA1c, with time, may not have been observed in women who enrolled before pregnancy due to the smaller sample size, as well as a smaller HbA1c difference between the CSII only and CGM + CSII therapies, at study start. For instance, this group demonstrated near-target HbA1c at T1, compared with the HbA1c of women who enrolled during pregnancy. While they also spent a lower percentage of time in hypoglycemia, all women using CGM with CSII spent time in target range that exceeded > 70% by the third trimester.
Exploratory analyses showed that achieving lower HbA1c and increased time in target glycemic range was associated with better neonatal outcomes. For the overall group of women, those who used CSII only and those who used CGM with CSII, the LGA delivery incidence rates were lower than other previously reported rates that reached ≥ 50%, in pregnant women with pregestational TD [21, 36]. When evaluated against the World Health Organization criteria [37], the LGA rates for each aforementioned group were 35.3%, 39.9%, and 31.9%, respectively.
Several organizations have recommended targeted diabetes management for pregnancies complicated by T1D: an HbA1c target of < 6.0% (< 42 mmol/mol) [34, 35], a fasting glucose level of < 90 mg/dL (< 5.0 mmol/L) [35] or < 95 mg/dL (< 5.3 mmol/L) [34], and a 1-h postprandial glucose concentration of < 140 mg/dL (< 7.8 mmol/L) [34, 35]. These metrics worsen in the later trimesters of pregnancy where challenges with gastric emptying and insulin kinetics [38] and impaired glucose metabolism [39] result in increased time above SG target range [20, 21, 28]. In the present study, however, these metrics met or aligned closely with consensus recommendations (e.g., average SG, 1-h postprandial SG of < 120 mg/dL, and CV of SG < 36%) [34, 40].
Prospectively randomized [28, 29, 41] and retrospective [21, 42] studies of CSII and/or CGM use versus MDI and SMBG measurements have demonstrated clinical benefits for mothers and their babies. Although the proportion of time spent in target glucose range increased and HbA1c improved (or did not change) with CGM technology relative to control [21, 28], only a small percentage of study participants reached the international consensus recommended TIR of > 70% (~ 17 h of the day). In addition, the overall rates of LGA deliveries in some of these trials remained rather high, averaging close to 50% in the intervention groups and up to 70% in the control groups. A recent observational study of pregnant women with T1D (N = 81, 11 on MDI and 70 on CSII [28 used CGM]), some of whom underwent pregnancy planning, demonstrated significantly improved HbA1c in those who used CGM with CSII compared to CSII or MDI therapy only (time spent at sensor glucose ranges was not analyzed) [27]. However, there was no difference in macrosomia risk between groups and the rate observed for women using CGM + CSII was 21.4%, but 16.7% for women using CSII only. In the present study, rates of macrosomia (weight of ≥ 4000 g) trended similarly and were 22.8% (43/189) for women using CGM + CSII and 18.0% (25/139) for those using only CSII.
Limitations of the current study include its observational and non-randomized design, and the relatively good glycemia management in study participants before and/or during the first trimester, which may preclude generalizability of findings. In addition, a majority of participants received multidisciplinary clinical support from gynecologists/obstetricians, diabetologists, nurses, and dieticians during the study. Similar findings of significantly reduced adverse pregnancy outcomes during prospective observational [25] and retrospective [43] studies have been reported in women with ideally managed T1D receiving comprehensive preconception-to-pregnancy planning or healthcare management. Thus, a clear distinction between the contribution of technological devices and a comprehensive multidisciplinary approach to diabetes management during pregnancy cannot be easily delineated. Indeed, the observational design was intended to bench mark the achievements of care in diabetes pregnancy clinics that used diabetes technology, not provide specific comparative outcomes. Strengths of this study include its report of outcomes observed in over 300 pregnancies complicated by T1D in women who demonstrated good compliance, enrolled pre- and postconception, and for whom HbA1c and CGM data could be analyzed.
Conclusions
This observational investigation determined that good maternal glycemia and positive neonatal outcomes can be achieved in a majority of women who were pregnant or planned pregnancy and used CSII only or CGM with CSII. Maternal HbA1c and glucose levels improved throughout the course of pregnancy and positive neonatal composite outcomes were associated with an increased duration of maternal time spent within target glucose range. Although current insulin delivery therapies have advanced to include predictive insulin suspension and/or automated insulin delivery based on CGM, present study findings serve as a benchmark for pregnancy outcomes in women with T1D using only CSII or CGM with CSII.
Data availability
Study data can be accessed via this manuscript and its supplementary information or materials.
References
Beck RW, Riddlesworth T, Ruedy K et al (2017) Effect of continuous glucose monitoring on glycemic control in adults with type 1 diabetes using insulin injections: the diamond randomized clinical trial. JAMA 317(4):371–378
Bergenstal RM, Tamborlane WV, Ahmann A et al (2010) Effectiveness of sensor-augmented insulin-pump therapy in type 1 diabetes. N Engl J Med 363(4):311–320
O’Connell MA, Donath S, O’Neal DN et al (2009) Glycaemic impact of patient-led use of sensor-guided pump therapy in type 1 diabetes: a randomised controlled trial. Diabetologia 52(7):1250–1257
Bode BW, Steed RD, Davidson PC (1996) Reduction in severe hypoglycemia with long-term continuous subcutaneous insulin infusion in type I diabetes. Diabetes Care 19(4):324–327
Misso ML, Egberts KJ, Page M, Oconnor D, Shaw J (2010) Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus. Cochrane Database Syst Rev 1:CD005103
Feldman AZ, Brown FM (2016) Management of type 1 diabetes in pregnancy. Curr Diab Rep 16(8):76
Evers IM, de Valk HW, Mol BW, ter Braak EW, Visser GH (2002) Macrosomia despite good glycaemic control in type I diabetic pregnancy; results of a nationwide study in the netherlands. Diabetologia 45(11):1484–1489
Cullen MT, Reece EA, Homko CJ, Sivan E (1996) The changing presentations of diabetic ketoacidosis during pregnancy. Am J Perinatol 13(7):449–451
Cohen AL, Wenger JB, James-Todd T et al (2014) The association of circulating angiogenic factors and HbA1c with the risk of preeclampsia in women with preexisting diabetes. Hypertens Pregnancy 33(1):81–92
Evers IM, de Valk HW, Visser GH (2004) Risk of complications of pregnancy in women with type 1 diabetes: nationwide prospective study in the netherlands. BMJ 328(7445):915
Lapolla A, Dalfra MG, Di Cianni G, Bonomo M, Parretti E, Mello G et al (2008) A multicenter Italian study on pregnancy outcome in women with diabetes. Nutr Metab Cardiovasc Dis 18(4):291–297
Boulot P, Chabbert-Buffet N, d’Ercole C et al (2003) French multicentric survey of outcome of pregnancy in women with pregestational diabetes. Diabetes Care 26(11):2990–2993
Persson M, Cnattingius S, Wikstrom AK, Johansson S (2016) Maternal overweight and obesity and risk of pre-eclampsia in women with type 1 diabetes or type 2 diabetes. Diabetologia 59(10):2099–2105
Persson M, Pasupathy D, Hanson U, Norman M (2011) Birth size distribution in 3,705 infants born to mothers with type 1 diabetes: a population-based study. Diabetes Care 34(5):1145–1149
Penney GC, Mair G, Pearson DW (2003) The relationship between birth weight and maternal glycated haemoglobin (HbA1c) concentration in pregnancies complicated by type 1 diabetes. Diabet Med J Brit Diabet Assoc 20(2):162–166
Casson IF, Clarke CA, Howard CV et al (1997) Outcomes of pregnancy in insulin dependent diabetic women: results of a five year population cohort study. BMJ 315(7103):275–278
Clausen TD, Mathiesen ER, Hansen T et al (2008) High prevalence of type 2 diabetes and pre-diabetes in adult offspring of women with gestational diabetes mellitus or type 1 diabetes: the role of intrauterine hyperglycemia. Diabetes Care 31(2):340–346
Cyganek K, Skupien J, Katra B et al (2017) Risk of macrosomia remains glucose-dependent in a cohort of women with pregestational type 1 diabetes and good glycemic control. Endocrine 55(2):447–455
Hillier TA, Pedula KL, Schmidt MM et al (2007) Childhood obesity and metabolic imprinting: the ongoing effects of maternal hyperglycemia. Diabetes Care 30(9):2287–2292
Kerssen A, de Valk HW, Visser GH (2004) Day-to-day glucose variability during pregnancy in women with type 1 diabetes mellitus: glucose profiles measured with the continuous glucose monitoring system. BJOG 111(9):919–924
Kristensen K, Ogge LE, Sengpiel V et al (2019) Continuous glucose monitoring in pregnant women with type 1 diabetes: an observational cohort study of 186 pregnancies. Diabetologia 62(7):1143–1153
Manderson JG, Mullan B, Patterson CC (2002) Cardiovascular and metabolic abnormalities in the offspring of diabetic pregnancy. Diabetologia 45(7):991–996
Cyganek K, Hebda-Szydlo A, Katra B et al (2010) Glycemic control and selected pregnancy outcomes in type 1 diabetes women on continuous subcutaneous insulin infusion and multiple daily injections: the significance of pregnancy planning. Diabetes Technol Ther 12(1):41–47
Neff KJ, Forde R, Gavin C et al (2014) Pre-pregnancy care and pregnancy outcomes in type 1 diabetes mellitus: a comparison of continuous subcutaneous insulin infusion and multiple daily injection therapy. Ir J Med Sci 183(3):397–403
Zheng X, Yang D, Luo S et al (2021) Association of implementation of a comprehensive preconception-to-pregnancy management plan with pregnancy outcomes among Chinese pregnant women with type 1 diabetes: the carnation study. Diabetes Care 44(4):883–892
Evers IM, de Valk HW, Mol BW, ter Braak EW, Visser GH (2002) Macrosomia despite good glycaemic control in type 1 diabetic pregnancy; results of a nationwide study in the netherlands. Diabetologia 45(11):1484–1489
Lason I, Cyganek K, Witek P (2021) Continuous glucose monitoring and insulin pump therapy in pregnant women with type 1 diabetes mellitus. Ginekol Pol 92(10):675–681
Feig DS, Donovan LE, Corcoy R et al (2017) Continuous glucose monitoring in pregnant women with type 1 diabetes (CONCEPTT): a multicentre international randomised controlled trial. Lancet 390(10110):2347–2359
Murphy HR, Rayman G, Lewis K et al (2008) Effectiveness of continuous glucose monitoring in pregnant women with diabetes: randomised clinical trial. BMJ 337:a1680
Sieradzki J, Cyganek K, Cypryk K et al (2018) Objectives and methods of the orchestra foundation registry study: a multicenter observational study of the use of insulin pump therapy in pregnant women with type 1 diabetes mellitus in Poland. Clin Diabetol 7(3):151–158
von Elm E, Altman DG, Egger M et al (2007) Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 335(7624):806–808
Battelino T, Danne T, Bergenstal RM et al (2019) Clinical targets for continuous glucose monitoring data interpretation: recommendations from the international consensus on time in range. Diabetes Care 42(8):1593–1603
Palczewska I, Niedzwiedzka Z (2001) Somatic development indices in children and youth of Warsaw [wskazniki rozwoju somatycznego dzieci I mlodziezy warszawskiej]. Med Wieku Rozw 5(2):18–118
Draznin B, Aroda VR, Bakris G et al (2022) 15. Management of diabetes in pregnancy: standards of medical care in diabetes-2022. Diabetes Care 45(Suppl 1):S232–S243
Araszkiewicz A, Bandurska-Stankiewicz E, Borys S et al (2021) Guidelines on the management of patients with diabetes a position of diabetes Poland. Clin Diabetol 10(1):1–113
Hauffe F, Schaefer-Graf UM, Fauzan R et al (2019) Higher rates of large-for-gestational-age newborns mediated by excess maternal weight gain in pregnancies with type 1 diabetes and use of continuous subcutaneous insulin infusion vs multiple dose insulin injection. Diabet Med 36(2):158–166
Fenton TR, Kim JH (2013) A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr 13:59
Murphy HR, Elleri D, Allen JM et al (2012) Pathophysiology of postprandial hyperglycaemia in women with type 1 diabetes during pregnancy. Diabetologia 55(2):282–293
Mazze R, Yogev Y, Langer O (2012) Measuring glucose exposure and variability using continuous glucose monitoring in normal and abnormal glucose metabolism in pregnancy. J Matern Fetal Neonatal Med 25(7):1171–1175
Murphy HR (2019) Continuous glucose monitoring targets in type 1 diabetes pregnancy: every 5% time in range matters. Diabetologia 62(7):1123–1128
Law GR, Ellison GT, Secher AL et al (2015) Analysis of continuous glucose monitoring in pregnant women with diabetes: distinct temporal patterns of glucose associated with large-for-gestational-age infants. Diabetes Care 38(7):1319–1325
Kallas-Koeman MM, Kong JM, Klinke JA et al (2014) Insulin pump use in pregnancy is associated with lower HbA1c without increasing the rate of severe hypoglycaemia or diabetic ketoacidosis in women with type 1 diabetes. Diabetologia 57(4):681–689
Yoeli-Ullman R, Dori-Dayan N, Mazaki-Tovi S et al (2020) Towards implementation of the saint vincent declaration: outcomes of women with pregestational diabetes. Isr Med Assoc J 22(3):137–141
Acknowledgements
The authors thank the study participants, the Fundacja Wielka Orkiestra Swiatecznej Pomocy for its support during the study, and investigational staff for their conduct of the study. Fen Peng, PhD; Mong-Hang Nguyen, BSc; and Yongyin Wang, PhD, MSc (Medtronic, Northridge, California, USA) assisted with statistical analyses. Marion Jamieson (Medtronic, Melbourne, Australia) helped develop and edit the manuscript.
Funding
This study was funded by Medtronic (Northridge, California, USA). Insulin pumps were donated by the Fundacja Wielka Orkiestra Swiatecznej Pomocy.
Author information
Authors and Affiliations
Contributions
KC, EWO, KC, and JS developed the study concept and designed and managed the study conducted at their investigational sites, contributed to the data analyses and interpretation of results, and reviewed and edited the final work. KS, JS, XC, TLC, and OC (employees of Medtronic) analyzed data or interpreted data for the work, drafted or critically revised the work, and agreed to accountability for the final work. KC had complete access to all data and, as guarantor, has taken responsibility for the integrity of the data and the accuracy of data analyses.
Corresponding author
Ethics declarations
Conflicts of interest
KC received speaker honoraria from or participated on advisory boards for Novo Nordisk, Eli Lilly and Company, Sanofi, AstraZeneca, Boehringer Ingelheim, Medtronic and Servier Laboratories; received research support from Medtronic. EWO received funding for teaching and lecturing study participants, attending the Steering Committee meetings, and received research support from Medtronic. KC received consultant honoraria from or participated on advisory boards for Medtronic, Roche, and NovoNordisk; received speaker honoraria from Medtronic, Roche, Eli Lilly and Company, NovoNordisk, Acensia Diabetes Care, and Sanofi; and received research support from Medtronic. JS received research support from Medtronic. KS, XC, TLC, JS and OC are employees of Medtronic.
Ethical approval
This study was conducted in compliance with the Declaration of Helsinki of 2008 by means of an informed consent process, Medical Ethics Committee (Regional Chamber of Physicians at Krakow) approval (15/KBL/OIL/2013), study training, and clinical trial registration (CinicalTrials.gov identifier NCT01779141).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Portions of this work have been previously presented in poster format at the 10th International Symposium on Diabetes, Hypertension, Metabolic Syndrome and Pregnancy (Florence, Italy, May 29–June 1, 2019).
This article belongs to the topical collection Pregnancy and Diabetes, managed by Antonio Secchi and Marina Scavini.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cypryk, K., Wender-Ozegowska, E., Cyganek, K. et al. Insulin pump therapy with and without continuous glucose monitoring in pregnant women with type 1 diabetes: a prospective observational Orchestra Foundation study in Poland. Acta Diabetol 60, 553–561 (2023). https://doi.org/10.1007/s00592-022-02020-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-022-02020-9